
Abstract
Objective
To determine the prevalence of treatment of early childhood caries (ECC) using general anesthesia (GA) in children with cleft lip and/or palate (CL/P).
Design
Retrospective chart review of children followed by the Manitoba Cleft Lip and Palate Program (MCLPP) to determine the frequency of treatment for ECC under GA.
Setting
Children's Hospital, Winnipeg, Canada (a tertiary care centre).
Patients
Children registered with MCLPP between January 1, 2008- December 31, 2019.
Interventions
The chart review collected data on the following variables: sex, date of birth, postal code, type of cleft, whether child had treatment of ECC using GA, age at the time of GA, and cost of treatment.
Main outcome measures
Association of CL/P with ECC.
Results
Overall, 441 children had CL/P. 17% had isolated cleft lip (CL), 46% had isolated cleft palate (CP), and 37% had both cleft lip and palate (CLP). Overall, 24.3% of children with CL/P underwent dental surgery using GA while 14.5% underwent dental surgery to treat ECC between 12-59 months of age. When compared to a reference of Canadian healthy children 12-59 months of age, a child with CL/P was 15 times more likely to require GA to treat ECC.
Conclusion
Treatment for caries under GA in children with CL/P is common. In the children with CL/P the rates of GA for treatment of ECC are significantly higher when compared to the general population. Children with CL/P require comprehensive oral health prevention to reduce the risk for caries and the need for treatment under GA.
Introduction
Every year, approximately 500 children are born with orofacial clefts in Canada. 1 Those affected require multidisciplinary surgical and non-surgical care from birth until adulthood. Without information on which to base primary preventive strategies, orofacial clefts continue to pose a major challenge to affected individuals, their families and society. 2
Clefts of the lip and/or palate (C/LP) are recognizable disruptions of the normal facial structure. While not a major cause of mortality in developed countries, CL/P does cause considerable morbidity to affected children and imposes significant financial strains for families with an associated societal burden. 3 CL/P are among the most prevalent congenital malformations of the orofacial structures and constitute approximately 65% of anomalies affecting the head and neck. 4 The occurrence of CL/P is influenced by complex genetic and environmental factors. While the prevalence of oral clefts varies with different ethnic backgrounds, international literature reports epidemiological indices of CL/P ranging from 0.87 to 1.03 per 1000 live births. 5 The prevalence at birth of CL/P in Canada from 1998-2007 was 0.94 per 1000 and of isolated cleft palate (CP) 0.70 per 1000. 2
Dental caries is a global public health problem and constitutes to be one of the main threats to children's oral health.6–8 Early caries experience and premature loss of primary teeth due to caries in children with CL/P can affect the success of surgical treatment, orthodontic treatment, and speech therapy. 5 A healthy primary dentition with avoidance of early extractions is crucial in order to preserve space and bone adjacent to the alveolar cleft. Patency between the oral and nasal region compromises feeding, breathing, and causes the most significant morbidity in patients. Oronasal patency is also thought to disrupt the normal oral flora at a time when the teeth are erupting. Prolonged bottle-feeding to ensure adequate nutrition as well as the challenges of maintaining oral hygiene secondary to abnormal teeth and the cleft itself, have been proposed to contribute to the increase in caries incidence in these children. 9
Slow oral food clearance times, the presence of enamel defects, high mutans streptococci and lactobacilli counts, and deficient oral hygiene practices have been reported to be contributing factors for caries in CL/P patients. 10 Several case-control studies have reported that toddlers and preschool children with orofacial clefts have higher caries increments than similarly aged non-cleft control children.11–14 These studies found that 20%—75% of patients with CL/P harbor caries, depending on the populations studied.12–14 Likewise, the decayed-missing-filled teeth scores (dmft) for patients with CL/P 6 years old and younger are noted to range from 1.3 to 9.95 teeth in several epidemiological studies. 11 By contrast, other studies have found no difference in caries risk in patients with non-syndromic CL/P, or a lower caries risk, when compared to the general population.8,15
Early childhood caries (ECC) describes tooth decay in the primary dentition in children <72 months of age. 16 A 2016 study reported that the overall rate of dental surgery to treat ECC was 12.1 per 1000 children 12-59 months of age in Canada. 17 When children with orofacial clefts develop ECC, the health and longevity of the primary dentition and the success of future cleft care interventions can be jeopardized. Severe forms of ECC (S-ECC) must be treated aggressively to prevent declines in oral function and cosmetic outcomes, as well as to promote optimal surgical outcomes in the future. 11
Age-appropriate behavior patterns coupled with an extensive history of orally focused surgery and examination can make patients with CL/P orally defensive. This behavior pattern can limit the ability to perform restorative and surgical dental procedures without sedation or general anesthesia (GA). Moderate and deep forms of sedation, as defined by the AAPD, 18 may be contraindicated for these patients. This is because head and neck anomalies could jeopardize resuscitation efforts in a medical emergency. For these patients, dental surgery using GA is a common option for treatment of ECC. 11
There is little information on the oral health status of children with oral clefts in Canada. The oral health needs vary considerably, and the clinical management of orofacial anomalies involves considerable resources. In Manitoba, the costs for dental restorations and orthodontic treatment are covered by the Manitoba Cleft Lip and Palate Program (MCLPP) up to the year in which the patient reaches their 25th birthday. In order to be accepted into the program, the patient needs to be a resident of Manitoba, maintain a good oral hygiene regimen at home, and present at least once a year to a dentist for an oral health exam and assessment.
There is significant literature reporting on the etiological factors for CL/P. In addition, much is written on the outcomes of patients with CL/P relating to the surgical interventions that the patients undergo. However, the current literature on both the incidence of CL/P, as well as knowledge on caries prevalence in Canadian children with CL/P is sparse. In the light of the global decline in caries in children, 19 it is important to evaluate the incidence of CL/P, along with the current burden of caries among these children. The primary objective of this study was to determine the prevalence of treatment of caries using GA in children with CL/P, and to examine the burden of caries among these children followed at Winnipeg's Children's Hospital between January 1, 2008 and December 31, 2019. A secondary objective was to determine the rate for children with CL/P requiring a GA for the treatment of ECC.
Methods
This study was approved by the University of Manitoba's Health Research Ethics Board and Children's Hospital in Winnipeg, Canada. Data were obtained from a retrospective chart review of children followed by the Manitoba Cleft Lip and Palate Program (MCLPP) to determine the frequency of treatment for ECC under GA.
Children born in the province of Manitoba with confirmed orofacial clefting are registered at birth (children can also be registered on relocation to Manitoba) through the MCLPP and are periodically followed by the craniofacial team, which includes the Children's Hospital Dental Clinic at Winnipeg's Health Sciences Centre.
Inclusion criteria for the retrospective chart review included children registered with the MCLPP between January 1, 2008 and December 31, 2019. Children in the MCLPP presenting with an underlying syndrome or significant medical history were also included. Children who were stillborn, did not survive beyond the perinatal period, or relocated outside the province of Manitoba were excluded.
The following variables of interest were retrieved through a direct search of MCLPP registry, MCLPP billing records, the craniofacial team charts, and electronic patient dental charts in the Dentrix software (Henry Schein One, American Fork, Utah) used by the Children's Hospital Dental Clinic: sex, date of birth, postal code, type of orofacial clefting (ie, isolated cleft lip (CL), isolated cleft palate (CP), cleft lip and palate (CLP)), presence of a syndrome, and whether GA was required to treat ECC. All relevant findings from each initial and periodic comprehensive exam were noted. Data were entered into a REDCap database without any patient identifiers. For children who were treated for caries under GA, the following additional information was collected: oral hygiene status (good, fair, poor, unknown) prior to treatment under GA, age at the time of GA, cost of treatment, and the type of treatment rendered. For children who underwent subsequent GA's for treatment of caries, the initial visit was used to calculate age at GA, however the cumulative treatment required, and cumulative cost was recorded. Cumulative scores of decayed, extracted, and filled primary teeth (dmft) were also calculated from the post-operative report after treatment was rendered. All data were collected by the principal investigator (FS). Imputation using substitution of mean age at time of surgery was used for those children with missing age information at the time of surgery.
Data were analyzed using standard descriptive (eg, frequencies, means ± standard deviations (SD)) and bivariate statistics (chi square, t test) using NCSS and SPSS. Odds ratios (OR) and 95% confidence intervals (CI) were calculated. A recent national report on the treatment of ECC using GA in Canada reported that the average rate was 12.1/1000 children age 12-59 months. 17 For this CL/P cohort, we performed a subgroup analysis for children 12-59 months to determine their rate of dental surgery and compare it against the Canadian average of 12.1/1000. In order to do this, data were expressed as rates per 1000 using population health data for this age group in Manitoba. Rates were also calculated for those with CL/P, those with CL/P with any medical comorbidity, and those with CL/P with a syndrome. Proportion chi-square testing was performed to compare rates between children with CL/P and the Canadian average and between otherwise healthy children with CL/P and those with an associated syndrome. A p value ≤ 0.05 was significant.
Results
The retrospective chart review of the MCLPP identified that total of 441 children with a diagnosis of CL/P during the time period of interest with 52.8% being males. Overall, 17% had an isolated cleft lip (CL), 46% had an isolated cleft palate (CP), and 37% had both a cleft lip and a cleft palate (CLP). Additional characteristics of these children appear in Table 1. Analysis of the first 3 digits of the postal code for participants revealed that 49.1% resided in urban Manitoba, 34.4% in rural Manitoba, 2.2% were from the Northwest Territories, and 5.0% were from Northern Ontario. Postal code data were missing for 9.3% of participants.
Demographic Characteristics of the Anonymized Data for Children Registered with Manitoba Cleft Lip and Palate Program (MCLPP) Between January 1, 2008 – December 31, 2019. (Note: Values Obtained from MCLPP Anonymized Data set.).

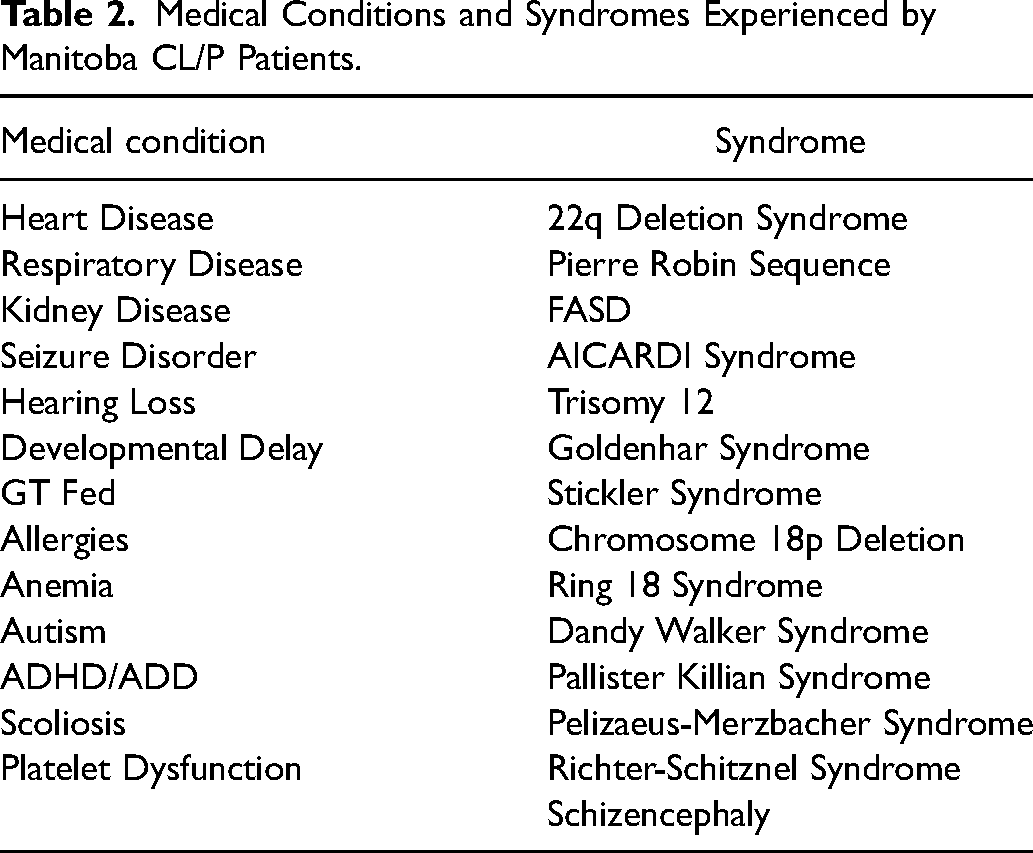
Approximately 10% of patients with a CL/P also presented with one or more additional medical comorbidity. Of the patients with an additional comorbidity, over 40% expressed a syndrome associated with their CL/P; translating to approximately 4.5% of the total population with CL/P in Manitoba having an associated syndrome. Table 2 reports a list of associated medical conditions and syndromes expressed in the Manitoba population with CL/P. There were a total of 14 different syndromes (Table 2) with 18 children having at least one syndrome.
Medical Conditions and Syndromes Experienced by Manitoba CL/P Patients.
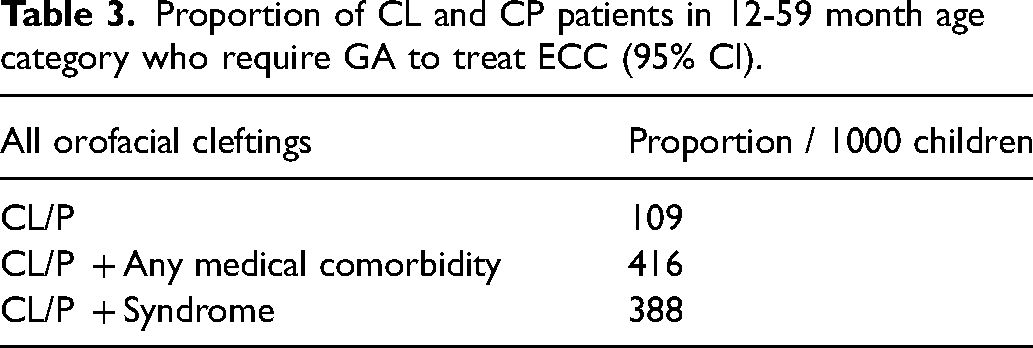
Proportion of CL and CP patients in 12-59 month age category who require GA to treat ECC (95% CI).
Overall, 107 of children underwent dental treatment using GA, accounting for 24.3% of the cohort of children followed by the MCLPP (Table 1). The average age of the 107 patients requiring dental treatment under GA was 48.5 ± 18.9 months. Types and location of clefting for these children appears in Table 1. Among the 107 requiring treatment under GA, the mean dmft was 9.8 ± 5.8. The majority received extractions (64.5%) and stainless steel crowns (78.5%). There was no significant difference in dmft scores between children with and without a syndrome (10.4 ± 4.5 vs. 9.7 ± 5.9, P = .72).
Of the cohort described in this study, approximately 1/4 required treatment under GA for ECC, of which we had the age on surgery date for 86 patients. In order to compare the treatment of ECC under GA amongst children followed by the MCLPP with the Canadian average, we then restricted further analysis to those 12-59 months of age. A total of 64 of these patients were in the age range of 12-59 months (Figure 1). The types and locations of clefting for these children also appears in Table 1. The mean dmft was 12.2 ± 4.0, with the majority receiving extractions (82.8%) and stainless steel crowns (98.4%). Again, there was no significant difference scores between those with and without a syndrome (10.8 ± 3.4 vs. 12.3 ± 4.1, P = .38).
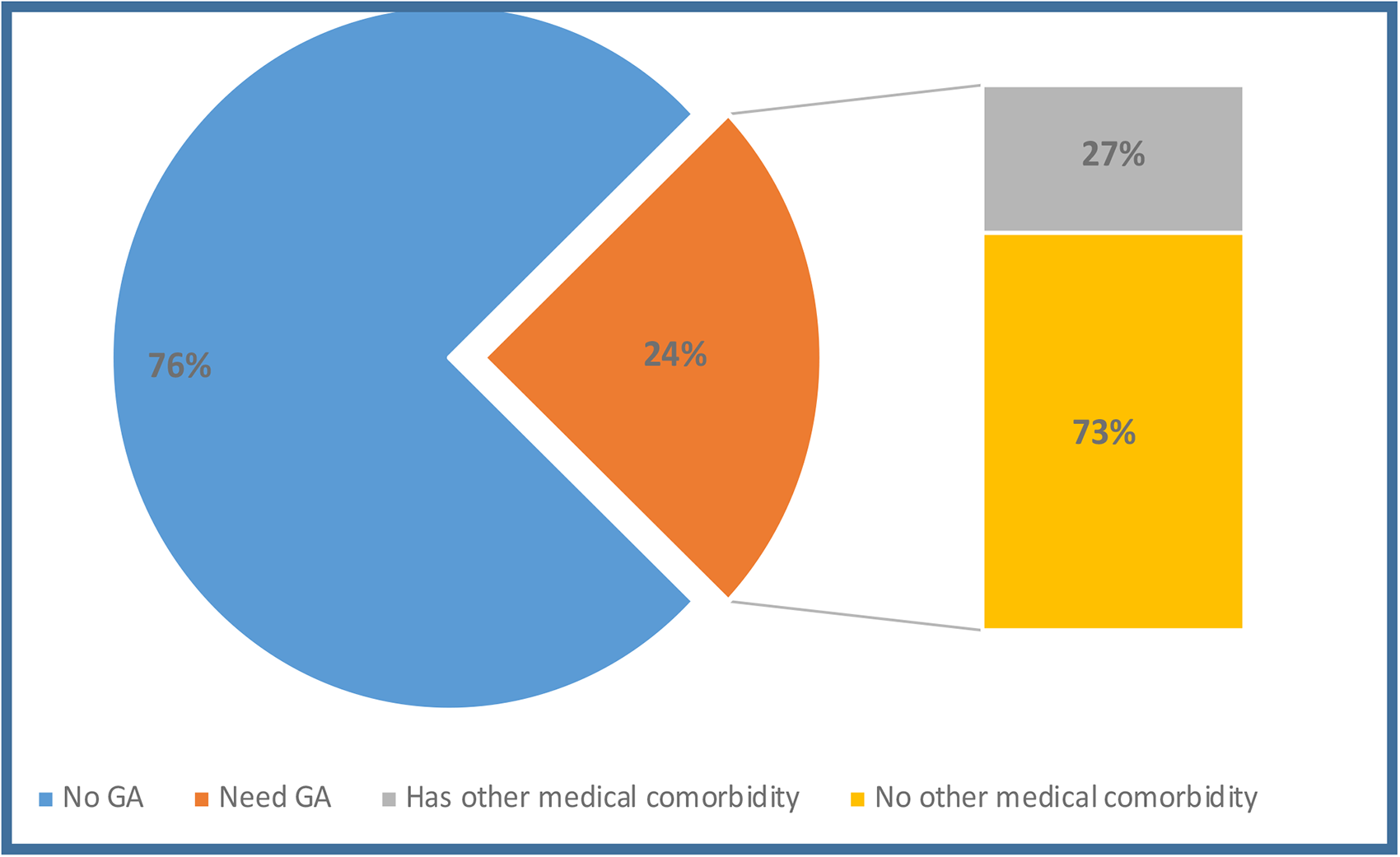
Percentage of children requiring GA to treat ECC, including those with additional medical comorbidities and syndromes.
For those patients whose age at surgery data was missing, we imputed the number that would have been in the same age range at the time of their surgery, assuming a similar age distribution as the patients for which we did have an age on surgery date. Thus, we estimated a total of 84 children that required GA to treat ECC in the age range of 12-59 months. The groups were then broken down into (1) All CL/P children requiring GA, (2) Otherwise healthy CL/P children requiring GA, (3) CL/P children with any additional medical comorbidity requiring GA, and (4) CL/P children with associated syndrome requiring GA. The proportion of patients with CL/P between 12-59 months age who required GA to treat ECC) were converted to rates per 1000 with a 95% confidence interval (Table 3). The rates to treat ECC for children with CL/P was 109/1000 children while the rate to treat ECC for children with CL/P with diagnosis of a syndrome was 388/1000. To test whether the rate of GA for ECC in children with CL/P between 12-59 months of age was different from the rate of GA for ECC in the general Canadian population (12.1/10 000), as well as to test whether the rates of GA for patients with CL/P who are otherwise healthy to the population with CL/P who have an associated syndrome, in Canada in the same age range, we used the proportion chi-squared test. A child with any form of CL/P, including those who are syndromic or present with additional medical comorbidities between 12-59 months were 15 times more likely to require GA to treat their ECC than a healthy child (the test statistic on the z scale was 34.1, P < .0001). A patient with CL/P who had an associated syndrome was 32 times more likely to require GA to treat ECC than their aged matched healthy counterparts, and 3.5 times more likely to require GA to treat ECC than a patient with CL/P who is otherwise healthy (The test statistic on the z scale was 3.5, P < .001).
Finally, The cost of the dental treatment under GA ranged from $687.10 to $4158.00 with an average of $2474 ± 817per child (Table 1). The decayed, missing, and filled (dmft) primary teeth score was calculated from operative reports. The average dmft score of patients after their GA was reported to be 11.8 ± 5.0 (extractions 4.4 ± 2.1, stainless steel crowns 7.2 ± 3.1, amalgam restorations 2.5 ± 0.4, composite restorations 2.9 ± 0.9, sealants 1.8 ± 0.2) (Figure 2).
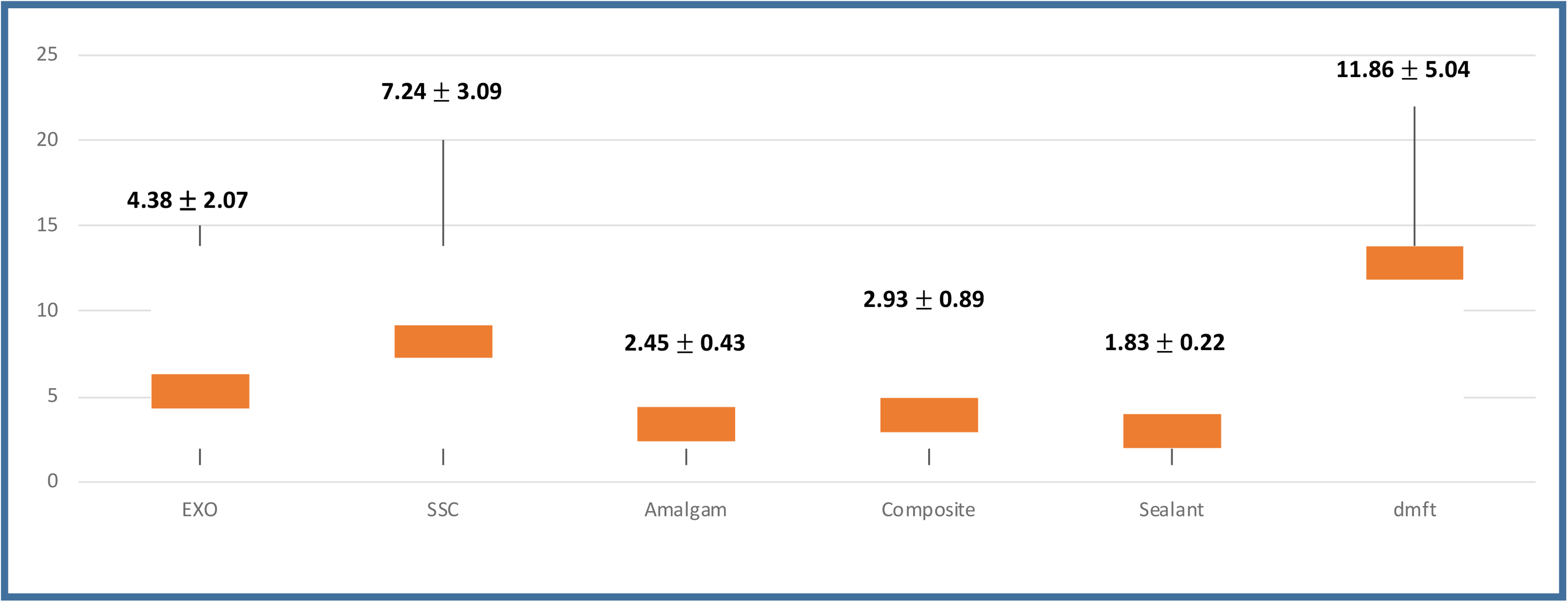
Average scores for extractions (EXO), stainless steel crowns (SSC), amalgam restorations, composite restorations, sealants and dmft (decayed, missing, filled tooth) score.
Discussion
The goal of this retrospective study was to update the epidemiological data on patients with CL/P in Manitoba. Orofacial clefting has a significant impact on both the patient and the family. Patients with CL/P utilize a higher prevalence of health care resources over their lives. In a publicly funded health care system as we have in Canada, the birth prevalence could influence both economic and resource planning for centers that attend to the needs of the population with CL/P. 20
While the birth prevalence of CL/P in Manitoba has been relatively stable from 2008-2019, the trend has increased from 2 per 1000 live births in the period of 1948-1977 to 2.46 per 1000 live births currently. The reason for this increase was outside the scope of this study, but we postulate that due to advanced medical interventions, more children with orofacial clefting are surviving beyond the perinatal period. It is also possible that the increase could be attributed to a growing Indigenous population who make up approximately 18% of the population in Manitoba versus the Canadian provincial average of 4.9%, 21 who are estimated to have up to 3 times higher rate or orofacial clefting than the non-Indigenous population. 22
A general consensus in CL/P literature is that males are more frequently affected with CL, or CLP (2:1) with an inverse seen in isolated CP (0.5:1). 23 Previous research by Matthews et al. indicated that there was an increase female prevalence for CP in Manitoba, however our study did not find this. While the rates of CL, or CL and CP in our study were higher (1.14:1, 52.8% vs. 46.2%) in males, the ratio of isolated CP was almost 1:1.
In Canada, there has been a reportedly stable incidence of orofacial clefting within the last few decades, despite efforts to reduce known risk factors such as increasing perinatal folate intake, encouraging peripartum smoking cessation and earlier and more accurate prenatal screening. It is unclear if other factors such as sociodemographic (rural vs urban households or socioeconomic status), maternal health history or prenatal care are greater influencers than previously suggested. 24 In this study, we did find that 49.1% of our population were from an urban community and 41.6% were from rural communities in Manitoba, Northwest Territories, and Northern Ontario.
Approximately 1 in 25 infants are born with a congenital anomaly in Canada. 21 Our study found that 4.5% of the population with CL/P in Manitoba had an associated syndrome. In developed countries such as Canada, individuals with congenital anomalies are surviving to a much older age than in previous decades, or in developing countries. 21 A recent study demonstrated that the mortality rate for children with orofacial clefting is higher during first 2 years of life, particularly in children who present with a congenital or chromosomal anomalies within the first 30 days of life. 24
Children with ECC often require oral rehabilitation under GA, which is the most frequent hospital day surgery procedure for preschool children in Canada. 17 The average age of patients with CL/P requiring treatment of ECC under GA between the age of 12-59 months was 39.4 ± 8.9 months with a dmft score of 12.2 ± 4.0. Extraction of primary teeth and stainless steel crowns were prevalent among the preschool group of children in our study. Due to the aggressive nature of ECC and a desire to avoid requiring retreatment for dental caries under GA, therapeutic intervention under GA should be definitive. This often dictates a more aggressive treatment approach and the judicious use of stainless-steel crowns (SSC's). 25 It appears that once a decision has been made to treat a child under GA for ECC, the level of treatment rendered is likely similar between CL/P and non-CL/P children. This present study revealed that there were no significant differences in dmft scores between otherwise healthy children with CL/P and those with syndrome. This is interesting considering that CL/P children with syndromes had a rate of treatment of ECC under GA 3.6 times greater than otherwise healthy children with CL/P. It also reveals that children with CL/P who had syndromes also had a high caries burden and were not just treated under GA for convenience.
According to the AAPD, “Children with known risk factors for severe ECC should have care provided by a practitioner who has the training and expertise to manage both the child and the disease process. Severe dental infections may result in medical emergency requiring hospitalization, antibiotics, and extraction of the offending tooth”. 18 Extracting teeth in a cleft site during the preadolescent period can result in widened cleft widths and reduced bone volume before alveolar bone grafting is completed. In addition, soft tissue remodeling can also be problematic as oronasal fistulae can become patent or increase in size after tooth extraction. 11
The cost of treating ECC using GA in a hospital setting are significant, with an average hospital associated cost of $1564 17 and an average dental treatment associated cost of $2474. This of course excludes the travel cost and other costs borne by the family. In Manitoba, both the hospital associated, and dental caries associated costs of treating CL/P patients are borne by the provincial health care system. Given that the hospital costs alone for dental day surgery to treat ECC in Canada exceed 21 million annually, more appropriate and sustained funding should be dedicated towards establishing effective preventive strategies for ECC. 17 A recent study demonstrated that providing parents of children with CL/P with counseling on caries prevention has been shown to reduce caries rates in children. 26
Limitations of this study would be the nature of retrospective study design including incomplete data collection and limited variables to consider for inclusion in the study. A challenge in the research of CL/P epidemiology is how stillbirth, neonatal death and terminations should be counted, whether children with associated congenital anomalies should be considered separately, how to categorize clefts, and how to account for variations in prenatal diagnosis and pregnancy termination. 20 The frequency of repeat dental surgery for treatment in ECC were not considered, nor were children who underwent treatment for ECC under GA in combination with other procedures. In Manitoba, dental data collection for patients born with CL/P is not collected in a systematic manner. Secondly, accuracy of initial diagnosis and consistency in reporting were lacking. Finally, there was also an inability to collect data on ethnic and cultural classifications, use of prenatal care, parental involvement in dental care, miscarriages, or therapeutic abortions with orofacial clefts.
In the absence of information on which to base primary preventive strategies, CL/P continue to pose a major challenge to the affected individuals, their families, and society. This study provides updated information relating to the oral health of children with CL/P who are followed by the MCLPP in Manitoba. It also provides new data regarding the caries burden experienced by these children. Further research should also focus on developing a system to ensure higher quality data collection. Further research could focus on looking at why the prevalence is higher in Manitoba when compared to the rest of Canada. 22 If a racial, environmental or genetic difference can be identified, further etiological studies can be conducted. This could also guide studies directed at intervention and prevention of orofacial clefting.
Conclusion
Rehabilitative dental treatment to address caries under GA in children with CL/P is common in Manitoba, with the majority requiring extraction and stainless steel crowns. In the children with CL/P the rates of GA for treatment of ECC are significantly higher when compared to the general population. When taking into consideration patients who have an associated medical comorbidity or an associated syndrome, the rates of GA increase 34-fold. Children with CL/P require comprehensive oral health prevention beginning at an early age to reduce the risk for caries and the need for treatment under GA.
Footnotes
Acknowledgements
Operating funds were provided by the Dr. Gerald Niznick College of Dentistry Endowment Fund. At the time of this study, Dr. Schroth was a Canadian Institute of Health Research Embedded Clinician Researcher in “improving access to care and oral health service delivery for young children in Manitoba”.
Anonymized Text
This study was approved by the University of Manitoba's Health Research Ethics Board and Children's Hospital in Winnipeg, Canada. Data were obtained from a retrospective chart review was undertaken of children followed by the Manitoba Cleft Lip and Palate Program (MCLPP) to determine the frequency of treatment for ECC under GA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.