
Abstract
Objective
The aim of this study was to compare the orbitomalar region projection in patients with cleft lip and palate (CLP) with skeletal class 1 cases.
Design
Retrospective.
Setting
Single center.
Patients
Cephalometric data of 52 cases with unilateral CLP, 25 cases with bilateral CLP, and 60 healthy participants in skeletal class 1 without CLP were included.
Main Outcome Measure(s)
A total of 5 parameters, 3 in the orbital and 2 in the suborbital region, that determine the projection of the orbitomalar region on lateral cephalograms, and 13 parameters of the craniofacial region were evaluated.
Results
Lateral, inferior, and anterior orbital parameters were similar between groups, while suborbital parameters were in a retrusive position in the CLP groups compared to the control group (P < .05). No significant difference was found between the CLP groups in terms of suborbital parameters. A moderate positive correlation was found between orbitomalar parameters and the anteroposterior positions of the maxilla and mandible. The lateral orbital region had a moderate negative correlation with anterior maxillary height, and the suborbital region had a negative moderate correlation with maxillary inclination.
Conclusion
Suborbital projection was more retrusive in CLP compared to the control group, but no difference was found between the CLP groups. On the other hand, the correlation between orbitomalar projection and maxillary and mandibular development was significant. The results show that there is a need for alternative treatment modalities for the suborbital region in patients with CLP.
Introduction
Cleft lip and palate (CLP) is the most common congenital anomaly of the head and neck region and its incidence is 1 in 700 to 1000 live births.1–4 Hypoplasia can be observed in bones and soft tissues due to deviation from normal development in cases with CLP. Considering the embryological development of the face, this hypoplasia can often be seen at varying rates in the midface region, and generally the intrinsic factors of the cleft itself, functional causes and previous surgeries (iatrogenic) are among the main causes.5–13 The midface is mainly composed of the maxilla and the body of the zygomatic bone, and this region also includes the lower part of the orbital and the malar region. Studies in the literature have reported that hypoplasia in the midface area is mostly limited to the areas adjacent to the cleft (cleft region, nose, and septum).14–17 However, there is no consensus on whether there is hypoplasia in more distant and deeper midfacial structures, and studies evaluating the sagittal projection of the orbitomalar region are also very limited.18–22 It has also been reported that changes in this region can often be overlooked during routine examination.
23
In our clinical experience, it was also observed that midface hypoplasia was accompanied by orbitomalar region projection insufficiency in some cases in this patient group.
Therefore, the aim of the present study was to evaluate whether the orbitomalar region projection is different compared to the normal population and To investigate whether this region shows any correlation with other craniofacial parameters (anteroposterior and vertical positions of the maxilla and mandible, skull base angle, etc.; Figure 1).

An example of cases with loss of projection (arrow) in the sagittal plane in the orbitomalar region in cases with CLP.
The results will address the gap in the literature on the orbitomalar region and help clinicians evaluate this region with a more comprehensive and careful approach during treatment planning in terms of functional facial balance and esthetics.
Materials and Methods
Approval was obtained from the local ethics committee of our hospital before the study (G.Ü-ET 562). Written consent was obtained from the parents of all the patients included in the study. The cases included in the study were divided into 3 groups as unilateral and bilateral CLP groups and the control group. Minimum sample size for each group was calculated as 24 cases with a power of 90% at 0.4 effect size and α an error level of .05.
The medical records and cephalometric images of the patients who were operated for unilateral or bilateral complete CLP in our clinic between 2010 and 2015 were analyzed retrospectively.
Inclusion criteria in the study group were as follows:
Complete unilateral or bilateral CLP; Absence of craniofacial anomalies or syndromes; Completion of CLP repairs within 18 months; Undergoing the same surgical techniques were used in lip and palate repair (modified Millard for the lip, V-Y pushback palatoplasty for unilateral cleft palate, 2 flap palatoplasty for bilateral cleft palate); Not having received orthodontic treatment before surgery; Being 7 to 14 years old before orthodontic treatment; and Having lateral cephalometric x-ray images before alveolar bone grafting. Absence of craniofacial anomalies or syndromes; Physically healthy and having class I maxillomandibular relationship; Having no temporomandibular joint disorder; and Being 7 to 14 years old before orthodontic treatment, and having lateral cephalometric x-ray images.
Inclusion criteria in the control group were as follows:
Cephalometric Analysis
In all cases, lateral cephalometric x-ray (PM 2002 CC Proline; Planmeca) was taken after the head was positioned with the Frankfort horizontal plane parallel to the ground, the teeth in centric occlusion, and the lips in a relaxed position. The data and images in the x-rays were corrected according to the level of magnification in all cases. Reference points, planes, and angles to be used in measurements on cephalometric x-rays were determined (Figure 2a to c). In order to minimize the measurement error, all cephalometric evaluations were made by a single practitioner (in order to avoid differences between observers) and repeated 3 times with an interval of 2 weeks. Mean values of the measurements was included in the analyses. Pearson’s correlation coefficient was used to examine intraclass variability. The correlation coefficient was above 0.90 in all reference measurements, confirming no intraclass variability. A total of 5 parameters representing the orbitomalar region were determined as
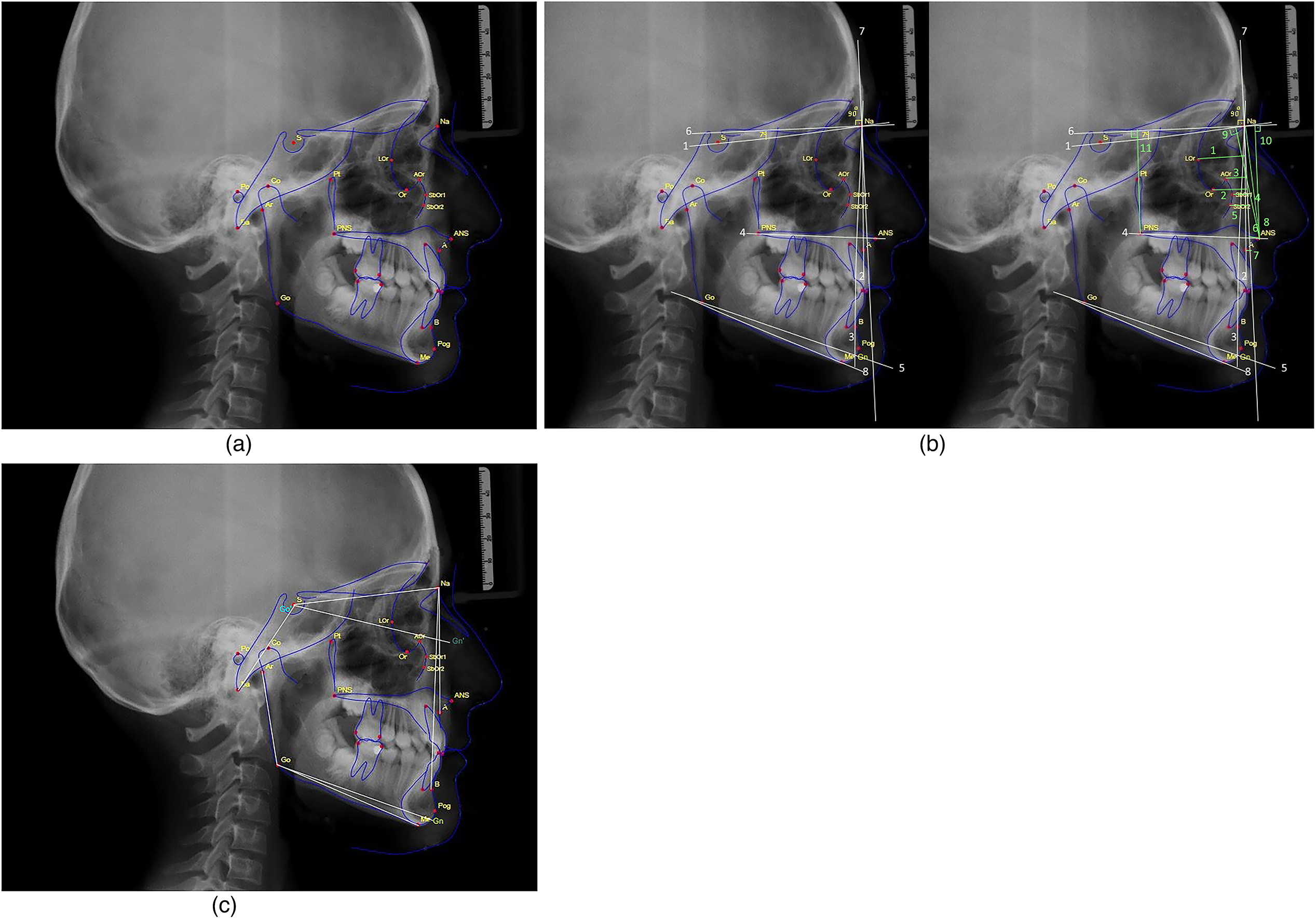
(a) Reference points are used in lateral cephalometric analysis.
Statistical Analysis
Data analysis was performed with IBM Statistical Package for the Social Sciences (SPSS) version 26. Categorical variables were presented as numbers and percentages. Skewness and Kurtosis values were used to check whether the variables conformed to normal distribution. Skewness values should be between ± 1.5 for a variable to be normally distributed. 24 Accordingly, all parameters except for the Gonial Angle (Ar-Go-Me) (°) were normally distributed. Differences between categorical variables were evaluated by the chi-square test. One-way analysis of variance (ANOVA) test was used to compare normally distributed linear and angular parameters between the study groups, and Kruskal–Wallis test was used to compare nonnormally distributed linear and angular parameters between the study groups. Post hoc tests were used to investigate the source of the differences. Pearson and Spearman tests were used for correlation analysis. A correlation coefficient of 0.00 to 0.30 was considered as weak correlation, 0.30 to 0.70 as moderate correlation, and 0.70 to 1.00 as strong correlation.24,25 The values of P < .05 and < .01 were considered statistically significant.
Results
Evaluation of Cases in Terms of Descriptive Statistical Findings
Out of 137 patients included in the study, 52 had unilateral CLP and 25 had bilateral CLP, while 60 patients were included in the control group. In terms of gender distribution, 50% of the control group were females and 50% males. The unilateral CLP group were 38.5% females and 61.5% males. The bilateral CLP group were 48% females and 52% males. Mean age was 10.40 (±2.02) in the unilateral CLP group, 10.54 (±2.62) in the bilateral CLP group, and 10.44 (±1.33) in the control group. There was no significant difference between the study groups in terms of age and gender. Gender and age distribution of the cases are shown in Table 1.
Linear and Angular Parameter Measurement Values According to Groups.
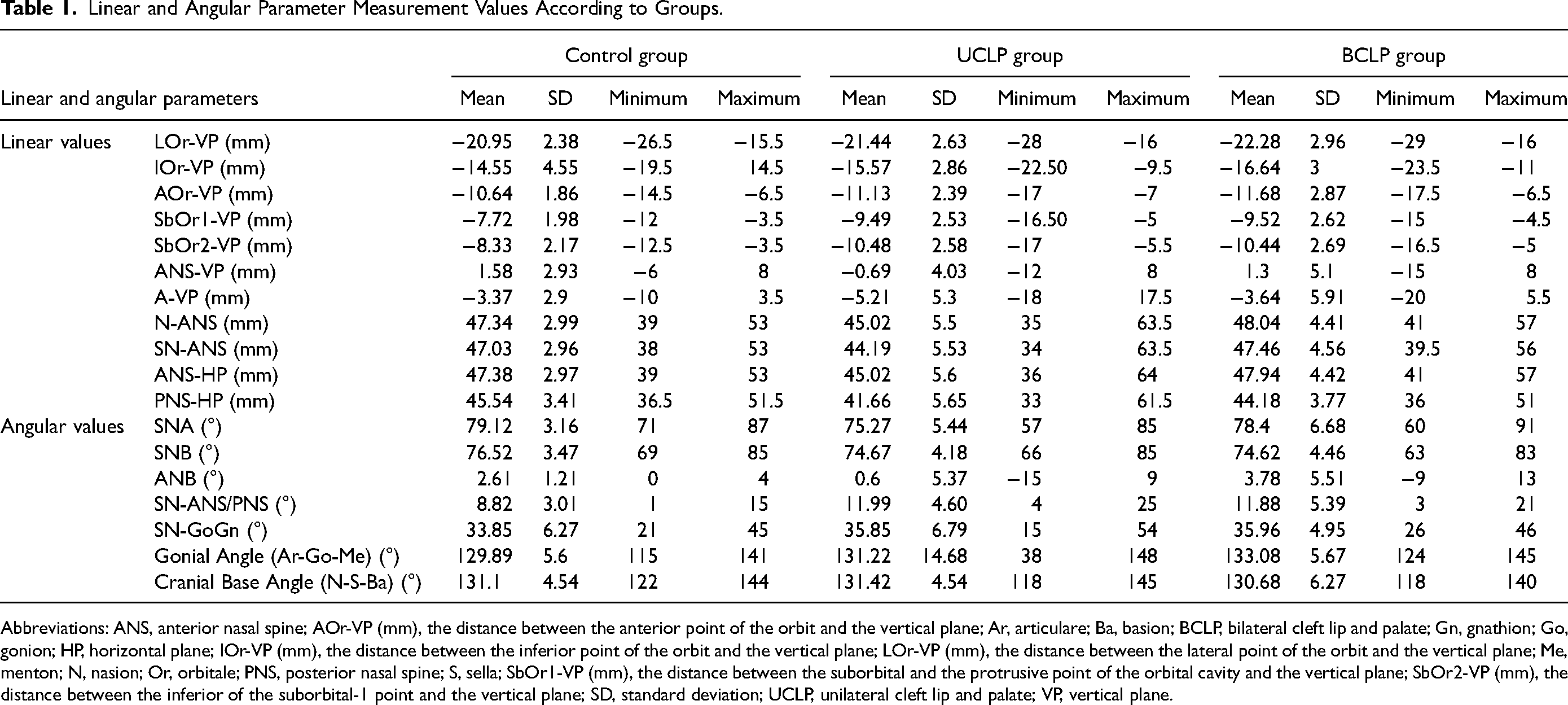
Abbreviations: ANS, anterior nasal spine; AOr-VP (mm), the distance between the anterior point of the orbit and the vertical plane; Ar, articulare; Ba, basion; BCLP, bilateral cleft lip and palate; Gn, gnathion; Go, gonion; HP, horizontal plane; IOr-VP (mm), the distance between the inferior point of the orbit and the vertical plane; LOr-VP (mm), the distance between the lateral point of the orbit and the vertical plane; Me, menton; N, nasion; Or, orbitale; PNS, posterior nasal spine; S, sella; SbOr1-VP (mm), the distance between the suborbital and the protrusive point of the orbital cavity and the vertical plane; SbOr2-VP (mm), the distance between the inferior of the suborbital-1 point and the vertical plane; SD, standard deviation; UCLP, unilateral cleft lip and palate; VP, vertical plane.
Linear and Angular Measurement Parameters of the Cases
The mean, standard deviation (SD), minimum and maximum values of the linear, and angular measurement parameters of the groups are shown in Table 2.
Comparison of Linear Measurement Parameters of Orbitomalar Region According to Groups.
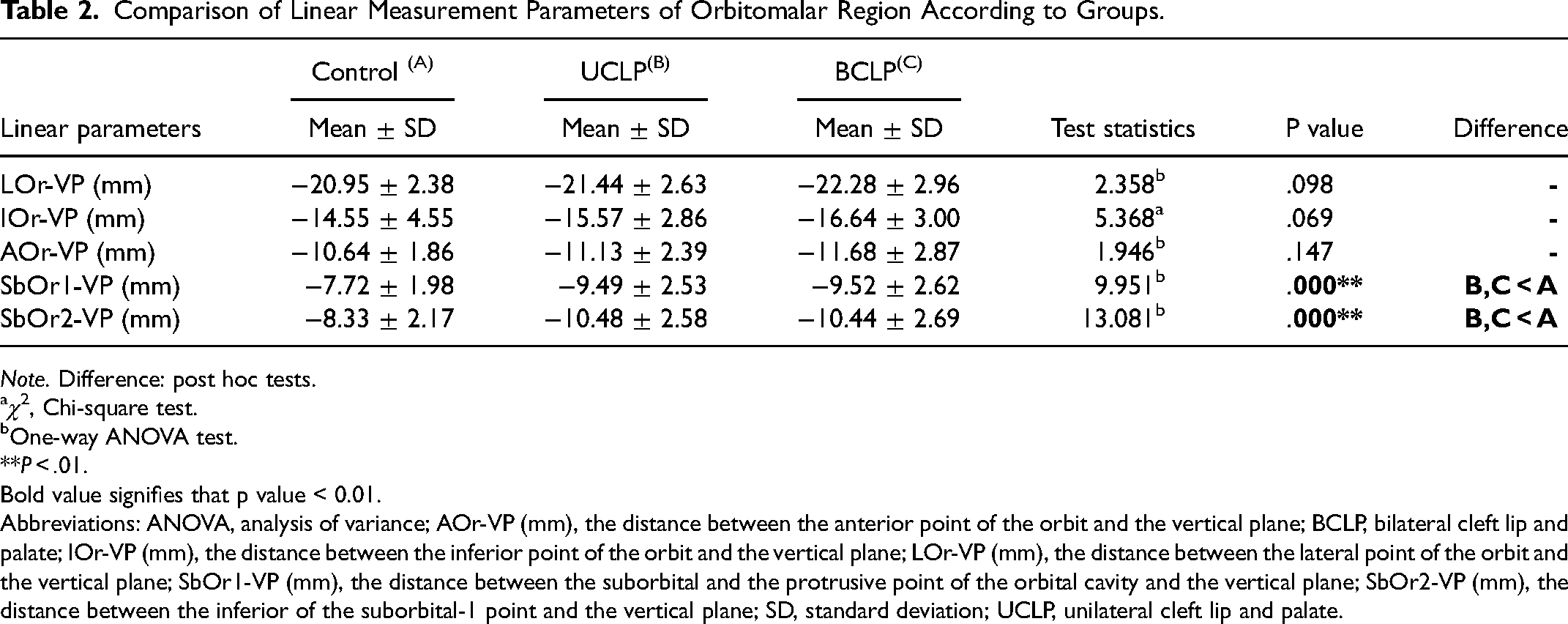
Note. Difference: post hoc tests.
χ2, Chi-square test.
One-way ANOVA test.
**P < .01. Bold value signifies that p value < 0.01.
Abbreviations: ANOVA, analysis of variance; AOr-VP (mm), the distance between the anterior point of the orbit and the vertical plane; BCLP, bilateral cleft lip and palate; IOr-VP (mm), the distance between the inferior point of the orbit and the vertical plane; LOr-VP (mm), the distance between the lateral point of the orbit and the vertical plane; SbOr1-VP (mm), the distance between the suborbital and the protrusive point of the orbital cavity and the vertical plane; SbOr2-VP (mm), the distance between the inferior of the suborbital-1 point and the vertical plane; SD, standard deviation; UCLP, unilateral cleft lip and palate.
The mean values of the parameters representing the orbitomalar region were evaluated between the groups. Accordingly:
Comparison of Orbitomalar Region Parameters Between the Groups
The comparison of orbitomalar region parameters between the groups is shown in Table 2. No significant difference was found in the measurement values from the orbital lateral, inferior, and anterior points [(LOr-VP (mm), IOr-VP (mm), and AOr-VP (mm)] between the study groups. In contrast, a significant difference was found in the projection parameters of the suborbital region [(SbOr1-VP (mm) and SbOr2-VP (mm)] (
Correlation Relationship Between Orbitomalar and Other Craniofacial Measurement Values in the CLP Group.
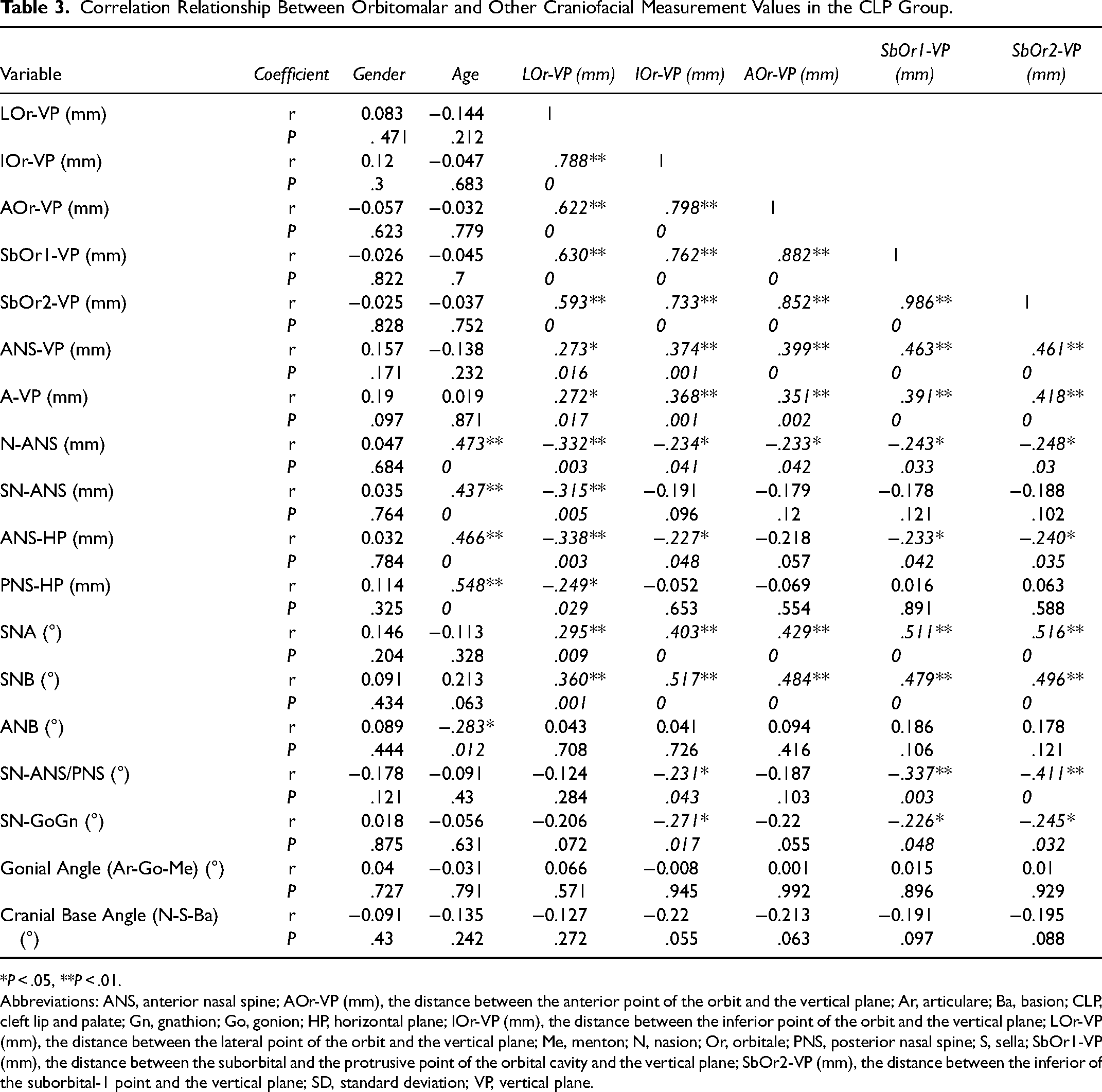
*P < .05, **P < .01.
Abbreviations: ANS, anterior nasal spine; AOr-VP (mm), the distance between the anterior point of the orbit and the vertical plane; Ar, articulare; Ba, basion; CLP, cleft lip and palate; Gn, gnathion; Go, gonion; HP, horizontal plane; IOr-VP (mm), the distance between the inferior point of the orbit and the vertical plane; LOr-VP (mm), the distance between the lateral point of the orbit and the vertical plane; Me, menton; N, nasion; Or, orbitale; PNS, posterior nasal spine; S, sella; SbOr1-VP (mm), the distance between the suborbital and the protrusive point of the orbital cavity and the vertical plane; SbOr2-VP (mm), the distance between the inferior of the suborbital-1 point and the vertical plane; SD, standard deviation; VP, vertical plane.
Correlation Analysis Between the Orbitomalar Parameters and Other Craniofacial Parameters in Cases With CLP
The correlation between orbitomalar parameters and other craniofacial parameters in cases with CLP (unilateral and bilateral) is shown in Table 3.
Discussion
In cases with CLP, problems in facial development can be grouped under 3 main categories: embryological, surgical, and intrinsic factors.26–30 This problem has been reported to affect areas close to the cleft, such as the maxilla, nose, nasal septum, and upper lip, but it can also affect more distant areas such as the upper face, malar region, and even the skull base, albeit less frequently.20,31–36 Although cephalometric analysis has some disadvantages such as converts three-dimensional (3D) plane to two-dimensional (2D), allowing only profile evaluation, and low resolution, it is still the standard imaging method in orthodontic/orthognathic diagnosis and treatment. It also requires less technical infrastructure and in some studies, there is no significant difference between cephalometric analysis and cone-beam computed tomography (CT) evaluation.37,38 The abovementioned factors were the main reasons we chose this imaging modality.
In the present study, gender distribution was similar between the groups. Previous studies in the literature also reported that gender did not have a significant effect on cephalometric measurements in cases with CLP.26,33,39,40 Furthermore, age was also similar between the study groups, eliminating the differences in cephalometric values that may be caused by age. Laowensiri reported that in late childhood (after the first 5 years of life), the vertical growth phase of the face becomes more dominant compared to sagittal growth. 41 The mean age of the cases in the present study was above 10 years, which means that the sagittal growth of the face is completed to a large extent and possible projection losses can be evaluated in a correct manner. Since postrepair hypoplasia is limited only to the alveolar region in cases with isolated CLP repair does not cause serious changes in maxillary morphology and spatial position in cases with isolated cleft palate, these groups were not included in the study.42,43
Interpretation of Orbitomalar Parameter Measurements
No significant difference was found in lateral, anterior, and inferior orbital measurements [LOr-VP (mm), AOr-VP (mm), and IOr-VP (mm)] between the groups. This finding was interpreted as CLP not causing a developmental pathology at the orbital rim level. Although there are various publications about the orbital region in the literature, most of these studies evaluate soft tissue reference points (intercanthal, interocular distance, and lid fissure width) or orbital diameter in the transverse plane.23,33,44–46 Suri et al 47 reported that in cases with unilateral CLP, the orbital rim in the sagittal plane showed similar projections to the control group in craniofacial CT analyses, and these findings were consistent with the results of the present study. Kane et al 48 conducted a 3D CT analysis of 28 cases with unilateral CLP and reported that serious asymmetries were observed in the orbital region compared to the normal side. The asymmetries detected in this study were most likely due to the early (3 months) CT analysis of the cases. In fact, it has been reported in the literature that although some abnormalities are found in orbital morphology in the early period of life (2 months) in cases with CLP, the cases may exhibit normal morphological structure in the later follow-up periods (>24 months). 33
The suborbital projection parameters [SbOr1/2-VP (mm)] was found to be lower in the CLP groups compared to the control group, which showed that this region was negatively affected in terms of development, and this finding supported our clinical observation and hypothesis. Projection loss in the malar region has been previously reported in a limited number of studies.30,45,49 Zheng et al reported that the most common projection loss in cases with unilateral CLP after the alveolar region was seen in the zygomatic and infraorbital regions. The results obtained in the present study in the suborbital region were consistent with the study of Zheng et al, additionally, cases with bilateral CLP were also included in our sample. 22
The suborbital region being affected in contrast to the orbital rim level may be due to the fact that this region is closer to the cleft region and that the maxilla is more affected by the factors that cause sagittal growth restriction.
Interpretation of Correlation Analysis Results
The fact that the orbital region contains many anatomical sutures and the surrounding bone structures show development in multiple vectors shows that the growth in this region is dependent on a multivariate and complex mechanism. Orbital measurements showed moderate positive correlation with SNB (°), which suggested that the orbital projection was associated with the position of the mandible relative to the skull base. This finding was consistent with Enlow’s hypothesis on orbital embryology. Enlow mentioned that the middle cranial fossa is the driving force in the anteroposterior development of the nasomaxillary region (also the orbital region), and stated that this region plays a role in the anteroposterior development of the mandibular ramus indirectly via the pharynx. 50 In the present study, orbital and suborbital measurements showed a moderate positive correlation with SNA (°) and maxilla anteroposterior positions 1 to 2 [(ANS-VP (mm) and A-VP (mm)], which can be explained by the interplay between orbital and maxillary development. In fact, one of the bone structures that make up the orbital region is the maxilla, which hosts a large part of the orbital floor. For this reason, the projection of the maxilla in the sagittal plane is expected to directly affect the projection of the orbital.
Many factors such as genetic coding, biomechanical forces, sutures, nasal septum, and functional matrix theory play a critical role in facial development. 50 In addition, problems in the nasal septum (deviation) and loss of anatomical integrity in the premaxilla and lateral maxillary segments seen in patient groups with CLP may lead to the disappearance of the pacemaker effect of nasal septum in midface development and, subsequently, to the growth retardation in the sagittal plane. 51
When these factors are considered, the lateral orbital projection [LOr-VP (mm)] in patients with CLP showing a moderate negative correlation with anterior maxillary height can be explained by the changes in the growth vector caused by the scar secondary to lip and palate surgery, problems in the nasal septum, and biomechanical imbalances resulting from abnormal muscle anatomy. In particular, these factors shift the developmental vector more to the inferior due to the restrictive effect on sagittal growth in the maxilla, and this helps explain the negative correlation between maxillary height and lateral rim projection. In addition, sutures are anatomical points sensitive to tissue tension and respond in the form of bone resorption in areas of increased tension (eg, scarred areas). 50 This is another factor affecting projection loss. The moderate negative correlation between suborbital projection [SbOr2-VP (mm)] and maxillary inclination (SN/ANS-PNS) can also be attributed to the abovementioned sagittal growth-limiting factors. Maxilla, whose growth is restricted in the sagittal direction, moves toward the inferior and causes an increase in maxillary inclination by clockwise rotation.
Conclusion
While no developmental pathology was found at the orbital level in patients with unilateral and bilateral CLP, the projection of the suborbital region was significantly lower in these patients compared to the control group. This is an issue that should be considered in treatment planning, and as a clinical solution that are as follows:
High-level Le Fort I ± only bone grafts (or Le Fort II/III in selected cases) applications; Suborbital/malar implants; and Camouflage procedures such as soft tissue augmentation (fat grafts) should be recommended to ensure the harmony of the face.
Since the orbitomalar region shows a moderate positive correlation with the anterioposterior positions of the maxilla and mandible, careful analysis of the orbital and malar regions is also required in patients with CLP with anteroposterior positioning disorders in the maxilla and mandible or with increased maxillary inclination.
The results of this study will guide future correlation studies with a broader set of craniofacial parameters for projection analysis of this region.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The informed consent was obtained from the parents of the patients whose photographs were used in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.