
Abstract
Objective
This article examines and summarizes the published epidemiological literature on cross-cultural variations. Particular emphasis was put on addressing cross-cultural beliefs on the causes, management, and attitude toward cleft lip and/or cleft palate. A healthcare provider's awareness of these cross-cultural attitudes and beliefs is vital for promoting effective collaboration with patients’ families and ensuring a favorable medical outcome.
Design
Systematic review.
Setting
Not applicable.
Participants
Patients with cleft lip and/or cleft palate, their families, their communities, and healthcare providers.
Interventions
Not applicable.
Main Outcome Measures
Not applicable.
Results
All relevant and eligible studies were identified using PubMed and Google Scholar databases. The cultural belief was categorized and measured using Murdock's Theories of Illness. The study was reported in compliance with PRISMA guidelines. The quality of the selected studies was evaluated in accordance with the Critical Appraisal Skills Programme criteria (CASP). Fourteen articles covering thirteen countries on four continents met the inclusion criteria. In diverse communities, cleft lip and/or cleft palate was attributed to natural (infection, medication, improper diet, smoke, or radiation) or supernatural (God, eclipse, ancestral spirit, and curse) causes. Reported consequences include stigmatization, inappropriate treatments, leaving patients untreated, and infanticide.
Conclusion
Cultural beliefs are the main cause of misconceptions surrounding a cleft lip and/or cleft palate. There is also a need for public health care providers’ intervention to educate society about the natural causes and ease of management, thereby increasing opportunities for patients substantially.
Introduction
Cleft lip and/or cleft palate (CL/P) is typically considered one of the most frequent congenital malformations affecting orofacial areas. Worldwide, the incidence of CL/P varies considerably within multiethnic groups, with the highest prevalence reported among Asians and Native Americans (1 per 500 live births). 1 CL/P could be one feature of more than 300 syndromes. Nonetheless, two-thirds of these conditions are non-syndromic (isolated), and their etiology is unknown so far. 2
CL/P can be classified as complete or incomplete and unilateral or bilateral. Obviously, with the increasing severity of the cleft, there is an increase in levels of morbidity among children with CL/P. Of these morbidities, the children with CL/P could have obvious facial disfigurement, speech, hearing, feeding difficulties, and psychosocial challenges that can profoundly lower their life outcomes. Of note, the consequences of CL/P are not limited to the children, but their parents might also be severely affected. For example, parents of a child with CL/P have been noted to complain of psychological burdens, such as helplessness, guilt, distress, or depression. 3 Another critical hurdle facing the parents is the burden of care because the patients require many surgical corrective therapies, special education, rehabilitation, and other nonmedical services. 4 These physical, psychological, and financial burdens are often worsened by stigmatization, particularly in lower-income countries, where the causes of this phenomenon are often misunderstood, and people resort to their cultural perceptions to provide a plausible explanation for its occurrence. Indeed, linking these facial defects with cultural beliefs could further exacerbate the social stigma and exclusion and negatively affect the management protocol.
Historically, Ballantyne provided significant overviews describing the past theories suggested to explain the causes of deformities, including facial clefts in infants. 5 Of particular interest is that maternal impression theory has been found to be culturally universal. Some recent works have also been conducted to describe the current cultural perceptions, ideas, or folklore surrounding deformity in specific contexts and settings across the globe.6,7 Such insights into various assumptions concerning cleft causation and management are valuable to enrich cross-cultural understanding of these conditions, mainly because the cultural background of the CL/P patients and their families can significantly influence their choices of medical and psychosocial treatments.
It is widely accepted that the systematic neglect of cultural beliefs in health and healthcare is a significant barrier to advancing the highest standard of health worldwide. Concerning CL/P patients treated by multidisciplinary clinical care, gaining knowledge on cross-cultural variation and attitudes toward these conditions is crucial to improving the medical outcomes and social development of these groups of patients. Even though several reports have evaluated the cultural attitude toward CL/P causation, management, and the reaction of societies in specific countries, to our knowledge, no systematic review of epidemiological literature has discussed and summarized the cross-cultural variations on these topics so far.
To achieve this aim, the study seeks to answer three specific questions: (1) what are the causes of CL/P from cultural perspectives, (2) what cultural medications are used to treat a CL/P patient, and (3) how is society around the patients respond to the birth of a CL/P child?
Materials and Methods
This systematic review was conducted following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) checklist. 8 The Prisma Statement checklist is presented in the supplementary material (Tables S1 & S2). It was also registered at the International Prospective Register of Systematic Reviews (PROSPERO) database (CRD42022384382). 9 Ethics approval and informed consent prior to the study were not required for this systematic review because the authors used publicly accessible documents as data and evidence.
Inclusion Criteria
Studies were considered eligible if they aimed to assess the perspectives of the societies and/or parents on the cause, treatment, and response to CL/P. Given the variability in the definition of perspective in the literature, for this review, we defined perspective as follows: 1) Ideas and perception of the causes of CL/P, 2) Belief and perception of the causes of CL/P from both religious and cultural perspectives, 3) Knowledge about the etiology of CL/P, 4) Reaction to the birth of a child with CL/P, 5) The response toward the grown-up CL/P patients. 6) How a society treats CL/P patients, 7) Experience of patients and family regarding the issues surrounding CL/P, and 8) Miscellaneous aspects associated with CL/P. All measurements, including validated or invalidated questionnaires, interviews, and observations, were considered suitable. The included articles were English language sources only.
Exclusion Criteria
Literature reviews were ineligible for data extraction, yet they were considered for cross-reference purposes. Studies that evaluated cultural perceptions on the causes, treatment, and responses to child deformities other than CL/P were also excluded.
Information Sources and Study Selection
A thorough search was conducted to explore PubMed and Google Scholar to select the articles. All searches were performed in February 2020 and updated in March 2022. The Boolean operators “AND” and “OR” combined and narrowed the search. All variations of (cleft lip and/or palate, culture, religion, ideas, perspective, response, treatment, and belief or belief) were searched in combination with all other search terms (details in appendix). After determining the studies relevant to the research questions, the reference lists of those studies were searched as well for similar studies. There were no restrictions regarding the geographic origin or year of publication.
The first two authors (H&AAA) worked independently to find related literature and made a narrative database in Microsoft Excel, which included: a bibliographic record, type of source, title, setting, cultural perspective on the causes, management, and responses to the birth of a child with a CL/P. Further, a proforma was prepared by the same authors to identify the following features of each study: checked for duplication, checked if the sources met all the specified eligibility criteria, checked the data reliability and validity, and reviewed the narrative data that had been tabulated. These two authors also performed a quality assessment to prevent the inclusion of literature from unreliable sources. The entire selection process was monitored by further authors (TF & MNH)
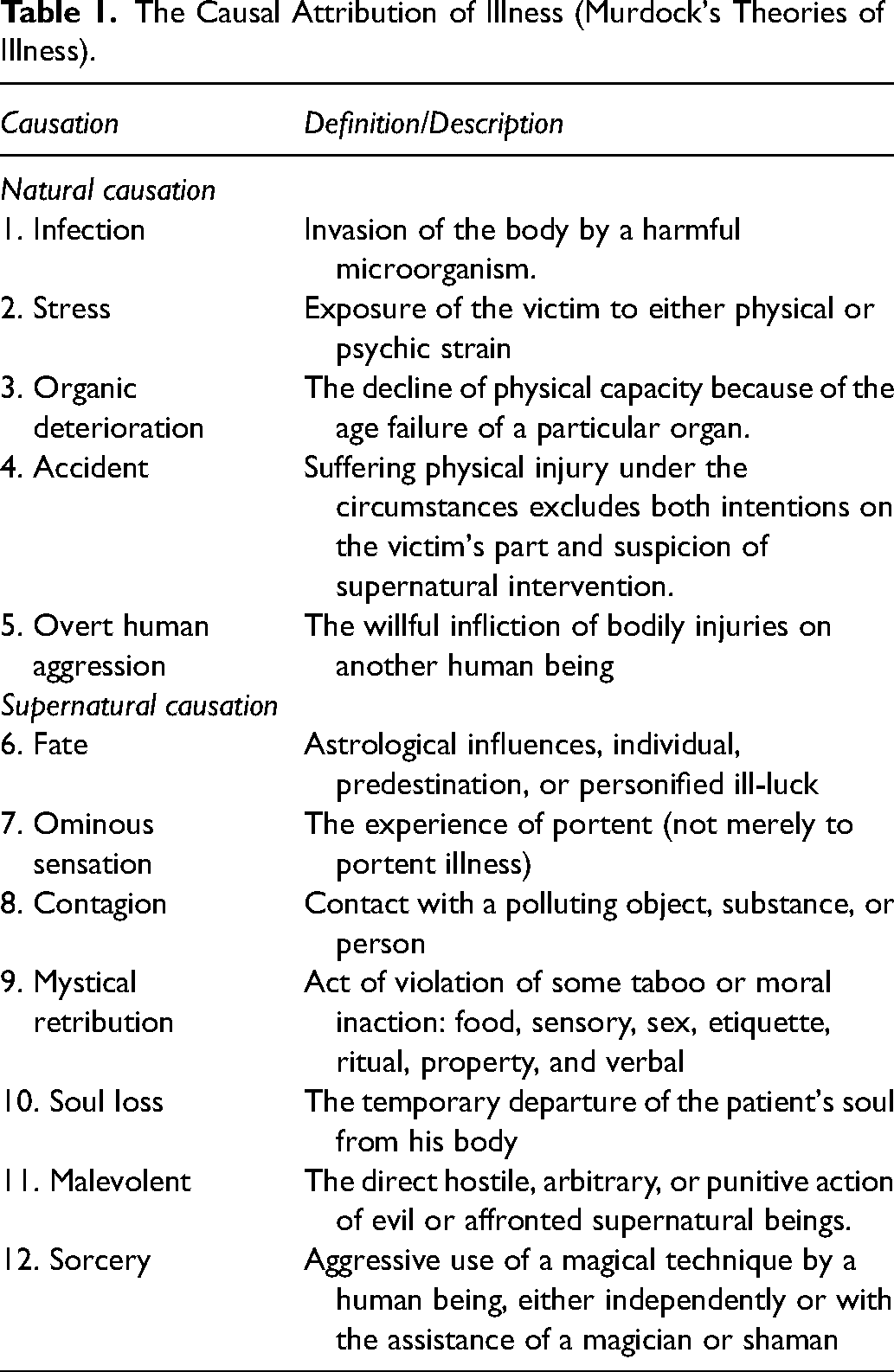
As reported in the included literature, the cultural belief was categorized and measured using the causal attribution theory of Murdock et al. 10 (Table 1). This category was used because it is the most comprehensive theory to explain illness causation. This category was made after thoroughly studying 139 cultural regions in Africa, East Asia, North and South America.
The Causal Attribution of Illness (Murdock's Theories of Illness).
Quality Assessment
The quality of each included study was assessed independently by three authors (H, AAA&MNH) based on the criteria as formulated in the Critical Appraisal Skills Program (CASP) tool. 11 Each item in the CASP checklist was assigned a numerical value: Yes = 1, Can't tell = 0, No = 0. The total score for each included study was calculated with a maximum possible score of nine. Articles with a score equal to or greater than 7 points were classified as having high quality, while studies that did not reach this score were considered lower quality. Any disagreement between the authors was resolved by discussion with a further author (MR &TF). The median score for the included studies was 8.6, showing that the articles included in this review are of high quality. The quality assessment results can be viewed in the supplementary material (Table S3).
Results
Literature Search
The selection process (Figure 1) fetched 269 PubMed and Google Scholar articles. Physical searching from the bibliography of the articles resulted in an additional 12 articles. After titles and abstract screening, 210 records were excluded as the papers did not include the perspective on CL/P's causes, treatments, and management of CL/P. Five articles were excluded due to duplication.
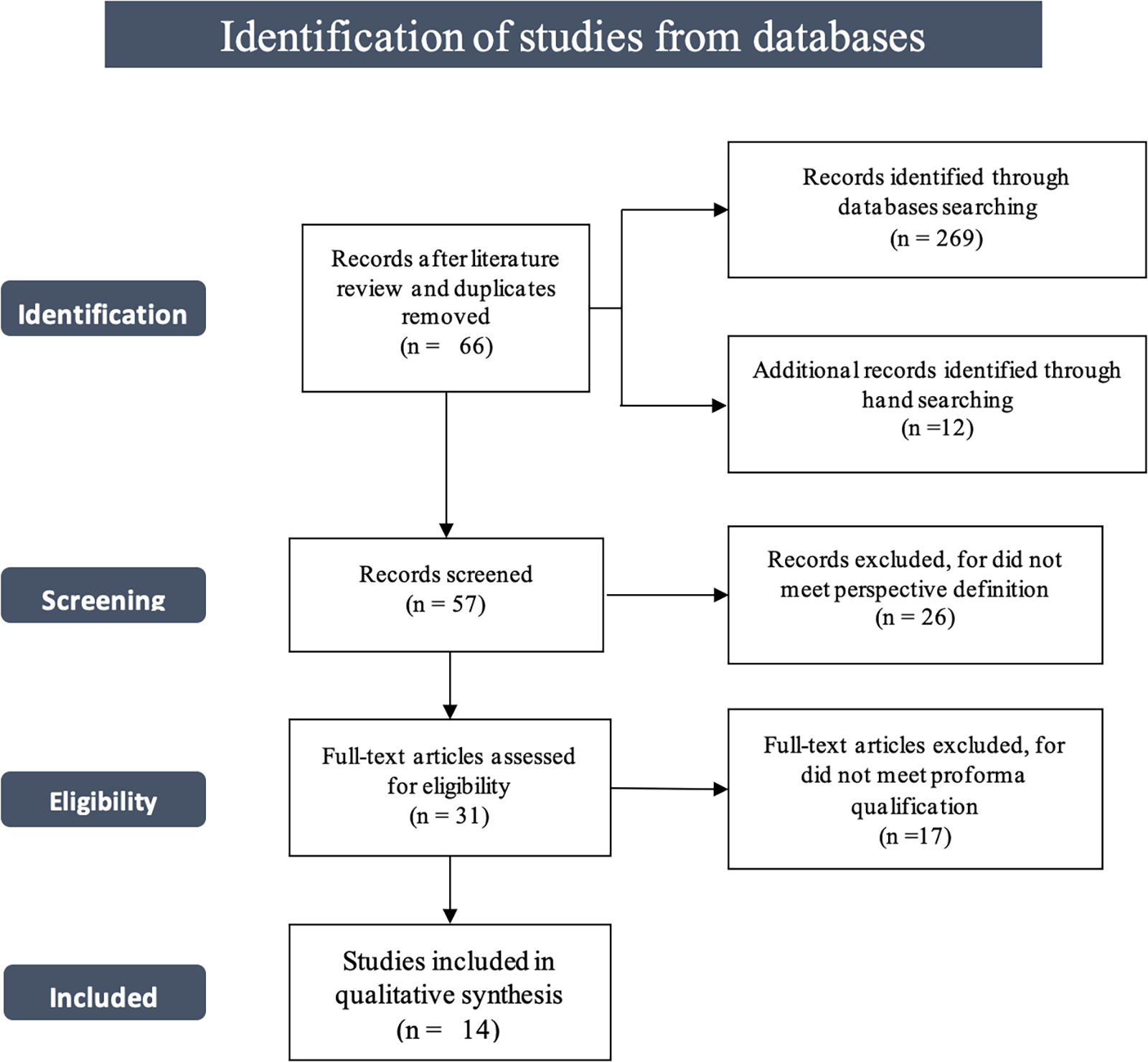
Flow diagram of the study selection process.
Among the 57 Full-text papers reviewed, 26 were excluded as they did not satisfy the inclusion criteria. Thirty-one papers fulfilled the inclusion criteria, and 17 were excluded due to a lack of quality assessment. Amongst the 17 excluded articles, one did not clearly state the beliefs of the causes and treatment of CL/P, nine book chapters referred to other sources, five articles’ full text were inaccessible, and the English version of two articles was not found. Finally, fourteen records were included in the final qualitative analysis.
Description of Studies
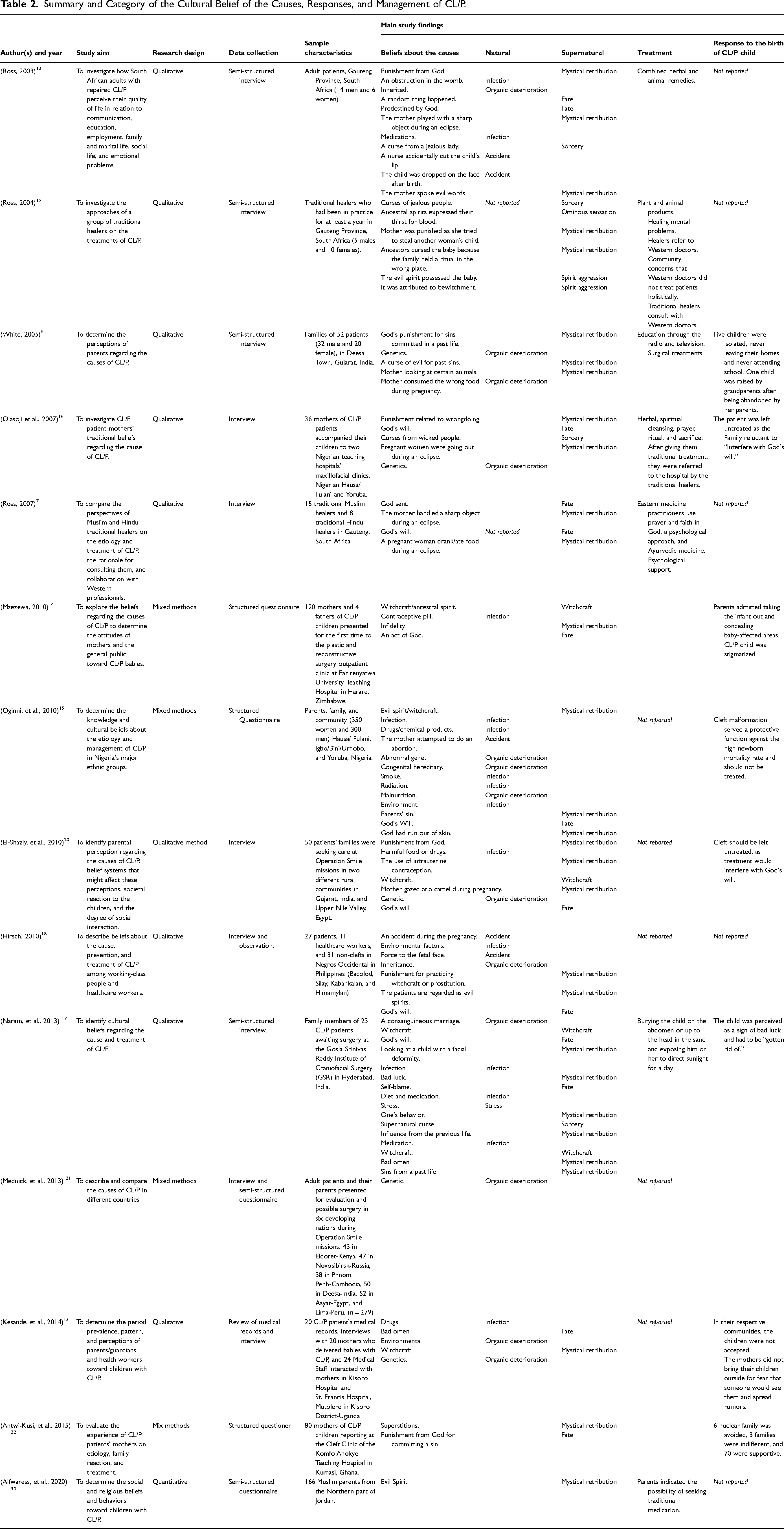
Table 2 shows the selected characteristics of all 14 included studies that were structured and categorized following the Murdock et al. typology. These studies were based in thirteen countries on four different continents: Africa (South Africa, Zimbabwe, Egypt, Nigeria, Kenya, Uganda, and Ghana), Asia (India, Philippines, Jordan, and Cambodia), Europe (Russia), and South America (Peru) (Figure 2). The geographic distribution of studies included in our review was heavily focused on African countries (n = 7, 53%). These studies estimated three essential topics on the ethnomedical aspect of CL/P, including the cultural beliefs of the causes, responses to birth, and management.
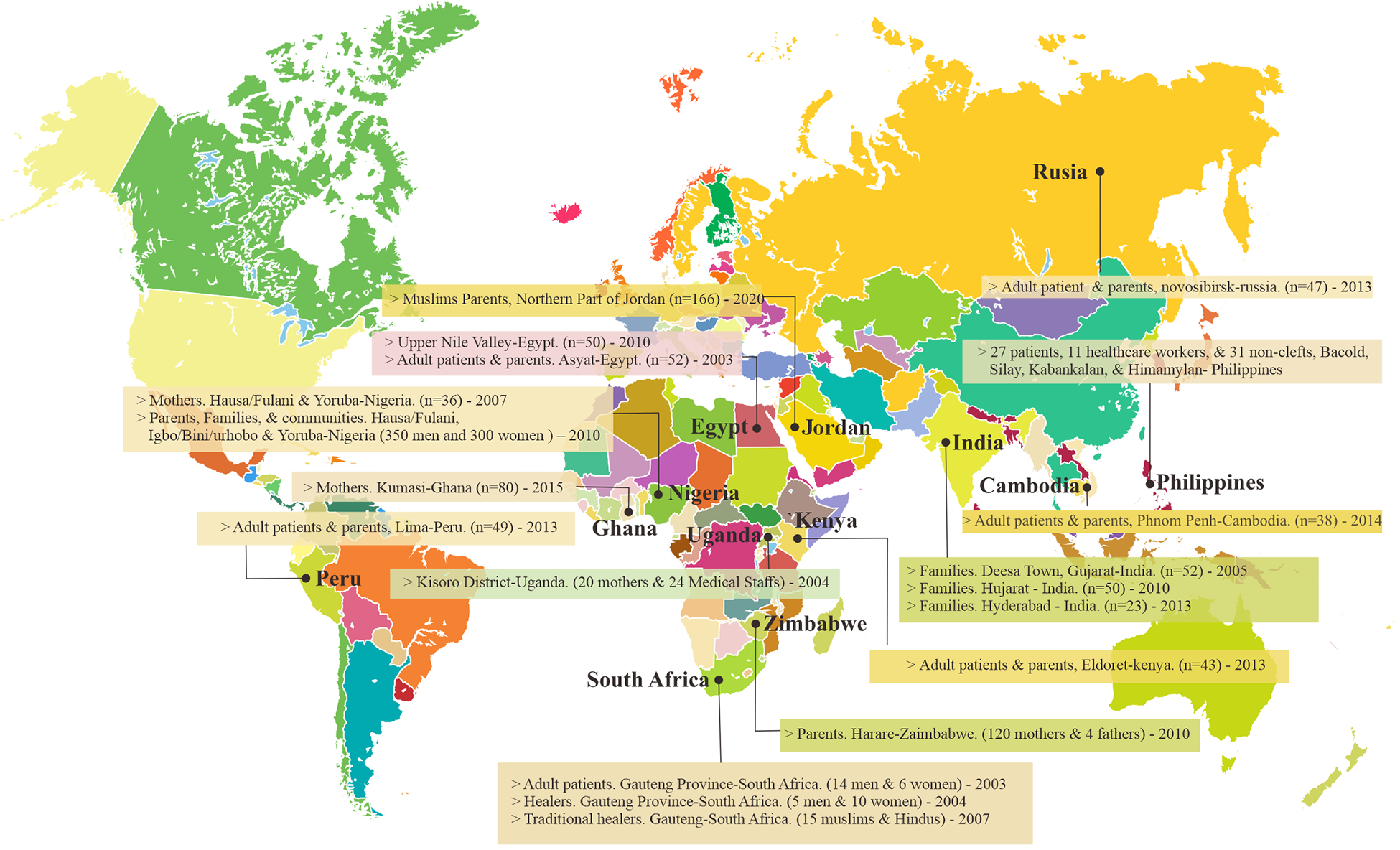
Countries of the studies included in the systematic review.
Summary and Category of the Cultural Belief of the Causes, Responses, and Management of CL/P.
Beliefs on the Cause of CL/P
Beliefs prevailing in societies concerned with the causes of CL/P vary significantly across the globe, most of which are linked to natural causes. Our results showed that infection was the most commonly held cultural belief regarding natural causes.12,13 In India, the infection was assumed to be caused by an obstruction in the womb or medication during pregnancy. 12 Another study in India revealed that the wrong foods a mother consumed during pregnancy were a risk for CL/P. 6 Medications were also suggested as a cause of CL/P in Zimbabwe, wherein the patients’ families believed that contraceptive pills taken by the mothers during pregnancy were a significant risk factor. 14 Likewise, the major ethnic groups in Nigeria believed maternal smoking and exposure to radiation or other environmental substances were etiologies of CL/P. 15
A second common natural cause assumed as a risk factor for CL/P by the societies was genetic abnormalities. Such a belief was reported by four studies based on data from African countries (South Africa, Nigeria, Egypt, and Uganda) and two studies based on data from Asia (India and Philippines).6,12,13,15,16 In India, another belief that has received particular focus was that men or women who married their close relatives (consanguineous marriage) were more likely to have babies with a CL/P. 17
We also identified two studies that suggested accidents as a cause of CL/P. One study from South Africa assumed that nurses were responsible for CL/P, for whom they either accidentally cut the baby's lips or dropped the baby on the face, which eventually resulted in CL/P malformation. 12 Similarly, a study from the Philippines reported that the fetal forces associated with a mother falling might result in a baby being born with a CL/P. 18
Another important aspect of cultural beliefs of CL/P attributable causations, despite the advanced understanding of the natural world, was that people continue to report beliefs in supernatural phenomena. Indeed, population beliefs that CL/P occurred as a God's destiny were reported in South Africa, Nigeria, Zimbabwe, India, Kenya, Russia, Cambodia, Egypt, Peru, Uganda, and Ghana.7,12,15–18 This observation indicates that believing in God's destiny was culturally universal. Even though a CL/P child was perceived as the child of God in most studied societies, linking those children with bringing bad luck to societies was also common.
Another supernatural causation reported in association with CL/P was the ancestor spirit. This belief was informed by traditional healers around Gauteng Province-South Africa. 19 The healers said that a baby was born with a CL/P as a sign that an ancestral spirit thirsted for blood or was cursed by an ancestor. Society around the CL/P patients in Deesa town, Gujarat, India, perceived that CL/P was a curse from an evil. 6 Some factors were associated with this curse, such as parents’ sin, 15 gazing at the camel, practicing prostitution, 20 and looking at a child with a CL/P, 17 sins of past life, or destructive behavior. 21 Overall, it seems that societies often hold multiple causal beliefs simultaneously.
Response to the Birth of a Child with CL/P
Eight studies (Table 2) reported the reaction of societies toward children with CL/P and revealed that those babies were intentionally isolated, stigmatized, or left untreated. This was reported in India, Nigeria, Uganda, Zimbabwe, and Ghana.6,13–20,22 In Uganda, social rejection of the child with CL/P and ashamed feelings of the parents with their babies’ condition were common reactions. 13 Additionally, the babies born with a CL/P were not given a family name, but they were called “ajok” (female) or “ojok” (male), a local language that means “Satan”. 13 In Zimbabwe, patients with facial deformities and their mothers experienced social stigma, and because of that those mothers were found to cry over their baby's condition at the initial stages. The mothers also admitted to taking the baby to postnatal clinics and ensuring they covered the clefting area. 14
Rural Muslim and Hindu families in Gujarat in India and the upper Nile valley in Egypt believed that facial deformity was a punishment from God. Those families avoided surgeries because they were concerned that if the child's cleft was surgically treated, the further child would suffer the same defect, for interfering with God's will. 20 Likewise, in Nigeria, there was resistance to repairing facial cleft malformations because these defects were considered to serve as a protective function against the high newborn mortality rate. 15 Of note, in Hyderabad-India, a study found that the neighbors of CL/P individuals thought of them as bad luck and should be gotten rid of. Such a belief may directly threaten the patients’ lives. These highly adverse reactions toward CL/P patients were not constant as a belief that the CL/P was the “will of God (Allah)” encouraged some families in India and Egypt to accept the CL/P child and relieved the concern about the child's health and social life. 20
Management of CL/P
Of thirteen studies included in this review, only six mentioned the type of treatment CL/P patients received. Even though the patients had been surgically treated, traditional medications and other healing practices were also used. These traditional means of healing were widely practiced in Hindu and Muslim communities in India, for instance. In Hyderabad-India, parents treated the CL/P by burying the patients in sand up to the head and leaving them in direct sunlight for the entire day. 17
The rural area communities in India also used prayer and faith in God and applied a psychological approach, herbs, special diets, and other unique health practices to cure CL/P. 7 The treatments varied and depended on the healer and healthcare professionals consulted. 23 Although traditional healers in South Africa accepted that the patients should be medically treated, they still had to apply conventional medication/healing, considering Western doctors did not treat patients physically and mentally. 19 In Nigeria, the Hausa/Fulani ethnic group reported that the patients would be referred to the hospital by traditional healers after being given conventional treatments. 16
Discussion
This systematic review aimed to explore studies investigating cultural beliefs on causes, management, and reactions to the birth of children with CL/P worldwide. The results have demonstrated that belief about CL/P causation varies across countries, and societies often hold multiple causal beliefs simultaneously. Beliefs in natural causes, such as infection and genetic factors, and supernatural causes, like God's destiny, were almost culturally universal.14,15,18 Practicing spiritual interventions and traditional medication, leaving patients untreated, stigmatization or even infanticides were among commonly reported responses to CL/P patients.
A wide range of beliefs was found concerning the etiology of CL/P that in most countries are not grounded in empirical science. These beliefs, instead, are strongly influenced by sociocultural views. Culture itself, which is difficult to define, implies ideas, perceptions, and values that collectively constitute a way of life. It is unsurprising, therefore, that cultural values and worldviews substantially impact communities’ attitudes toward causal attributions and treatment of these deformities. Hammond-Tooke (1989) maintained that the definition of health issues in various ethnic groups was oriented toward traditions or folks’ models. 24 Of note, three paradigms are commonly held across all cultures to explain the causality of illness: naturalistic, personalistic, and emotionalistic. 25 The naturalistic theory attributes illness to loss of balance inside the body and is the most accepted theory in the Western world. Personalistic and emotionalistic theories which attribute disease occurrence, including CL/P, to supersitional power and feelings like anger or jealousy, respectively, are widely spread in low-income countries.
Since most of our studies were conducted in the middle- and low-income world, this might explain why we have found different cultural beliefs simultaneously in one setting; most were either personalistic and/or emotionalistic. In India, for example, some believed that CL/P happened because mothers saw the eclipse during pregnancy, and others mentioned that CL/P was a curse from a jealous person. 17 In Africa, mainly in Nigeria, some ethnic groups like the Yoruba attribute the etiology of the cleft to supernatural forces (evil spirits and ancestral spirits), while the will of God was believed to be the dominant cause of CL/P among the Hausa/Fulani groups. 16 Additionally, Patel et al. reported that some people from South Africa attributed the etiology of CL/P to mothers speaking harsh words. 12 Thus, governments or notable organizations should put more effort in encouraging the acceptance of naturalistic theory within middle- and lower-income countries.
Notably, Winkelman (2009) reported that families generally have little faith in scientific medical explanations and utterly rely on cultural views to define the causes and treatment of the illness. 26 Unfortunately, some of the cultural beliefs are misconceptions, conceive negative stigmas, and result in a “folks’ illness,” “imaginary disease,” or “psychosomatic illness” that affects patients’ well-being and quality of life. 27 One example concerning CL/P is that South African adult patients asked a priest why they had this kind of deformity, and the priest responded that it was because their parents were sinners. 12 Viewing this deformation as a punishment for a parent's sins could constitute a significant negative social and emotional well-being. Although most of the patients in the same study (16/20) expressed that the CL/P did not affect their social life, still, twelve patients still felt introverted, anxious, shy, sensitive, and moody.
It is well known that cultural belief affects conceptions concerning CL/P etiology and plays an important role in shaping ontological health systems. It is often reflected in varied methods; patients or their parents choose to treat this facial defect. Based on the Western medicine paradigm, the proper management of patients with CL/P is carried out by a multidisciplinary team involving maxillofacial surgeons, pediatricians, plastic surgeons, and others. Nonetheless, many populations in low-income countries still believe in Eastern medicine and tend to use prayers, faith, and traditional medicine to heal CL/P. 17 In contrast, we have seen in this review that most families from low-income countries consult traditional healers concurrently or prefer Western approaches. However, of particular interest, a study from Nigeria found that some families reported their referral to modern medical practitioners by traditional healers. 16 Likewise, two major religions in South Africa advise using Western medication. Still, they practice traditional healing during psychosocial consultation, using herbs as cures and attempting to treat patients through “supernatural powers.” This emphasizes the importance of collaboration between traditional healers and Western practitioners on culturally sensitive issues.
CL/P is usually associated with facial disfigurements, dental problems, difficulty in speech, hearing, feeding, and many other challenges. Such challenges result in various reactions from parents, families, friends, and whole societies towards these children. One of the shocking findings in this review was that a study reported a direct threat to the safety of children born with CL/P, and the main reason was the belief that those children brought bad luck to their entire communities and should be gotten rid of. 17
Another important reaction to the CL/P defect that needs great attention was leaving the child without treatment. 15 Some families believe that since the deformity was a gift from God, no intervention should be done. These observations, in particular, revealed how cultural beliefs may lead to very devastating consequences. Bullying, rejection, and social stigma have been found as common responses to CL/P patients, even at the time, from their families. Of note, a recent systematic review evaluated the impact of social stigma on a child with CL/P and found significant and remarkable negative outcomes. For example, some children drop out of education, could not reach their ideal employment, face economic burdens, and eventually lose productivity in their societies. 28
Globalization and immigration continue to increase and building societies with very diverse cultures becomes inevitable everywhere in this world. This diversity mandates the medical team responsible for the management of CL/P patients to consider these patients’ cultural backgrounds, mainly because the cultural perspectives may pose barriers to treating these patients appropriately. It is noteworthy that good cross-cultural awareness by all medical team members would improve communication and foster trust between CL/P patients and their families and the health care providers. The importance of this cross-cultural understanding by healthcare providers of their patient's backgrounds ultimately helps to create and deliver culturally competent services to all CL/P patients, irrespective of their ethnicity or race.
To overcome the misconceptions surrounding etiology and society's reactions toward CL/P patients, a wide range of communication approaches could be adopted in middle- and low-income countries. This was identified to be a highly relevant approach for vaccination programs lately, and a recent review described several approaches to accomplish this. 29 Some of these approaches should primarily be directed to the families, while others to health care workers. For example, health education to parents or mothers during home visits or antenatal clinic visits, flyers and posters in hospitals and clinics, and radio-, TV- or social media-based health promotion campaigns that explain the naturalistic theory about causes of CL/P could be important tools to improve the societal knowledge about CL/P. The engagement of traditional and religious leaders as advocates for these naturalistic theories would be another intervention that might work very well in these societies. Frequently providing brochures and fact sheets to healthcare providers to update and enrich their knowledge might facilitate and spur efforts to educate society and convey appropriate CL/P information.
This study should be understood in the context of some limitations, which may have introduced bias in our assessments. Firstly, some classical works presenting folk beliefs, myths, and historical perspectives of the causes were presented in a non-English language, and an English translation was not found. Therefore, the researchers found it difficult to explore its valuable information. Secondly, most studies included in this review were in rural areas with low socioeconomic status and little or no educational qualification. Thus, the samples relied on cultural and religious beliefs to determine the causes and treatment. These might be an undeniable cause of bias in the sources included. Due to more advanced access to media technology worldwide, people's perspectives within the research populations may have changed, even in rural areas. Hence, more explorations of the current perception, reaction, and treatment of CL/P should be undertaken.
Conclusion and Recommendation for Practice
Cultural belief about CL/P causation varies across countries, and societies often hold multiple causal beliefs simultaneously. While the naturalistic theory is attributed to the illness being accepted mainly by Western nations, personalistic and emotionalistic theories are shared among the populace of the low-income world. The reaction of families and societies to a child born with CL/P might lead to devastating consequences. A good cross-cultural understanding of patients’ and their families’ backgrounds will create a better opportunity to deliver culturally competent health services to all CL/P patients worldwide.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231209823 - Supplemental material for Cultural Beliefs on Cleft lip and/or Cleft Palate and Their Implications on Management: A Systematic Review
Supplemental material, sj-docx-1-cpc-10.1177_10556656231209823 for Cultural Beliefs on Cleft lip and/or Cleft Palate and Their Implications on Management: A Systematic Review by H. Hasanuddin, Aisha AH. Al-Jamaei, Ellen M. Van Cann, Muhammad Ruslin, Marco N. Helder, Prasannasrinivas Deshpande and Tymour Forouzanfar in The Cleft Palate Craniofacial Journal
Footnotes
Authors’ Contribution
All authors contributed to the study's conception and design. Conceptualization: H. Hasanuddin, Tymour Forouzanfar, Muhammad Ruslin, Ellen Van Cann; Study design: H. Hasanuddin, Tymour Forouzanfar, Muhammad Ruslin, Ellen Van Cann; Data acquisition: H. Hasanuddin, Aisha AH. Al-Jamaei, Tymour Forouzanfar. Quality data control: Ellen Van Cann, Muhammad Ruslin, Marco N. Helder; Data analysis and interpretation: H. Hasanuddin, Tymour Forouzanfar, Marco N. Helder; Manuscript preparation: H. Hasanuddin, Tymour Forouzanfar; Manuscript editing: Aisha AH. Al-Jamaei, Prasannasrinivas Deshpande; Manuscript review: Tymour Forouzanfar, Ellen Van Cann, Muhammad Ruslin, Marco N. Helder.
Funding
This study was partially supported by the Program 5000 Doctor-MORA Scholarship, the Ministry of Religious Affairs, Republic of Indonesia.
Data availability statement
The authors confirm that the data supporting the findings of this review are available within the article and its supplementary materials.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Keywords
To review cultural and religious beliefs, these keywords have been applied, culture, religion, cleft lip, cleft palate, perception, assumption, idea, and belief. Further, those mentioned keywords were formulated into some keywords formula using the Boolean operator “and” and “or”; Cleft- 42.255 articles, Cleft Lip 16.995 articles, Cleft Lip and Palate- 14.375 articles, Cleft Lip and Religion- 21 articles, Cleft Lip and Palate and Religion- 15 articles, Cleft Lip and Palate or Religion- 75.726 articles, Cleft Lip and Culture- 298 pieces, Cleft Lip or Culture- 973.954 articles, articles, Cleft Lip and Palate or Culture- 971.363 articles, Cleft Lip and Palate and Perspective- 269.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.