
Abstract
Objective
To describe the process of developing a craniosynostosis decision aid.
Design
We conducted a mixed-methods exploratory study between August 2019 and March 2020 to develop a decision aid about surgical treatment for single suture craniosynostosis.
Setting
A single tertiary care academic children’s hospital.
Participants
The decision aid development team consisted of surgeons, research fellows, a clinical nurse practitioner, clinical researchers with expertise in decision science, and a university-affiliated design school. Qualitative interviews (N = 5) were performed with families, clinicians (N = 2), and a helmeting orthotist to provide feedback on decision aid content, format, and usability.
Interventions
After cycles of revisions and iterations, 3 related decision aids were designed and approved by the marketing arm of our institution. Distinct booklets were created to enable focused discussion of treatment options for the 3 major types of single suture craniosynostosis (sagittal, metopic, unicoronal).
Results
Three decision aids representing the 3 most common forms of single suture craniosynostosis were developed. Clinicians found the decision aids could help facilitate discussions about families’ treatment preferences, goals, and concerns.
Conclusions
We developed a customizable decision aid for single suture craniosynostosis treatment options. This tool lays the foundation for shared decision-making by assessing family preferences and providing clear, concise, and credible information regarding surgical treatment. Future research can evaluate this tool’s impact on patient–clinician discussions about families’ goals and preferences for treatment.
Introduction
Shared decision-making (SDM) is a process by which patients and practitioners communicate to reach medical decisions based on patient-specific factors and the best available evidence.1–3 SDM supports patients and their families such that they are informed and involved in making important medical decisions with clinical equipoise or trade-offs between benefits and drawbacks of options. 3 SDM is often used in conjunction with a decision aid when engaging in health decisions. The purpose of decision aids is to enhance the physician-family encounter and facilitate SDM rather than replace it. 4 Decision aids can be versatile and take on several forms such as videos, pamphlets, online booklets, or interactive media to suit the clinical scenario. 4
Little is known about the role of SDM in facilitating the physician-family discussion about surgical management of patients with craniosynostosis. Multiple options exist for the treatment of single suture craniosynostosis and no single procedure stands out as clearly superior.5–12 There is significant variability in the presentation of surgical options during the physician-family discussion, and physicians might influence decisions based on their own bias or preferences.13,14
Three popular surgical methods for repair of single suture craniosynostosis are open cranial vault remodeling, spring-assisted craniectomy, and endoscope-assisted craniectomy with postoperative molding helmet therapy.15–18 Both open and endoscopic repairs may be used in patients under 5 months of age, but each has specific benefits and challenges. The advantages of endoscopic repair include shorter duration of surgery, decreased blood loss, and faster recovery.1,8,19–21 Frequent postoperative visits are required, however, to manage the helmet molding therapy. In contrast, while spring-assisted craniectomy does not require post-operative helmeting, all patients undergoing spring-assisted craniectomy will require a second operation for spring removal. 18 Open cranial vault remodeling, spring-assisted craniectomy, and endoscope-assisted craniectomy have shown comparable clinical outcomes for head shape correction in single suture craniosynostosis.7,10,22–27 When a patient is eligible for multiple surgical approaches, SDM is appropriate to assist the family and physician in choosing the procedure that best aligns with their clinical needs, care goals, and preferences.
At our institution, open cranial vault remodeling and endoscope-assisted craniectomy are offered to eligible patients less than 6 months of age for metopic and sagittal and under 5 months for unicoronal synostosis. Prior to developing this tool, our preoperative counseling process was not standardized across surgeons. Practice patterns also vary widely among practitioners at other craniofacial centers. 13 According to a survey distributed to 26 clinicians at high-volume craniofacial centers, surgeons use a wide range of approaches in presenting the choice of repair technique. 13 Additionally, there is variation in the extent to which SDM is used during clinic visits. While 22 of 26 surgeons believe they use SDM in guiding families to a decision, about 44% strongly or somewhat strongly steer families to their preferred surgical option. This suggests that many practitioners find it difficult to apply SDM fully and impartially. A decision aid could facilitate SDM or augment existing decision-making approaches, leading to more personalized and individualized healthcare. The purpose of this paper is to describe the systematic process of creating a decision aid to augment the SDM process for the treatment of craniosynostosis.
Methods
After approval from the Institutional Review Board (201906139), creation of the decision aid was conducted within a single tertiary care children’s hospital from August 2019 to March 2020. See Figure 1 for a timeline describing the development of the decision aid and Figure 2 for a schematic illustrating the overall process of development.
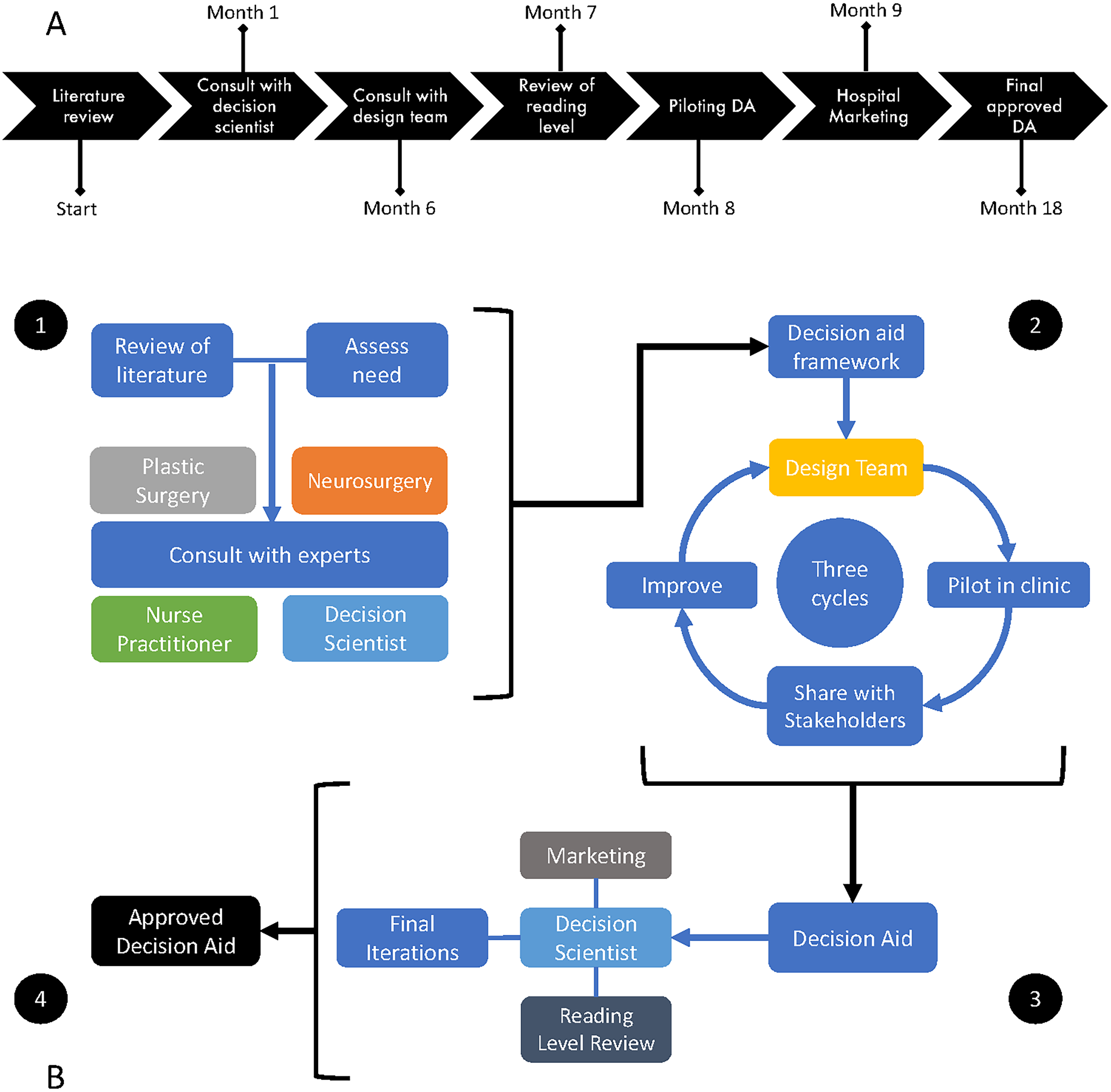
(A) A timeline depicting the process of decision aid development. (DA: decision aid). (B) A structured iterative process was used to develop a decision aid for the treatment of single suture craniosynostosis. The process began with a review of current literature and assessment of the need for a decision aid. Consulting with experts is necessary to formulate a framework of content to be included in the decision aid. Once the framework and content were finalized, the design team developed the decision aid after 3 modified plan-do-study-act cycles. The decision aid was reviewed by our decision scientist and medical librarian to ensure that the reading level was appropriate. Finally, the hospital marketing team made minor stylistic changes to the decision aid to match the themes of other informational booklets.
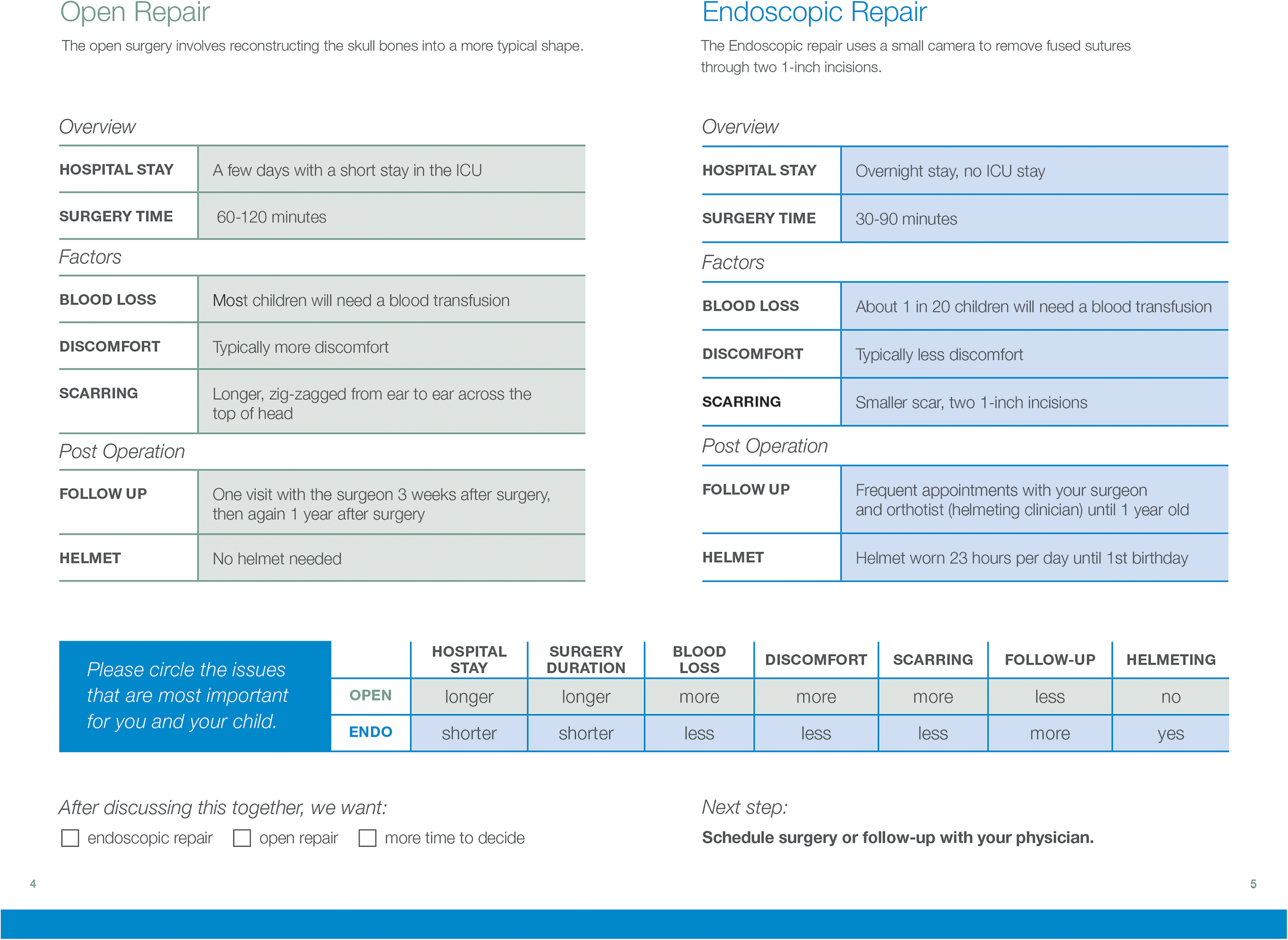
The center fold provides a head to head comparison of the open and endoscopic repair for sagittal synostosis. Using this chart, the physician is able to identify issues that are most important to the family and then guide the family to the treatment option that best fits their values and goals.
Development of Initial Content
The foundations of the decision aid were developed by reviewing literature and aggregating the known risks and benefits of both endoscopic and open repair. The literature review was performed by using the PubMed.gov database and the following search terms: outcomes, school age outcomes, craniosynostosis, endoscopic repair, open repair, sagittal, metopic, coronal, decision aid, decision tool, SDM were used. Decision aid prototypes were then developed in collaboration with the University’s affiliated School of Design and Visual Arts. After obtaining feedback on the prototypes from our lead craniofacial surgeon, neurosurgeon and clinical nurse practitioner, a version of the tool was created for testing. This new printed decision aid was then piloted by our physicians in our craniofacial clinic during the iterative production phase. Overall, the decision aid was piloted in clinic during 3 separate clinical encounters during this production phase. Physicians used the decision aid to facilitate the SDM process and then provided qualitative feedback in addition to feedback from families to guide future versions of the decision aid.
Engage Stakeholders and Advisors
The development team was based at our institution and consisted of a design team from the university-affiliated design school, clinical researchers with expertise in pediatric plastic surgery and decision science, 2 plastic surgery research fellows, 1 craniofacial plastic surgeon, 1 pediatric neurosurgeon, and 1 clinical nurse practitioner with a specialty in craniofacial anomalies.
To develop the craniosynostosis treatment booklets, the project development and improvement team reviewed existing decision aids, 28 performed qualitative interviews with families (N = 2) and physicians (N = 2), a craniofacial research fellow, and helmeting orthotist, and directly observed clinical encounters. Additionally, we used the International Patient Decision Aid Standards (IPDAS) checklist as a guide to systematically develop the decision aid with a focus on content, development process, and effectiveness. 4 The project development and improvement team prioritized family education about the diagnosis and treatment of craniosynostosis, risks and benefits of each procedure, and follow-up care.
Once the basic content for the first prototype was agreed upon, we began the design phase. We aimed to create a booklet with illustrations to depict the written content. The content explained the advantages and disadvantages of endoscopic and open repair as reported in the literature, the important points to consider when deciding between surgical options, and next steps after making that decision. A medical librarian was consulted to simplify the text to be at or below a 9th grade reading level. Prototype decision aids were critiqued by our development team and tested using plan-do-study-act (PDSA) cycles during outpatient clinical encounters PDSA directions. 29 Feedback for revisions was elicited during weekly meetings with the development team and relayed to our design team. After 3 major revisions (a total of 4 iterations), our stakeholders found the pamphlets acceptable for use in the clinic. See Figure 1 for the development timeline.
Pilot Test in Practice
After observing physician workflow, it was decided that the decision aid would be introduced at the end of a standard consultation in order to efficiently summarize the consultation and proceed with the decision-making portion of the visit. Once the routine presentation introducing the diagnosis of craniosynostosis and the treatment options was completed, the physician would present the decision aid to reiterate the risks and benefits of each surgical approach. Then, the physician would prompt the family to circle the 3 issues most important to them regarding surgery: hospital stay, surgery duration, discomfort, blood loss, scarring, follow-up (number of post-operative visits in 1 year), or helmeting (Figure 2). At this point, the physician could highlight the treatment option most appropriate for the patient and family given the specific issues deemed most important by the family. After reviewing the decision aid and discussing the information, the family and physician could choose to schedule a date for surgery or take more time to weigh the options and schedule follow-up.
Conduct Qualitative Interviews With Users
Follow-up semi-structured qualitative interviews with families (N = 4) and practitioners (N = 2) were done to assess the effectiveness of the decision aid on select parameters: content, readability, usability, acceptability, and lack of bias. Families found the decision aid to be a concise and useful tool, which explained craniosynostosis clearly and presented the treatment options in a brief but accurate fashion. Pages 4 and 5 (Figure 2) were especially useful to discuss the pros and cons of each surgery. Physicians had the opportunity to ask families to identify the issues most important for them and their child. Blood loss was the most commonly cited concern among families, followed by the need for post-operative helmeting and presences of post-operative scar. Other concerns cited by families included length of hospital stay, surgery duration, and discomfort. The main changes and improvements resulting from iterations and feedback were regarding words noted to be “scary” and potentially confusing by families. For example, “pain” was changed to “discomfort,” “premature” was changed to “early.” Percentages were converted to frequency. About 5% of children will need a blood transfusion was changed to 1 in 20 will need a blood transfusion. Feedback from families and practitioners was positive and simplification of language was noted to facilitate a more streamline discussion during the initial clinical encounter.
Results
Three craniosynostosis booklets (Supplemental Material) were created to enable physicians and families to efficiently discuss treatment options for the 3 most common types of craniosynostosis (sagittal, metopic, and unicoronal). Using pictorial representations of the affected suture and plain language, the booklets explained the diagnosis of each type of synostosis. An overview of the advantages and disadvantages of open and endoscopic repairs was located in the center-fold. Representative before and after photographs of each type of repair were included. The booklets also included frequently asked questions that families could refer to regarding helmeting or postoperative care.
Discussion
The aim of this project was to develop and implement a decision aid to facilitate SDM between physicians and families with children affected by single suture craniosynostosis. This aid is not a stand-alone tool and relies on the clinician to elaborate on certain aspects of the decision aid during the initial clinical encounter. This decision aid was developed using an iterative participatory design approach to fit the needs of families and physicians. Our unique multidisciplinary approach allowed for a rapid and comprehensive development. Each professional contributed their expertise to streamline the initial prototypes in collaboration with other members of the multidisciplinary team. Throughout this process, we referred to the IPDAS checklist as a framework to develop high quality content, maintain an organized development process, and ensure effectiveness of the decision aid.
In this paper, we present a 1-year timeline for production of a decision aid that was created in conjunction with families and stakeholders, meeting the needs of both parties. In order to develop this decision aid, a multi-disciplinary team consisting of clinicians and experts in graphic design, decision science, and medical language was assembled. Through several revision and iteration cycles, the decision aid was crafted and approved by the marketing arm of our institution. We acknowledge that bias is a valid concern regarding creation of a decision aid. During the initial visit, there is an extensive discussion that occurs between the physician and family regarding treatment options that is not reflected when analyzing the decision aid alone. For example, the burden of post-operative endoscopic care such as the burden of helmeting, cost associated with helmeting, and more frequent visits are heavily discussed under the need for helmeting in the endoscopic repair section.
Ultimately, our goal was to develop a customizable, accessible, and practical decision aid with the aim of educating families by providing convenient, evidence-based, and concise information about treatment options for single suture craniosynostosis. The decision aid functions to guide SDM between the physician and family and can be adjusted as new studies emerge regarding neurodevelopmental outcomes for this patient population or improved via user feedback. The decision aid itself was developed to be published and tailored to the unique surgical protocols of other craniofacial institutions. It is our current practice to ask families to identify at least 3 issues most important to them regarding the surgical treatment of their child’s craniosynostosis. This information is recorded and will be used to tailor future consultations and inform care.
Conclusion
The process of SDM works best when there is clinical equipoise between 2 or more surgical treatment options. We developed a customizable decision aid for the surgical treatment of single suture craniosynostosis which promotes SDM by assessing family preferences and by providing clear, concise, and credible information regarding the 2 surgical options. Investigators can use this study as a reference and guide to develop decision aids in the future. Further studies can evaluate the decision aids in a randomized trial to examine its impact on SDM and families’ decision quality.
Supplemental Material
sj-jpg-1-cpc-10.1177_10556656221128413 - Supplemental material for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis
Supplemental material, sj-jpg-1-cpc-10.1177_10556656221128413 for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis by Abdullah M. Said, Ema Zubovic, Kristin D. Pfeifauf, Gary B. Skolnick, Jude Agboada, Penina Acayo-Laker, Sybill D. Naidoo, Mary C. Politi, Matthew Smyth and Kamlesh B. Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-2-cpc-10.1177_10556656221128413 - Supplemental material for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis
Supplemental material, sj-jpg-2-cpc-10.1177_10556656221128413 for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis by Abdullah M. Said, Ema Zubovic, Kristin D. Pfeifauf, Gary B. Skolnick, Jude Agboada, Penina Acayo-Laker, Sybill D. Naidoo, Mary C. Politi, Matthew Smyth and Kamlesh B. Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-3-cpc-10.1177_10556656221128413 - Supplemental material for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis
Supplemental material, sj-jpg-3-cpc-10.1177_10556656221128413 for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis by Abdullah M. Said, Ema Zubovic, Kristin D. Pfeifauf, Gary B. Skolnick, Jude Agboada, Penina Acayo-Laker, Sybill D. Naidoo, Mary C. Politi, Matthew Smyth and Kamlesh B. Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-4-cpc-10.1177_10556656221128413 - Supplemental material for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis
Supplemental material, sj-jpg-4-cpc-10.1177_10556656221128413 for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis by Abdullah M. Said, Ema Zubovic, Kristin D. Pfeifauf, Gary B. Skolnick, Jude Agboada, Penina Acayo-Laker, Sybill D. Naidoo, Mary C. Politi, Matthew Smyth and Kamlesh B. Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-5-cpc-10.1177_10556656221128413 - Supplemental material for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis
Supplemental material, sj-jpg-5-cpc-10.1177_10556656221128413 for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis by Abdullah M. Said, Ema Zubovic, Kristin D. Pfeifauf, Gary B. Skolnick, Jude Agboada, Penina Acayo-Laker, Sybill D. Naidoo, Mary C. Politi, Matthew Smyth and Kamlesh B. Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-6-cpc-10.1177_10556656221128413 - Supplemental material for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis
Supplemental material, sj-jpg-6-cpc-10.1177_10556656221128413 for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis by Abdullah M. Said, Ema Zubovic, Kristin D. Pfeifauf, Gary B. Skolnick, Jude Agboada, Penina Acayo-Laker, Sybill D. Naidoo, Mary C. Politi, Matthew Smyth and Kamlesh B. Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-7-cpc-10.1177_10556656221128413 - Supplemental material for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis
Supplemental material, sj-jpg-7-cpc-10.1177_10556656221128413 for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis by Abdullah M. Said, Ema Zubovic, Kristin D. Pfeifauf, Gary B. Skolnick, Jude Agboada, Penina Acayo-Laker, Sybill D. Naidoo, Mary C. Politi, Matthew Smyth and Kamlesh B. Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-8-cpc-10.1177_10556656221128413 - Supplemental material for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis
Supplemental material, sj-jpg-8-cpc-10.1177_10556656221128413 for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis by Abdullah M. Said, Ema Zubovic, Kristin D. Pfeifauf, Gary B. Skolnick, Jude Agboada, Penina Acayo-Laker, Sybill D. Naidoo, Mary C. Politi, Matthew Smyth and Kamlesh B. Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-9-cpc-10.1177_10556656221128413 - Supplemental material for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis
Supplemental material, sj-jpg-9-cpc-10.1177_10556656221128413 for Shared Decision-Making: Process for Design and Implementation of a Decision Aid for Patients With Craniosynostosis by Abdullah M. Said, Ema Zubovic, Kristin D. Pfeifauf, Gary B. Skolnick, Jude Agboada, Penina Acayo-Laker, Sybill D. Naidoo, Mary C. Politi, Matthew Smyth and Kamlesh B. Patel in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
The authors thank Mychal Voorhees, Eve Wallack, Amanda Im, Lianne Kang, Ali White, and Kristina You. The authors would like to thank the St. Louis Children’s Hospital Foundation Board for their support of the Washington University School of Medicine Cleft Palate Craniofacial Institute.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.