
Abstract
Objective
Determine if the ideal location of the construct in microtia reconstruction for hemifacial microsomia (HFM) can be more accurately derived from measurements on the cranium.
Design
High-resolution computerized tomography (CT) images were analyzed through craniometric linear relationships.
Setting
Our tertiary care institution from 2000 to 2021.
Patients/Participants
Patients diagnosed with HFM and microtia, who had high-resolution craniofacial CT scans, yielding 36 patients accounting for 44 CT scans.
Main Outcome Measure(s)
First, the integrity of the posterior cranial vault among HFM patients was determined. If proven to be unaffected, it could be used as a reference in the placement of the construct. Second, the position of the ear in relation to the cranium was assessed in healthy age-matched controls. Third, if proven to be useful, the concordance of these cranium-based relationships could be validated among our HFM cohort.
Results
The posterior cranial vault is unaffected in HFM (P > .001). Further, craniometric relationships between the tragus and the Foramen Magnum, as well as between the tragus and the posterior cranium, have been shown to be highly similar and equally precise in predicting tragus position in healthy controls (P > .001). These relationships held true across all age groups (P > .001), and importantly among HFM patients, where the mean absolute difference in predicted tragus position never surpassed 1.5 mm.
Conclusions
Relationships between the tragus and the cranium may be used as an alternative to distorted facial anatomy or surgeon's experience to assist in pre-operative planning of construct placement in microtia reconstruction for HFM patients.
Keywords
Background
Among hemifacial microsomia (HFM) patients, 66% to 99% are born with microtia.1–3 Microtia reconstruction in general remains a formidable challenge, but this is especially true in this patient population. The facial landmarks and measurements normally used on the unaffected side to determine the ideal antero-inferior position for the auricular construct cannot be used for patients with severe facial hypoplasia and asymmetry.4,5 Moreover, temporal bone depression complicates achieving proper auricular projection.6,7 Surgeons must therefore rely on their subjective experience when placing the constructed auricle.
Given that the associated facial asymmetry is of primary concern for patients and their surgeons, the study of cranium morphology among HFM patients has not been of much interest in the literature. Those focusing on endocranial morphology have provided mixed conclusions, with none formally studying the impact of HFM on the posterior cranial vault.8–12 In addition, a few authors believe the auricle is not located on the face per se, but rather on the temporal bone, a structure of the cranium itself.13,14 If the posterior cranial vault is in fact unaffected in patients with HFM, the normal ear's position in relation to the cranium may therefore be a reliable guide as to its position on the contralateral affected side. Thus, we hypothesize that the ideal location of the reconstructed auricle in HFM can be derived from the cranium rather than the face.
While it has been suggested that free-hand techniques may be sufficiently precise in determining auricular position, 4 a more scientific approach with calibrated anatomic measures would prove more useful. The goal of this study is to propose a novel, clinically applicable method for establishing the ideal location of the auricle in microtia reconstruction for HFM patients, derived from the cranium.
Materials and Methods
Following Institutional Review Board approval (#2022-3597), a retrospective review of all patients presenting to the department's craniofacial clinic between 2000 and 2021 was conducted. Inclusion criteria consisted of patients diagnosed with HFM and microtia, who had high-resolution craniofacial computerized tomography (CT) scans. Exclusion criteria consisted of patients who had incomplete medical records, had scans with too low resolution for accurate 3-D reconstruction, had scans where select landmarks were amputated, and/or had concomitant deformational plagiocephaly. Data regarding age, gender, comorbidities, OMENS( + ) classification, operative details, and follow-up were then retrieved from patients’ electronic medical records. Additionally, once the final HFM cohort was identified, age-matched healthy controls with CT scans were retrieved. Control patients had CT scans mainly due to facial trauma or internal auditory canal evaluation, and had the same type of CT examination to ensure homogeneity in CT protocol parameters.
Essentially, this study was accomplished in three steps. First, the integrity of the posterior cranial vault among HFM patients was determined. If proven to be unaffected, it could be used as a reference in the placement of the construct. Second, the position of the ear in relation to the cranium was assessed in healthy age-matched controls. Third, if proven to be useful, the concordance of these cranium-based relationships could be validated among our HFM cohort. Practically, the goal of these analyses was to determine the correlation between two types of cranium-based relationships among HFM patients: precise measurements of the endocranium and simple linear distances between the ear and the cranium, the latter of which could be easily reproduced in a clinical setting.
General Image Analysis
In conjunction with a radiologist experienced in pediatric craniofacial imaging, a protocol was developed to evaluate the CT scans. Many of the included patients received a CT scan to evaluate internal auditory canal integrity, whose imaging solely focused on the mastoid region. These scans included thin axial bone window slices (0.6 mm) of the temporal bone and the inner, middle, and external ear structures. Therefore, using some of the more classical landmarks (eg, vertex) and previously validated methods of assessment (eg, volume) were not possible.15,16 Although the literature is devoid of a consensus regarding the overall integrity of endocranial morphology in HFM, studies seem to agree that the cranial base axis is unaffected or is minimally (1°-2°) affected.9,11,12 This axis is usually measured in relation to the line bisecting the Foramen Magnum (FM) and passing through the occipital protuberance (P), in addition to other landmarks. 17 It was thus assumed that the FM occupies a relatively stable, central position in the posterior cranial vault. The Basion (Ba) and Opisthion (Op) were used as the main cranial landmarks in this study given that they fall on the line bisecting the FM, are present in all mastoid scans, and are easily identifiable. Finally, given that the tragus is an easily identifiable and central landmark of the ear, it was used as a correlate for the ear's position on the healthy side.
Scans were aligned along the midline of the posterior cranial vault, defined as traversing the Ba, Op, and P, and along the Frankfurt Horizontal (FH) plane. 18 Linear distances could then be measured on Multi-Planar Reconstruction (MPR) images generated by the Voxar 3D workstation (Barto, Kortrijk, Belgium). In light of the fact that the antero-posterior (A-P) position and projection of the construct are the foremost challenges in achieving symmetry in HFM patients, emphasis was placed on determining these positions. In reality, although the cephalo-caudal position of the construct is even more noticeable than the A-P position, it can easily and accurately be determined by the naked eye and was thus not included in our analysis. The detailed, step-by-step radiological protocol can be found in Supplemental Figure 1, and the craniometric points/planes used are defined in Supplemental Table 1. Of note, given the Ba and Op are not on the same level as the tragus, their coronal plane was used as a correlate for their true position—allowing the measure of direct linear distances with the tragus along the FH axis (Figure 1).
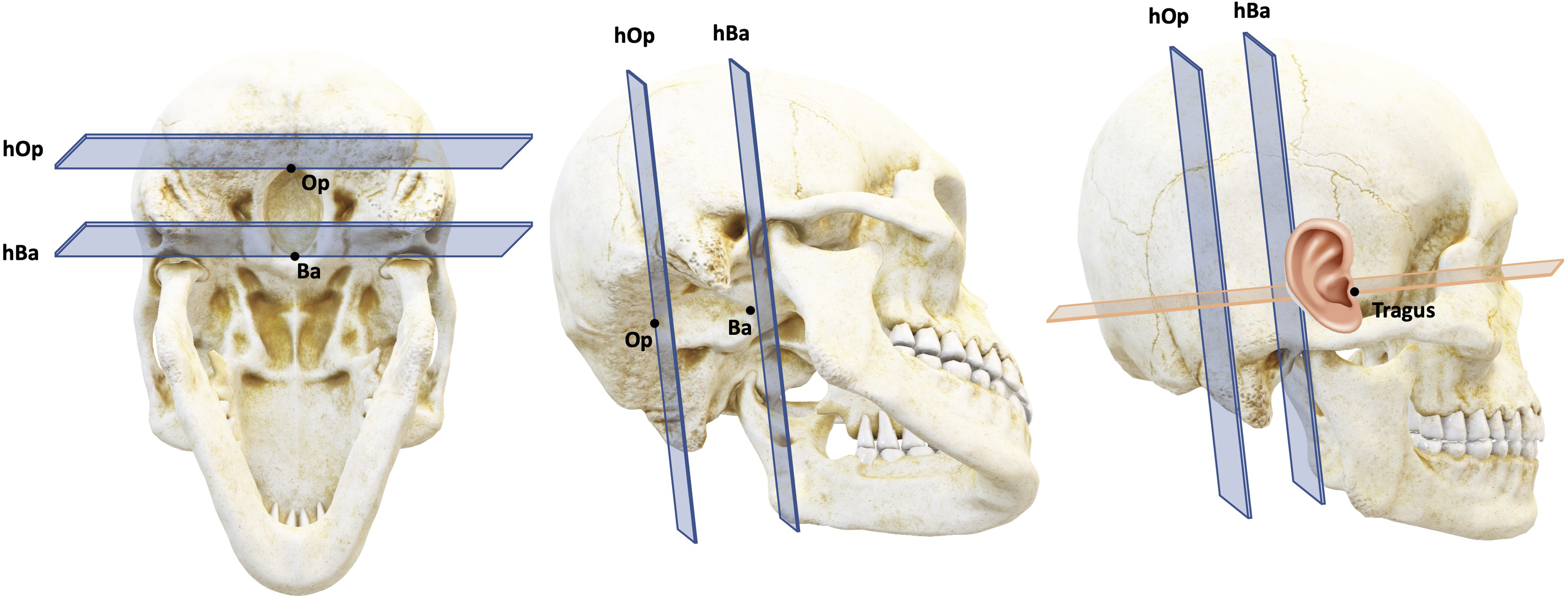
3-Dimensional representation of the Foramen Magnum-based landmarks and planes used. Abbreviations: Ba, Basion; Op, Opisthion; hBa, horizontal plane at the Basion; hOp, horizontal plane at the Opisthion.
Inter and intra-observer reliability were assessed by a secondary data collector repeating 10 of the scans’ measurements and the primary data collector also repeating 10 of the scans’ measurements 2 weeks later. Intra- and inter-rater reliability were evaluated using the intra-class correlation coefficient (ICC). Data retrieved from image analyses were compared as detailed below. All differences that were less than 1 mm were rounded up to 1 mm to facilitate data analysis. All statistical analyses were carried out using SPSS Version 24 (IBM Corp., Armonk, NY), with statistical significance set at P
Posterior Cranial Vault Measurements in HFM
The symmetry of the posterior cranial vault among HFM patients was first assessed through craniometric measurements. Craniometric distances were measured within the boundaries of the posterior cranial vault,
16
similarly to previously published protocols.19–21 Firstly, the length of the posterior cranial vault was evaluated by measuring the A-P distance between the following two planes to the posterior-most part of the scalp on the axial image: the horizontal plane at the Basion (hBa) and the horizontal plane at the Opisthion (hOp; Supplemental Figure 2). Secondly, the width of the posterior cranial vault was evaluated by measuring the horizontal (Right-to-Left) distance from the midline of the posterior cranial vault to the lateral-most points of the scalp at three levels: the Op, the posterior-most aspect of the unaffected concha (Co) and the P (Supplemental Figure 2). Measured distances were compared between the healthy and affected sides of HFM patients by means of an Asymmetry Index (AI) as per the following formula and with the affected side as the reference value: [(affected − unaffected/(affected + unaffected)) × 100].
22
The statistical significance of the AI was determined by a one-sample t-test with a reference value of 0 and a corrected P-value of P
Cranium-Based Relationships in Controls
Prior to using the anatomical relationship between the tragus and the cranium as a basis for our proposed measurements, they must first hold true in healthy controls. Therefore, the correlation between the true position of the tragus and its predicted position based on mirrored, cranium-based relationships in controls was assessed. Firstly, the precise position of the tragus in relation to the FM was determined. On the axial image, the A-P distance from the center of the tragus to the horizontal planes formed by the FM (hOp and hBa) was measured. In addition, the horizontal distance from the level of the Ba to the tragus was measured (Supplemental Figure 3). Respectively, these correspond to the ideal A-P and projection positions of the ear. Separately, the A-P distance from the tragus to the posterior-most level of the scalp and the horizontal distance from the level of the tragus to the P were measured on the axial image (Supplemental Figure 4). These distances will be referred to as the “L measures.”
All of the above-mentioned distances were mirrored onto the contralateral side. The difference in millimeters was then calculated between the true position of the tragus and the predicted position as determined by the FM-based relationships and L-measures. The horizontal and A-P differences generated by the L-measures and the FM-based relationships were compared by means of an independent sample t-test and an ANOVA, respectively.
Cranium-Based Relationships in HFM
With the craniometric relationships validated among controls, they could then be used to evaluate our HFM cohort. Finally, the above-described FM-based relationships and L-measures were determined on the unaffected side of each of the HFM patients. These distances were mirrored onto the affected side, and the difference between their respective ideal positions of the tragus was determined. Given the ultimate goal of this study is to validate the L-measures, they were used as the reference when computing the absolute difference among measurement methods. The horizontal and A-P differences generated by the FM-based relationships were compared by means of an independent sample t-test and an ANOVA, respectively.
Results
Demographics
A total of 36 HFM patients were included. Eight patients had undergone scans at multiple ages, amounting to a total 44 CT scans included in the final analysis. Patients were on average 10.57 ± 7.2 years old and more frequently boys (M:F ratio, 23:13). As per the OMENS( + ) classification, patients were mostly M1 (n = 17) and E3 (n = 23). Patients were followed for a mean of 125.8 ± 50.5 months, and all received medical imaging. Complete patient demographics can be found in Supplemental Table 2.
Data Collection Reproducibility
The ICC for inter-rater reliability was 0.991 and the ICC for intra-rater reliability was 0.999. This demonstrates the high reproducibility of the proposed CT scan measurements.
Posterior Cranial Vault Measurements in HFM
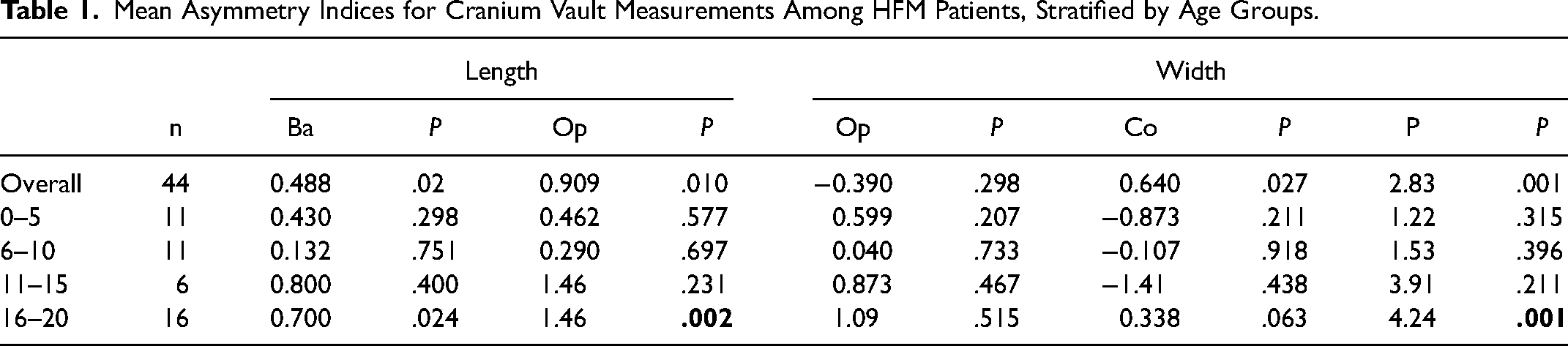
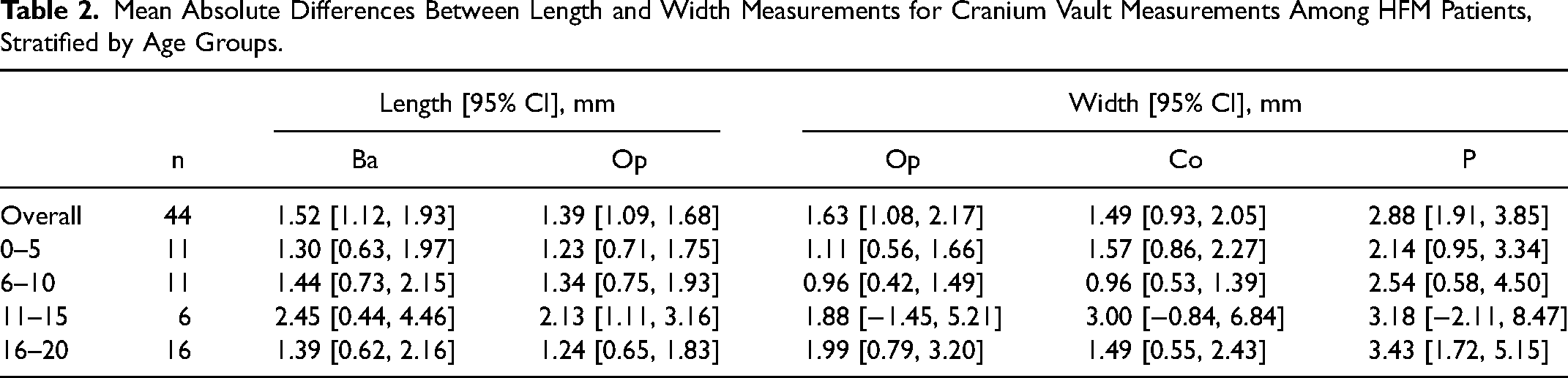
Overall, none of the computed AIs were significant, as most were closely aggregated around 0 (Table 1 and Figure 2). In terms of overall length and width measurements, mean absolute differences between sides were all between 1 and 3 mm (Table 2). This demonstrates no noticeable differences exist between the affected and unaffected sides. However, when stratified by age, only AIs corresponding to length at the Op (P = .002) and width at the P (P = .001) among the 16 to 20 age group were significant. Finally, mean absolute differences tended to be slightly higher in the 10 to 15 age group and among width at P across categories.
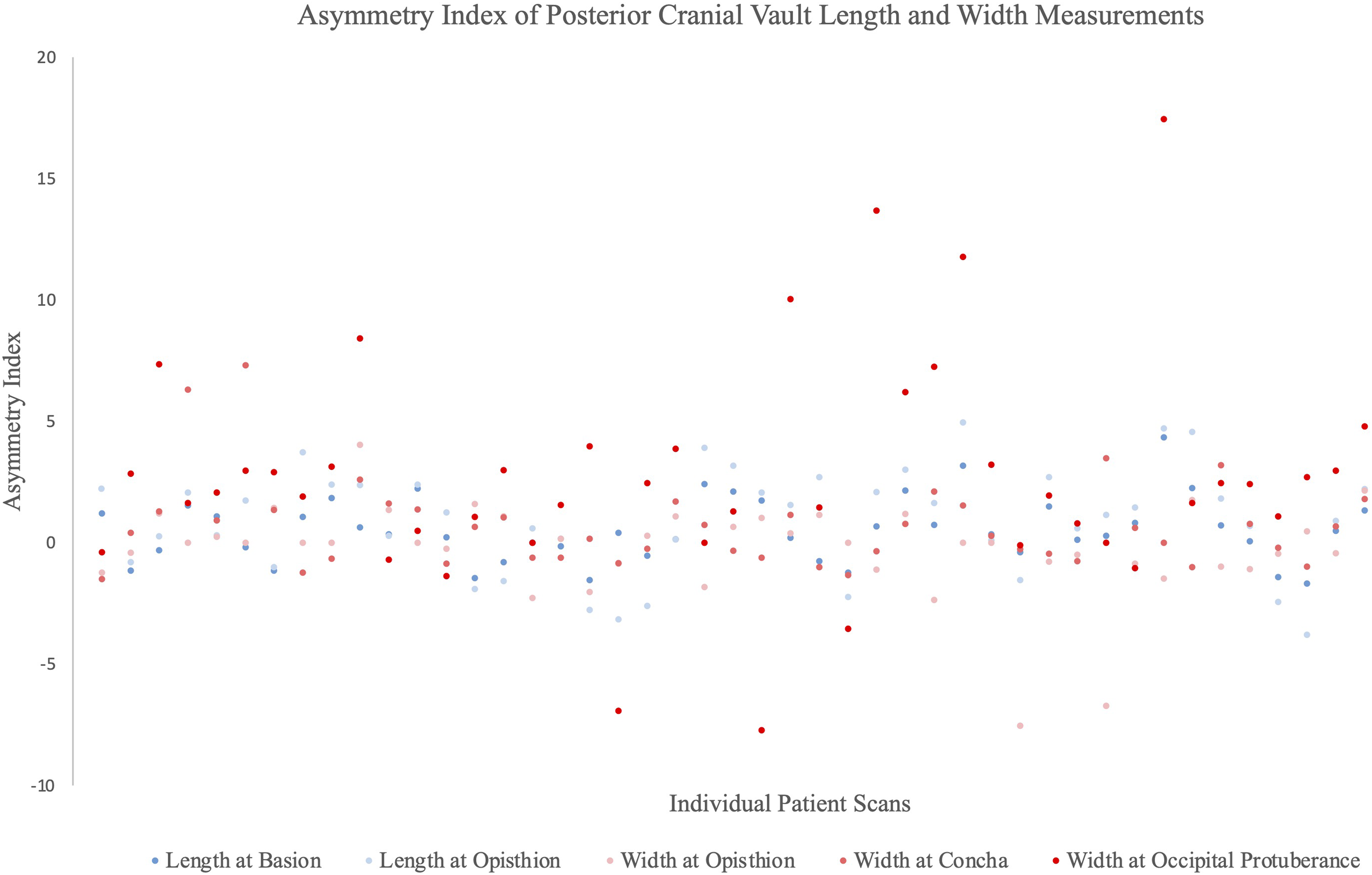
Asymmetry index of posterior cranial vault length and width measurements. Positive values represented asymmetry toward the affected side (affected>healthy), while negative values represented asymmetry toward the healthy side (healthy>affected).
Mean Asymmetry Indices for Cranium Vault Measurements Among HFM Patients, Stratified by Age Groups.
Mean Absolute Differences Between Length and Width Measurements for Cranium Vault Measurements Among HFM Patients, Stratified by Age Groups.
Cranium-Based Relationships in Controls
Among controls, mean overall differences between the predicted tragus position from both the L-measures and the FM-based measures, and the actual tragus, were not significantly different for both A-P (P = .229) and horizontal (P = .005) axes (Supplemental Table 3). Therefore, there are no significant differences yielded from predicting the tragus’ position with either of the two methods. This was also true among all age groups.
Cranium-Based Relationships in HFM
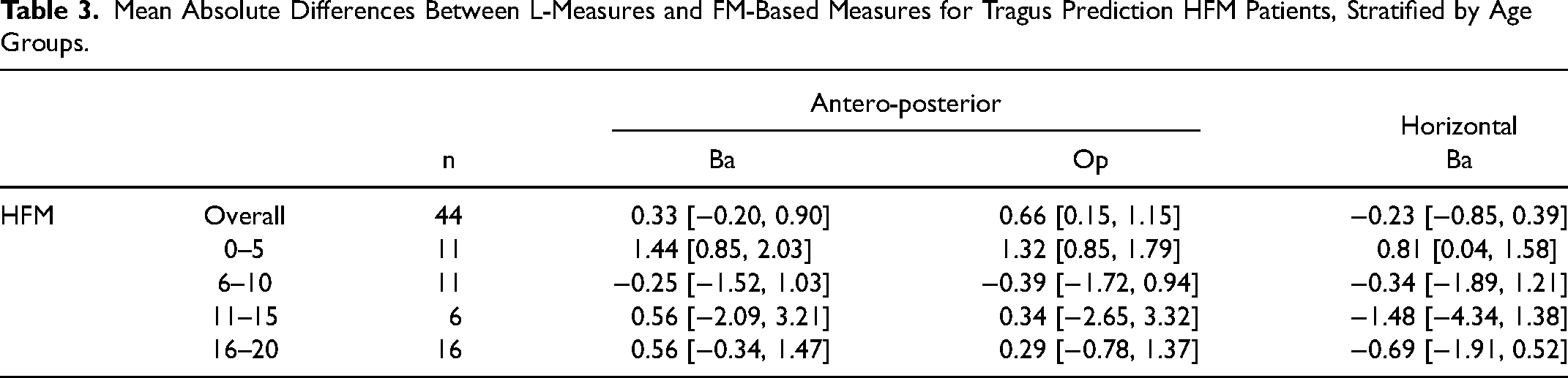
Among HFM patients, mean overall differences between the predicted tragus position from L-measures (reference) and FM-based measures were within the range of ±1 mm (Table 3), demonstrating the high correlation between these measures even when used in this patient population. When stratified by age groups, differences were also relatively small, with the largest one being −1.5 mm (horizontal distance at Ba). Therefore, the L-measures may be used to accurately determine the A-P and R-L position of the construct in HFM patients.
Mean Absolute Differences Between L-Measures and FM-Based Measures for Tragus Prediction HFM Patients, Stratified by Age Groups.
Discussion
Facial asymmetry in HFM patients renders symmetric placement of the construct during microtia reconstruction a challenging task. Previous studies have suggested that the FM is accurately aligned in this patient population. Results from this study suggest the posterior cranial vault is unaffected in HFM, and may thus be used as a reliable anatomic landmark. This study also demonstrates that the linear relationships between the tragus and the FM, as well as between the tragus and the posterior cranium (L-measures), may be highly similar. The L-measures, easily measurable in a clinical setting, can therefore be used as a guide in the pre-operative planning of symmetric construct placement in microtia reconstruction for HFM patients. Although FM-based measures may be slightly more precise, this becomes a negligible concern when weighed against the clinical applicability and high degree of correlation of the L-measures.
While many aspects of the cranial base may be affected in HFM,9,12 the present study suggests the posterior vault is unaffected by the condition. The results from this study also suggest that clinically, the proposed L-measures and FM-based measures are equally precise in predicting tragus position among controls. These relationships also seem to hold true in HFM patients, and demonstrate a minimal difference in predicting construct position. In addition to conferring validity to these measures, their reliability (ie, inter- and intra-observer) was also vetted. Importantly, age does not seem to have an effect on the validity of these relationships.
Classically, the distance from the oral commissure to the lobule and from the lateral canthus to the helix is measured and transposed onto the contralateral side to accurately predict the construct position in microtia reconstruction. 23 However, given the constricted facial dimensions in HFM patients, application of this method would result in the ear positioned far too posteriorly. Although no definitive solution has been proposed, many authors have attempted to address this issue. Some have suggested waiting until at least 8 years of age for correction 24 or advocate for skeletal correction before ear placement 14 in order to mitigate this challenge. Firmin 13 proposes relying on the usual facial landmarks as a guide, but then adjusting the construct's position based on experience and subjective assessment. Qian et al 6 propose placing the crus of the helix 1.5 to 2 cm from the temple, while Park and Park 25 suggest using the posterior margin of the mandibular ascending ramus as a guide. Recently, more technologically advanced solutions have been proposed, such as using stereophotogrammetry-based morphing of the unaffected ear onto the affected side through landmark-based facial proportions 4 or by using a 3-D printed model of the patient's head to pre-determine the best possible location. 26
Given the tragic outcome of an auricular reconstruction placed in an improper location, and the heterogeneity and relative lack of specific techniques for symmetric construct placement in microtia reconstruction for HFM patients, the potential utility of this study is evident. Practically, our proposed method can be translated to direct clinical use in a simple and effective manner. The L-measures can be measured and mirrored using a straight rule, with the patient's head resting on a straight surface (eg, wall, operating room table). Figure 3 demonstrates a depiction of such, through photographs obtained from a patient following informed consent for their use. In order to clearly demonstrate the difference yielded from classical freehand techniques, a photo of a post-operative patient was chosen rather than a preoperative one. The A-P distances from the healthy and reconstructed sides were equal to 9.7 and 10.3 cm, respectively. The horizontal distances were measured for the healthy and reconstructed sides at 9.4 and 9.7 cm, respectively. This suggests the construct might have been placed slightly too anteriorly and was slightly too projected. Of note, cephalo-caudal position can be determined by examination of the patient's face on frontal view.6,25 This exact method may be used pre- or intra-operatively to help decide on the reconstructed ear's position.
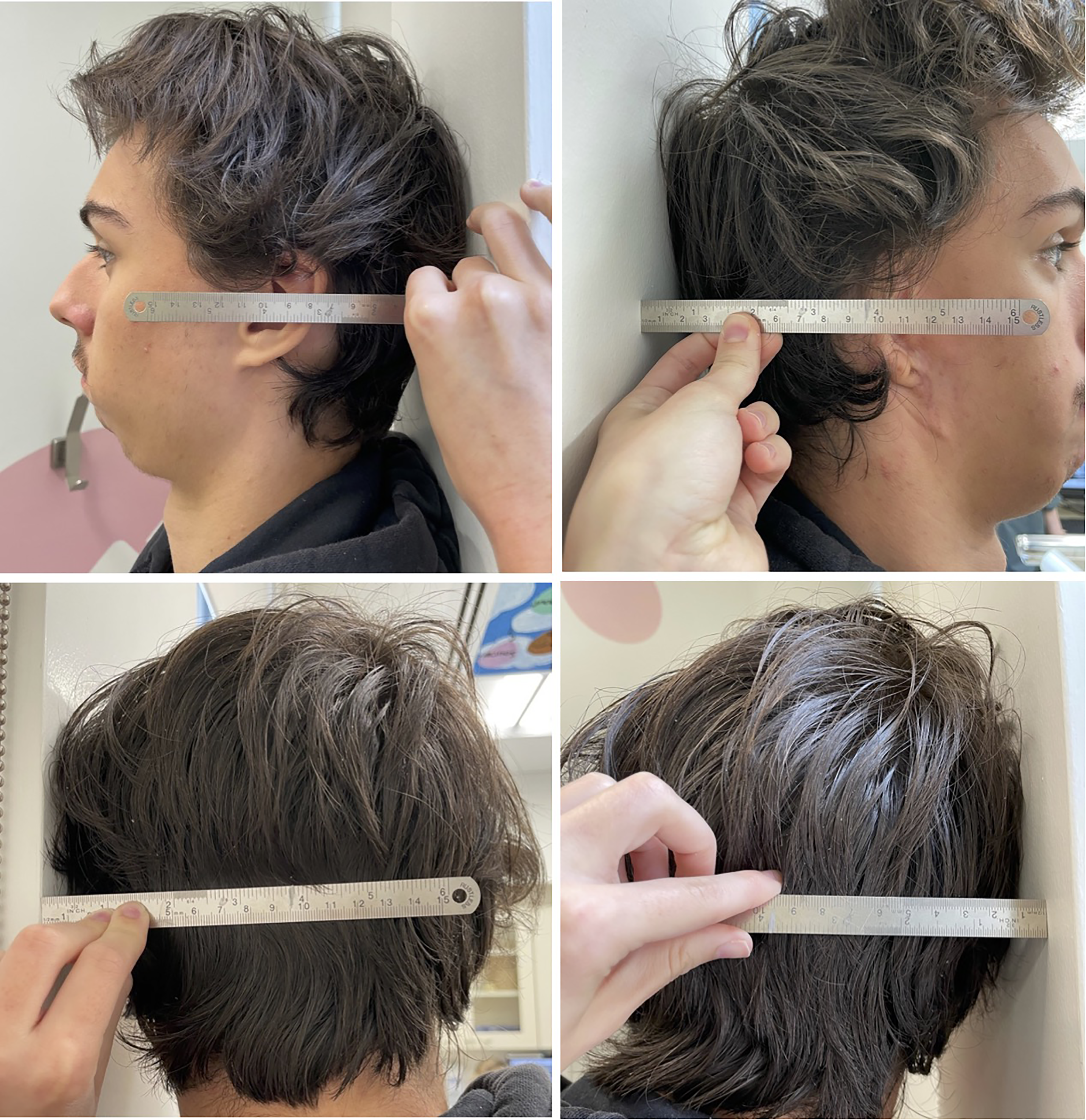
Example of the L-measures. The measures are taken with a straight ruler, between the patient's head and the wall. For antero-posterior measurements, the distance from the wall (back of the head) to the tragus is measured. For horizontal measurements, the distance from the wall (tragus resting on the wall) to the center of the head (determined by palpation of external occipital protuberance and/or C1) is measured.
Some authors are strong proponents of internal auditory canal evaluation in all children with microtia, through a scan of their mastoid region.24,27 Therefore, if a CT scan is available, FM-based relationships can be measured and mirrored onto the affected side. The predicted position of the tragus can then be measured in relation to anatomical landmarks of the author's choosing, and then drawn on the patient pre-operatively. Further, adequately performed CT scans according to neuro navigation protocols could potentially assist the surgeon intraoperatively.
Limitations and Future Directions
The present study is not devoid of limitations. Firstly, given the retrospective nature of the study and the non-blinding of the primary scan assessor, the results may be subject to a measurement bias. The authors recognize the limited internal validity of the proposed craniometric measurements, however, given the type of scans available, classical volume-based analyses could not be utilized. Although the goal was to devise a simple and reproducible method, the few landmarks and measurements used may be an oversimplification. The authors also recognize that the use of the FM as a central landmark remains an assumption, and may limit the internal validity of our results. Especially since the literature is heterogeneous in terms of its assessment of the cranial vault in HFM patients. Practically, surgeons may need to take existing remnants and the position of the external auditory canal into consideration when deciding on the placement of the construct. While this may affect the ear's final position, knowing the ear's ideal position is important in guiding the surgeon's decision, hence the importance of this article. It may also appear that a significant limitation of this measurement method is the fact that they are measured on a single craniometric plane, which may not be the resting position of patients’ heads (due to orbital dystopia, muscle imbalances, etc). This was mitigated by using the FH plane, passing through the tragus, which could be objectively determined by the surgeon. Finally, given the skull may not be static until about 12 years of age, 28 pooling of results among patients from 0 to 20 years of age may not be accurate. This was partially mitigated through age stratification. The L-measures require validation in a prospective cohort in order to be deemed truly useful. Additionally, future studies may strive to devise more objective methods of determining the ear's cephalo-caudal positioning, should it be deemed necessary despite the literature being clear that constructs should be placed at the same height, which is easily determinable by eye using the earlobe as a guide.6,25
Conclusion
The novel cranium-based method proposed can be utilized in determining the ideal A-P and R-L location for construct placement in microtia reconstruction for HFM patients, among which facial measurements extrapolated from the unaffected side are less useful. This method is simple in application and of virtually costless applicability, regardless of age. While the authors concede that the ideal construct position derived with this technique may not yield a precisely symmetric position, determining position in a more objective fashion may be of value in more complex cases of auricular reconstruction. This is especially true as microtia is most often the anomalous feature to be addressed first in facial symmetrization in this patient population.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656221135925 - Supplemental material for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients
Supplemental material, sj-docx-1-cpc-10.1177_10556656221135925 for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients by Gabriel Bouhadana, Jordan Gornitsky, Eli Saleh, Ramy El Jalbout, Daniel E. Borsuk and Sabrina Cugno in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-2-cpc-10.1177_10556656221135925 - Supplemental material for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients
Supplemental material, sj-jpg-2-cpc-10.1177_10556656221135925 for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients by Gabriel Bouhadana, Jordan Gornitsky, Eli Saleh, Ramy El Jalbout, Daniel E. Borsuk and Sabrina Cugno in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-3-cpc-10.1177_10556656221135925 - Supplemental material for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients
Supplemental material, sj-jpg-3-cpc-10.1177_10556656221135925 for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients by Gabriel Bouhadana, Jordan Gornitsky, Eli Saleh, Ramy El Jalbout, Daniel E. Borsuk and Sabrina Cugno in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-4-cpc-10.1177_10556656221135925 - Supplemental material for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients
Supplemental material, sj-jpg-4-cpc-10.1177_10556656221135925 for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients by Gabriel Bouhadana, Jordan Gornitsky, Eli Saleh, Ramy El Jalbout, Daniel E. Borsuk and Sabrina Cugno in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-5-cpc-10.1177_10556656221135925 - Supplemental material for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients
Supplemental material, sj-docx-5-cpc-10.1177_10556656221135925 for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients by Gabriel Bouhadana, Jordan Gornitsky, Eli Saleh, Ramy El Jalbout, Daniel E. Borsuk and Sabrina Cugno in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-6-cpc-10.1177_10556656221135925 - Supplemental material for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients
Supplemental material, sj-docx-6-cpc-10.1177_10556656221135925 for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients by Gabriel Bouhadana, Jordan Gornitsky, Eli Saleh, Ramy El Jalbout, Daniel E. Borsuk and Sabrina Cugno in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-7-cpc-10.1177_10556656221135925 - Supplemental material for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients
Supplemental material, sj-docx-7-cpc-10.1177_10556656221135925 for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients by Gabriel Bouhadana, Jordan Gornitsky, Eli Saleh, Ramy El Jalbout, Daniel E. Borsuk and Sabrina Cugno in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-8-cpc-10.1177_10556656221135925 - Supplemental material for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients
Supplemental material, sj-jpg-8-cpc-10.1177_10556656221135925 for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients by Gabriel Bouhadana, Jordan Gornitsky, Eli Saleh, Ramy El Jalbout, Daniel E. Borsuk and Sabrina Cugno in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-9-cpc-10.1177_10556656221135925 - Supplemental material for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients
Supplemental material, sj-docx-9-cpc-10.1177_10556656221135925 for Determination of Novel, Cranium-Based Relationships for Construct Placement in Microtia Reconstruction for Hemifacial Microsomia Patients by Gabriel Bouhadana, Jordan Gornitsky, Eli Saleh, Ramy El Jalbout, Daniel E. Borsuk and Sabrina Cugno in The Cleft Palate-Craniofacial Journal
Footnotes
Financial Disclosure Statement
The authors declare that there is no conflict of interest. This article was written in the context of a Master's degree, funded by the Biomedical Sciences Recruitment Grant from the University of Montreal, the Canada Graduate Scholarship-Master's (CGSM) from the Canadian Institutes of Health Research (CIHR) and the Master's Training Award from the Fonds de recherche du Québec-Santé (FRQS).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research, Fonds de Recherche du Québec-Santé.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.