
Abstract
Objective
Midface hypoplasia (MFH) is a long-term sequela of cleft lip and palate repair, and is poorly understood. No study has examined the aggregate data on sagittal growth restriction of the midface following repair of the lip, but not palate, in these patients.
Methods
A systematic review of 3780 articles was performed. Twenty-four studies met inclusion criteria and 11 reported cephalometric measurements amenable to meta-analysis. Patients with Veau class I-III palatal clefts were included so long as they had undergone only lip repair. Groups were compared against both noncleft and unrepaired controls.
Results
Cephalometrics were reported for 326 patients (31.3% female). Noncleft controls had an average SNA angle of 81.25° ± 3.12°. The only patients demonstrating hypoplastic SNA angles were those with unilateral CLP with isolated lip repair (77.4° ± 4.22°). Patients with repaired CL had SNA angles similar to noncleft controls (81.4° ± 4.02°). Patients with unrepaired CLP and CL tended toward more protruding maxillae, with SNA angles of 83.3° ± 4.04° and 87.9° ± 3.11°, respectively. Notably, when comparing SNA angles between groups, patients with CLP with isolated lip repair had significantly more hypoplastic angles compared to those with repaired CL (P < .0001). Patients with CLP with isolated lip repair were also more hypoplastic than noncleft controls (P < .0001). In contrast, there was no significant difference between the SNA of patients with repaired CL and controls (P = .648).
Conclusion
We found that cleft lip repair only appeared to contribute to MFH in the setting of concurrent cleft palate pathology, suggesting that scarring from lip repair itself is unlikely to be the predominant driver of MFH development. However, studies generally suffered from inadequate reporting of timing, technique, follow-up time, and cleft severity.
Introduction
Isolated cleft lip (CL) and palate (CLP) account for a major portion of the global burden of surgical disease.1,2 Cleft repair has well-document social and functional benefits, 3 and surgical repair has been shown to be cost-effective when analyzed in terms of disability-adjusted life years (DALY) even in low- and middle-income countries that rely on foreign medical teams to provide care.4–6 However, treatment of complications can be costly and may be especially cumbersome to socioeconomically disadvantaged patients. Ideally, minimal to no revision would be necessary, even in the most difficult of cases. Gillies and Millard famously wrote that “speed in surgery consists of not doing the same thing twice.” 7 What is true regarding efficiency in the operating room applies also to the lifetime of care experienced by patients with cleft conditions.
Midface hypoplasia (MFH) is a well-described complication of cleft repair.8,9 A considerable portion (14%-45%) of patients with CLP require subsequent correction of a hypoplastic midface. 10 In contrast, patients with CLP who do not have surgical repair frequently present with near-normal maxillary projection.11,12 Several studies have looked at the rates of MFH in the cleft population, though few have distinguished between cleft subtypes and many are limited by sample size and lack of controls. 13 Rates of MFH requiring surgical correction appear to be higher in patients with both cleft lip and palate than isolated CL or CP. For example, Oberoi et al reviewed 648 patients over a 20-year period and found an overall orthognathic surgery rate of 9.1%, with a rate of 1.9%, 3.3%, and 12.2% for CL, CP, and CLP, respectively. 10 Good et al reviewed 177 patients and found that 47.4% of their CLP, but none of their CP or CL patients, required a Le Fort I procedure. 9 Our group has shown higher rates of corrective orthognathic surgery for unilateral CLP (30.2%) in comparison to 4.4%, and 1.8% for isolated CP and isolated CL, respectively. 14 The need for maxillary advancement is largely subjective and currently without standardized criteria,13,14 which may account for the variability noted in the literature.14–16
Several factors have been thought to contribute to MFH in cleft conditions. Disruption in embryonic fusion pathways and abnormal insertions of facial musculature, 17 as well as sequelae of cleft repair such as scarring.18–21 Animal studies by Eisbach and Bardach demonstrated higher lip pressures and decreased sagittal maxillary growth in postnatal rabbits.22,23 In contrast, scarless in-utero repair of CL in rabbits resulted in no difference in maxillary growth compared to controls. 24 A study comparing lip repair with and without wide tissue undermining of the maxilla in beagles found higher lip pressures with undermining but no significant difference in maxillary growth. 25 Goz et al compared electromyographic findings and skeletal measurements in human cleft lip patients and noted a decrease in anteroposterior maxillary dimension that the authors attributed to scarring. 26 There is precedent for the theory that scar tissue may inhibit craniofacial growth in the burn literature, where facial burn contractures have negatively influenced facial growth.27–30
Despite these investigations, it remains unclear whether innovations in surgical timing or techniques could prevent MFH in a subset of cases. The effect of early palatal surgery on facial growth has been postulated to be a major player in restricted maxillary growth.3,31–33 However, no systematic review of the literature has examined the impact of isolated lip repair alone on MFH, therefore leaving the influence of this important variable unresolved.9,34–36 The objective of this study was to investigate the role of isolated lip repair in the development of MFH.
Methods
A literature review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 37 using the PubMed, Scopus, and Embase databases. Inclusion criteria included English-language articles examining repaired isolated CL and unilateral CLP patients with cleft lip repair only. Patients with Veau class I-III palatal clefts were included so long as they had not undergone palatal repair, such that the impact of the lip repair on midfacial growth could be examined independent of the effect of any palatal surgery. Exclusion criteria included non-English language articles, abstracts without full-text articles available, duplicate articles, letters to the editor or replies, non-peer-reviewed publications, and studies that did not distinguish between the impact of cleft palate versus cleft lip repair.
Articles that met inclusion criteria had the following data abstracted: publication year, study type, study population, MFH metric used, SNA measurements with standard deviations (SDs) if included, whether MFH was noted or not, age at the time of lateral cephalometric measurements, and patient sex. Cephalometric analysis has been widely employed in craniofacial research but is not without criticism from within the fields of orthodontics and craniometry. 38 Aside from inevitable errors in measurement, 39 cephalometric “norms” are known to vary widely between different ethnic populations. 40 Despite these limitations, our review found cephalometrics to be the only objectively comparable data consistently obtained in studies examining MFH. Its advantages include reproducibility, clinician familiarity, and a methodology that is relatively less resource-intensive than other methods making it accessible to lower-resource settings.
Data on age and region-matched controls without a cleft deformity were included where available. SNA averages weighted for age were obtained for the following groups: CL with repaired lip, CL with unrepaired lip, unilateral CLP with repaired lip only, unrepaired unilateral CLP, and noncleft controls.
All data were prepared and compiled using the Statistical Package for the Social Sciences program version 26.0 for Macintosh (SPSS Inc). Scaled variables were compared with an independent t test. An alpha value of .05 was used to define statistical significance.
Results
3780 articles met screening criteria, and of those 24 met criteria for inclusion in our study. 11 articles contained data amenable to inclusion in our meta-analysis (Figure 1). Data for a total of 326 patients were included in the meta-analysis (Tables 1 and 5). 13 studies met inclusion criteria for qualitative analysis but did not report cephalometric data amenable to meta-analysis (Table 4). Of those, 4 studies (30.8%) reported observing sagittal growth deficiency of the maxilla in CLP patients with lip repair only. Study populations had a wide geographic spread, ranging from China to Brazil and Sri Lanka (Tables 4 and 5).
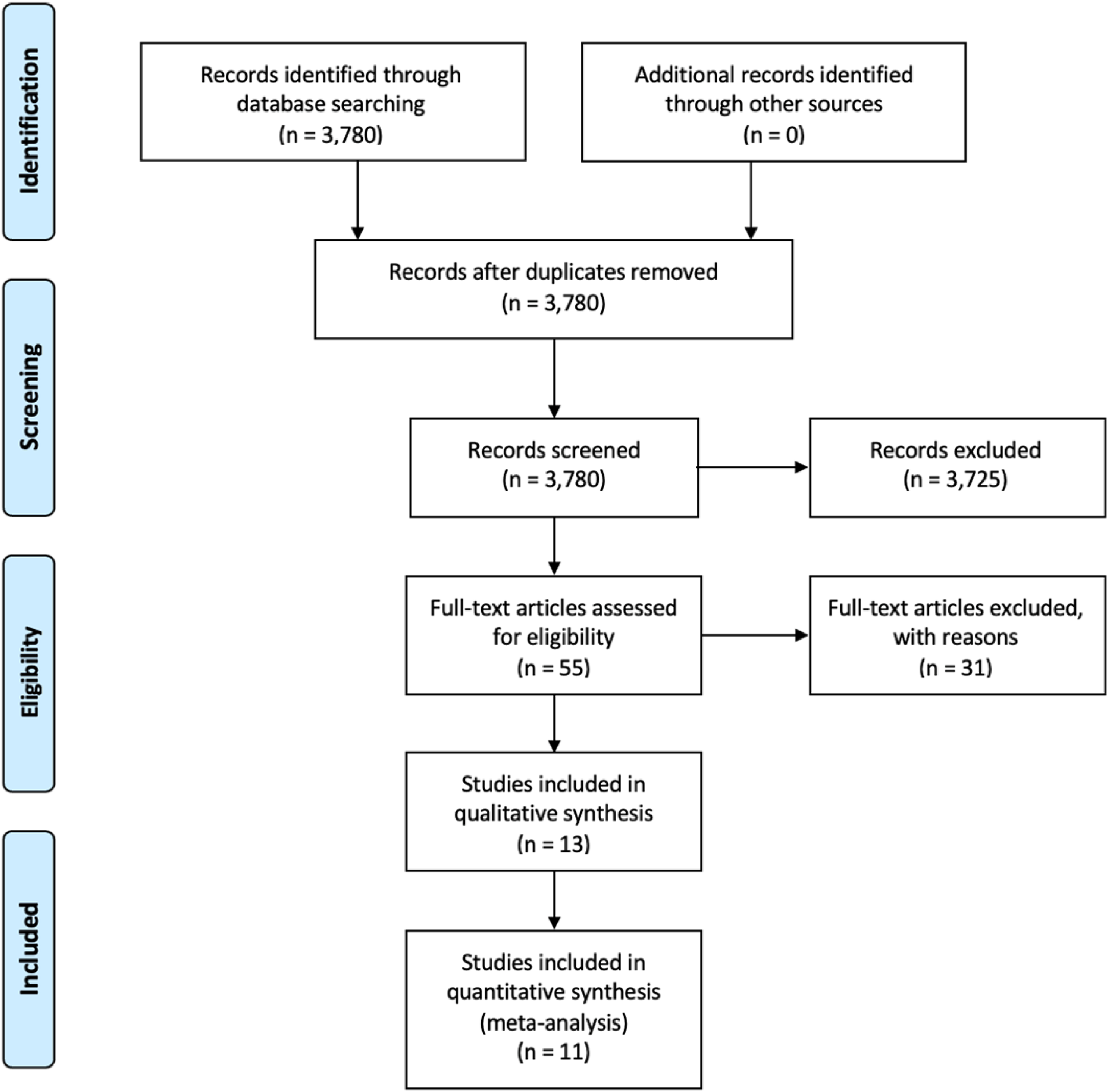
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart.
Demographic Data for Studies Included in Meta-Analysis.
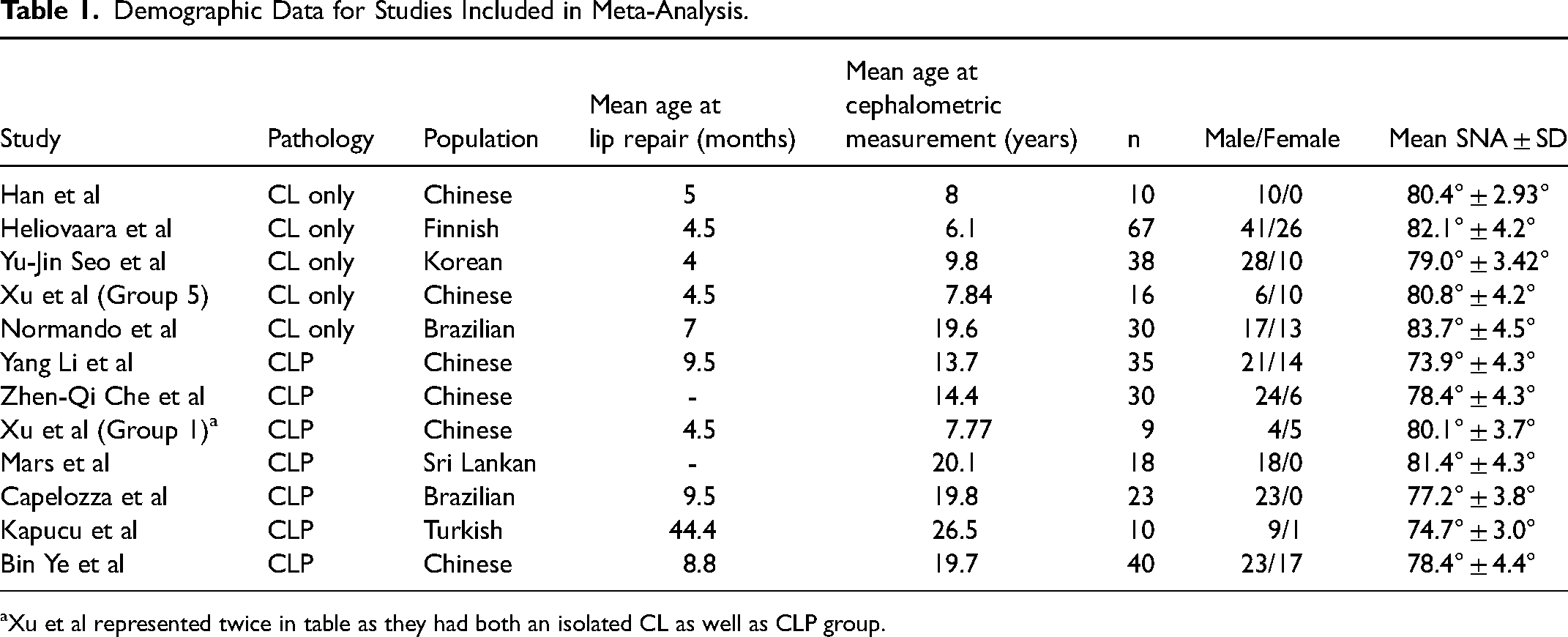
Xu et al represented twice in table as they had both an isolated CL as well as CLP group.
Studies Not Included in Meta-Analysis.
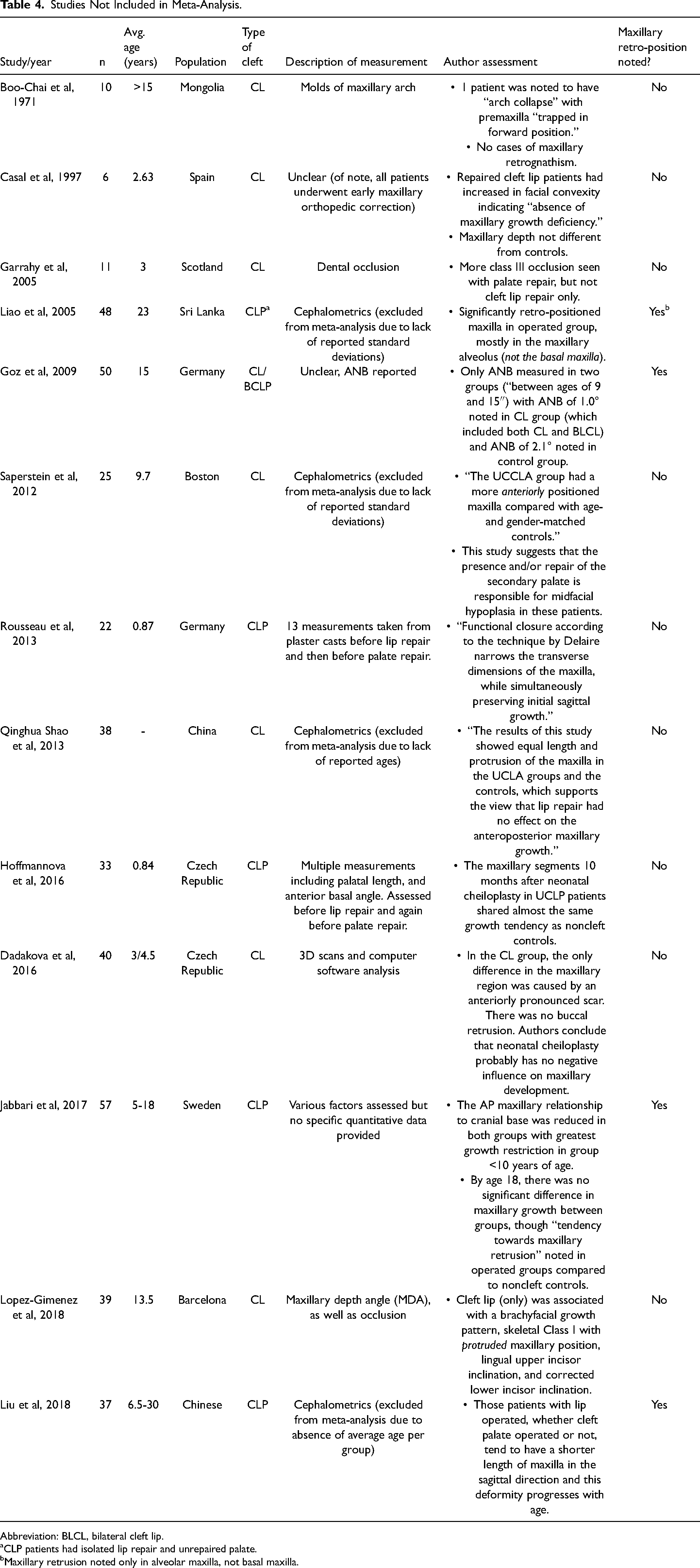
Abbreviation: BLCL, bilateral cleft lip.
CLP patients had isolated lip repair and unrepaired palate.
Maxillary retrusion noted only in alveolar maxilla, not basal maxilla.
Studies Included in Meta-Analysis.
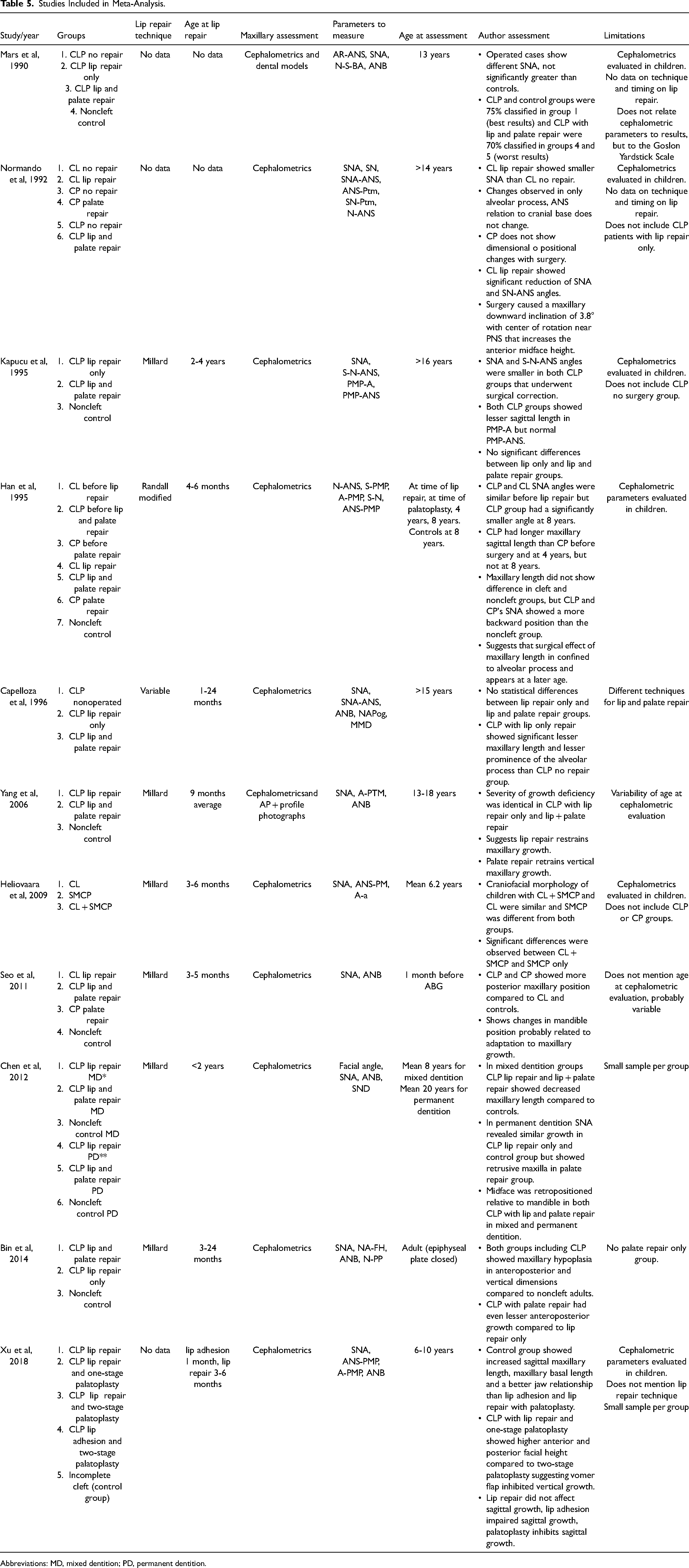
Abbreviations: MD, mixed dentition; PD, permanent dentition.
161 patients (36.6% female) with isolated CL underwent lip repair at an average age of 5 months (range 4-7). Reported average age at the time of cephalometric measurements for this group was 10.3 years. 165 patients (17.6% female) with unilateral CLP and isolated lip repair (no palate repair at the time of cephalometric measurement) were identified. These patients underwent lip repair at an average age of 14.4 months (range 4.5-44.4). Average age at the time of cephalometric evaluation was 16.7 years. 171 age- and region-matched healthy noncleft controls were reported with cephalometric measurements taken at an average age of 16.1 years (Table 1).
Noncleft controls had an average SNA angle of 81.25° ± 3.12°. The only patients demonstrating hypoplastic SNA angles were those with unilateral CLP with isolated lip repair (77.4° ± 4.22°). Repaired CL patients had SNA angles most similar to noncleft controls (81.4° ± 4.02°). Unrepaired CLP and CL tended toward more protruding maxillae, with SNA angles of 83.3° ± 4.04° and 87.9° ± 3.11°, respectively (Table 2).
Weighted SNA Averages by Group.
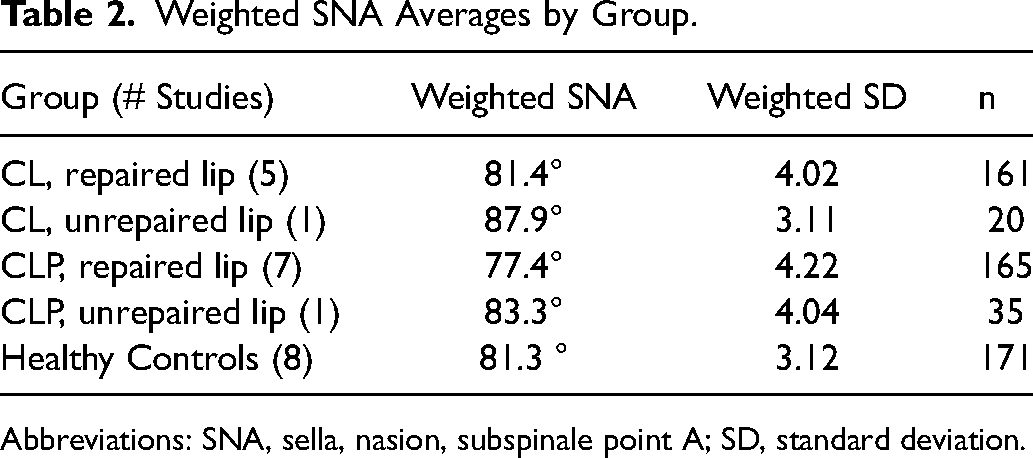
Abbreviations: SNA, sella, nasion, subspinale point A; SD, standard deviation.
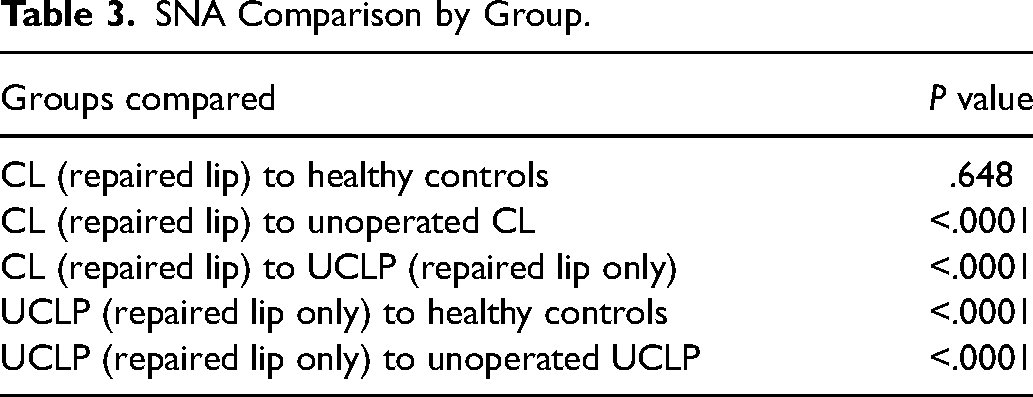
A statistical comparison of these SNA angles to each other is shown in Table 3. Notably, CLP with isolated lip repair had significantly more hypoplastic angles compared to repaired CL patients (P < .0001). As mentioned previously, the only variable that was different between these groups was the unrepaired palate in the CLP group. CLP patients with isolated lip repair were also more hypoplastic than noncleft controls (P < .0001). In contrast, there was no significant difference between the SNA of repaired CL patients and controls (P = .648).
SNA Comparison by Group.
Discussion
Comprehensive cleft care is a complex, multidisciplinary endeavor that spans the patient's childhood and often extends well into adulthood. The additional procedures, cost, and time caused by iatrogenic complications add significant stress to the patient and family. It also widens socioeconomic disparities that may already reduce access to care in this vulnerable population. There is evidence that patients with orofacial clefts are at higher risk of complications associated with surgical correction of MFH.41,42 A higher rate of relapse after Le Fort I advancement in cleft patients was attributed to the amount of advancement needed and resulting soft tissue tension. 41 Other reported complications may be the result of anatomic irregularities, such as malposition of the nasal septum when repositioning the maxilla after Le Fort I osteotomy, or hemorrhage following irregular pterygoid or maxillary downfracture. 42 It is thus imperative to continue to examine modifiable parameters in cleft care to reduce rates of MFH.
Prior studies have shown that patients with CL, with or without alveolar involvement, tend to exhibit normal midface projection.32,33,43,44 Work from our group has shown that patients with unrepaired unilateral and bilateral CLP have protruding, as opposed to hypoplastic, maxillae. 11 Surgical intervention on the growing craniofacial skeleton is therefore felt to be responsible for MFH, and most studies have suggested that palatal repair in a patient with CLP may be the primary culprit.3,31–33,45 Our group has shown that optimal timing for palatal repair falls between 13 and 18 months to mitigate this risk. 45
The question remains whether lip repair, often performed prior to palate repair, significantly contributes to MFH. While certainly in the minority opinion, Filho et al concluded that lip repair appeared to be the main driver behind deficient maxillary growth. 46 There is a need to elucidate the impact of lip repair in the growing midface, especially with the advent and increasing popularity of neonatal cleft lip repair.47,48
Our results for repaired CL patients demonstrated SNA angles nearly identical to controls, which was expected due to the absence of palate pathology. Patients with unrepaired CL had a protuberant, as opposed to hypoplastic, maxilla which is a finding that is consistent with previous studies looking at unoperated cleft lip patients. 49 It is possible that restoring a physiologic soft tissue sling in the presence of cleft lip corrects sagittal maxillary overgrowth enough to result in normal projection.
When maxillary hypoplasia was observed in CL patients, it was frequently noted to be present only in the alveolar process of the maxilla. Normando et al found that patients with repaired CL had a smaller SNA angle compared to unrepaired CL patients, though these changes were noted only in the alveolar process of the maxilla. 50 Han et al performed one of the only prospective studies in the literature, and findings suggest that the surgical effect is confined to the alveolar process of the maxilla and becomes more apparent with age. 35
Unilateral CLP patients with isolated lip repair demonstrated significantly more hypoplastic midface measurements compared to controls or unoperated CLP patients. The only intervention that these patients underwent was lip repair. This group also had significantly more MFH compared to repaired CL patients, the only difference between the two being the palate pathology in the CLP group. Taken together, these results suggest that lip repair in the setting of palate pathology may contribute to MFH. One possibility is that restoring the soft tissue sling around the maxillary alveolus in the setting of disrupted transverse and median palatine sutures encourages aberrant growth in different vectors (transverse, vertical). Laowansiri et al noted that vertical growth outpaces sagittal growth during late childhood and adolescence. 51 Since sagittal growth is more prominent earlier in childhood, the extensive surgical repair experienced by patients with CLP could potentially further restrict this growth, resulting in the observed findings.
As in the CL cohort, the maxillary alveolus was also frequently noted to be hypoplastic in the CLP population. Filho et al performed a retrospective review of Brazilian CLP patients with no repair, lip repair only, and both lip and palate repair. 52 Although there were no significant differences between repaired groups, the lip repair only group showed decreased prominence of the maxillary alveolar process. Of the studies not included in our meta-analysis, two noted decreased maxillary projection in the alveolar region of the maxilla but not the basal maxilla in both bilateral 26 and unilateral 53 CLP with repaired lips only (Table 4). This corroborates the findings discussed above by Normando and Han et al, which suggest that if lip repair alone has an effect on the developing maxilla, it is most likely to occur in the alveolar process and less likely to cause true MFH in relation to the cranial base.
Interestingly, CLP patients also underwent lip repair at an average age of 14.4 months, which is notably later than the average age of 5 months for the CL cohort. Although difficult to confirm with the available data, one explanation may be that patient with more severe deformity (cleft lip and palate) and only partial repair (lip repair, no palate repair) may have more difficulty obtaining access to care and therefore present at a later age. This possibility drives home the importance of reducing the need for secondary interventions like MFH repair, as even primary palate repair may frequently be delayed due to lack of access.
Despite our focus on cleft lip repair, multiple studies in our review included palatoplasty cohorts and determined that palatal repair was the main contributor to MFH 54 likely due to postoperative scarring.20,21 Mars et al concluded that “palatal closure is likely to cause maxillary hypoplasia that may be severe.” 34 Bin Ye et al concluded that the results of their study “suggest that palatoplasty primarily affected the growth of maxillary alveolar process and resulted in sagittal dysplasia.” 55 Xu et al state that “repaired palates had a less protruding maxilla, short maxillary sagittal length, and unmatched jaw relationship. Thus, palatoplasty—both 1-stage and 2-stage palatoplasty—adversely affected maxillary sagittal length and position.” 56 These statements are in keeping with previous literature on the subject, which attributes MFH mainly to palatal surgery.
The average age at cephalometric measurement was less for the CL cohort than for CLP and controls. Lack of standard deviation reporting precluded statistical comparison for this variable. Using cephalometric measurements and a definition of skeletal maturity at 15 and 17 years for females and males, respectively, Laowansiri et al found that maxillary growth increased the most in all dimensions over the first 4.5 postnatal years (ages 0.4-5) compared to the subsequent 11 years (ages 5-16). 51 This study also found that vertical growth outpaces AP growth during late childhood and adolescence. 51 It is therefore possible that the CL cohort in our study was unable to demonstrate the full impact of growth restriction, although a substantial portion of the total AP growth would have been completed by the average reported age.
Our study has several limitations, including the quality of the primary data. Of the 24 studies that were identified, only 11 included cephalometric data amenable for meta-analysis. As shown in Table 5, almost no study reports the severity of the cleft palate and lip, with one paper even stating that “Studies have shown that surgical technique is not an important variable.” 50 Most studies were of a retrospective nature and therefore susceptible to bias (only one study was prospective). 19 Sample sizes of the study groups were usually small, limiting the power of each study. Control groups were inconsistent or absent. Age at the time of cephalometric measurement also varied, which may produce inconsistent results given, for example, the normalization of maxillary morphology over time noted by some.31,57
The lack of consistent reporting of data is understandable given the challenges presented by long-term follow-up. Several intercenter, regional efforts have been made to standardize outcomes reporting and protocols in cleft care. Eurocleft and Americleft efforts each produced 5-part papers with this goal in view.58,59 Unfortunately, such efforts are hindered by the complexity of the analysis employed and ultimately address a portion of the global population affected. Our group has collaborated with Operation Smile to develop a systematic approach to cleft outcomes reporting, beginning with a phenotypic analysis across a wide geographic range. 60 For cleft lip patients, the cleft width ratio (preoperative cleft width divided by commissure width) was developed in order to produce a prognostic severity scale that correlates with outcomes. 61 This measurement is simple, objective, and reproducible. A similar tool was then used to develop a severity scale for unilateral cleft palate, using a width of the cleft at the hard-soft junction, divided by the palate width. 62 These incremental, simple, globally reproducible methods are needed to both better understand the etiology of MFH, as well as accurately measure its impact and treatment.
Conclusion
This study systematically evaluates the literature regarding the association between cleft lip repair only and MFH in patients with unilateral CL or unilateral CLP. Our findings in this study suggest cleft lip repair only contributes to MFH in the setting of concurrent cleft palate pathology, and that scarring from lip repair itself is unlikely to be the predominant driver of MFH development. Given that patients with unoperated CLP appear to develop normal maxillary projection11,12 and given our exclusion of patients who underwent palate repair, it appears to be the combination of both cleft palate pathology and surgery that places patients at risk for developing MFH. However, inadequate reporting of timing, technique, follow-up time, and cleft severity precludes definitive conclusions. Our review of the available literature demonstrates that further high-quality studies are needed to elucidate the etiology of MFH in operated cleft patients. These studies should be prospective, multicenter, and employ tools that are simple, objective, and reproducible in low-resource settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.