
Abstract
Objective
This study aimed to propose digitally designed impression trays, for newborns with cleft lip and palate (CLP) defects, using the computer-assisted design and manufacturing (CAD/CAM) technique, based on measurements of width, length, and height made on processed and scanned plaster models. Thus, we will describe the different software and concepts that can be used for the design of these impression trays.
Design
A total of 59 plaster casts of newborn patients with CLP were collected and then scanned. After that, digital dental casts were three-dimensional (3D) evaluated, using precise anatomical landmarks.
Setting
The Maxillofacial Prosthodontics Team at the Dental consultation and treatment center in Rabat, Morocco.
Patients and Participants
The study involved plaster casts of newborns with CLP, who had undergone presurgical neonatal treatment in the Maxillofacial Prosthodontics service in Rabat, Morocco.
Interventions
None,
Main Outcome Measure(s)
3D evaluation of 59 scanned plaster casts of newborn patients with CLP.
Results
This work allowed us to obtain digital impression trays for each anatomical variation of orofacial clefts. These trays will limit the problems linked to conventional techniques for making neonatal orthopedic plates. We also emphasized the importance of a multidisciplinary approach involving several professionals in Morocco from various fields and specialties.
Conclusion
This original technique is advantageous for the practitioner as well as for the patients and their parents. It allows for precise recording, better adaptation, time-saving, and parental comfort.
Introduction
Cleft lip and palate (CLP) are the most common craniofacial birth defects. The management of these anomalies requires a multidisciplinary approach. Maxillofacial prosthodontists play an important role in the preoperative orthopedic management of patients with CLP, by providing orthopedic appliances, including palatal and nasal conformation.1,2
Orthopedic procedures associates any type of presurgical neonatal treatment of nasolabial deformities attributed to infants with CLP. 3
Many maxillary orthopedic appliances have been described in the literature. The most used are maxillary passive and active appliances and presurgical nasoalveolar molding (PNAM).
Passive appliances or feeding obturator/plate are simple maxillary plates that restore the communication between the nasal and oral cavities caused by the cleft, facilitate feeding and breathing, and avoid the interposition of the tongue in the cleft.
Whereas, active appliances apply force to the jaw segments using an active force transmission system, such as a verrin system. This appliance can be used to treat patients with bilateral cleft lip and palate (BCLP). It aims to reposition the protruding premaxilla helping to bring the cleft together. As a result, it facilitate the surgical treatment.4,5
PNAM was at first proposed by Grayson and Cutting and it consists of molding presurgically the alveolus, the lip, and the nose.
Several benefits of PNAM have been reported in the literature. The authors confirmed that these devices decrease the cleft width and improve nasal symmetry and postoperative results.2,6,7
Impression taking is a crucial step in this early treatment, and the conventional technique is a process that involves a lot of risks. Inadequate impression trays can lead to alteration of the fibromucosa, which is still fragile and sensitive; respiratory obstruction can also occur due to fragmentation of the impression material. 5
Nowadays, digital techniques of computer-aided design and manufacturing (CAD/CAM) and rapid prototyping have enabled relevant progress in dentistry, especially in Maxillofacial Prosthodontics. The introduction of digital technologies in the field of cleft care ensures better reproducibility and accuracy. 8
This work is a generation of a stock of digitally designed impression trays by the CAD/CAM technique. The aim of this technique is to provide more precision and comfort for the patient and the practitioner, and to avoid the risks inherent in making impressions using the conventional technique.
Materials and Methods
Study Sample
Plaster models from the impression of 59 newborn patients with CLP were collected. The patients involved have undergone preoperative orthopedic treatment in the dental center of consultations and treatment of Rabat.
Inclusion Criteria
The patients included in this study presented velopalatal (VCP), unilateral (UCLP), and BCLP. Patients with systemic diseases and syndromes were also included in this study.
All patients were less than 6 months old.
Exclusion Criteria
Newborns with CLP more than 6 months old and patients with CLP who have undergone first lip surgery/cheiloplasty.
Data Collection and Measurement
The 59 cast models were collected, then numbered, and prepared for scanning (Figure 1).

Gypsum models prepared for scanning.
The collected models were scanned using a three-dimensional (3D) scanner, Identica Hybrid of Medit. This scanner is considered as one of the leading scanners in the digital dentistry market. It is a system that uses the advantages of blue LED light and has 3 cameras with an accuracy of ± 7 µm. This system allows scanning of large and small models, as well as the deepest occlusal areas. 9
Thus, the entire surface of each model was scanned uniformly to obtain the maximum recording in all directions with high accuracy.
The obtained datasets were converted to stereolithography to generate a standard tessellation language (STL) file format, before being digitally processed using Blender® software.
After that, 3D measurements regarding width, length, and height were performed based on some anatomical landmarks, taken as reference, as shown in Table 1 (Figure 2).
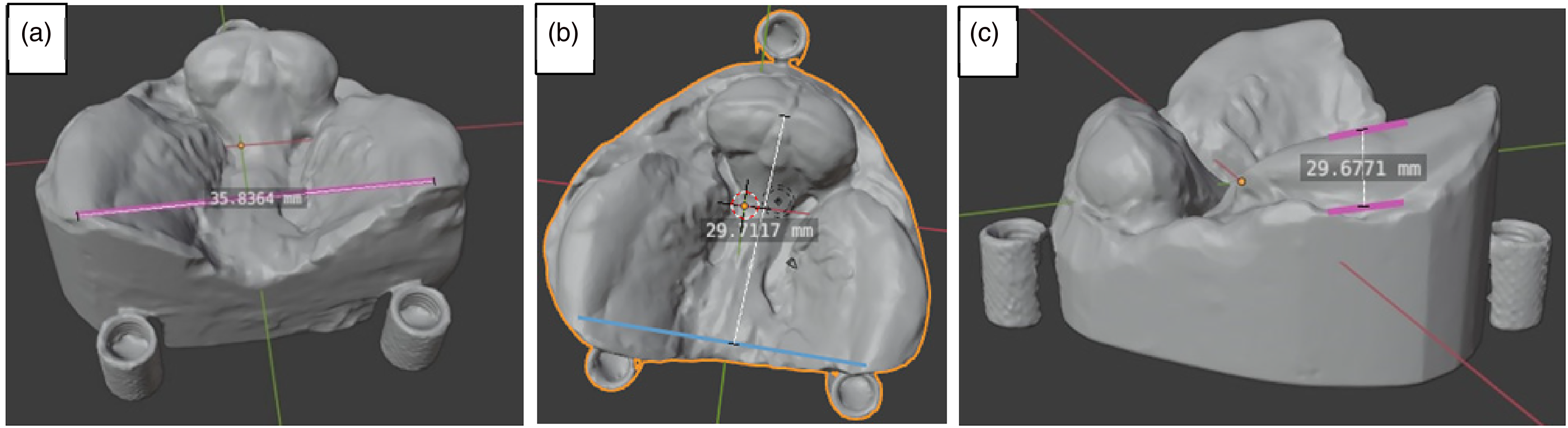
The measurements realized on a digital model/example of a bilateral cleft lip and palate (BCLP). (A) Measurement of the width. (B) Measurement of the length. (C) Measurement of the height.
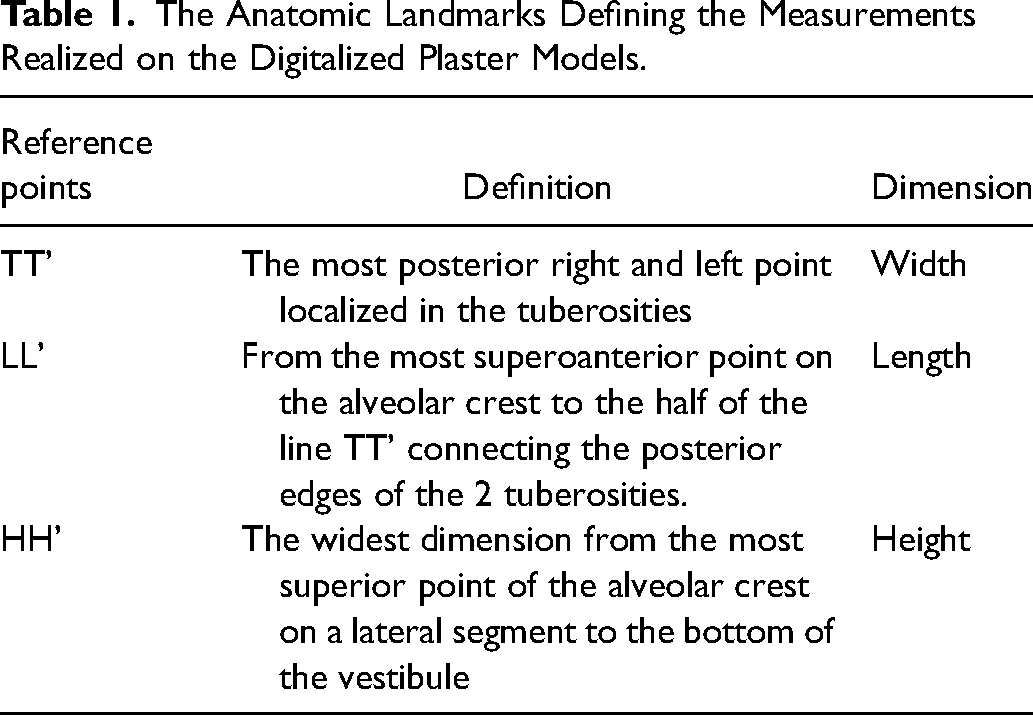
The Anatomic Landmarks Defining the Measurements Realized on the Digitalized Plaster Models.
Classification of the Models
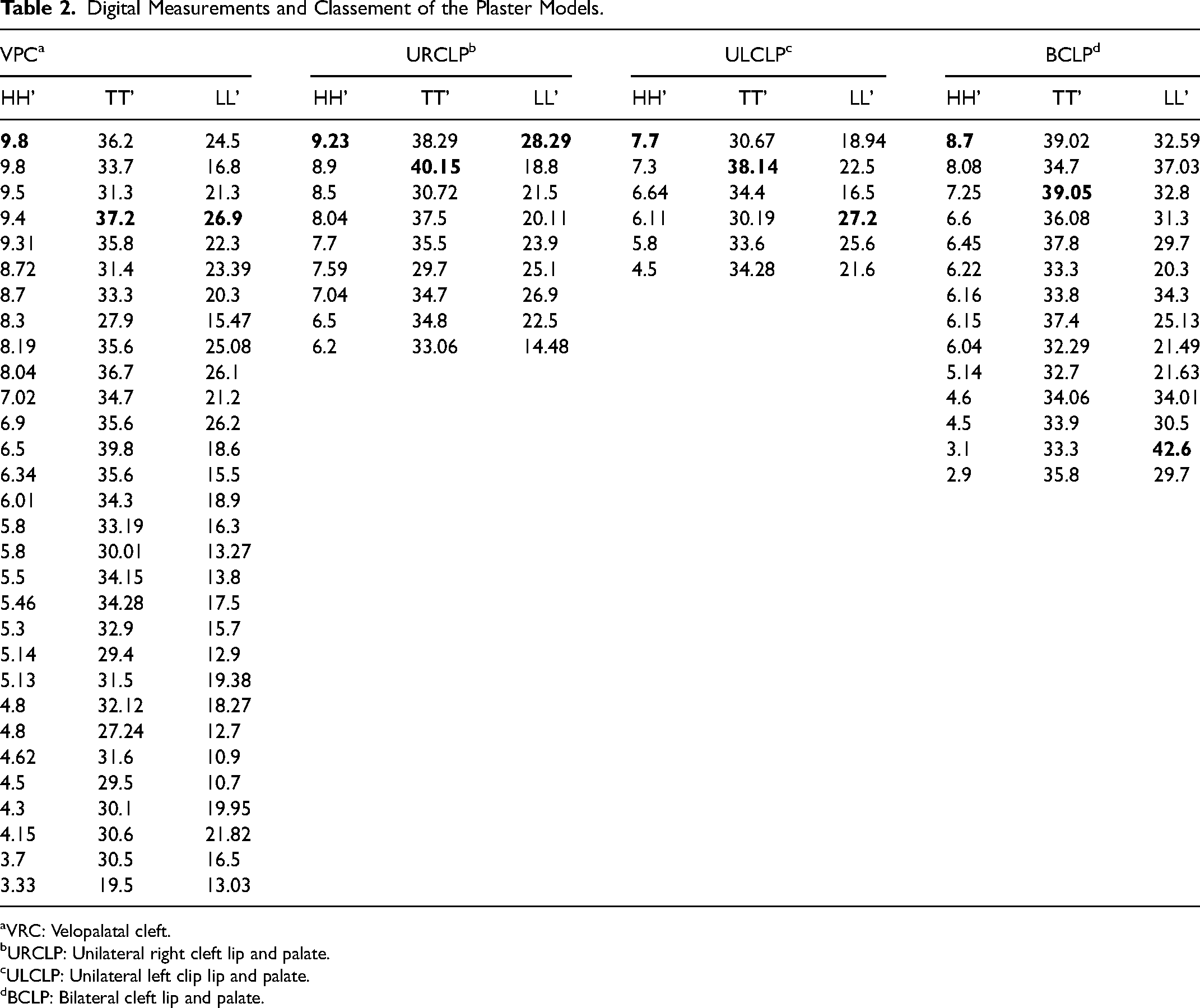
The models were classified according to the nature of the cleft: VPC, unilateral right cleft (URCLP), unilateral left cleft (ULCLP), and BCLP. On the other hand, the models were ranked, in decreasing order, according to the measurements made by the Blender® software (Table 2).
Digital Measurements and Classement of the Plaster Models.
VRC: Velopalatal cleft.
URCLP: Unilateral right cleft lip and palate.
ULCLP: Unilateral left clip lip and palate.
BCLP: Bilateral cleft lip and palate.
The measurements shown in red represent the highest values of TT', LL', and HH' distances for each of the anatomical variations of facial clefts.
Realisation of the CLP and Palate Trays
Based on the measurements typed in bold as shown in Table 2, which represent the highest widths, lengths, and heights for each anatomical class of clefts, we performed the digital design of 5 impression trays using BLENDER® software (Figure 3: A-E).
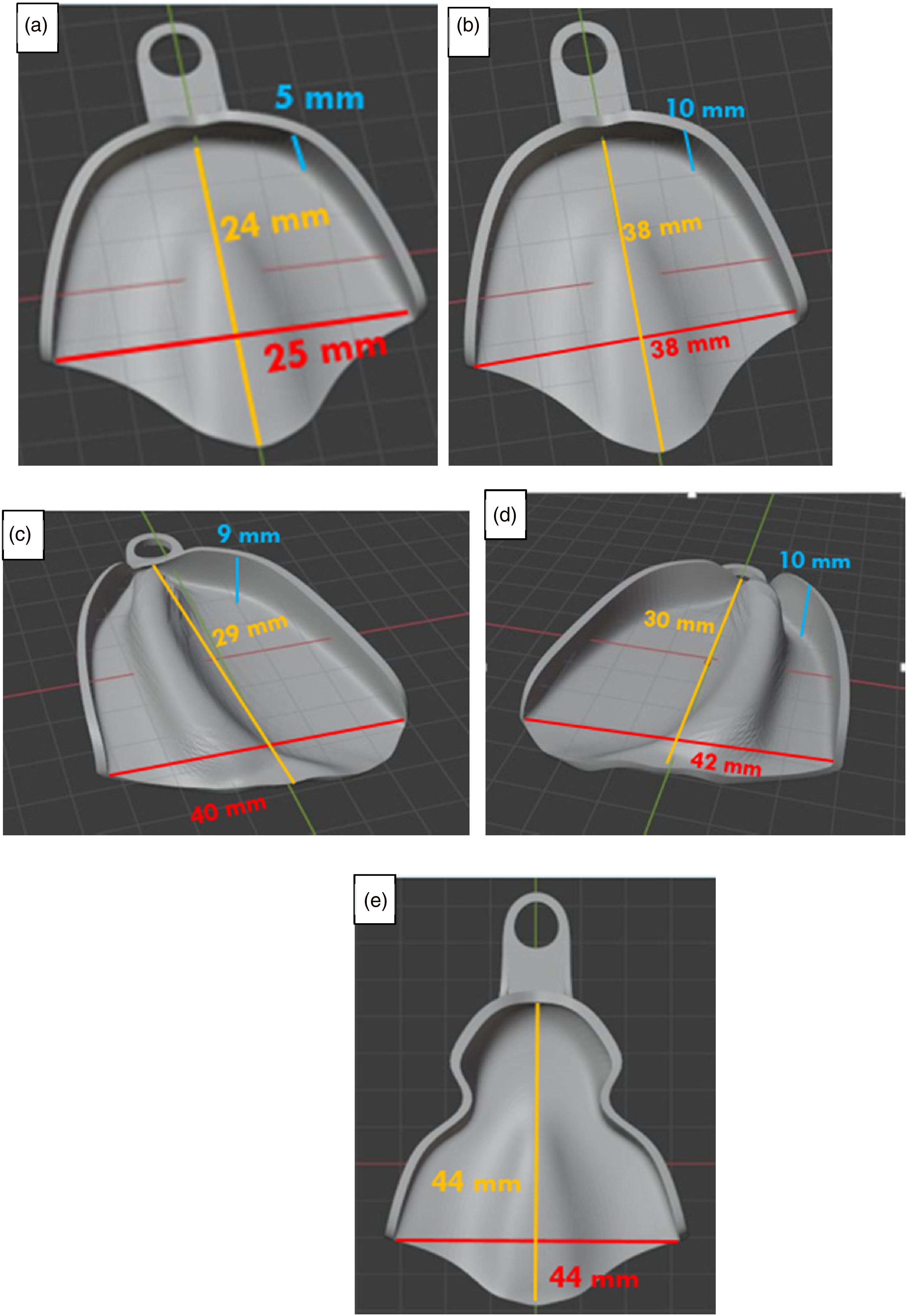
The 5 digitally designed impression trays are proposed. (A) A large impression tray for velopalatal cleft (VPC). (B) A medium-sized impression tray for VPC. (C) An impression tray for unilateral right cleft lip and palate (URCLP). (D) An impression tray for unilateral left cleft lip and palate (ULCLP). (E) An impression tray for bilateral cleft lip and palate (BCLP).
Results
This original study allowed us to generate 5 impression trays for infants with CLP from measurements of the distances between precise anatomical landmarks (TT',LL', and HH') made on 59 plaster models, from neonatal impressions previously taken by the team of Maxillofacial Prosthodontics team of Rabat.
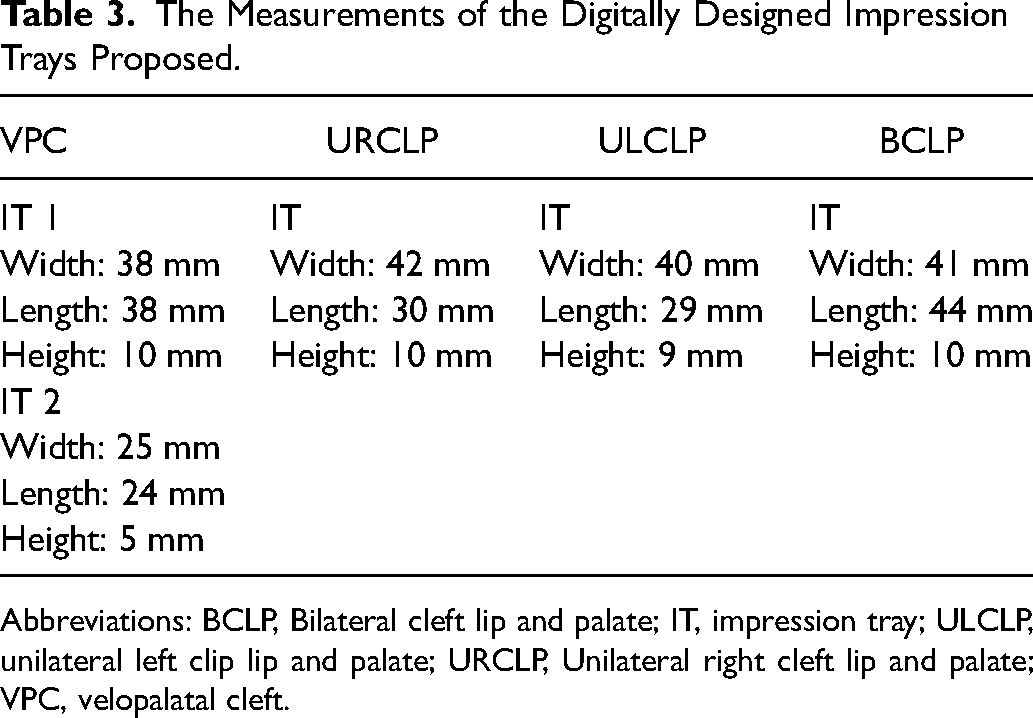
Concerning the VPC, they are the most encountered in daily practice. We proposed 2 impression trays, the first one is large, and it was made based on the basis of the largest intertubercular distance obtained TT' = 37.2, the largest width LL' = 37.2mm, and the largest height between the bottom of the vestibule and the ridge line HH' = 9.8, thus, our impression tray measures are 38mm in length and width and 10mm in height. The second impression tray is medium-sized, 25 mm wide, 24 mm long, and 5 mm high.
For the URCLP, a digitally designed impression tray is proposed based on the same anatomic landmarks. The longest intertubercular distance was TT' = 40.15mm with a width of LL' = 28.29mm and a deep height of HH' = 9.23mm. For that, our impression tray is 42mm wide, 30mm long, and 10mm high.
Regarding the ULCLP, the longest intertubercular distance is TT' = 38.14, the widest width is LL' = 27.2mm, and the deepest height is estimated as HH' = 7.7mm. Thus, an impression tray with a width of 40mm, length of 29mm, and height of 9mm were proposed.
For the BCLP, the largest intertubercular distance is TT' = 39.05mm, the length is LL' = 42.6mm, and the height is evaluated as HH' = 8.7mm. Thus, an impression tray of 41mm width, 44mm length, and 10mm height is proposed (Table 3).
The Measurements of the Digitally Designed Impression Trays Proposed.
Abbreviations: BCLP, Bilateral cleft lip and palate; IT, impression tray; ULCLP, unilateral left clip lip and palate; URCLP, Unilateral right cleft lip and palate; VPC, velopalatal cleft.
Discussion
Newborns with CLP have incomplete palatal structures, responsible for oronasal communication. As a result, they suffer from several functional limitations that include feeding, breathing, swallowing, and facial growth. Feeding difficulties are one of the most common problems. Sucking efficiency is altered due to the inability to generate intraoral negative pressure. Nasal regurgitation of food complicates also the process of feeding.
Surgical treatment starts around 3 months. However, it can be delayed when the baby is underweight for his age.
Meantime, prosthodontic management is planned to facilitate the different altered functions, and more specifically, the feeding function. Depending on the class and the severity of the cleft, feeding appliances are realized to restore the communication between oral and nasal cavities. They create a rigid contact point helping the baby to extract milk.10–12
Conventional impression technique to fabricate feeding and molding devices carries many risks, such as fragmentation of the impression due to the defective morphology of the maxillary in newborns with CLP, possible aspiration of impression fragments leading to respiratory obstruction or episodes of cyanosis, and inadaptation of the impression tray selected, which may affect the success of treatment.3,4,6
An accurate impression tray must have a sufficient transverse size to include the lateral maxillary segments, cover the maxillary tuberosities posteriorly and allow good reproduction of the mucobuccal folds associated with the cleft. However, prefabricated acrylic impression trays are not all the time suitable, since each orofacial cleft remains individual and unique.3,6
Thus, in order to face these problems, it seems necessary for us to propose digitally designed impression trays by taking advantage of CAD/CAM technologies. Our study is an original technique that enables practitioners to avoid the disadvantages and risks associated with the conventional method.
A total of 59 plaster models were collected from patients with CLP, who are previously treated by the Maxillofacial Prosthodontics Team in Rabat. The study concerned isolated CLP, ULCLP, and BCLP. The plaster models were then prepared, scanned, then the width, length, and the height were measured through precise anatomical marks.
CAD allowed us to acquire 3D images with easy manipulation and retouching.
This technique is time-saving, safe, and comfortable for both practitioners and patients. It allows the materialization of precise and well-adapted digitally designed impression trays, having as particularities the capacity to encompass and perfectly fit the concavities and folds of the clefts, presenting sufficient transverse dimensions to cover the lateral segments and the maxillary tuberosities, as well as a good anteroposterior width allowing a good recording of the premaxilla in the case of BCLP.
In most cases, cleft reaches the junction of hard and soft palate. Therefore, our stock of impression trays presents a soft palate/velar border extension to prevent the tongue from protruding into the cleft.
Thus, the orthopedic appliances obtained through these proposed impression trays would present a good restoration of swallowing, feeding, and breathing functions, generating comfort for the practitioner, the patient, and the parents.
For treating the plaster models, we used the software Blender, which is a free open-source software program for editing and designing 3D objects of all kinds. Recently, Blender is increasingly used in the medical field. For Bruns, 13 Blender is employed as a 3D surgical planning software, which allowed a better visualization of bony structures, an interesting animating joints, and a suitable simulation of prosthesis dislocations. Another advantage of this software program is that is suitable for the purification of STL files before the 3D designing and manufacturing. 13
In our study, we preferred to applicate the measurements from digital models rather than plaster models for greater precision and accuracy. In their systematic review, Aragón et al. 14 reported that digital models measurements offer more reliability and accuracy than gypsum models.
Nowadays, CAD/CAM techniques are considered as a revolutionary alternative in cleft care.
Chaudhari et al. (2017) argued that 3D technologies will completely replace conventional techniques in cleft care in the near future. CAD-CAM are actually used for generating and printing palatal plates and PNAM devices. 15
In a comparative study realized by Patel et al., 16 the authors stated that the use of digital impression to scan oral structures for patients with BCLP is a time-saving, comfortable, and safe technique compared to conventional impression methods.
Xepapadeas et al. 8 described a digital process of designing and manufacturing palatal plate for newborns with craniofacial anomalies based on intraoral scanning. The authors confirmed that this technique is advantageous for the patients since it avoids any aspiration or infection by the impression material, which might remain in the oronasal cavity.
All those techniques are advantageous, for both the practitioner and the patient. But unfortunately, the high cost of digital technologies is unaffordable for lower-middle-income countries. In addition, intraoral scanner cannot be available in all prosthodontics centers.
Taking into consideration these limitations, we adopted a multidisciplinary approach, involving many stakeholders from the medical profession, and other fields, to propose prefabricated trays stock for the impression of CLP orthopedic appliances.2,17 These devices considerably reduce the risk of aspiration of the impression material, as they are well adapted to the morphology of the cleft and require a small amount of impression material, the risk of distortion is minimal. So, the risk of aspiration of the impression material is much lower than with handmade trays.
Kalaskar et al. 18 compared the effectiveness of novel impression trays “Cleftray” with that of the traditional finger technique for recording impressions of infants with CLP. They prepared 4 acrylic impression trays based on measurements of transverse lateral and anteroposterior dimensions and cleft width, performed on plaster models. The authors reported that impression trays are superior to the traditional finger, spoon, or ice cream stick methods of creating impressions. Yet, that study concerned exclusively patients with left-sided UCLP, another limitation of this study is that the measurements were performed on plaster models, which offer less precision and accuracy compared to digital ones.
However, our study presents some limitations which are the lack of post insertion follow-up of patients with CLP after presurgical orthopedic treatment, to confirm the clinical effectiveness of our impression trays at long term and the non-perforation of the impression trays, for more retention during the impression.
Similar studies in large populations are, therefore needed, in order to offer more impression trays, of different shapes and sizes, for patients with CLP.
Conclusion
This work aimed to describe an original technique of proposing digitally designed impression trays for infants with orofacial clefts.
This technique of impression was noninvasive, time-saving, and allowing a good reproduction of the details related to the cleft morphology. Parental comfort was also perceived during the process of taking impressions, using the proposed impression trays. However, long-term follow-up periods are needed to evaluate the effectiveness and the well-adaptation of the orthopedic appliances designed by this procedure.
Footnotes
Acknowledgments
The authors would like to thank Mr Karim Berdai, dental technician owner of “Laboratoire 2000” in Rabat for his help. The authors would also like to express their deepest appreciation to all the patients who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.