
Abstract
Objective
To examine linguistic disparities between English- and Spanish-speaking patients in access to care, satisfaction, and telehealth appointment attendance.
Design
Retrospective study recording demographics for non-attendance analysis and conducting phone surveys assessing satisfaction with telehealth.
Setting
Data was collected between March and December 2020 at the UCSF Craniofacial Center (CFC), a multidisciplinary pediatric clinic. Patients: English- and Spanish-speaking patients with a telehealth appointment. Interventions: The CFC offered language-concordant outreach, assistance with the telehealth platform, and interpreters at all telehealth appointments.
Main Outcome Measures
Demographics and patient-reported satisfaction with telehealth, barriers, and instruction clarity.
Results
Medicaid insurance was the only predictor of non-attendance. Surveys revealed that Spanish-speakers had 12.4 times the odds of lacking access to telehealth technology and 10.7 times the odds of needing help with logging on compared to English-speakers. There were no significant differences in satisfaction outcomes.
Conclusions
We attribute this equity in satisfaction to our language-concordant outreach efforts.
Introduction:
Telehealth has been widely adopted across pediatric specialties in the wake of the COVID-19 pandemic. However, studies have shown that telehealth exacerbates existing health disparities, often stemming from unequal utilization of technology due to socioeconomic and language barriers.1–3 Black patients and Spanish-speaking patients were less likely to access care through telehealth compared to White and English-preferring patients during the pandemic, especially if they lived in zip code with a lower mean income and higher average household size. 1 Additionally, Spanish-speaking patients were more likely to report technological challenges with accessing care through telehealth. 2 Studies have shown that the most common barriers to accessing telehealth include lack of technical literacy, availability of technology, and connectivity. 3 Despite these barriers, telehealth has the potential to reduce disparities to accessing health care by eliminating transportation costs for an in-person visit. 4
Given the rapid adoption of telehealth at our multidisciplinary Craniofacial Center (CFC) during the COVID-19 pandemic, we implemented several interventions to improve the care provided through the telehealth platform. Our center offered language-concordant outreach, assistance with the telehealth platform, and interpreters at all virtual appointments in an effort to mitigate health inequities stemming from the adoption of telehealth. Language-concordant outreach consisted of calling patients and explaining instructions on how to access the telehealth appointment in their preferred language. Additionally, providing language-concordant outreach allowed our center to identify patients who lacked access to necessary technology (internet access, tablet, computer) in order to invite them to clinic to attend a remote telehealth visit regardless of accessibility issues.
Here, we assess the efficacy of these interventions in reducing linguistic disparities between English-speaking and Spanish-speaking patients in access to care, experience, and telehealth appointment attendance at our multidisciplinary CFC and hypothesize that the implementation of these interventions will increase equity in patients’ satisfaction with telehealth.
Methods
This retrospective study identified all English- and Spanish-speaking pediatric patients at the University of California San Francisco (UCSF) CFC who had in-person or remote telehealth appointments between March and December 2020. If a patient did not have access to necessary technology or needed additional assistance logging on, they were invited to attend an in-person telehealth appointment at the center. Due to the multidisciplinary nature of our clinic, these visits can include a visit with a plastic surgeon, pediatrician, neurosurgeon, medical geneticist, oral maxillofacial surgeon, dentist, orthodontist, ophthalmologist, or otolaryngologist. Patients can have multiple appointments on the same day. For the non-attendance analysis, patients who did not attend at least one of these appointments were identified. Demographic information was extracted from the medical record.
For the patient-reported outcomes analysis, we performed a phone survey of all patients’ parents who did attend their appointments to record demographics and assess satisfaction, barriers to care, and understanding of instructions and provider's role. Survey questions addressed the following variables: highest level of education, if there was an audio/video interpreter present during the telehealth visit, if they received assistance setting up their telehealth visit, access to necessary technology, comfort with using the telehealth platform, understanding of the provider's role during their visit, confidence in the interpreter used, overall satisfaction with the telehealth visit, and understanding of next steps in their child's visit. Responses were collected based on a Likert scale rating system with 1 indicating “strongly disagree” and 5 indicating “strongly agree”. All surveys were conducted by a single member of our team who used a script and was also fluent in Spanish. Additionally, all surveys were conducted within 60 days of the patient's telehealth visit. These questions were selected to help us better assess what specific variables affect patients’ experiences of telehealth and how this may differ between English- and Spanish-speaking patients.
Univariate comparisons with Chi-squared testing with Benjamini-Hochberg adjustment and logistic LASSO regression were performed to identify significant predictors of each care outcome, with α=0.05. R version 3.6.3 was used for statistical analysis. This analysis was designated as a quality improvement initiative; thus IRB approval was not required at our institution. Patients provided verbal consent to participate in the phone survey and all patient responses were kept anonymous and confidential to protect patients’ privacy.
Results
During the study period, 114 patients did not attend at least one telehealth appointment out of a total of 452 patients (Table 1). Among patients who did not attend their telehealth appointment 24 (21.1%) preferred Spanish, and among patients who did attend their telehealth appointment, 47 (13.9%) preferred Spanish. Non-White race, Medicaid insurance, and Spanish language preference (p = 0.02, p < 0.001, and p < 0.001, respectively) were individually associated with non-attendance (Table 1). There were no statistically significant differences in attendance across income groups (p = 0.45). However, having Medicaid insurance was the only significant predictor of appointment non-attendance in the multiple logistic regression model with race, insurance, and language preference as predictors (Table 2).
Demographic Information of non-Attendance at Telehealth Appointments.
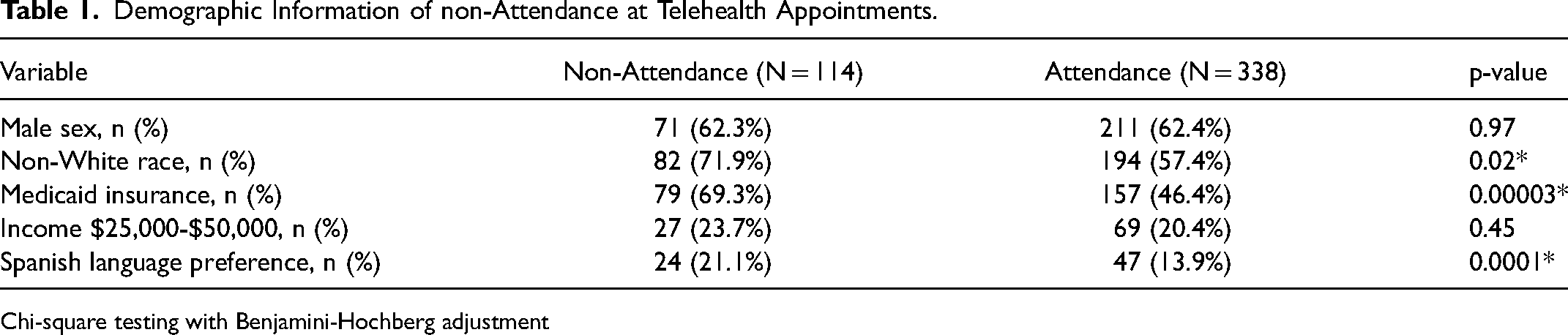
Chi-square testing with Benjamini-Hochberg adjustment
Predictors of Non-Attendance at Telehealth Appointments.
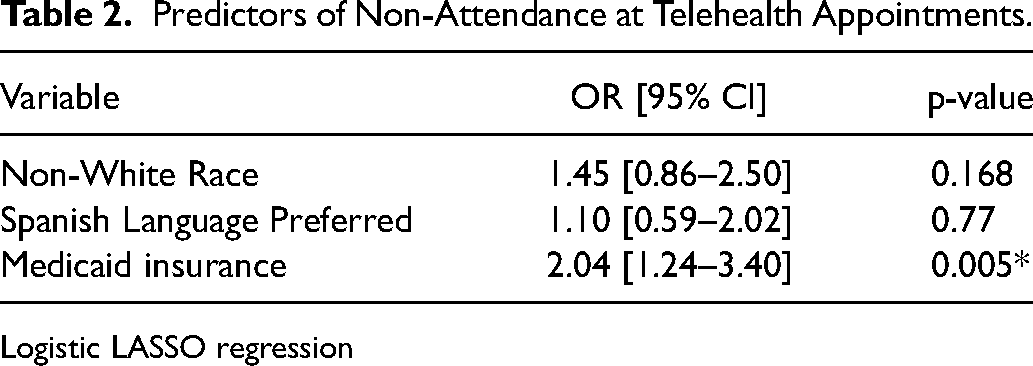
Logistic LASSO regression
Patient phone surveys (response rate 32%) revealed that Spanish-speaking families had 12.4 times the odds of lacking access to telehealth technology and 10.7 times the odds of needing help with logging into the video visit platform compared to English-speaking families (Table 3). Despite that, there were no significant differences across language groups in families knowing each multidisciplinary provider's role (p > 0.99), understanding the next steps after their visits (p = 0.44), or overall satisfaction with their telehealth visit (p = 0.30).
Barriers in Access to Telehealth.
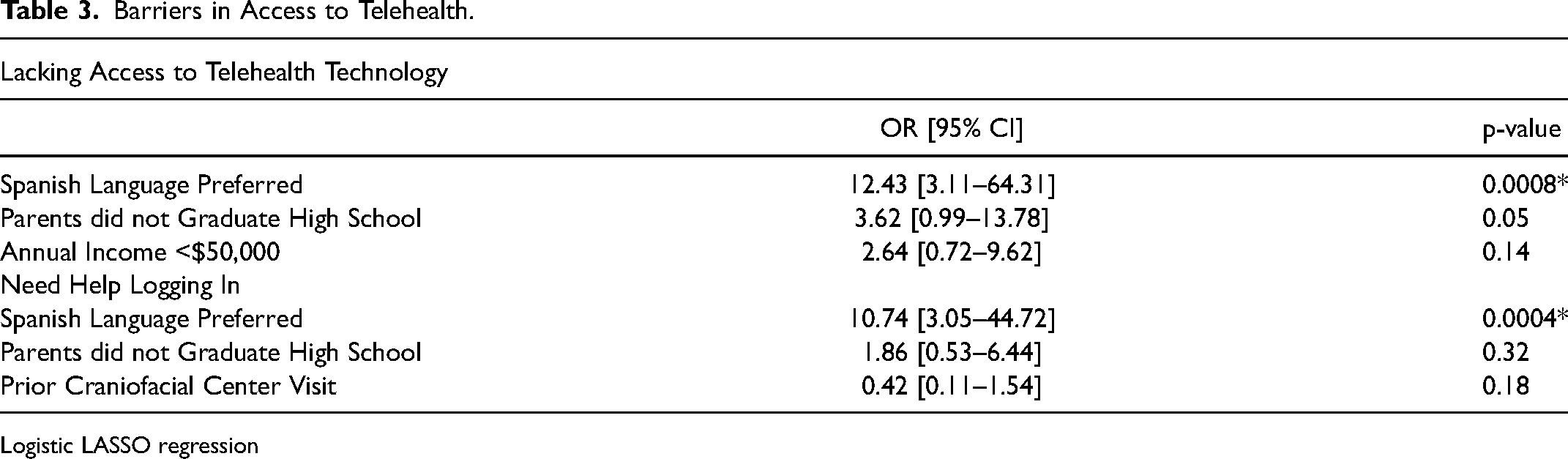
Logistic LASSO regression
Discussion
Despite increased telehealth non-attendance in patients with a Spanish language preference, having Medicaid insurance was the only predictor of appointment non-attendance. Additionally, Spanish-speaking families were more likely to lack access to telehealth technology but continued to have similar satisfaction outcomes. In contrast to prior studies, our analysis showed similar satisfaction outcomes among English-and Spanish-speaking patients following a telehealth visit. 5 This equity may be attributed to our language-concordant outreach efforts, which sought to address established barriers to care such as lack of digital literacy and providing language-concordant instructions for accessing the telehealth visit. 5 Our response rate was typical for patient surveys and likely did not affect the significance of the results. 6 to increase response rate, we made efforts to contact patients multiple times at different times of the day. Based on these results, the UCSF CFC will continue utilizing language-concordant outreach including asking patients about their preferred language, explaining how to access the telehealth appointment in their preferred language, and including interpreters during the visit to promote equity in telehealth appointments.2,7
Access to telehealth technology remains one of the greatest threats to telehealth equity. 3 This analysis was unique in that it captured patients who typically lack access to technology by conducting in-person telehealth visits, allowing us to better understand their satisfaction with telehealth, regardless of accessibility issues. 8 Since the CFC is a multidisciplinary pediatric clinic, the findings of this study likely apply broadly to other high-volume, multidisciplinary centers. Future work to refine telehealth practices that are patient-centered and ensure equitable access to care include utilizing local pediatrician clinics in a hub-and-spoke model as trialed in other healthcare settings such as the Veterans Health Administration to help reduce the barrier of technology inaccessibility. 9 To our knowledge, we are not aware if this model has been formally trialed in a pediatric population. Further efforts to refine telehealth practices in ways that are patient-centered and tailored to patients’ language preferences and access to technology are warranted to help ensure equitable access to telehealth for all patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Sciences, (grant number UCSF-CTSI Grant Number TL1 TR 001871).