
Abstract
Objective
The development of the maxillary sinus is different in patients with cleft lip and palate (CLP) compared to non-CLP individuals. To investigate the prevalence and features of maxillary sinus septa (MSS) in patients with CLP in comparison with the non-CLP population.
Design
Retrospective study.
Intervention
Cone beam computed tomography (CBCT) evaluation.
Setting
CLP center in Shiraz faculty of dentistry, Iran.
Patients
A total 306 sinuses (88 cleft and 218 noncleft) on 153 images (CLP group: n = 66; control group: n = 87) were examined to determine the prevalence of septa and characterize them.
Main Outcome Measures
Sinus septa were characterized according to height, orientation, angle, origin, and location. The chi-square test, Mann-Whitney U test, and Fisher's exact test were used for statistical analysis.
Results
The prevalence of septa was 28.9% and 32.1% in the CLP and control groups, respectively. No significant difference was found between the study groups in terms of prevalence, location, and orientation of MSS. The average height and angle of septa were significantly higher in the control group compared to the CLP group. Inferior origin was significantly more prevalent in the control group than in the CLP group (P = .004).
Conclusion
There was no difference in the prevalence of MSS between patients with CLP and non-CLP individuals. However, certain features of the septa were different in patients with CLP.
Introduction
Cleft lip and palate (CLP) are among the most common congenital anomalies affecting the orofacial region.1,2 A wide variety of clinical manifestations associated with CLP have been reported, ranging from an isolated cleft lip to complete CLP, oropharyngeal, and airway complications, as well as facial, esthetic, and dental deformities. 3 Moreover, due to developmental deficiency in patients with CLP, the face, teeth, paranasal sinuses, and maxillary and mandibular arches are adversely affected.4–6
Some studies have evaluated different aspects of maxillary sinuses in patients with CLP.6–8 It has been reported that sinusitis is more prevalent in children with CLP, possibly due to abnormal embryonic development of the maxillary sinus.4,6,8 These patients typically have a smaller maxillary sinus volume, which may increase the risk of sinusitis.7,9 The hypoplastic structures on the cleft side of patients with a unilateral cleft palate are responsible for the nasal septum deviation and lower height of the maxillary sinus. 5
Maxillary sinus septa (MSS) were first described by A.S. Underwood as thin bony walls rising from the sinus floor, varying in height, number, location, and thickness. 10 Septa are classified into 2 groups based on their origin, namely primary septa (formed during the development of maxilla and tooth eruption) and secondary septa (due to sinus pneumatization after tooth extraction). 11 While anatomical variations of MSS are normal, they do have implications for some dental procedures. 12 Sinus lift surgery is the most common procedure in conjunction with implant placement in the posterior maxilla. Perforation of the sinus membrane is one of the complications of this surgery. From a clinical point of view, MSS originating from the inferior wall (floor) would interfere with sinus augmentation. 13 Since, the adhesive strength of the Schneiderian membrane is higher in the area of a maxillary septum, there is an increased risk for perforation during the lifting procedure. 13 Patients with CLP often need a wide variety of orthodontic and prosthetic treatments for dental complications (eg, dental malalignment and impacted, missing, or supernumerary teeth) associated with the different types of clefts. Therefore, sinus augmentation surgery or other pretreatments may be necessary.5,13
Following a literature review which indicated a lack of any previous investigations, the present study aimed to evaluate the prevalence and features of MSS in patients with CLP in comparison with non-CLP individuals, using the cone beam computed tomography (CBCT) imaging technique.
Materials and Methods
Study Design and Patient Selection
This study was approved by the Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran (code: IR.SUMS.DENTAL.REC.1399.115). The study was performed in accordance with the Declaration of Helsinki developed by the World Medical Association.
In a retrospective study, we selected 153 CBCT images of individuals referred to the Department of Oral and Maxillofacial Radiology Centre, Faculty of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran: 66 patients with CLP and 87 non-CLP individuals (control group). All participants were assessed for maxillary sinuses and matched for sex and age (range: 15-35 years). The exclusion criteria were a history of trauma, craniofacial syndrome or anomalies other than CLP, surgical interventions involving the sinuses; detectable pathologies, foreign bodies, or biomaterial in the sinus; motion artifacts, and fracture or destruction of the maxillary sinus wall.
CBCT Images and Analysis
The CBCT images were generated using a NewTom VGi CBCT system (QR Srl). The acquisition settings were 4.71 mA tube current, 110 kVp tube voltage, 3.8 s exposure time, and 15 × 15 cm field of view. Three orthogonal planes (coronal, sagittal, and axial) and panoramic images (1 mm slice thickness and 1 mm step) were used for visualization and evaluation. Evaluations were based on all projections of bone (septa) with a height >2 mm (Figure 1). Each maxillary sinus was evaluated separately (right/left and cleft/noncleft). The prevalence of septa and their location, number, origin, height, orientation, and the angle between the septum and median sagittal suture were measured.
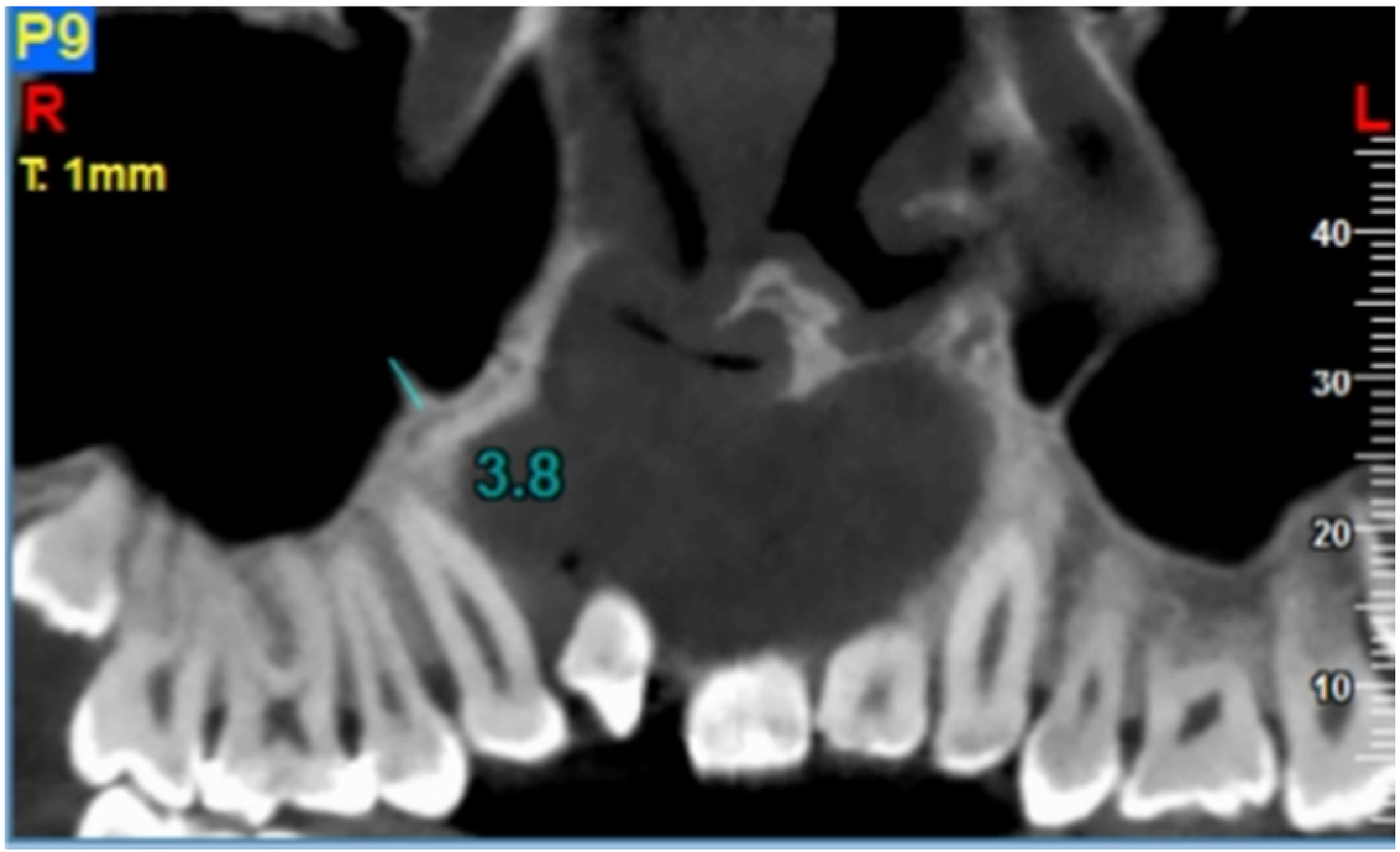
Height measurement of the septa.
Origin. The origin of partial septa was defined as the location where the septum arose from the sinus floor. Accordingly, the origin of MSS was categorized as inferior (floor), superior, anterior, posterior, medial, and lateral walls of the sinus.
Location. To measure the location of the septa, the antral cavity was divided into 3 regions, namely anterior (from the anterior wall of the sinus to the distal aspect of the second premolar), middle (the mesial aspect of the first molar to the distal aspect of the second molar), and posterior (the distal aspect of the second molar to the maxillary tuberosity region) (Figure 2).
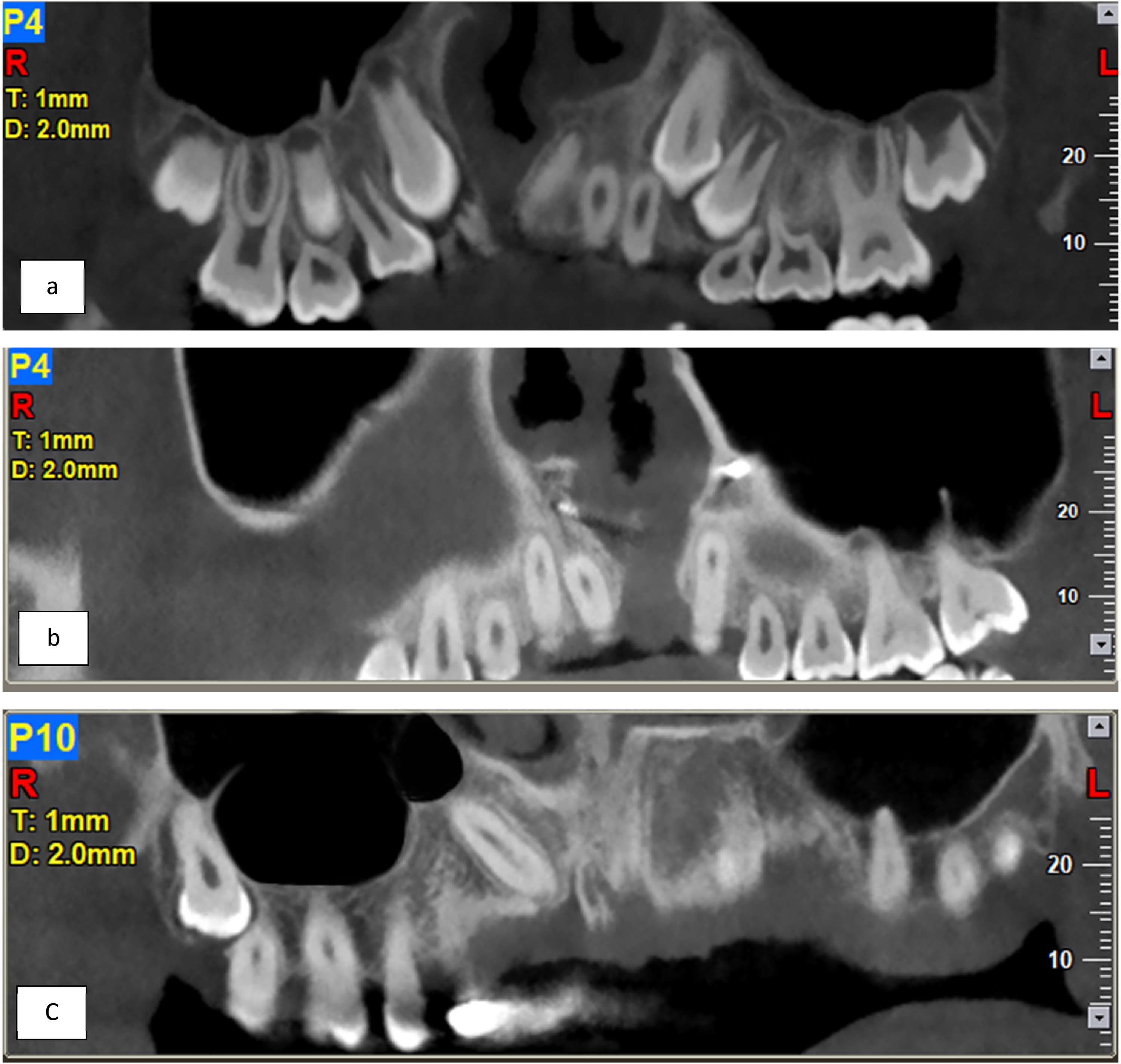
Location of the septa: (a) anterior, (b) middle, and (c) posterior in patients with cleft lip and palate (CLP).
Orientation. To determine the orientation and angle of the septa, a line was drawn parallel to the midpalatal suture (MPS) from the anterior nasal spine to the posterior nasal spine in the axial plane. The orientation was determined based on the angle between the septa and the MPS. An angle of 90°, >90°, or parallel to the MPS was defined as transverse, oblique, or sagittal orientation, respectively.
Risk classification. Based on the classifications proposed in a previous study, 14 the risk of sinus membrane perforation during sinus augmentation surgery was categorized as high, moderate, and low depending on the height and location of the MSS (Table 1). All CBCT images were independently visualized and evaluated by 2 raters (MP and SZ). To quantify measurement errors, 25 randomly selected CBCT images from both study groups were reevaluated 4 weeks later by the raters.
Risk Assessment Based on the Shape, Height, and Location of Septa.
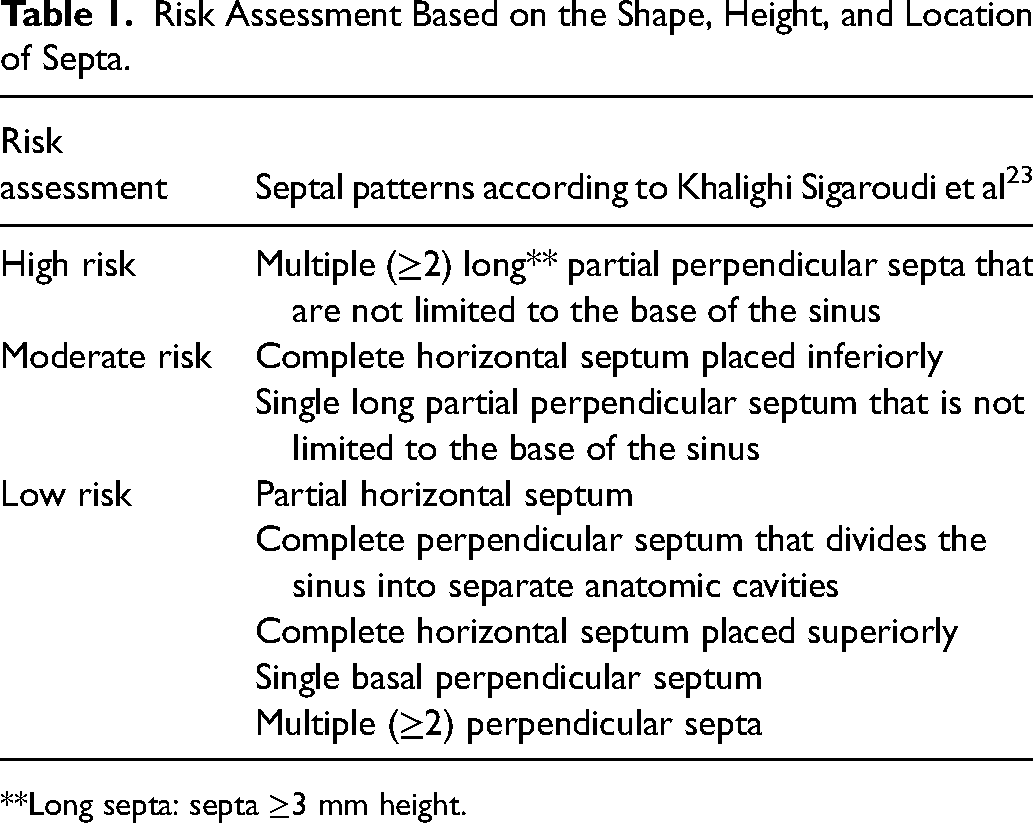
**Long septa: septa ≥3 mm height.
Statistical Analysis
Data were analyzed using SPSS software, version 15.0 (SPSS Inc.). A chi-square test was used to evaluate between-group and within-group correlation between septa features (orientation, location, classification, and origin). Mann-Whitney U test was used to compare differences in height and angle and to examine the normal distribution of the data. Fisher's exact test was used to assess the association between the presence of MSS and CLP. Intra- and interrater reliability was examined using the intraclass correlation coefficient (ICC). P < .05 was considered statistically significant.
Results
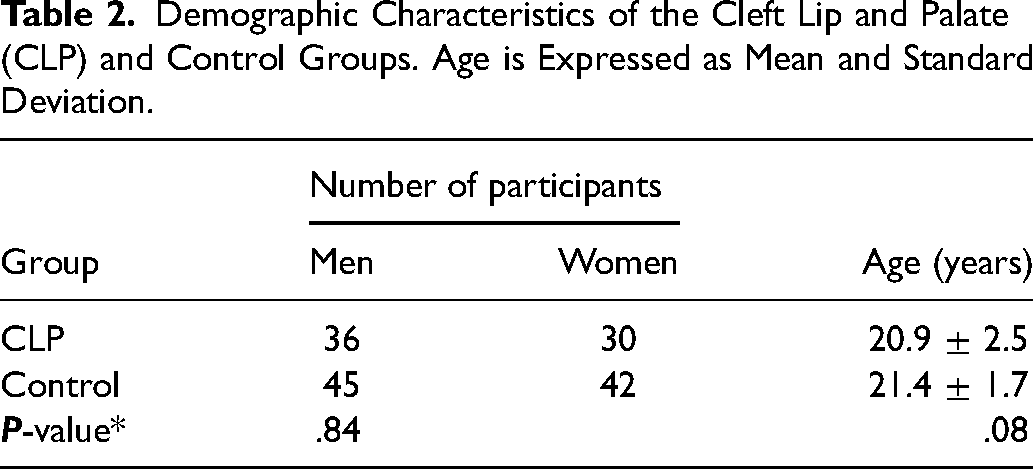
All ICC values were higher than 0.80, indicating acceptable interobserver agreements for all measurements. The intrarater reliability was also high for both examiners (MP: 1, SZ: 0.94). The study samples were from 81 men and 72 women with a mean age of 24.1 years. The CLP group consisted of 44 patients with unilateral CLP and 22 patients with bilateral CLP. A total of 306 sinuses were examined (218 noncleft and 88 cleft). There was no significant difference between the study groups in terms of sex and age (Table 2).
Demographic Characteristics of the Cleft Lip and Palate (CLP) and Control Groups. Age is Expressed as Mean and Standard Deviation.
Detection of MSS
The results showed no significant difference in the prevalence of MSS between the CLP and control groups. The prevalence was calculated based on both the number of sinuses and patients with septa (P = .57 and .62, respectively). The number of sinuses with septa in the control and CLP groups was 69 (32.1%) and 25 (28.9%), respectively. The number of people with at least 1 MSS in the control group (n = 87) and CLP group (n = 66) was 34 (39.0%) and 24 (36.3%), respectively. In terms of all CLP and non-CLP participants, the frequency of septa in women and men was 45.5% and 54.5%, respectively. There was no statistically significant difference between the sex of participants and the presence of septa (P = .065). Comparing the prevalence of the septa between the cleft and noncleft sides in the unilateral CLP, our results demonstrated no statistically significant difference (P = 0.22).
Characteristics of MSS
The results showed that the height of sinus septa was significantly higher in the control group compared to the CLP group (P = .025). The mean height of septa was 9.99 ± 7.12 mm and 6.82 ± 3.58 mm in the control group and CLP group, respectively. The mean septum positional angle in the control group was 98.65° ± 57.12°, which was significantly higher than the 71.22° ± 46.23° in the CLP group (P = .008) (Table 3).
The Height and Angle of Septa in the CLP and Control Groups.
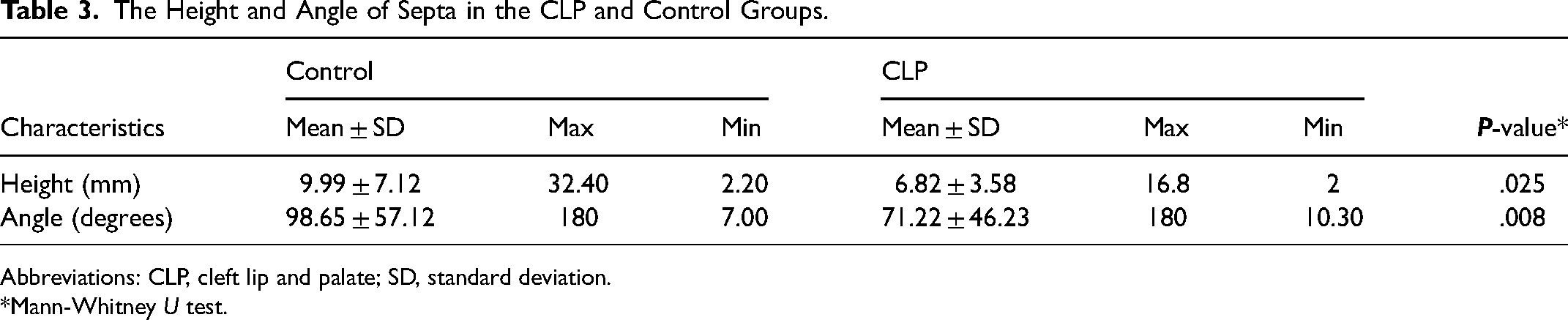
Abbreviations: CLP, cleft lip and palate; SD, standard deviation.
*Mann-Whitney U test.
The results showed no significant difference between the study groups in terms of orientation, location, and complete/partial septa (Table 4) In both study groups, the septa were mainly incomplete. In the CLP group, the location of most septa was in the anterior region. The difference in the orientation of the septa between the groups was not significant (P = 0.09). However, in both groups, oblique orientation (77.8% and 66.1% in the control and CLP group, respectively) was more prevalent than sagittal or transverse orientation.
The Prevalence of Complete/Partial, Location, Orientation, Origin and Risk Classification of Septa in the Cleft Lip and Palate (CLP) and Control Groups.
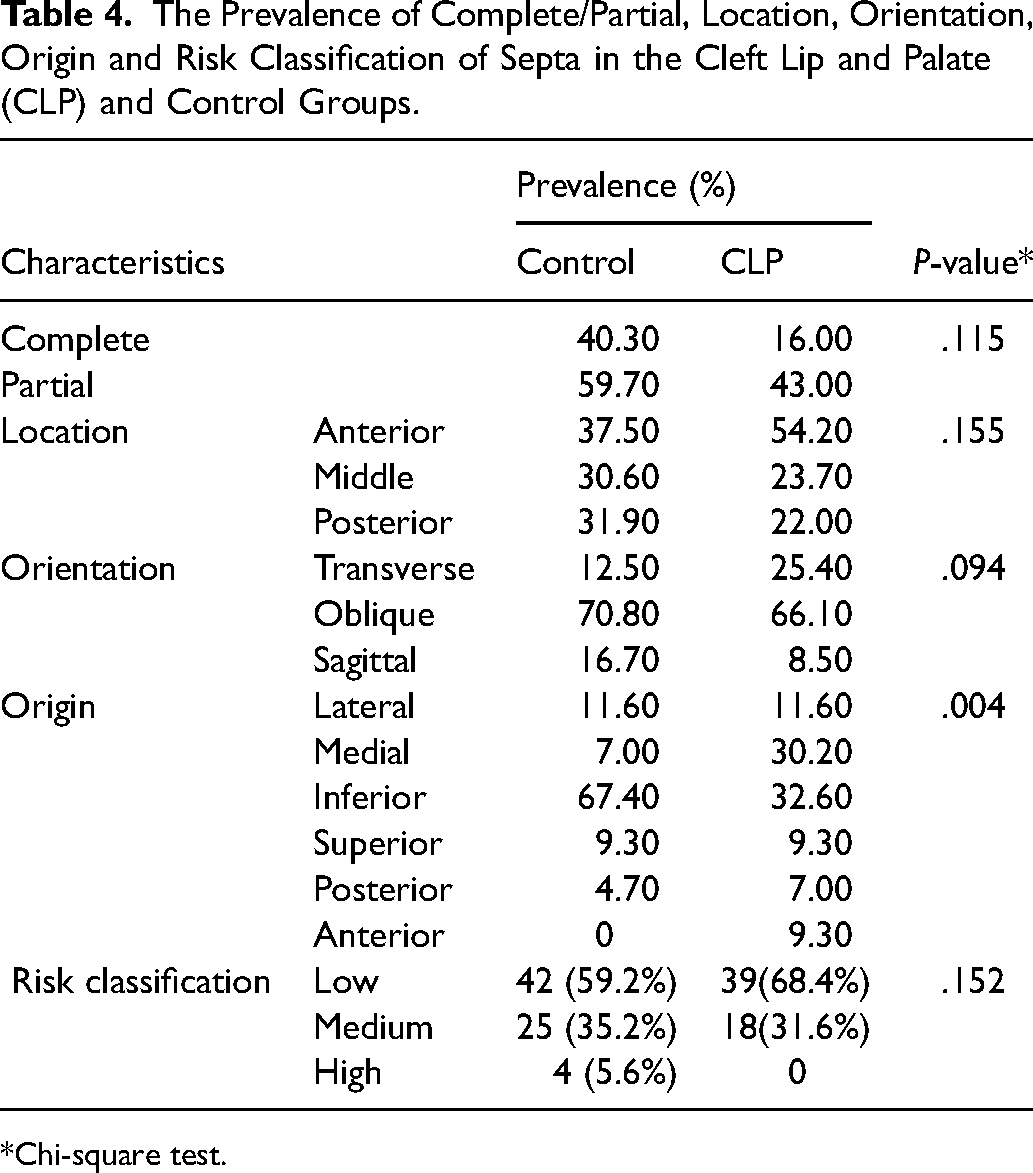
*Chi-square test.
In terms of the origin, there was a significant difference in the distribution of MSS between the groups (P = 0.004). The origin of most septa in the control group was the inferior wall of the sinus. However, in the CLP group, septa mostly originated from the inferior and medial walls. The prevalence of the inferior septa was significantly higher in the control group compared to the CLP group (67.4% and 32.6%, respectively). The prevalence of the risk for sinus membrane perforation is presented in Table 4. The results showed no significant difference in risks between the groups (P = 0.152). The patients in both groups were mostly in the low-risk category.
Discussion
Patients with CLP face a variety of problems. 3 Sinusitis and missing teeth are the most prevalent issues in these patients.3–6 Dental implant to replace the missing tooth is one of the treatment options, but patients may also need pretreatment procedures such as sinus augmentation surgery. Although anatomical variations of MSS are normal, they complicate sinus augmentation procedures and increase the risk of sinus membrane perforation.5,10,13 In parallel with an increasing number of maxillary sinus surgeries, there is a growing momentum for radiological evaluations to determine the size, shape, and location of a septum. In the present study, we evaluated the prevalence and features of MSS in patients with nonsyndromic CLP in comparison with non-CLP individuals.
Our results showed no significant difference in the prevalence of MSS between the CLP and control groups. Other studies have also evaluated the prevalence of MSS in non-CLP individuals.15–26 It is noteworthy that the reported prevalence rates vary greatly. Studies with evaluations based on the number of sinuses have reported a prevalence rate of MSS ranging from 9.5% to 58%.15–17,19,20,22,26 However, those with evaluations based on the number of patients reported a prevalence rate from 10.7% to 70.6%.15,16,21,23–25 In our study, the prevalence of septa in patients with CLP and non-CLP individuals was 28.9% and 32.1%, respectively. Although these rates are well within the prevalence rates reported in previous studies, the wide gap could be due to differences in radiographic methods, septum identification criteria, sample size, and age range. Moreover, the frequency of septa in women and men was 45.5% and 54.5%, respectively, in the present study. The results showed that gender was not related to the septa prevalence. This finding is in line with the previous studies.27,28
The results showed no significant difference in the location of septa between the groups; however, the location of most septa was in the anterior region. This is of concern because the prevalence of missing premolars in patients with CLP is high.29 This results in a higher demand for dental implants to replace the missing teeth in the premolar region, that is, an increase in the risk of intraoperative complications due to sinus membrane perforation. Our findings are in line with the results of some previous studies reporting that the anterior region is the most prevalent location for a septum.21,25,28,30,31 We only found 1 study that evaluated the development of MSS in patients with CLP, which reported a higher prevalence in the second molar region. 32 However, their results must be interpreted with caution since the study only included 3 individuals, that is, an extremely low sample size. Other studies that evaluated the location of septa in non-CLP individuals reported their averaged presence in the anterior (28.1%), middle (52.55%), and posterior (25.19%) regions.22,32–35 In contrast, another study questioned the higher prevalence of septa in any of these regions. 36 Such contradictory results could be due to nonstandardised classifications for the location of a septum. 19 Septa location is important in sinus drainage interruption and pathology formation. 36
Morphologically, our results showed a higher prevalence of partial septa than complete septa in both groups. In contrast, previous studies reported the dominance of complete septa with a prevalence rate ranging from zero to 89.5%.13,17,21,31,33,37–39 The difference in the results may be attributed to assessments based on different reference planes for CBCT imaging, different age groups, dentition status, and race. The clinical significance of partial and complete septa depends on their location, height, and the type of surgery performed. 36 However, Hong et al 39 stated that dentition status, location, and the origin of septa were not associated with complete septa.
Orientation
Our results showed that oblique septa were the most prevalent orientation in both study groups (66.1% and 70.8% in CLP and control group, respectively), 1 study investigating the relationship between septa orientation and sinus lift complications, reported that the risk of membrane perforation highly elevated in the presence of transverse septa and severity of this perforation depends on septa size and height. 36 In light of this information, transverse septa cases should be approached carefully. The prevalence of transverse septa in the present study was almost twice in the CLP group compared to the control group (25.4% and 12.5%, respectively).
Origin
We found a significant difference in the origin of septa between the CLP and control groups. The inferior origin of MSS was more prevalent in the control group compared to the CLP group. This means that sinus augmentation surgery to place dental implants may be easier in patients with CLP than with non-CLP. Our findings were in line with other studies reporting a higher prevalence of inferior origin of MSS.17,22,38 On the other hand, it is found that in patients with CLP inferior and medial origins were significantly more prevalent than in other regions.
Height
The height of a septum plays an important role in window preparation for sinus augmentation surgery.19,40 Reported height of septa varies from 2.5 to 12.5 mm in non-CLP individuals.16,19,31,34,41 In our study, the average height of all septa was 8.57 mm with a maximum height of 32 mm. The mean height of septa in the control group was 10.0 ± 7.12 mm, which was significantly higher than in the CLP group (6.83 ± 3.58 mm). Such a wide variation in the reported septa heights could be due to different measurement methods, radiographic techniques, age, and dentition status.
Angle
The angle of the septa was measured by drawing a line parallel to the MPS from the anterior nasal spine to the posterior nasal spine in the axial plane. This angle was significantly wider in the control group compared to the CLP group. A previous study reported septal angles ranging from 31° to 120°, in which 68% were under 90°. 42 Naitoh et al 32 stated that the septal angle alters during growth in children with CLP. Various methods have been used to measure the septal angle, including the sagittal plane of the sinus, 13 sinus floor in the coronal cut, 42 and MPS.13,22,42 In the present study, we used MPS as the origin for measuring the angle which is a reliable and standardized line for investigating computed tomography (CT) images of patients with CLP. Moreover, MPS accommodates any distortion that may occur in the morphology of the sinus and its floor.
Risk Assessment
Despite our concerns about the risk of sinus augmentation surgery in patients with CLP, we found no significant difference in the risk of sinus membrane perforation between the CLP and control groups. However, the results of the present study showed that at least one-third of patients with CLP had septa in the inferior wall of the maxillary sinus. In addition, due to missing premolars and the high prevalence of a septum in the anterior region in patients with CLP, this procedure is prone to intraoperative complications. So, radiological evaluation is highly recommended to define and locate the MSS prior to sinus lifting surgery to reduce preoperative and postoperative complications.
A number of methods have been proposed for the diagnosis of sinus septa, namely CBCT, panoramic radiograph, CT, direct examination, endoscopy, percussion, palpation, and transillumination. 43 Among these, a panoramic radiograph (a 2-dimensional image) has the disadvantage of producing distorted images, overprojection of sinus pathology, and overlap of anatomic structures. 42 As a result, differentiation of a septum from other anatomic structures becomes difficult and there is potential for a false-positive diagnosis.10,13,21,22,42 In comparison to panoramic radiography, CT is more accurate and reliable for imaging hard tissue. Among the above-mentioned methods, CBCT is a superior radiographic imaging tool allowing detailed evaluation of sinus septa. CBCT produces reconstructed 3-dimensional images with reduced image artifacts, eliminates the superimpositions of structures, and has a lower radiation dose compared to CT. 44
The main limitation of the current study was its retrospective design in a single oral and maxillofacial radiology center. Also, for the purpose of data comparison, there were no other studies that evaluated the prevalence and features of MSS in patients with CLP.
Conclusion
There was no significant difference in the prevalence, location, and orientation of MSS between CLP and control groups. However, the height and angle of septa were higher in non-CLP individuals. No additional risk of sinus membrane perforation in patients with CLP was found.
Footnotes
Acknowledgments
The authors would like to thank the Vice Chancellery of Shiraz University of Medical Sciences (Shiraz, Iran) for supporting the research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vice Chancellery of Shiraz University of Medical Sciences, (grant number 21294).