
Abstract
Ankyloblepharon filiforme adnatum (AFA) is a rare, benign congenital anomaly. Notably, it is characterized by the adhesion of the ciliary edges of the upper and lower eyelids at the trabecular line. AFA is usually a solitary malformation of sporadic occurrence; however, it can occur in conjunction with other congenital diseases. Herein, we report a case of cleft lip with AFA. A patient was referred to the ophthalmology department of our hospital. The ophthalmic diagnosis was AFA in both the eyes. The left eye was observed to have a fibrous adhesion in the center, and she underwent surgery to excise the fibrous adhesion of tissue with scissors. The right eye was observed to have a fibrous adhesion in the external canthus and was excised during lip plasty. After surgery, her eyes were able to fully open, and no other apparent disease was diagnosed. AFA is thought to be caused by an ectodermal-derived developmental abnormality. Notably, cases of AFA with a cleft lip are rare. Diagnosis and surgery should be performed promptly to minimize any risk of amblyopia and for the early detection of congenital diseases, including glaucoma.
Introduction
Ankyloblepharon filiforme adnatum (AFA) is a rare congenital anomaly characterized by the partial or complete adhesion of the ciliary body margins of the upper and lower eyelids to a fibrous adhesion. 1 There are few reports of AFA with a cleft lip and palate.2–8 There have been 55 reports of AFA in Japan and abroad, 9 and it is said that AFA often occurs alone. 10 However, congenital heart disease (patent ductus arteriosus and ventricular septal defect), 11 syndromes, such as syncytial finger 12 and imperforate anus, 13 18-trisomy,11,14 and Hay-Well syndrome15–17 have also been reported to present with AFA. To the best of our knowledge, there are only 7 reports of AFA in patients with cleft lip and palate only; however, cases with only cleft lip have not been reported. In this study, we report a case of only cleft lip with AFA.
Case
A newborn girl infant was born at 39 weeks of gestation by vaginal birth. The birth weight was 3555 g. Family history was unremarkable. A cleft lip was observed, and the patient was referred to our department at the age of 6 days. An initial examination revealed a left-side incomplete cleft lip and alveolar cleft (Figure 1).

Preliminary findings; a left-sided incomplete cleft lip was revealed.
The left eyelid was suspected to be closed and the patient was examined by our ophthalmology department. Fibrous adhesions were observed in the middle and external canthus of the left eye and in the external canthus of the right eye. The fibrous adhesions in the external canthus of both the eyes were attached only to the upper and lower eyelids and were not continuous with the external canthus (Figure 2). The cornea of the right eye was transparent, the pupil was round, and there was no obvious iris abnormality. In the left eye, the eyelid opening was restricted by fibrous adhesions, making the examination difficult.
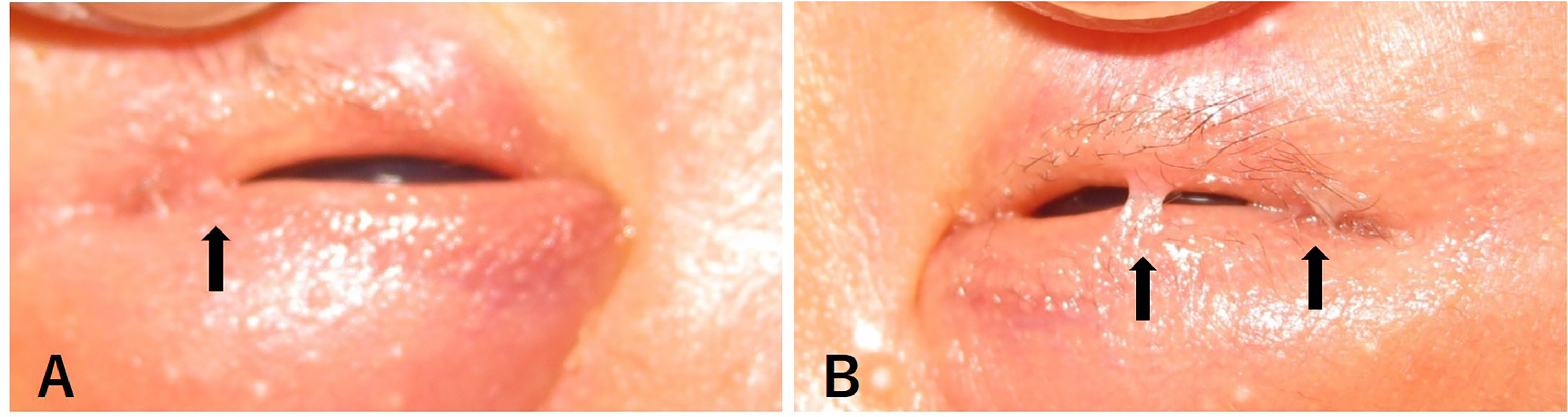
Preliminary findings of ophthalmology. (A) There were fibrous adhesions in the external canthus of the right eye. (B) There were fibrous adhesions in the middle and external canthus of the left eye.
The presence of these multiple morphological abnormalities, including cleft lip, indicated a suspicion of some syndrome, and a chromosome analysis was performed. However, no chromosomal abnormalities were observed. There were no pediatric problems, and the diagnosis was cleft lip only with AFA.
In the left eye, the fibrous adhesion in the center of the eyelid caused severe restriction while opening the eyelid; additionally, early treatment was considered desirable because of concerns about developmental problems. At the outpatient clinic of the ophthalmology department at the age of 9 days, the 2 fibrous adhesions connecting the left eyelids were separated with a shear knife for eyelid adhesion dissection. The cornea of the left eye was transparent, the pupil was round with no difference between the right and left eyes, and no obvious iris abnormality was observed (Figure 3). Postoperatively, the restriction of eyelid opening of the left eye was relieved (Figure 4).

The eyelid adhesion dissection of the left eye at the age of 9 days. There was oozing hemorrhage from the detached fibrous adhesions.

Postoperative eye surgery; the restriction of eyelid opening in the left eye was relieved.
At the age of 4 months, lip plasty was performed under general anesthesia. At the same time, eyelid adhesion dissection was performed on the external canthus of both the eyes. As in the previous case, the fibrous adhesions in the external canthus of both eyes were excised with a shear knife. The postoperative course was good and there were no restrictions on eyelid opening; additionally, it was confirmed that there was no difference in the eyelid shape or visual acuity between the left and right eyelids at 3 months after surgery (Figure 5). The patient is now 2 years old and has no obvious visual impairment or other ocular lesions.

At 3 months after surgery; there was no difference in the eyelid shape or visual acuity between the left and right eyelids.
Discussion
AFA consists of partial or complete fusion of eyelid margins. 1 The pathological findings of the fibrous adhesions that attach to the upper and lower eyelids have been reported to be surrounded by stratified squamous epithelium with blood vessels in the center. 18 In our case, the fibrous adhesions were only detached and could not be submitted for pathological examination. However, we observed oozing hemorrhage from the detached fibrous adhesions, suggesting that the fibrous adhesions contained blood vessels.
The eyelid originates from the neural crest cells of the head. 10 The eyelid develops as folds of the skin above and below the cup at the sixth week of gestation, covering the anterior surface of the cornea. At 12 weeks' gestation, only the epithelial layers of the upper and lower eyelids come into contact with each other, and the eyelid epithelium adheres to the eyelid suture, which separates at 21 to 24 weeks' gestation. 19 AFA is caused by abnormal interaction between the eyelid epithelium and mesenchymal tissue, resulting in the abnormal proliferation of the mesenchymal tissue or temporary cessation of epithelial growth, without separation.10,20,21
The incidence of AFA is estimated to be 4.4 per 100,000 live births.
1
AFA occurs alone in most cases.
10
Few cases were associated with complications. Complications reported in the past include 18-trisomy,11,14 Hay-Well syndrome,14–17 CHAMNDS syndrome,
22
pterygopalatine syndrome,
23
congenital heart diseases, patent ductus arteriosus, ventricular septal defect,
23
bilateral syndactyly,
23
anorectal atresia,
23
bilateral patellar patellae,
12
parapapillary,
12
cryptorchidism,
12
spinal meningocele,
13
hydrocephalus,
13
and anal prolapse.
13
Glaucoma has also been reported to be associated with AFA; additionally, the possibility of congenital glaucoma due to abnormal neural crest cell differentiation during development has been pointed out.
10
Therefore, it is necessary to keep the development of glaucoma in mind after AFA treatment and to carefully monitor the patient.
We found 7 cases of AFA associated with cleft lip and palate, as far as we could confirm (Table 1).2–8 All of them were cases of cleft lip and palate. Additionally, there were no reports of cases with cleft lip only, such as the present case.
Reports of AFA With Only Cleft Lip and Palate.
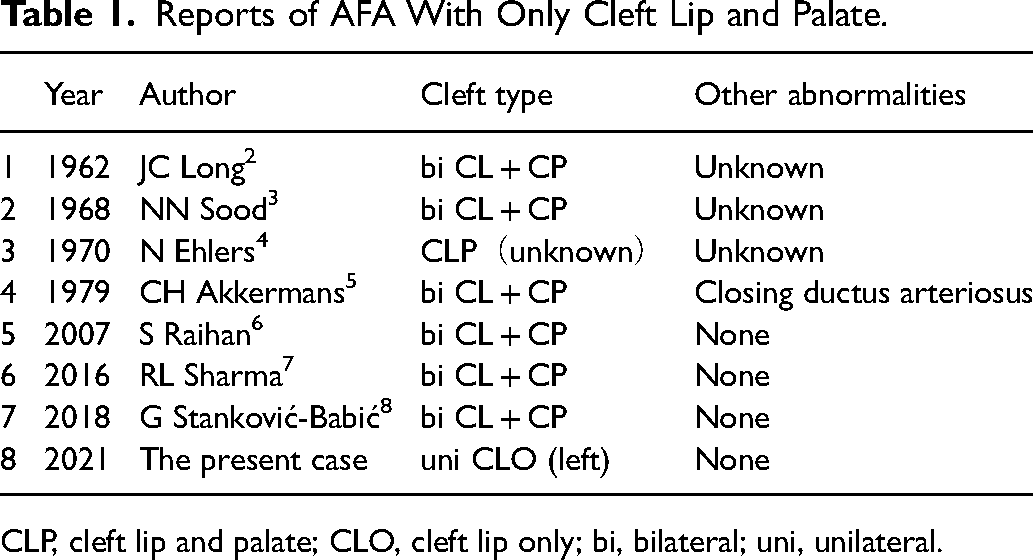
CLP, cleft lip and palate; CLO, cleft lip only; bi, bilateral; uni, unilateral.
The basic treatment of AFA is surgery; the fibrous adhesions are dissected out using a shear knife and scalpels. 24 The fibrous adhesions that remain at the edge of the eyelid after excision usually shrink and disappear. 25 Because the visual function develops immediately after birth and eyelid restriction associated with AFA may impair the development of visual function, treatment should be performed early in life.7,24 In our case, the AFA of the left eye, which was associated with significant eyelid restriction, was treated at the age of 9 days; further, the remaining AFA was treated at the age of 4 months with lip plasty and eyelid dissection. After that, no developmental disturbance in the vision was noted, and the patient was doing well.
Conclusion
AFA is a congenital anomaly of the face, including cleft lip and palate. Additionally, an early diagnosis and surgery are effective for early detection of congenital complications, including glaucoma and prevention of secondary complications, such as amblyopia. It seemed necessary to examine, bearing in mind that AFA is a congenital anomaly of the facial region, including cleft lip and palate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.