
Abstract
Objectives
Within current research, little is known about the long-term outcomes of craniosynostosis. A priority-setting exercise by UK charity Headlines Craniofacial Support identified 2 key questions in this area: (1) What are the long-term physical and psychological effects for individuals with syndromic and non-syndromic craniosynostosis? and (2) Are individuals with craniosynostosis likely to suffer from mental health difficulties, or are they more resilient? The aim of the current study was to conduct an initial investigation of these priority questions.
Methods
A comprehensive UK-wide survey consisting of 9 standardized psychological outcome measures and open-ended questions was distributed online. Thirty-six eligible adults (69.4% female) with a mean age of 30.8 years responded to the survey. Participants reported having single suture craniosynostosis (27.8%) or syndromic craniosynostosis (52.8%), with 19.4% being unsure of their diagnosis. Sample means were compared to published norms using independent samples t tests. Qualitative responses were analysed using inductive content analysis.
Results
Compared to the general population, participants reported significantly less favorable scores related to appearance concerns, attachment in adult relationships, anxiety, optimism, and resilience. Self-worth, depression, and social anxiety scores were similar to norms. Qualitative responses provided additional insight into participants’ satisfaction with appearance, physical health, medical treatment, employment, relationships, and recurrence risks. Few participants had accessed psychological support.
Discussion
This preliminary study illustrates the potential long-term implications for individuals with craniosynostosis. Improved treatment protocols are needed to address physical health concerns in adulthood, while dedicated psychological resources are necessary to promote emotional well-being, social confidence, and resilience.
Introduction
Craniosynostosis is a relatively rare and complex condition, in which the clinical presentation can vary considerably (Kajdic et al., 2018). It occurs when 2 or more of the cranial plates fuse prematurely in utero and affects approximately 1 in every 2000 live births (McCarthy et al., 2012). Syndromic forms of craniosynostosis (including Apert, Pfeiffer, and Crouzon syndromes) are much rarer. Depending on the severity of the condition, early surgical intervention and ongoing multidisciplinary treatment throughout childhood may be necessary. Craniosynostosis can result in the individual having a visible facial difference, alongside a range of medical challenges (Kajdic et al., 2018).
In recent years, the potential psychological impacts of congenital craniofacial conditions have become more widely recognized within both clinical practice and research (Feragen and Stock, 2017). Nonetheless, the literature to date has focused predominantly on the early years, examining the psychological impacts of craniosynostosis on children born with the condition and their parents. However, studies published in the last few years have also begun to explore the longer-term outcomes of those affected, using both quantitative and qualitative methods to examine quality of life in adulthood (Feragen and Stock, 2017).
While some studies have identified a range of difficulties faced by adults with syndromic and non-syndromic craniosynostosis, including depressed mood, poor physical health, and fewer friends and romantic partners compared to controls (Stavropoulos et al., 2011; Tovetjärn et al., 2012; Fischer et al., 2014), others have found adults with craniosynostosis to report equal or superior quality of life to the general population (Lloyd et al., 2016; Mazzaferro et al., 2018; Salokorpi et al., 2019). Correspondingly, a recent review of the craniofacial literature (Feragen and Stock, 2017) reported that findings in regard to psychological adjustment to craniofacial conditions were largely inconclusive. The authors of the review concluded that, rather than assessing broad quality of life, researchers should seek to examine individual domains of psychological well-being. The authors also recommended an increase in the use of qualitative methods to elicit a more holistic understanding of what it is like to live with a craniofacial condition, and a need to investigate the positive, as well as the negative impacts. Finally, collection of samples including both syndromic and non-syndromic cases was recommended, so that any differences and/or commonalities across diagnostic subtypes can be explored.
In the United Kingdom (UK), care for those affected by craniosynostosis is delivered by 5 supra-regional specialist units, with additional community-based support offered by Headlines Craniofacial Support (Headlines), a UK-wide organization that became a registered charity in 1996. Over the years, Headlines has developed a range of services, including a helpline, a welfare fund, information leaflets, family events, fundraising activities, e-newsletters, and a biennial conference. However, Headlines currently offers little for adults. Similarly, the 5 specialist units did not exist when the majority of today's adults were growing up, and are not currently commissioned to provide care throughout adulthood. As such, the current adult population has received comparatively less support.
In 2017, Headlines carried out a wide-ranging consultation with their members and with health professionals working in the field to produce a list of priority research questions. Two of these priorities focused on long-term outcomes: (1) What are the long-term physical and psychological effects for individuals with syndromic and non-syndromic craniosynostosis? and (2) Are individuals with craniosynostosis likely to suffer from mental health difficulties, or are they more resilient? The aim of the current study was to conduct an initial exploration of these 2 priority research questions via the administration of a comprehensive UK-wide survey among adults with syndromic and non-syndromic craniosynostosis.
Methods
Design
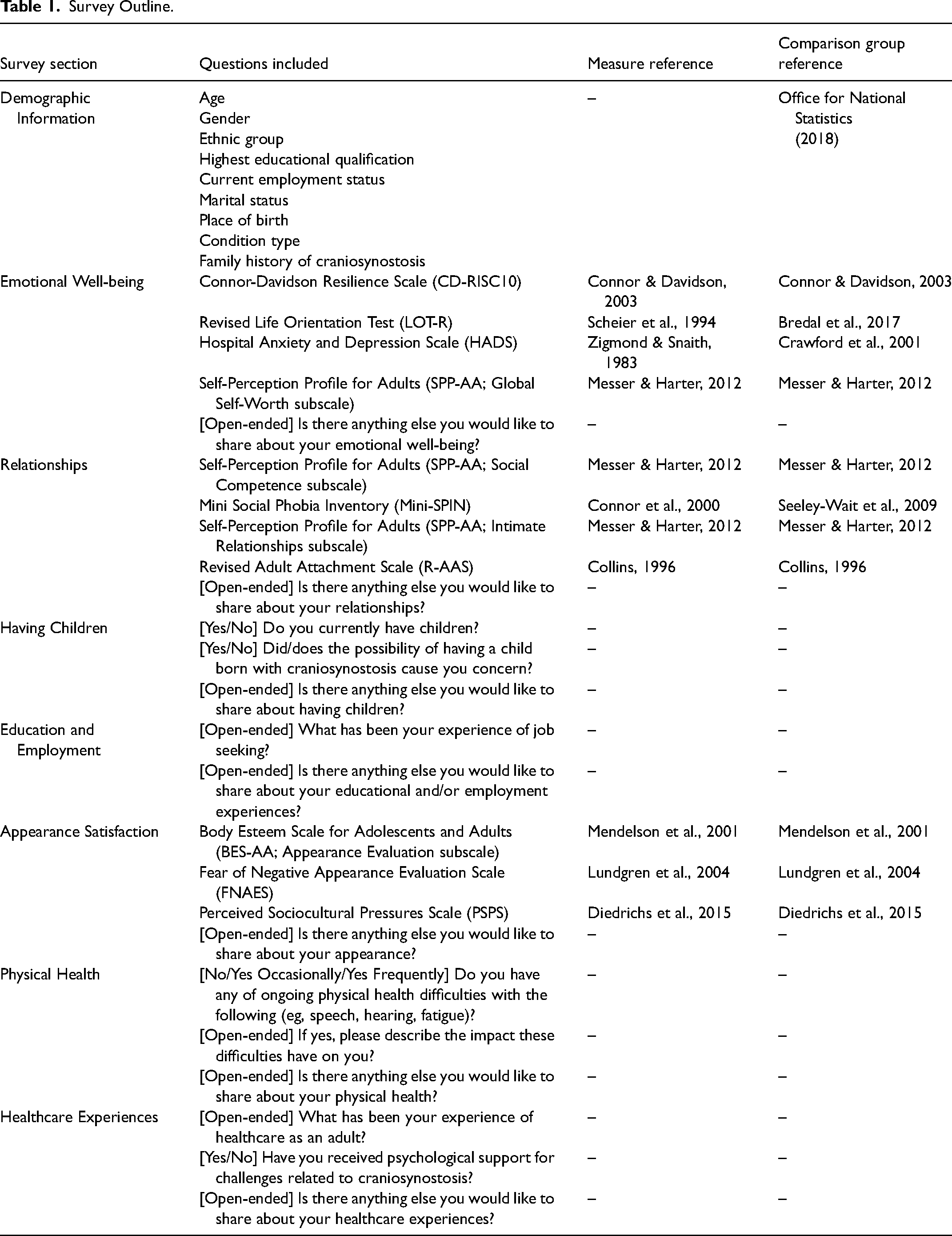
Ethical approval to conduct the study was obtained from the Faculty Research Committee at the University of the West of England. An online survey (Table 1) was designed using the platform Qualtrics, drawing upon current craniofacial literature (eg, Feragen and Stock, 2017) and clinical and research expertise. The survey consisted of 9 standardized patient-reported outcome measures, chosen for their psychometric properties, clinical utility, the availability of general population norms, and for consistency with related studies (see Stock et al., 2020a for a review). Topics of interest included satisfaction with appearance, social experiences, symptoms of anxiety and depression, physical health, self-worth, and resilience. Demographic data were also collected (Table 2), alongside open-ended questions for participants to provide more detail if they wished. Clinical psychologists from the 4 specialist units in England and 10 adults born with craniosynostosis provided feedback on the study design and draft materials. A version of the survey was also administered to parents of children born with craniosynostosis, the findings of which are detailed in separate papers (under review).
Survey Outline.
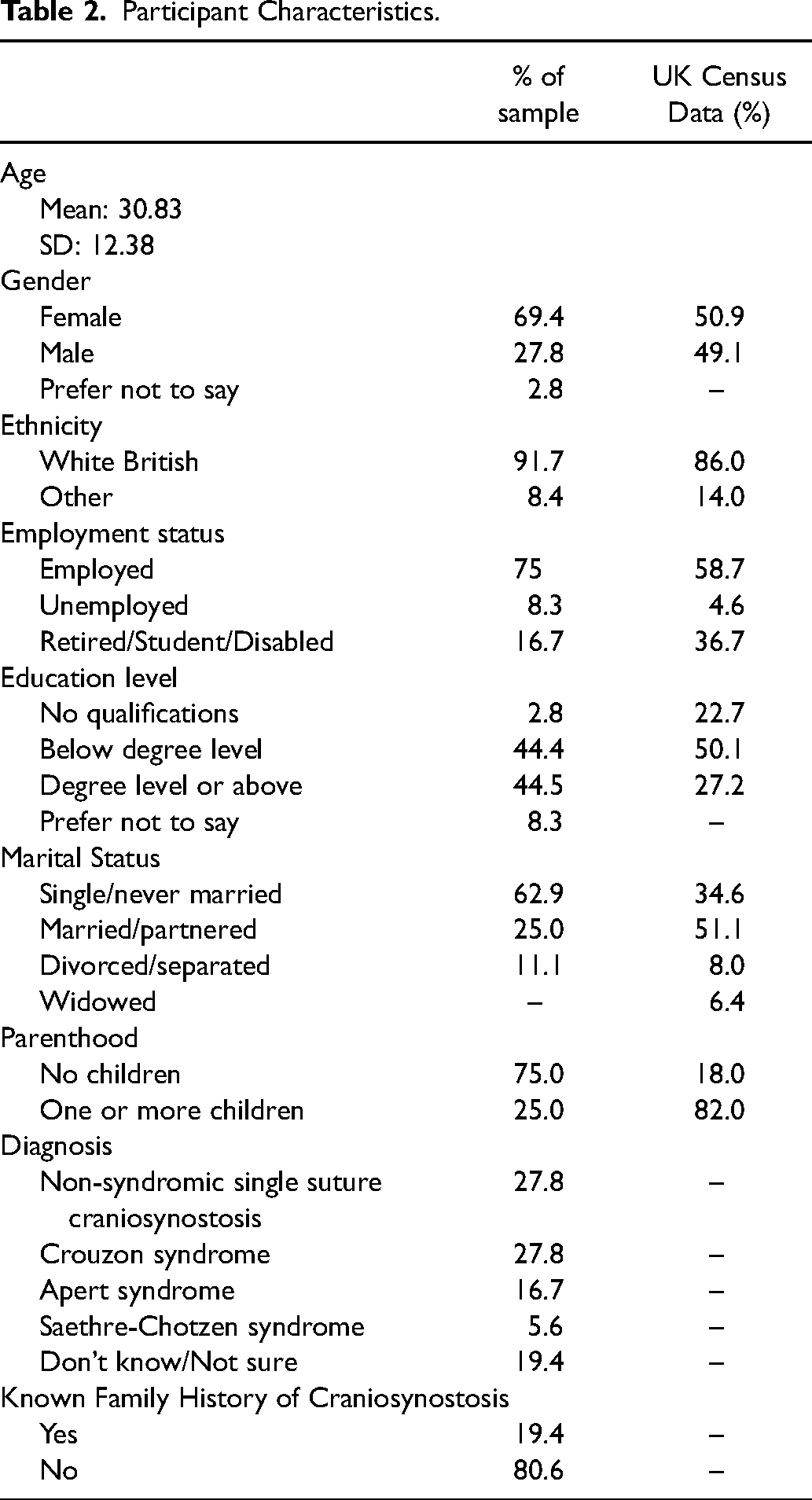
Participant Characteristics.
Procedure
A link to the online survey was distributed on relevant websites, social media, and e-newsletters inviting adults with craniosynostosis to take part. Before proceeding to the survey itself, participants were asked to read the Participant Information and Privacy Notice, and to indicate their consent to participate. Participants were eligible if they were born with craniosynostosis, aged 16 years or older, living in the UK, and understood written English well enough to provide informed consent. Both individuals with syndromic and non-syndromic craniosynostosis were invited to participate, in order to be inclusive (Feragen et al., 2014) and in an attempt to address the research priority questions in full. The survey was launched in October 2019 and remained open to responses until April 2020.
Analysis
A review, verification and validation of quantitative data was undertaken prior to analysis. To examine possible differences across the sample according to syndromic status, independent samples t tests were carried out. In 7 cases, the syndromic status could not be determined and these participants were excluded from the exploratory analysis.
Sample means were generated and compared to published general population data obtained from Europe and the United States (Table 1) using independent samples t tests. Cohen's d was also calculated, whereby a value of 0.2–0.5 represents a small effect, 0.5–0.8 represents a medium effect, and 0.8 or more represents a large effect (Cohen, 1988). Pearson's Correlation was used to assess the relationship between outcome measures. For statistically significant correlations, r values of approximately 0.1 in magnitude are considered to represent a small effect, 0.3 to represent a medium effect, and 0.5 to represent a large effect (Cohen, 1988).
Qualitative data were analysed independently using inductive content analysis (Hsieh and Shannon, 2005) by the first and second authors, who are trained in qualitative methods. First, the data were read and re-read, to establish an overall picture of the data. Common codes were then inductively grouped together in an iterative process and discussed until full agreement was reached. Finally, frequency counts were calculated. Preliminary findings were shared with patient representatives and clinical psychologists, and their feedback was integrated into the final paper.
Results
Thirty-six eligible adults born with craniosynostosis responded to the survey, with between 31 and 34 participants completing each of the standardized measures. Participants had a mean age of 30.4 years (SD 12.4) and were predominantly White British (91.7%) and female (69.4%). Compared to National Census data (Office for National Statistics, 2018; Table 2), the current sample had slightly raised levels of unemployment, despite being well educated on average. Participants were also more likely than the general population to be single and/or without children. The most common diagnoses reported were single suture craniosynostosis (27.8%) and Crouzon syndrome (27.8%). Most participants did not have a known family history of craniosynostosis.
No differences were found between adults with syndromic and non-syndromic diagnoses, with one exception, where adults with non-syndromic craniosynostosis (M = 3.19, SD = 0.273) reported significantly lower self-perceived competence in intimate relationships than adults with syndromic craniosynostosis (M = 3.50, SD = 0.364), t(25) = −2.218, P = .036, d = 0.964.
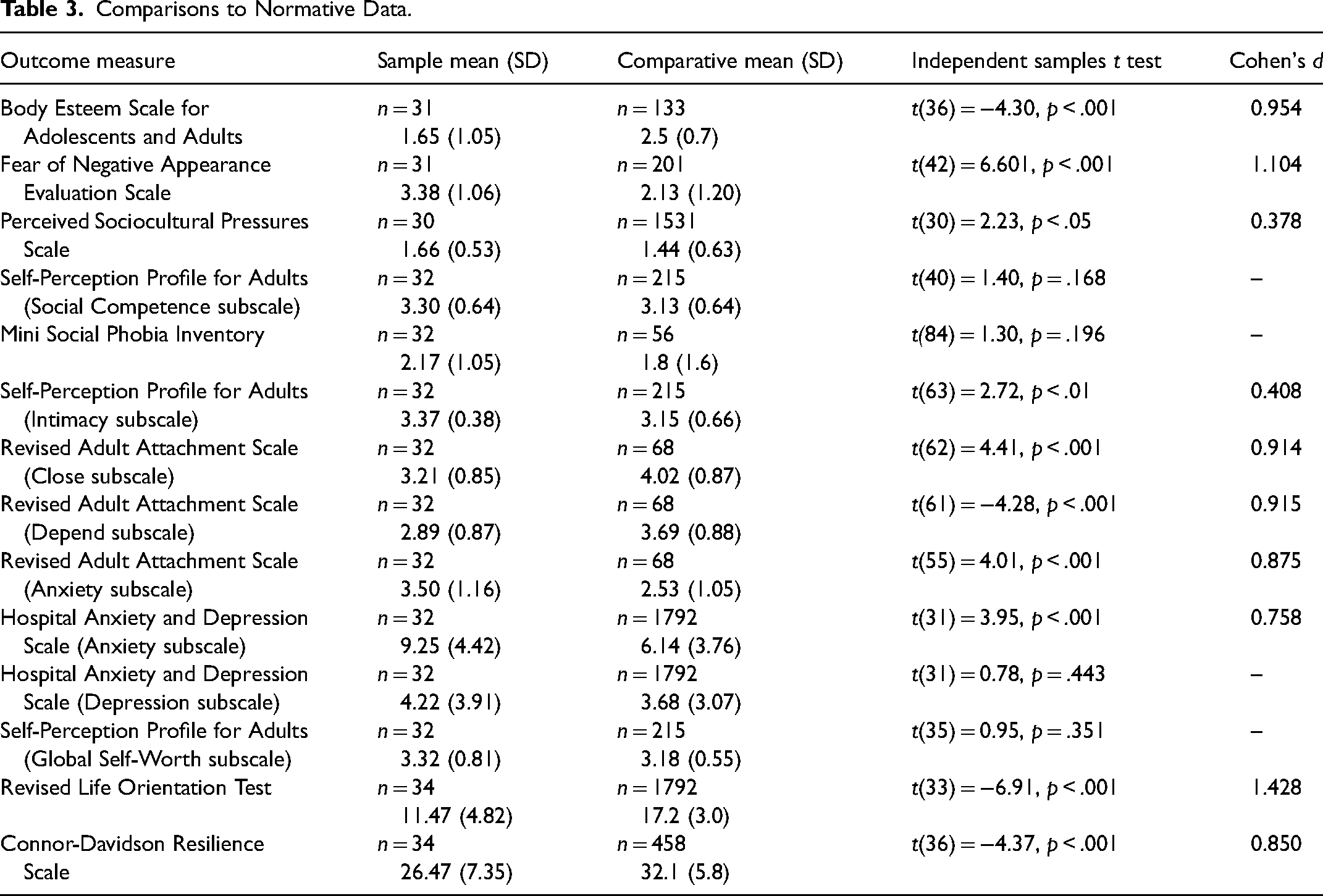
In comparison to the general population (Table 3), participants reported significantly more fear of negative appearance evaluation, poorer body image, and more pressure to conform to societal appearance ideals. Adults with craniosynostosis also reported significantly less comfort in adult relationships compared with the general population. Levels of optimism and resilience were significantly lower in adults with craniosynostosis compared to general population norms, and symptoms of anxiety were significantly elevated. However, levels of social anxiety, self-perceived social competence, depression, and self-worth were similar to the general population. Despite describing a range of ongoing challenges, only one participant (3.2%) reported having accessed psychological support as an adult.
Comparisons to Normative Data.
Pearson's Correlation analyses found that most outcomes were correlated to varying degrees (r = 0.042 to 0.838; Table 4). The most common physical complaints among adults with craniosynostosis were fatigue (51.6%), hearing difficulties (45.2%), vision problems (41.9%), migraines (38.7%), and dental issues (35.5%).
Associations Between Outcome Measures.
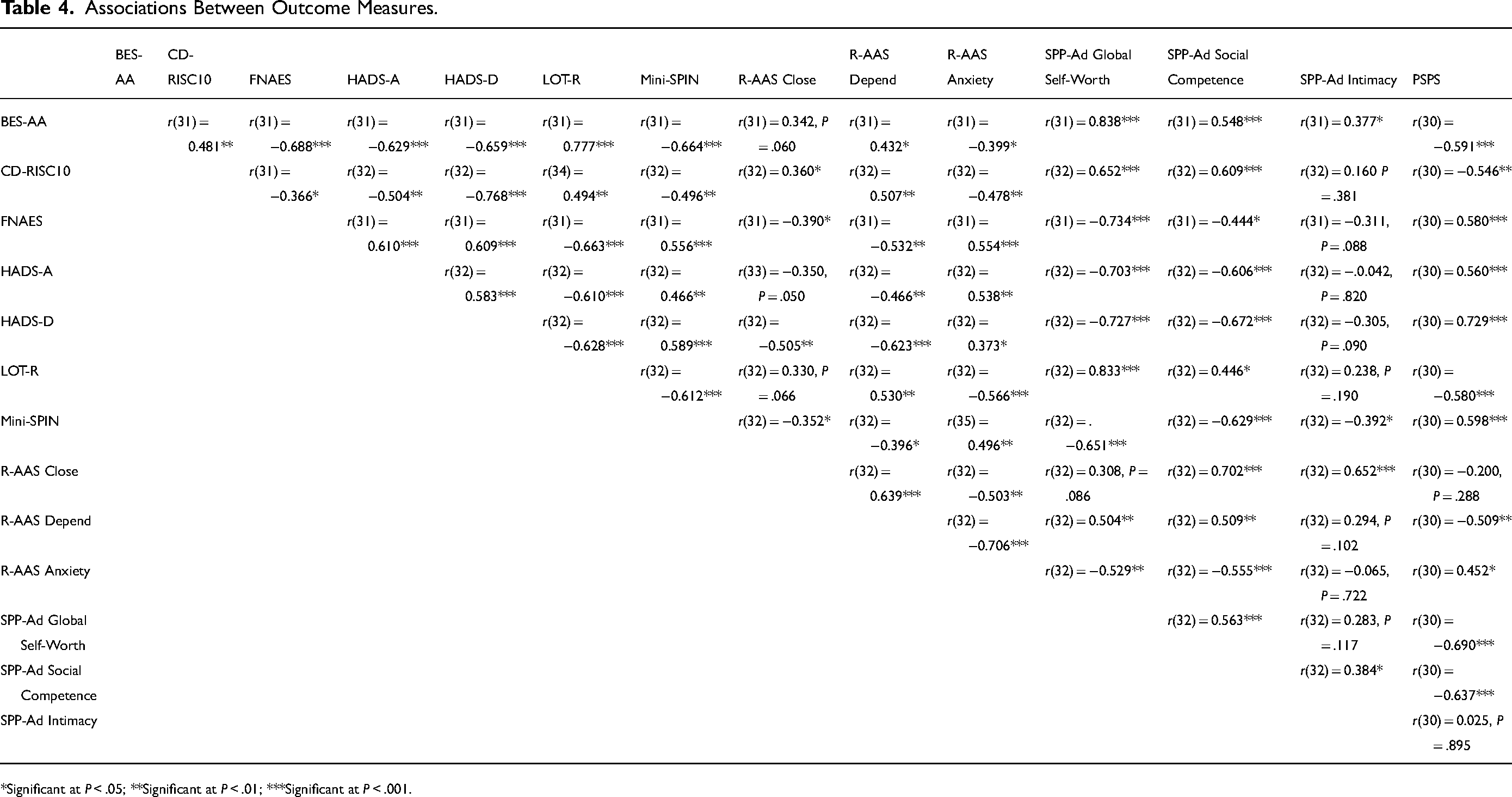
*Significant at P < .05; **Significant at P < .01; ***Significant at P < .001.
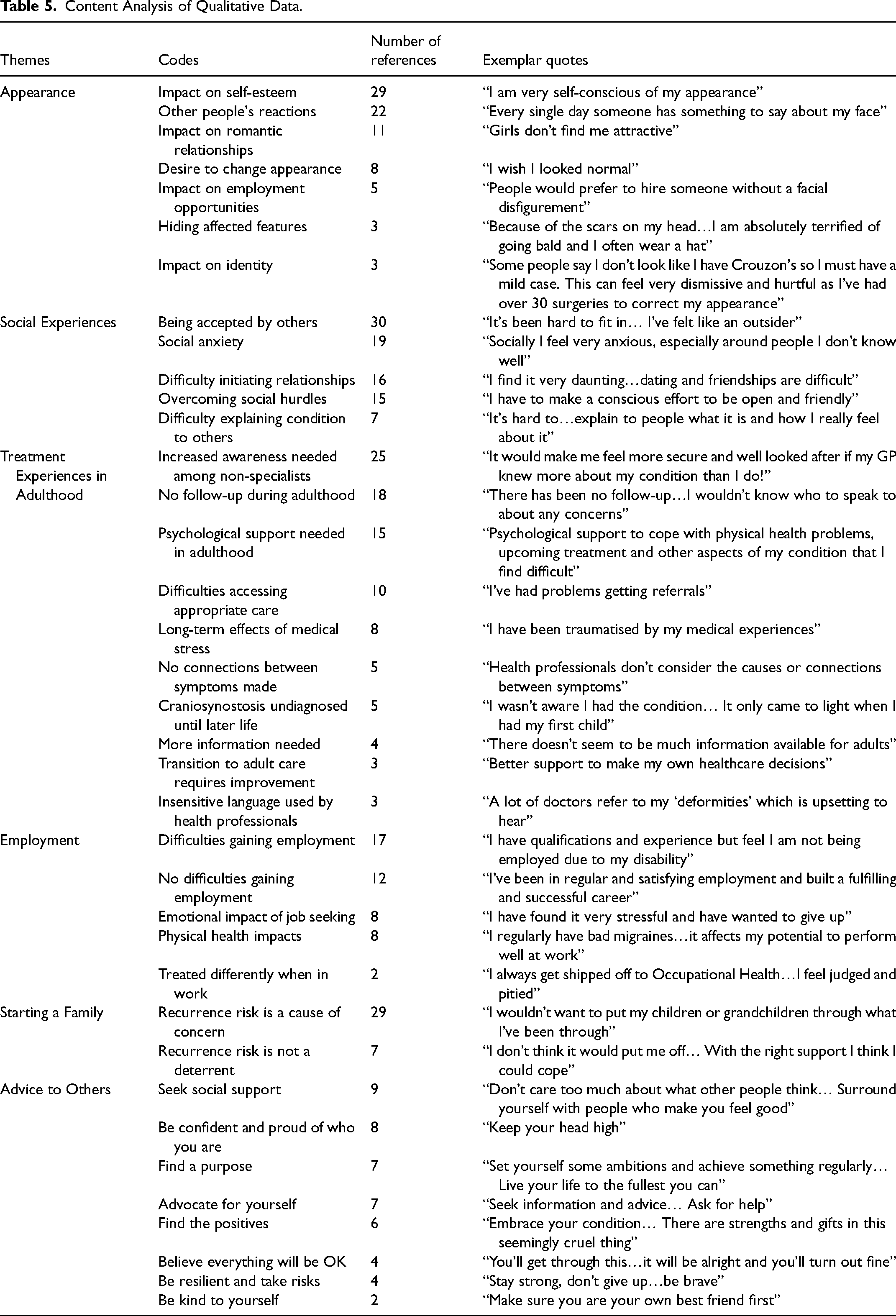
Common themes, codes, exemplar quotes, and frequency counts extracted from the qualitative data are provided in Table 5. Participants described how their appearance impacted on their self-esteem, romantic relationships, employment opportunities, and identity. They also outlined how having a difference that was visible to other people could evoke unwanted reactions, and a desire to hide/change their appearance. Social impacts of craniosynostosis included difficulties in feeling accepted by others, initiating new relationships, overcoming social hurdles, and explaining the condition to others. Participants also reported experiencing symptoms of social anxiety. In terms of treatment, participants reported challenges with the transition to adult care, a lack of follow-up from their craniofacial team during adulthood, and a desire for more information and psychological support. A lack of awareness of craniosynostosis among non-specialist health professionals was identified, alongside difficulties obtaining treatment referrals, important connections between symptoms being missed, and insensitive language being used during consultations. Some participants had not been made aware of their condition until adulthood. Participants also reported a cumulative effect of repeated medical stress on their mental well-being. Another theme identified in the qualitative data was employment, with different views on how much craniosynostosis had impacted participants in terms of finding work. Participants identified the emotional impact of job seeking, and felt their condition affected them regularly while in work. For the majority of participants, recurrence risk was a concern when considering starting a family, yet others did not feel this was a significant deterrent. Finally, participants offered advice to others with craniosynostosis. These were all positively framed in nature and reflective of adaptive self-care practices.
Content Analysis of Qualitative Data.
Discussion
The aim of the current study was to conduct an initial exploration of 2 of the priority research questions set by leading UK charity, Headlines: (1) What are the long-term physical and psychological effects for individuals with syndromic and non-syndromic craniosynostosis? and (2) Are individuals with craniosynostosis likely to suffer from mental health difficulties, or are they more resilient? Findings are discussed below in the context of current literature, and recommendations for future research and practice are made.
Synthesis of Findings
On average, adults who participated in this study were less satisfied with their appearance, were more afraid of others judging them based on appearance, and felt more pressure to conform to societal appearance ‘ideals’ than adults without craniosynostosis. Participants reported these appearance concerns to have a negative impact on their self-esteem, romantic relationships, employment opportunities, and identity. Although 2 previous studies found adults with syndromic and non-syndromic craniosynostosis to be generally satisfied with their appearance (Raposo-Amaral et al., 2012; Salokorpi et al., 2019), findings from the current study align with research from the wider field of health psychology, which indicates that adults with appearance-altering conditions are liable to struggle with appearance pressures and other people's reactions, irrespective of the objective ‘severity’ of the condition (Rumsey and Harcourt, 2012). Strategies such as hiding affected features can be useful in the short-term, but the underlying psychological discomfort is likely to persist (Rumsey and Harcourt, 2012). Equally, seeking a more permanent change in appearance through surgery and/or other treatment can enhance well-being, but can also trigger individuals to question their sense of self or identity (Stavropoulos et al., 2011; Myhre et al., 2021). In line with broader research, the data therefore suggest that psychological interventions could seek to address appearance-related anxiety using evidence-based approaches, preferably starting in early adolescence (eg, Clarke et al., 2013).
Participants reported similar levels of social anxiety and social competence to the general population. However, qualitative responses highlighted difficulties with ‘fitting in’ and explaining craniosynostosis to others, which invoked anxiety in certain social situations and made initiating relationships problematic for some. Previous research has described how having a health condition, particularly one that is visible to others, can result in fewer friendships and romantic relationships (Stavropoulos et al., 2011; Tovetjärn et al., 2012; Fischer et al., 2014; Sakamoto et al., 2021). When discussing adult relationships, participants reported anxiety about being abandoned or unloved, as well as discomfort with closeness and intimacy, and a lack of belief that other people can be relied upon. Similar findings were identified in a recent survey of adults with cleft lip and/or palate using the same measures (Ardouin et al., 2021b), and together suggest this could be a particular challenge for adults with craniofacial conditions. However, participants also stated they actively used positive coping strategies to overcome social barriers, such as conversational skills, positive body language, and explaining their condition to others; a finding replicated in other studies of craniosynostosis (Stavropoulos et al., 2011; Raposo-Amaral et al., 2012). Given the importance of social connection in people's lives, psychological interventions could therefore focus on developing helpful coping strategies and social skills from a young age (Kapp-Simon et al., 2005).
For most participants, the recurrence risk of craniosynostosis was a cause for concern in relation to starting a family. This has also been identified in other studies, particularly in the case of syndromic diagnoses (O’Hanlon et al., 2012; Phipps and Skirton, 2017) and may offer some explanation for the observed higher rate of childlessness within the sample. Current understanding of the genetic and environmental causes of craniosynostosis also remains limited, and therefore so does the information available to young adults (Wilkie et al., 2017). However, some participants did not believe the recurrence risk to be a significant deterrent and felt they could cope if their child was born with craniosynostosis. One study of adults born with cleft lip and/or palate found adults’ attitudes toward recurrence to be largely determined by their own psychological adjustment [Stock and Rumsey, 2015], suggesting that if young people are supported to cope well with the challenges they are presented with as they grow, they will view craniosynostosis more positively in adulthood and feel more at ease about starting a family of their own.
Reported experiences of employment were mixed, with some describing few difficulties in work settings and others stating that their condition impacted their work life considerably. Although the UK Equality Act (2010) provides legal rights for people with physical disabilities and appearance-altering conditions, discrimination remains common in the workplace (Changing Faces, 2017) and within society more broadly (Roberts, 2014). Taken together, these findings suggest that improved awareness among both employers and employees may help to reduce stigma, while more targeted interventions to increase adults’ confidence when applying for and entering employment may be helpful for the individual.
Adults participating in the current study reported a range of physical health concerns and treatment needs, alongside a lack of awareness of craniosynostosis among non-specialist health professionals, such as General Practitioners. Combined with the lack of follow-up in adulthood, this could lead to difficulties accessing appropriate information and treatment, with participants reportedly being left to self-manage their physical and psychological health. Similar findings have been reported previously among adults with cleft lip and palate and other craniofacial conditions (Tovetjärn et al., 2012; Ardouin et al., 2021a), and suggest that a large number of adults may be receiving inappropriate treatment, no treatment at all, and/or facing long and frustrating referral times. While health professionals cannot be expected to possess specialist knowledge on every condition they treat, access to educational materials when needed may provide a broad understanding of craniosynostosis and reduce uncertainty surrounding the best approach to care (Stock and Costa, 2020), with the ultimate aim of improving adults’ treatment experiences.
Finally, adults with craniosynostosis reported more symptoms of general anxiety than norms, in addition to lower levels of optimism and resilience. Given that today's adults did not have access to specialist care or psychological support while growing up, they may be more prone to psychological distress. However, participants also offered advice to others with craniosynostosis, all of which was positively framed and indicative of self-care practices. In light of the view that optimism is a skill that can be learned (Seligman, 1991), the current study lends further support for examination of interventions aimed at increasing optimism and resilience within the context of craniofacial conditions. Future research that replicates the present study and others like it will be important to determine whether and how the current organization of UK care for craniosynostosis has led to improvements.
Associations Between Outcomes and Psychological Domains
Almost all outcomes were correlated to some degree in the current study. In particular, global self-worth was strongly associated with a range of outcomes, including body esteem, fear of negative appearance evaluation, perceived sociocultural pressures, social anxiety, general anxiety, depressive symptoms, optimism, and resilience. This indicates that interventions targeted at increasing self-worth could have a potential protective effect across a range of psychological domains, making it a particularly important variable for further investigation.
Outcome variables were also categorized into 3 core domains of psychological adjustment: emotional (Global Self-Worth, HADS, LOT-R, CD-RISC10 and SPIN), social (Sociability, Intimacy and RAAS), and appearance-related (BES-AA, FNAES and PSPS). Findings suggest a strong association between emotional adjustment and appearance, between emotional adjustment and social adjustment, and to a lesser extent, between appearance and social adjustment. Previous craniofacial studies have also found associations between the different domains of psychological adjustment (eg, Roberts and Mathias, 2013; Feragen et al., 2015; Costa et al., 2021). Taken together, these findings suggest that intervening in one domain may indirectly improve adjustment in other domains. Further work is needed to confirm these associations and to assess the utility of this approach for psychological intervention.
Future Directions
Supported by previous research in the field of cleft and craniofacial conditions, this small-scale study has illustrated the potential long-term physical and psychological impact of craniosynostosis. Treatment needs may continue into adulthood, particularly in the case of those who received care prior to the integration of psychologists within specialist units. Commissioning support for adults with ongoing healthcare needs should be considered, in addition to an improved awareness among non-specialists to improve the patient experience and the timeliness and relevance of referrals. Psychological support needs in adulthood may include coping with appearance-related anxiety, initiating and maintaining friendships and romantic relationships, family planning, support in the workplace, and resilience-building. Future research should aim to further develop the evidence base for psychological intervention. In the meantime, health professionals could consider a variety of ways in which they can support their patients’ psychological and holistic needs (Stock et al., 2020b).
Methodological Considerations
This study represents an initial enquiry into 2 research priorities set by patient and parent representatives and health professionals in the area of craniosynostosis. The survey was largely based on robust, standardized measures consistent with other studies in the field. Along with the additional qualitative data collected, the survey allowed for key psychological and physical impacts of craniosynostosis in adulthood to be identified and preliminary recommendations for next steps to be made.
Nonetheless, a number of methodological limitations must be acknowledged. First, the sample obtained remained relatively small and, crucially, heterogenous. This made further analyses to investigate demographic and treatment-related variables unfeasible, and prevented the possibility of identifying predictors of psychological adjustment. Despite large effect sizes, the findings of this study should therefore be interpreted with caution and replicated using larger samples in future. Few differences between syndromic and non-syndromic cases were detected, which is contrary to previous literature (Feragen and Stock, 2017) and which could be attributed to a lack of power. While a greater impact of a syndrome should not be presumed, larger samples are needed to effectively examine potential variations across subgroups, including any additional impacts of cognitive impairment and other associated conditions (Feragen et al., 2014). Additionally, some participants were unaware of their exact diagnosis, and without medical records this makes the data more difficult to interpret. Future studies should also seek to include a matched control group where possible, rather than to rely upon general population norm data alone. Last, participants were predominantly recruited through Headlines and therefore cannot be assumed to be representative of the UK adult craniosynostosis population as a whole. Adults are a challenging group to recruit to research, since they are unlikely to be engaged in craniofacial treatment (Ardouin et al., 2021a). This is possibly most applicable to certain subgroups, such as those with less complex synostosis, who may have received little treatment since infancy and/or who may not identify with the diagnosis. Although online surveys attempt to bridge this gap and reach more individuals, there may have been several selection factors that narrow the generalizability of the results.
Conclusions
This initial investigative study illustrates the potential long-term physical and psychological implications for individuals born with craniosynostosis. Improved treatment protocols are needed to address physical health concerns in adulthood, while dedicated psychological resources are necessary to promote emotional well-being, social confidence, and resilience throughout the lifespan. Future studies should include large-scale qualitative investigation, alongside combined efforts to achieve representative quantitative data allowing for investigation of predictor variables, demographic variables, and subtype analyses. Additional research aimed at improving understanding of craniosynostosis in primary care is warranted. Finally, further development of the evidence base for psychological intervention is needed, from the point of diagnosis onward.
Footnotes
Acknowledgments
Thank you to our Public Involvement representatives and Dr Natasha Rooney for their input into the design of this study, and to Aida Mikkola for her assistance with the analysis. We are especially grateful to all study participants for candidly sharing their experiences with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the VTCT Foundation