
Abstract
Objective
To evaluate the applicability of transplanted teeth in young patients with craniofacial anomalies
Design
Observational study
Setting
Comprehensive Centre for Cleft Palate and Craniofacial Malformations
Patients/Participants
Patients with craniofacial anomalies who underwent tooth transplantation. Only children with complete clinical and radiological documentation and a follow-up period of at least 1.5 years were included.
Interventions
Tooth transplantation
Main Outcome Measure(s)
Retrospective evaluation of clinical records, pre- and postoperative radiographs, and operative charts. Clinical characteristics of patients, preoperative parameters and postoperative outcome parameters were collected.
Results
A total of 17 patients with 23 tooth transplantations were included. The median follow-up period was 6.7 years. The pooled survival and success rates were 91%. Notably, one out of two teeth that were transplanted into the bone grafted alveolar cleft site had to be extracted, which might indicating a higher risk for this procedure. In total, two transplanted teeth had to be extracted during the follow-up period, one due to external resorption and the other one due to perio-endo lesion. One patient needed endodontic treatment due to pulp necrosis.
Conclusion
We consider tooth transplantation to be a reliable and suitable procedure in the dental rehabilitation of young patients with craniofacial anomalies and fitting concomitant circumstances. We encourage craniofacial teams to reconsider this option more frequently in appropriate cases.
Introduction
Craniofacial anomalies are often associated with dental anomalies such as hypo-/oligodontia, displaced or supernumerary teeth and dental dysplasia.1-3 Dental rehabilitation is often complex and lengthy. This requires intensive and interdisciplinary treatment involving orthodontics, prosthodontics and oral and maxillofacial surgery. Dental implants are a common and reliable technique for replacing missing teeth. Numerous studies have shown excellent results of dental implants in adolescent patients. 4 However, due to the growth of patients, dental implants are not considered a suitable treatment option for young patients. 5 Of these, patients with craniofacial anomalies represent a particularly difficult group of patients. They need to be treated already at a young age and often the alveolar cleft requires bone grafting with iliac crest bone, which results in limited bone volume after finishing growth. Furthermore, combined dental and skeletal malocclusions require years of complex orthodontic tooth movements and, in some cases, also orthognathic surgery after growth completion. Hence, early occlusal rehabilitation is of great interest in this group of patients. In addition to orthodontic and/or prosthetic solutions, transplantation of teeth is a complementary treatment option for these challenging patients. Due to incomplete root formation and open apical foramen, transplantation in childhood has a good prognosis. Furthermore, the formation of functional periodontal ligament 6 is important, as it allows orthodontic movements 7 and alveolar crest growth. 8 Preserved pulp vitality and periodontium also allow intact proprioception. 9 Tooth transplantation is increasingly accepted in healthy patients with high levels of safety and success. 10 However, in contrast to traumatic tooth loss or single-tooth aplasia, patients with craniofacial anomalies often suffer from significant dental anomalies that are associated with dental and skeletal malocclusions and require elaborate orthodontic treatment. This makes dental rehabilitation and decision-making more complex. Due to the lack of available options, molar donor teeth and later stages of root formation as well as transplantation into the bone grafted site have to be applied more frequently in these patients. In addition, large orthodontic movements and difficult soft tissue conditions may have a negative impact on the outcome of tooth transplantation in craniofacial malformations. So far, there are not enough data in the literature on tooth transplantation in these patients. Existing evidence is scarce, as most reports are limited to personal experiences and case reports.11-16 Authors aimed to demonstrate the applicability of tooth transplantation for dental rehabilitation of young patients with craniofacial anomalies and to encourage craniofacial teams to reconsider this option more frequently in appropriate cases.
Material and Methods
Study Design and Data Collection
We searched our electronic database for patients with craniofacial anomalies who received tooth transplantation in our Centre for Cleft Palate and Craniofacial Malformations. Patient data were collected and pseudonymised from our electronic database and clinical records. Only children with complete clinical and radiological documentation were included. Other inclusion criteria were congenitally missing teeth and a follow-up period of at least 1.5 years. A follow-up period of less than one year may lead to an underestimation of complications and an overestimation of survival and success rates. 10
Patients who had an incomplete documentation or traumatic tooth loss as well as patients with congenitally missing teeth without an associated craniofacial anomaly were excluded. We retrospectively analysed clinical records, pre- and postoperative radiographs and operative charts. Clinical characteristics of patients, preoperative parameters and postoperative outcome parameters were collected. Stages of root formation were radiologically evaluated before transplantation according to Moorrees et al., as modified by Kristerson et al.17,18 Stage 1 (Ri), initial root formation; stage 2 (R1/4) one quarter root formation; stage 3 (R1/2), half root length; stage 4 (R3/4), three quarters root length; stage 5 (Rc), full root formation with open apical foramen; stage 6 (A1/2), full root formation with half-closed apical foramen; stage 7(Ac), full root formation with complete apical closure.
Postoperative radiographs were analysed regarding periodontal space, bone loss, sign of periapical, intra-, para-, or periradicular radiolucency, internal or external resorptions and pulp canal obliteration. The clinical data collection comprised dental pain and sensibility testing using carbon dioxide snow (CO2), tooth mobility, probing depths, signs of inflammation, pain and sound of percussion.
This study was carried out in accordance with the ethical standards and recommendations of the institutional ethics committee (407/2021BO2), and with the principles stated in the Declaration of Helsinki 1975, as revised in 2013.
Treatment Protocol
All patients in our centre are discussed by a multidisciplinary team, taking into account orthodontic and prosthetic treatment options. In this context, the necessity of a tooth transplantation is also carefully considered. Important criteria for decision-making are age of patient, skeletal and dento-alveolar relations, number and location of missing teeth, persistence and quality of deciduous teeth, availability and maturity of a possible donor tooth. In case of tooth transplantation, the height and width of alveolar bone and the available dental arch space must be carefully evaluated and correlated with the root length and dental crown of the potential donor tooth. The appropriate time for transplantation depends on dental root formation. Stages of root formation were radiologically evaluated before transplantation according to Moorrees et al., as modified by Kristerson et al.17,18
Surgery was performed in either general (GA) or local anaesthesia (LA). First, the donor tooth had to be harvested. In the case of a third molar, the germ to be transplanted was carefully freed from the covering bone after osteotomy. All donor teeth were luxated and removed very carefully to protect the periodontium and apex. The length and transverse-oval diameter of the root was measured for correct preparation of the recipient site. The donor teeth were then immediately stored in the natural socket to protect the cells on the surface. No primary endodontic treatment was performed. The recipient site was prepared by crestal incision and elevation of a full thickness mucoperiosteal flap. If necessary, the persisting deciduous tooth had to be removed at the recipient site. According to the previously measured dimensions, a socket was prepared in the recipient site using a drill from dental implants with suitable diameter and length. The transverse-oval diameter was achieved by additional use of surgical round burrs. Subsequently, the donor tooth was placed into the prepared socket in mild infra-position to avoid occlusal interference. Finally, mucoperiosteal flap was reattached by suturing. The grafted tooth was fixed with semi-rigid adhesive titanium-trauma-splint (TTS) or sutures. Clinical and radiological follow-up as well as the duration of splinting were determined individually. Patients received oral hygiene instructions including daily rinsing with chlorhexidine and a soft diet was followed. Perioperative antibiotic prophylaxis was not given.
Data Analysis
Due to the heterogeneity of the patients and the small sample size, statistical analyses are considered inappropriate. Descriptive statistics were performed using SPSS Version 24.0 (IBM, Armonk, NY). The results are provided as absolute values [median (range)] and percentage.
Results
Patient Characteristics (Table 1)
We included 17 patients (29% female, 71% male) in this retrospective study, the majority (n = 12, 71%) suffering from cleft lip and palate (CLP). In total, 23 tooth transplantations were performed in these patients. All but one surgical procedure was performed in general anaesthesia (transplant no. 3, local anaesthesia). All patients were operated by one highly experienced surgeon. The median age at surgery was 12.9 years (9.7-23.9 years). We transplanted 11 (48%) lower premolars, 8 (35%) upper third molars, 3 (13%) upper premolars and 1 (4%) supernumerary lower first molar. 17 teeth (74%) were transplanted to the maxilla, most of them in the premolar region (n = 14, 61%), but also in the incisor region (n = 3, 13%). The recipient sites in the mandible were the premolar (n = 5, 22%) and molar region (n = 1, 4%). Notably, in two patients with CLP, teeth were transplanted into the bone grafted site after alveolar bone grafting with cancellous bone from the iliac crest. In another 2 patients, vertical augmentation of the recipient site with onlay autogenous corticocancellous iliac crest grafts was performed prior to tooth transplantation. The interval between augmentation and transplantation was 2-4 months. Stages of root formation were radiologically evaluated before transplantation. The preferred stage of root formation was stage 4 (R3/4) (n = 11, 48%). However, also stage 3 (R1/2) (n = 5, 22%) and stage 5 (RC) (n = 7, 30%) were transplanted. Most transplanted teeth were fixed by titanium-trauma-splint (TTS) (n = 14, 61%). The median duration of splinting was 19 days (10-26 days).
Patient Characteristics.
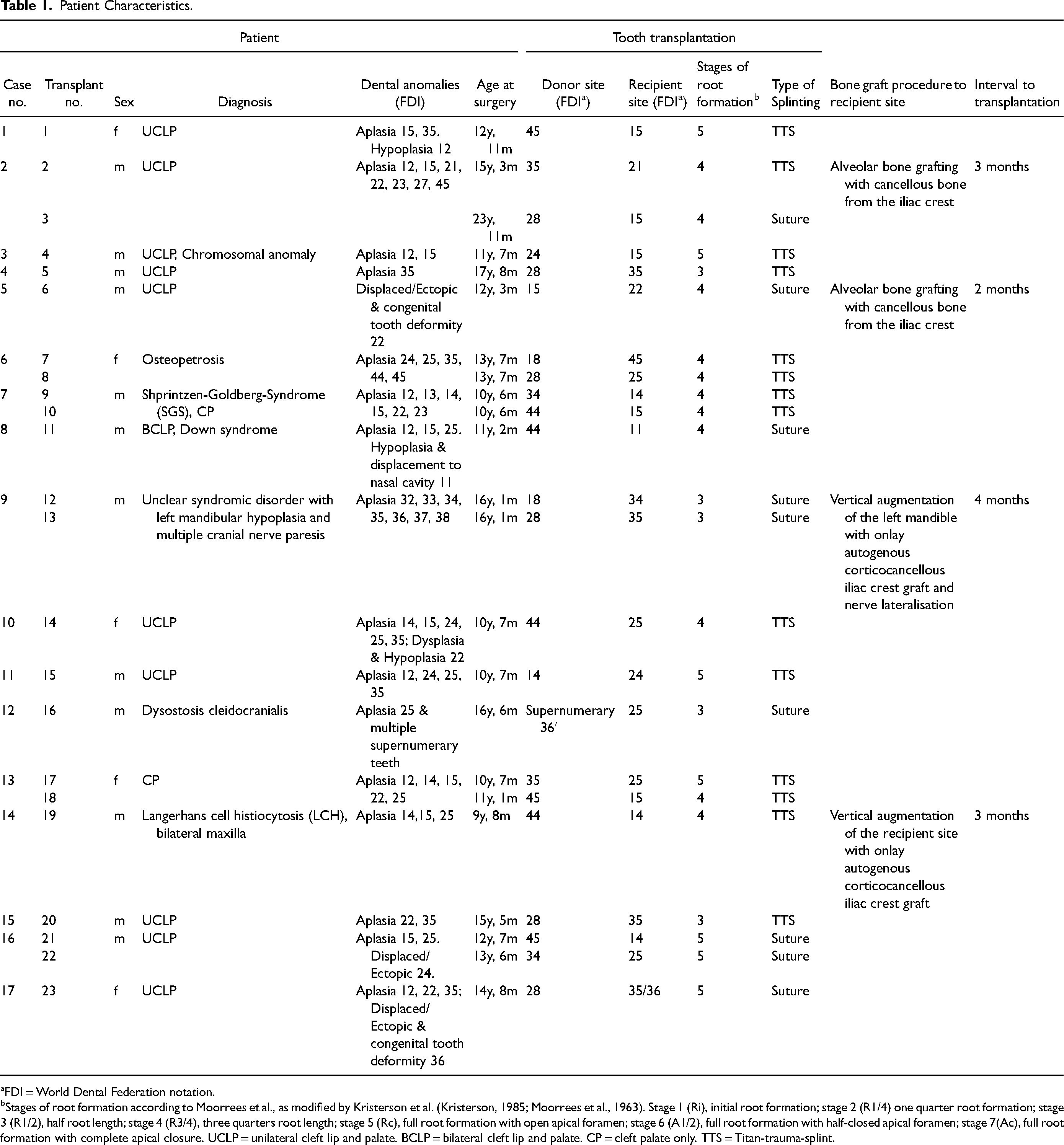
FDI = World Dental Federation notation.
Stages of root formation according to Moorrees et al., as modified by Kristerson et al. (Kristerson, 1985; Moorrees et al., 1963). Stage 1 (Ri), initial root formation; stage 2 (R1/4) one quarter root formation; stage 3 (R1/2), half root length; stage 4 (R3/4), three quarters root length; stage 5 (Rc), full root formation with open apical foramen; stage 6 (A1/2), full root formation with half-closed apical foramen; stage 7(Ac), full root formation with complete apical closure. UCLP = unilateral cleft lip and palate. BCLP = bilateral cleft lip and palate. CP = cleft palate only. TTS = Titan-trauma-splint.
Clinical Follow-up (Table 2)
The median follow-up period was 6.7 years (1.7-12.9 years). Looking at a heterogeneous group of patients (eg, tooth types, recipient site), the pooled survival rate of all included cases was 91%. Notably, one out of two teeth that were transplanted into the bone grafted alveolar cleft site had to be extracted. In total, two transplanted teeth had to be extracted during the follow-up period. In one patient with CLP (case no. 5) the transplanted upper premolar had to be extracted after 27 months due to external resorption after transplantation into the bone grafted site with cancellous bone from the iliac crest. In case no. 15 the patient consulted us because of increasing mobility of the transplanted tooth. Clinical examination showed pathological tooth mobility and probing depth (8 mm distal), as well as negative sensibility testing using carbon dioxide snow (CO2). Radiological examination revealed a perio-endo lesion with extended distal osteolysis. Consequently, the transplanted upper third molar had to be extracted after 34 months.
Clinical Follow-up.
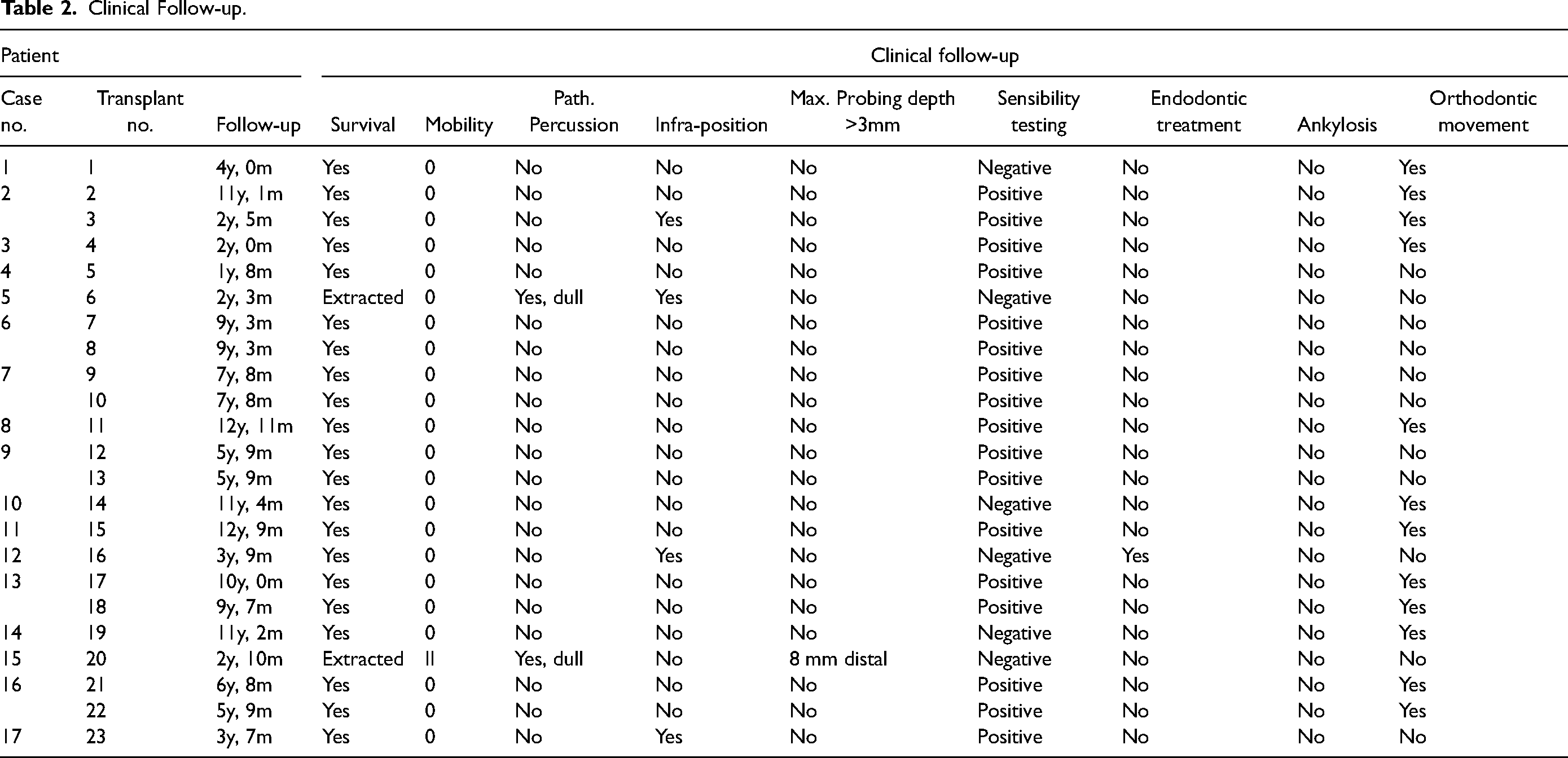
All other teeth (n = 21, 91%) showed good clinical follow-up without pathological percussion, tooth mobility or probing depths. There was a good healing with periodontal reattachment. In our data no ankylosis occurred. Sensibility testing using CO2 was positive in 81% (17/21) and negative or unclear in 19% (4/21). However, only one patient (no. 12) needed root canal treatment due to pulp necrosis 17 months after transplantation. Further follow-up (in total 45 months) was uneventful, and the tooth could be retained even after root canal treatment. 3 teeth (14%) were still in slight infraposition and showed no occlusal contact. Orthodontic tooth movement was performed in about half of the transplanted and survived teeth (12/21, 52%).
Radiological Follow-up (Table 3)
One tooth (4%) showed no root development, apexification or pulp canal obliteration after transplantation. The same tooth was extracted later due to external resorption (case no. 5). Of the two other teeth without apexification, one tooth later required root canal treatment (case no. 12). The other tooth (case no. 13) in addition showed no pulp canal obliteration. However, sensibility testing using CO2 was positive and the tooth remained clinically inconspicuous over a follow-up period of 10 years.
Radiological Follow-up.
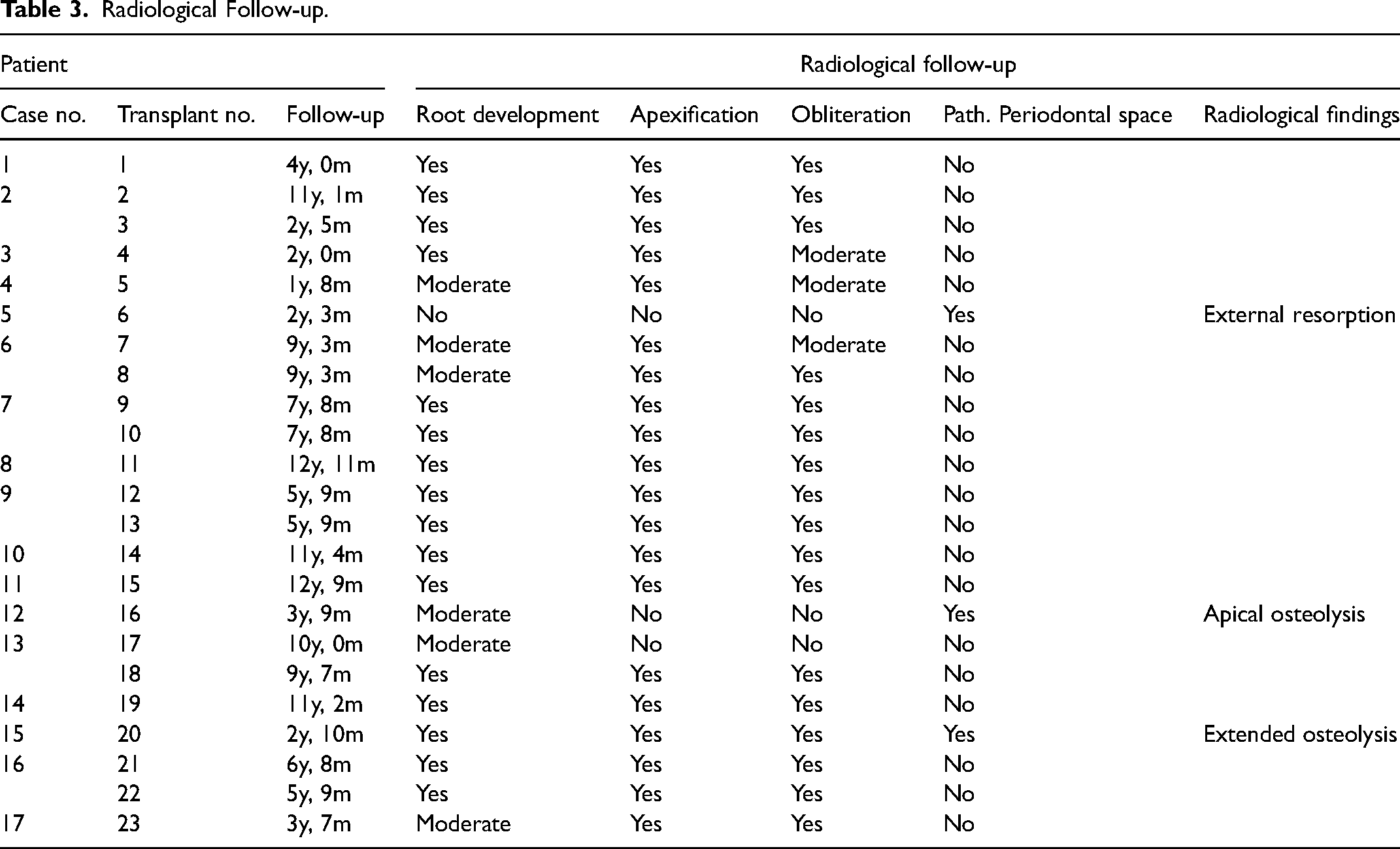
As already shown, case no.5 radiologically showed an external resorption at the grafted upper premolar, which had to be extracted 27 months after transplantation. Case no. 12 underwent root canal treatment after radiological signs of apical osteolysis and case no. 15 showed extended distal osteolysis due to perio-endo lesion.
Discussion
Tooth transplantation is increasingly accepted in healthy patients with high levels of safety and success. 10 The prognosis and success of tooth autotransplantation in patients in general may be valid for patients with craniofacial anomalies as well. We demonstrated that tooth transplantation is also applicable for dental rehabilitation of complex patients with craniofacial anomalies who often suffer from significant dental anomalies. This requires an intensive and interdisciplinary treatment involving orthodontics, prosthetics, and oral and maxillofacial surgery. Combined dental and skeletal malocclusions require years of complex orthodontic tooth movements. Formation of a functional periodontal ligament 6 is one great advantage of transplanted teeth allowing movements by orthodontic forces 7 and alveolar crest growth. 8 This enables the preservation of alveolar bone volume and formation of dental arch. However, patients with severe oligodontia also benefit from early occlusal rehabilitation in terms of self-esteem and oral health-related quality of life (OHRQoL). 5 Preserved pulp vitality and intact proprioception in transplanted teeth 9 may also contribute to OHRQoL in affected children. Anyway, so far there are limited data in the literature on tooth transplantation in patients with craniofacial anomalies. Existing evidence is scarce, as most reports are limited to personal experiences and case reports.11-16 As aforementioned, due to the lack of available options dental rehabilitation and decision-making is more complex in patients with craniofacial malformations. Resorting more frequently to molar donor teeth, later stages of root formation, transplantation into the bone grafted site, or large orthodontic tooth movements and difficult soft tissue conditions may have a negative impact on the outcome of tooth transplantation in craniofacial malformations. We were able to report on a cohort of 17 patients with craniofacial anomalies who underwent 23 tooth transplantations as part of oral rehabilitation. Also, of great importance in the context of our retrospective evaluation is the complete and long-term follow-up period, with a median follow-up of 6.7 years.
In the literature, high survival rates have been reported in non-malformation patients. In their comprehensive review, Almpani and colleagues calculated a pooled need for extraction of 7.8%, 9 which is consistent with our results of 8.7% with a median follow-up of 6.7 years. The stage of root development proved to be a consistent factor negatively affecting survival rate and complications such as ankylosis, pulp necrosis and root resorption, which were less likely in teeth with open apex. 9 When transplanting 100 premolars at different stages of root development, Kristerson et al. concluded stage 3 and 4 to be the preferred stages for donor teeth, whereas stages 5 and 6 were associated with a considerable risk of pulp necrosis and root resorption. 18 In a recent publication, authors attempted to improve outcome of mature transplants by extraoral root-end resection. 19 In our patients, teeth in the later stages of development also had to be transplanted as part of the complex treatment concept. Although a conclusive statement is only possible to a limited extent due to the comparatively small number of cases, there was no adverse effect for teeth in stages 5 in our cohort. None of the teeth that developed complications were at stage 5 (external resorption = stage 4, pulp necrosis and perio-endo lesion = stage3).
If only teeth with incomplete root formation are considered, the reported results are even better. Reviewing the current literature of immature teeth, Rohof et al. 10 calculated an annual weighted estimated survival rate of 98.2%, success rate of 96.6%, and complication rates in terms of ankylosis 2.0%, root resorption 2.9%, and pulp necrosis 3.3%.
Concerning ankylosis, it is known from dental trauma that extraoral time correlates with the risk of ankylosis. 20 In tooth transplantations, higher rates up to 11% were reported. However, it can be assumed that the inclusion of mature molars favoured these high rates. 21 In our procedure we stored the donor teeth in the natural socket to protect the cells on the surface. In our data no ankylosis was observed.
Available rates for root resorption also vary widely.10,22 Reasons for progressive root resorption are damaged periodontal ligament or pulp infection. In our cohort, in one patient with CLP (4%) the transplanted upper premolar had to be extracted after 27 months due to external resorption. Tooth transplantation into the area grafted with cancellous bone from the iliac crest may have contributed to root resorption. It should be noted that there are few data on tooth transplantation to the bone-grafted alveolar cleft site. Hillerup et al. reported 4 cases. Endodontic treatment was performed in all cases but one, and one also showed external resorption. 23 Later Hamamoto and colleagues published two cases, both teeth underwent endodontic treatment 3 weeks after transplantation as part of the protocol. Both teeth survived without root resorption after 12 and 20 months, respectively. 16 More recently, Aizenbud et al. reported four cleft affected patients with transplantation of mandibular premolars (stage 3-4) to the bone-grafted alveolar cleft site. No endodontic treatment and no adverse events were reported. 24
Due to the paucity of data, little is known about the correct timing of tooth transplantation after secondary bone grafting to the alveolar cleft. However, data indicate that the correct time interval is crucial. In their animal study, Stenvik et al. transplanted 14 teeth in 4 monkeys. In the cases where the transplantation was performed simultaneously with an autologous bone graft, extensive root resorption as well as ankylosis and loss of the transplanted teeth occurred on a large extent. On the other hand, good outcome was observed in teeth after delayed transplantation, 4 months after bone grafting. 25 It is known that cancellous alveolar bone graft is replaced by newly formed bone within 6 months. 26 However, histological findings indicate an ongoing active remodelling for another 6 months which is completed 12 months after grafting. On the other hand, grafted bone seems to undergo resorption in the absence of occlusal load. The authors therefore concluded that tooth transplantation should be performed soon after the formation of the bone bridge is confirmed, when bone remodelling is still underway. 16 Hillerup et al. 23 and Stenvik et al. 25 described a minimum of a 4 month interval between bone grafting and tooth transplantation. In our cohort in two patients with CLP, teeth were transplanted into the bone grafted site after cleft alveolar bone grafting with cancellous bone from the iliac crest and in another two patients, vertical augmentation of the recipient site with onlay autogenous corticocancellous iliac crest grafts was performed prior to tooth transplantation. Notably, one of two teeth that were transplanted into the bone grafted alveolar cleft site had to be extracted, indicating a higher risk for this procedure. However, from a retrospective point of view, the teeth in our cohort were transplanted comparatively early after augmentation (2-4 months). This might be a reason for the external resorption and loss of the tooth in case no. 5, which was transplanted 2 months after alveolar bone grafting. Nonetheless, many centers, including us, prefer spontaneous tooth eruption of the canine into the bone-grafted alveolar cleft site or in case of a persisting tooth gap the use of an adhesive bridge rather than tooth transplantation into this area.
The evaluation of pulp vitality may be challenging. Sensibility testing using carbon dioxide snow (CO2) is one evaluation option. Other factor indicating pulp vitality are pulp obliteration as well as root development and apexification. According to Aizenbud et al. 24 and Kristerson 18 all teeth with pulp revascularization show various degrees of pulp obliteration which increase with the observation period. In our cohort only three teeth showed no pulp obliteration. One tooth was extracted later due to external resorption and another one required endodontic treatment. The third tooth showed an uneventful 10-year follow-up with positive sensibility testing using CO2 and initial root development.
There are large differences in the rates of pulp necrosis in the literature, 0-34% of immature teeth, and 85-100% of teeth with mature root formation.18,19,27,28 However, as stated by Rohof et al. 10 the presence of pulp necrosis does not necessarily imply tooth failure or non-success, especially when endodontic treatment is sufficient. In our cohort, one patient (case no. 12, transplanted supernumerary 36′) had a pulp necrosis diagnosed 17 months after transplantation. After sufficient root canal treatment, further follow-up (45 months) was uneventful, and the tooth could be retained. It is assumed that the narrow and frequently multiple apical foramina apices impair revascularisation of transplanted molars.18,19,27 Also, multiple roots and complex root anatomy complicate harvesting molars. Consequently, prognosis of transplanted molars is known to be worse. 10 Lower premolars are the preferred donor teeth, especially in cases of maxillary retrognathia, such as in patients with clefts. However, especially in patients with complex craniofacial anomalies who often suffer from significant oligodontia, dentoalveolar compensation is not possible and appropriate donor teeth are missing. Hence, in these cases, molars must be considered more frequently, at the expense of an increased risk. In our cohort 8 (35%) upper third molars and 1 (4%) supernumerary lower first molar had to be transplanted. As aforementioned, one upper third molar had to be extracted (case no. 15) and one lower first molar required root canal treatment.
Limitations of the Study
The limitations of the present study include the retrospective study design, heterogeneity of the patients (eg, tooth types, recipient site) and the small sample size. Therefore, statistical analyses were considered inappropriate. Looking at a heterogeneous group of patients the pooled survival rate of all included cases was calculated. It is important to emphasize that lower rates were reported when looking at different subgroups. Although a conclusive statement is only possible to a limited extent due to the small number of cases in the subgroups, transplanting into the bone grafted alveolar cleft site (1/2) and transplantation of upper third molar (1/8) can be challenging procedures that might be associated with a higher risk. However, the heterogeneity of the data also reflects the complexity and difficult decision-making in the cases, which more often required unusual and individual solutions. Compared to the existing literature, we were able to include a large number of transplanted teeth (n = 23), despite the studied rare conditions. Also, of great importance in the context of our retrospective evaluation is the complete and long-term follow-up period, with a median follow-up of 6.7 years. It has been shown that most failures were observed within the first year after transplantation and that survival rates remain constant during a follow-up period of 10 years. 10 However, complications such as ankylosis can occur up to 2 years postoperatively. 29 In our patient, pulp necrosis was observed 17 months postoperatively. Studies with short follow-ups may lead to an underestimation of complications and an overestimation of survival and success rates. 10 For this reason, official guidelines for the minimum period of reported follow-up for transplanted teeth would be desirable.
Conclusion
With the advent, widespread and successful use of dental implants tooth transplantation has lost its broad application. However, the technique of tooth transplantation has various advantages. It is accepted in non-malformation patients with high levels of safety and success. Patients with craniofacial anomalies often suffer from significant dental anomalies that require intensive and interdisciplinary treatment already at a young age. Especially the need for dental rehabilitation in young age, when dental implants are not feasible, is the major advantage of tooth transplantation. Despite challenging conditions, the present cases series has shown favourable results. Therefore, we consider tooth transplantation to be a reliable and suitable procedure for dental rehabilitation of young patients with craniofacial anomalies. This work aims to encourage craniofacial teams to reconsider this option more frequently in appropriate cases.
Footnotes
Acknowledgements
Affiliated departments of this publication are members of the European Reference Network (ERN) for craniofacial anomalies and ear, nose and throat disorders.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.