
Abstract
Objective
This study evaluates long-term outcomes in adults with Unilateral and Bilateral Cleft Lip and Palate (UCLP/BCLP) treated during the period 1992 to 1995 with tibial periosteal graft in primary repair.
Design
Retrospective study.
Setting
Department of Plastic and Maxillofacial Surgery, Children's Hospital Bambino Gesù (Italy).
Patients
The study included 52 patients with non-syndromic BCLP/UCLP who met the inclusion criteria.
Interventions
All patients underwent a standardized surgical protocol using a tibial periosteal graft as primary repair of the hard palate.
Main Outcome Measure(s)
Long-term outcomes on maxillary growth, residual oronasal fistula, and leg length discrepancy.
Results
About <2% of patients showed oral–nasal communication. Mean value of maxillary depth was 86° ± 4.5°. The lower value for maxillary retrusion was 76.8° in relation to the Frankfurt plane. At the x-ray control, 12.2% of patients showed leg discrepancy with a difference of always <2 cm.
Conclusions
The rate of maxillary retrusion obtained was the same if compared to other techniques. Tibial periosteal graft reduces the risk of fistula and the need for reintervention after secondary bone graft. The study did not observe negative impacts on leg growth after 25 years.
Keywords
Introduction
Reconstruction of the hard palate has always been controversial in the surgical treatment of patients with Cleft Lip and Palate (CL/P). While, on the one hand, CL repair presents standardized protocols and surgical procedures, on the other hand, there is no definitive consensus for CP repair, regarding proper timing, sequence of the hard palate and soft palate closure, and choice of the surgical technique. One of the main areas of debate regarding surgical timing concerns the feasibility to develop good speech skills through an early closure of CP without impairing maxillary growth.
Until 1995, under the direction of Professor Lucio Standoli, the Cleft Center of the Children's Hospital Bambino Gesù used to perform primary repair in a single procedure using a periosteal tibial graft according to a modified Stricker technique.1, 2 The rationale of the technique was to reconstruct the hard palate through bone deposition obtained by placement of the periosteal graft along the alveolar and hard palatal cleft and to enhance bone growth since the initial time of lip reconstruction. 2 The initial results obtained with this technique have not brought to a statistically significant validation because of the young age of the patients and the short-term evaluation.
Therefore, the aim of this study is to investigate and objectively evaluate the long-term outcomes in unilateral or bilateral Cleft Lip and Palate (UCLP/BCLP patients (25-year follow-up) who underwent surgery using a tibial periosteal graft in primary repair.
Materials and Methods
In this study, we conducted a retrospective analysis on patients with CL/P who underwent surgery at Children's Hospital Bambino Gesù in the period between 1992 and 1995
Through a retrospective analysis of medical records, we initially identified 108 patients. In this regard, we considered the following inclusion criteria:
Patients with complete CL/P (UCLP/BCLP); Tibial periosteal graft as primary surgical repair of the hard palate. Incomplete medical records; Incomplete follow-up; Patients with syndromic disorders; Refusal of the patient.
We considered the following exclusion criteria:
Eventually, 36 patients were lost to follow-up, 9 were excluded due to syndromic disorders and 11 refused to participate in the study. Finally, 52 patients were included in the study.
We performed long-term evaluations to investigate maxillary/mandible growth, oronasal fistula rate, lower limb discrepancy and final aesthetical appearance.
The project was performed according to the principles expressed in the Declaration of Helsinki. Written patient consent was obtained. The Ethical Committee of the Children's Hospital Bambino Gesù granted ethical approval.
Surgical Technique
Lip incisions were made according to Tennison-Randall or Millard techniques in both UCLP/BCLP cases (see Supplemental Video).
Primary rhinoplasty was done only in UCLP according to the McComb technique, avoiding marginal incision of the nostril and using the same incisions of the lip repair procedures; dissection was done through the base of the columella and the alar base. No primary rhinoplasty was performed in BCLP at that time.
Lip incisions were then continued toward the hard palate of the cleft side and along the vomer on the non-cleft side and thereafter along the margins of the soft palate cleft. In BCLP, a bilateral vomer flap, one on each side, was raised.
Relaxing incisions (according to Von Langenbeck palatoplasty) were performed along the lateral edges, and 2 mucoperiosteal flaps were raised and elevated from the oral surface of the hard palate. The nasal sides of the cleft were sutured first on the midline to obtain a complete reconstruction of the nasal layer of the hard palate.
For soft palate repair, we adopted a modified Furlow procedure, which included a Z-plasty only on the nasal layer. On one side of the cleft, the muscle layer was identified and elevated, and only the mucosal Z-flap was raised; on the opposite side, a complete muscle-mucosal Z-flap was raised. After transposing and suturing the two Z-flaps, the elevated muscle was sutured and solidarized with the controlateral of the other cleft side. The oral layer of the soft palate was then sutured on the midline up to the posterior nasal spines.
At the same time, a second team worked on the periosteal graft. We performed a transversal skin incision (about 5 cm in length) on the middle of the anterior surface of the leg, we dissected until identification of the periosteum, which was harvested in a rectangular shape (about 4 × 2.5 cm).
At this point, the tibial periosteal graft was placed over the nasal layer of the hard palate and sutured from the posterior nasal spines up the piriform aperture, with the osteogenic surface facing the nasal layer and the other side left uncovered. The lateral edges of the graft were inserted with transfixing stitches beneath the borders of the palatal mucoperiosteum, and the proximal extremity was inserted along the piriform aperture.
Lip closure was completed after orbicularis oris muscle reconstruction, and the alar cartilages were sutured in the new position with external stitches.
A nasal stent was used and kept in place for at least 1 month.
Clinical Evaluation
Anamnestic and clinical data were collected at the preoperative and postoperative follow-ups.
Demographic data (age, sex), clinical data (UCLP/BCLP, age of first surgery, comorbidities), and surgical data (number of surgical steps, postoperative complications, and secondary corrective surgeries) were surveyed for the treated cases. The variables were described in terms of frequencies, means, and standard deviations (SDs).
Maxillary Growth Evaluation
Maxillary growth has been examined through cephalometric analysis performed at the completion of growth (range: 18-25 years old) and always before any orthognathic corrective surgery. Lateral cephalograms were taken with the head oriented parallel to the Frankfurt plane. All the lateral cephalograms were captured in accordance with a standardized procedure and orientated at 7° to the Sella-Nasion plane prior to landmark identification, to increase reproducibility and reliability. Through the Dolphin Imaging Software, a maxillofacial surgeon carried out cephalometric analysis based on Ricketts and Steiner criteria in order to evaluate facial growth.3–5 To assess the position of the maxilla at the end of growth in a sagittal and vertical plane, we took as baseline reference values presented in Table 1.
Cephalometric Parameters Analyzed for Maxillary Growth Evaluation.
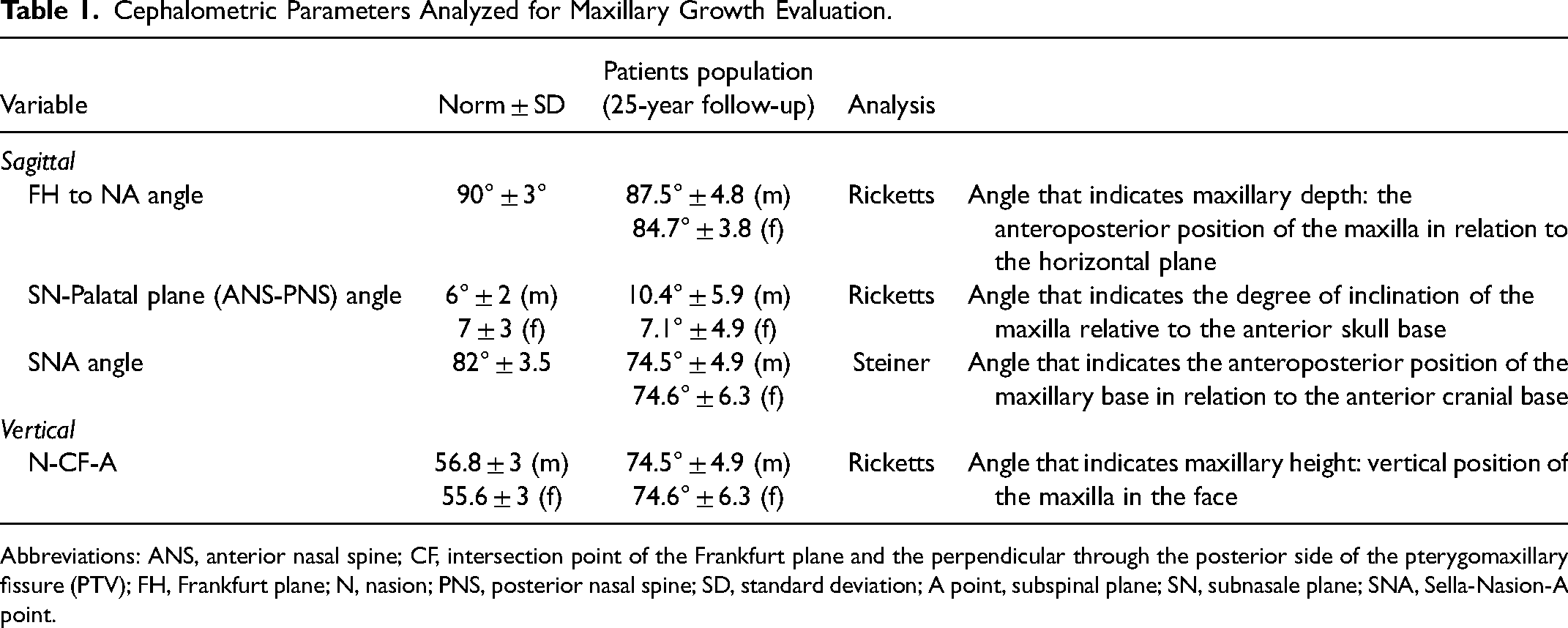
Abbreviations: ANS, anterior nasal spine; CF, intersection point of the Frankfurt plane and the perpendicular through the posterior side of the pterygomaxillary fissure (PTV); FH, Frankfurt plane; N, nasion; PNS, posterior nasal spine; SD, standard deviation; A point, subspinal plane; SN, subnasale plane; SNA, Sella-Nasion-A point.
Cephalometric parameters were tested for normality. The Kolmogorov–Smirnov test was used to determine the normal distribution of cephalometric variables. The values of the 4 cephalometric angles, calculated on the basis of our study population and stratified by gender, were described in means and SDs.
We tried to see if there were any variations in cephalometric measurements that could be related to the initial CLP diagnosis (ULCLP/BLCLP).
Moreover, we compared the Sella-Nasion-A point (SNA) angle obtained from our population to values reported by other Cleft Center groups (Table 2).
Mean Value for SNA in Comparison with Values of Main World Cleft Centers.

Abbreviations: SD, standard deviation; SNA, Sella-Nasion-A point.
Leg Discrepancy Evaluation
Radiography is the primary imaging modality for the evaluation of leg length discrepancy. 6 Standing full-length anteroposterior computed radiographs of the lower limbs were all assessed by the same radiologist. A leg discrepancy between 0 and 2 cm is considered a normal range. 7
Results
Clinical Evaluation
We recruited 52 non-syndromic patients (25 females and 27 males) in the study, 39 (75%) with UCLP and 13 (25%) with BCLP. Median age at the time of the first surgery was 8 months (interquartile range: 7-10 months).
The surgical procedure was performed by the same surgeon and consisted of 1 surgical step in all the UCLP cases or 2 surgical steps, when needed in BCLP cases with an excessive cleft width (11 BCLP—85%). A total of 63 periosteal grafts were performed in 52 patients. No graft failures were recorded.
Surgeon preference for periosteum harvesting was from the right leg: 44 (85%) patients showed a scar on the right leg, 7 (13%) patients on the left leg, and only 1 (2%) bilateral patient on both legs.
Median age at follow-up was 25 years old (interquartile range: 24.5-26.5).
Thirty-two (62.5%) patients underwent secondary rhinoplasty.
During clinical examination, no patient showed oro–nasal communication. The occurrence of a fistula was reported in the medical history of 3 patients (5.7%): 2 of these resolved spontaneously, while 1 (2%) required secondary surgery for fistula closure.
Between the ages of 8 and 12 years, 42 (80.7%) patients received a secondary alveolar bone graft (SABG) from the iliac crest. Among them, none underwent regrafting.
Ten (20.3%) patients did not require any SABG since we highlighted enough bone formation to allow proper teeth migration according to our orthodontist.
Fourteen (27%) patients underwent orthognathic surgery.
Maxillary Growth Evaluation
The results of cephalometric angular measurements are shown in Table 1 with sex-dependent differences analyzed in Figure 1. A P value of less than 0.05 was considered significant.

Cephalometric measurements for maxillary growth evaluation: (A) Maxillary depth in male and female patients (P < 0.05), (B) SN-Palatal plane angle in male and female patients (P < 0.05), (C) SNA angle in male and female patients (P = 0.94), and (D) maxillary height in male and female patients (P = 0.3).
While maxillary depth (P = 0.02) and SN-Palatal plane angle (P = 0.04) showed a statistically significant sex difference, the SNA angle (P = 0.94) and maxillary height (P = 0.3) did not result in a statistically significant sex difference.
We observed that out of the 32 patients (61%) showing values of maxillary depth inferior to normal ranges, 7 patients had BCLP and 25 had UCLP. However, the difference was not statistically significant (P =0 .3).
Neither the values of maxillary height (P =0 .9) nor those of SN-Palatal plane angle (P =0 .4) presented a statistically significant difference in UCLP and BCLP.
From the comparison of SNA angles (Table 2), our SNA mean value was found to be not significantly different from values reported by other groups.
Leg Discrepancy Evaluation
Six patients (12.2%) showed leg discrepancy at the x-ray control: 5 involving the right lower limb, 1 the left lower limb. The longer leg was always used for the tibial periosteum harvesting. The leg difference was always <2 cm and did not affect the patient’s posture nor walking.
Discussion
CL/P treatment varies among different worldwide Cleft Centers and requires long-term evaluation. 8 According to Knight et al., the 3D repair of CL/P requires a proper understanding of facial modifications that occur during growth and thus anticipation of changes in the fourth dimension that can be determined by periodic and objective evaluations. 9 Therefore, the most important assessment needs to be done at the end of growth, considering the following as paramount goals of treatments: normal socialization, normal appearance, normal speech, no oronasal fistula, normal skeletal growth, and reduction of the number of surgical procedures.
Our study analyzes the overall and specific results obtained at the end of growth (25-year follow-up) using the tibial periostioplasty protocol used in our Cleft Center until 1995. 2
The prevalence of fistula after primary palatoplasty reported in the literature ranges from 2% to 45%.9–15 In our series, the incidence of fistula resulted <2%.
According to Smarius and Breugem, the incidence of fistulas is an important indicator of a successful CP repair technique. Their overall fistula rate was 4% (von Langenbeck technique/vomer flap). 16
Becker and Hansson reported a rate of 5% (von Langenbeck technique/vomer flap). 17 Sommerlad highlighted his fistula rate of 15% (vomer flap). 18 Lin et al. reported 17% (two-flap palatoplasty). 19 Kahraman et al. (Veau-Wardill-Kilner) reported 17.7% 20 and Abdurrazaq et al (Langenbeck) 29.8%. 21
These different percentages were linked to initial cleft width and plastic surgeon's experience.22, 23 The type of cleft and its extension are variable and implicate the growth trajectory, which becomes unpredictable. 24 Maxillary growth varies among patients and depends on individual genetic factors. Each surgeon usually performs the procedure that has been learned, based on the school of thought where the training was done.22–24
We think that performing a periosteal tibial graft can minimize the above-mentioned bias. The low rate of fistula observed in our series should not be associated with initial cleft width or plastic surgeon's experience, but rather with the surgical technique that allows reduction of tension on the midline and satisfactory bone production.
Together with the risk of fistula, the main discussion concerns the development of maxillary hypoplasia. 25 The evidence that unoperated patients with CL/P showed normal maxillary growth has brought over time different authors to discuss the possibility of delaying hard palate repair in order to minimize the effect on maxillary growth.26–28 However, the delay of complete palatal cleft until 2 to 5 years of age carries a risk of inadequate speech development for many patients. In 1984, Witzel et al. and later in 2007, Holland et al. underlined that patients with delayed primary repair result in severe speech problems both before and after closure of the hard palate.28, 29 In addition, the evidence of improved maxillary growth was hardly convincing.28, 29 So, most of the world's Cleft Centers repair the hard palate within the first year of age.
Different surgical protocols have been shared and performed by different surgeons around the world.30–32 Nevertheless, there are significant controversies about the repair of the hard palate, the use of vomerine flap, and there are contradictory data available in the literature regarding the effect on maxillary growth.33, 34
The CL/P population tends to have a smaller length of maxilla sagittally, and this deformity progresses with age, 35 reaching around 68.97% showing maxillary retrusion. 36 In Standoli cases, 60% of patients showed maxillary retrusion compared with the normal population. Maxillary growth does not seem different from values submitted by other groups, with the exception of Oslo and Sommerlad, which provided, though, results only at 10 and 11 years of age, which are not sufficient for a definitive facial growth evaluation (Table 2).25, 32, 35–37
The better closure of the piriform aperture on the cleft side, visible at the x-ray controls, is an advantage highlighted in our review. The longitudinal placement of the tibial periosteal graft, from the posterior nasal spines to the piriform aperture, allows a clear separation between the oral and nasal spaces. As reported in the study by Losee and Smith, 38 which showed positive outcomes of acellular dermal matrix in palatoplasty, we believe that tibial periosteal graft could lead to a successful management of alveolar clefts. The hermetic sealing of nasal space and the creation of a three bony wall pocket lead to better chance of intake and and less resorption of the bone graft. Our study population, indeed, underwent alveolar bone grafting without the need for revision procedures. The evidence of newly formed bone allowed proper teeth migration and dentomaxillary development.
Other criticism raised against the periosteal graft technique concerns the potential negative interference with leg growth. The scar on the anterior side of the leg always appeared to be of good quality, and its transversal direction with respect to the longitudinal axis of the lower limb avoided scar stretching. When leg discrepancy was found, the longer leg was always used for the tibial periosteum harvesting, as disruption of periosteum has been largely demonstrated to accelerate growth in the developing skeleton. 39
The leg difference was always found to be <2 cm and, as shown through our follow-up and as stated in the literature, there seems to be a consensus in considering a small amount of length discrepancy not a problem for limb function.7, 40
Conclusion
Long-term results of tibial periosteal graft as primary repair of CL/P have allowed us to overcome controversies and reluctance against an effective but not sponsored technique, leading to the conclusion that it represents a valid option for reconstruction in CL/P. The examined 25-years-old patients showed fistula rate close to 0, skeletal growth comparable to the other techniques, with no evidence of impairment in leg growth. These outcomes were obtained using a technique that is easy to handle with the further advantage of a single-stage operation.
Looking to the future, on the basis of ongoing studies we are conducting in the fields of regenerative medicine and tissue engineering, we believe that the implementation of this technique could lead to great advances in CL/P repair.
Supplemental Material
sj-avi-1-cpc-10.1177_10556656221132043 - Supplemental material for 25-year Follow-up of Primary Tibial Periosteal Graft for Hard Palate Repair in Cleft Lip and Palate: Outcomes, Concerns and Controversies
Supplemental material, sj-avi-1-cpc-10.1177_10556656221132043 for 25-year Follow-up of Primary Tibial Periosteal Graft for Hard Palate Repair in Cleft Lip and Palate: Outcomes, Concerns and Controversies by Maria Ida Rizzo, Marta Cajozzo, Daria Bucci, Angelica Pistoia, Annapina Palmieri, Oriana Rajabtork Zadeh, Giancarlo Palmieri, Giorgio Spuntarelli and Mario Zama in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-pdf-2-cpc-10.1177_10556656221132043 - Supplemental material for 25-year Follow-up of Primary Tibial Periosteal Graft for Hard Palate Repair in Cleft Lip and Palate: Outcomes, Concerns and Controversies
Supplemental material, sj-pdf-2-cpc-10.1177_10556656221132043 for 25-year Follow-up of Primary Tibial Periosteal Graft for Hard Palate Repair in Cleft Lip and Palate: Outcomes, Concerns and Controversies by Maria Ida Rizzo, Marta Cajozzo, Daria Bucci, Angelica Pistoia, Annapina Palmieri, Oriana Rajabtork Zadeh, Giancarlo Palmieri, Giorgio Spuntarelli and Mario Zama in The Cleft Palate Craniofacial Journal
Footnotes
Author’s Note
The manuscript was presented at the European Meeting organized by the European Cleft Palate Craniofacial Association (ECPA) in 2019 in Utrecht (Netherlands) and at the National Meeting of the Italian Society of Plastic Reconstructive and Aesthetic Surgery (SICPRE) in 2019 in Palermo (Italy).
Author’s Contribution
The manuscript has been read and approved by all the authors; the requirements for authorship have been met; and each author believes that the manuscript represents honest work.
Author Note
Daria Bucci, School of Medicine, Vita-Salute San Raffaele University, Milan, Italy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.