
Abstract
Objective:
To document and analyze the overall longitudinal institutional treatment experience of children with nonsyndromic Robin sequence (RS) from infancy to early adulthood.
Design:
Retrospective longitudinal treatment review.
Setting:
A tertiary-care, referral, teaching hospital.
Patients:
Children with nonsyndromic RS and cleft palate (N = 117) born between December, 1985, and January, 2012.
Interventions:
Data regarding airway management, nutritional management, audiological interventions, orthodontic treatment, and surgical interventions were documented and analyzed in different growth/developmental stages. Comparative data from other international centers were collected from the literature.
Results:
Airway management during infancy involved prone positioning (92%), nasopharyngeal airway (6%), tracheostomy (2%), and mandibular distraction osteogenesis (1%). Feeding with nasogastric, gastrostomy, and/or gastrojejunostomy tubes was used in 44%, Haberman feeders in 53%, and Mead Johnson feeders in 3%. Gastroesophageal reflux disease was documented in 6% of the sample. During childhood and early adolescent years, pharyngeal flap surgery was carried out in 22% of the children, while 11% had secondary palatal surgery. Audiological management included the use of tympanostomy tubes in 62%, with several children needing multiple tube replacements. At least 18% were diagnosed with obstructive sleep apnea. Adenoidectomy or adenotonsillectomy was undertaken in 4%. Analysis of data pertaining to middle childhood and adolescent years showed that orthodontic treatment was conducted for most children for crowding, tooth agenesis, and skeletal and/or dental dysplasia. Orthognathic surgery frequency (<18%) was low.
Conclusions:
Institutional treatment experience of children with nonsyndromic RS involves multidisciplinary care at different ages and stages of their development.
Introduction
In 1923, Pierre Robin described the triad of micrognathia, glossoptosis, and resultant airway obstruction in neonates, adding cleft palate as an aggravating factor in a later publication (Robin, 1923, 1934). These features are now recognized as Robin sequence (RS). The prevalence of RS ranges from 1 in 8500 to 1 in 20 000 births, with cleft palate being present in up to 90% of these children (Bush & Williams, 1983; Caouette-Laberge et al., 1994; Tolarová & Cervenka, 1998). Despite the fact that this clinical entity is well recognized for almost a century, there is wide variability in the diagnosis and care of children with RS, and systematic evaluations of treatment approaches are lacking.
With mandibular micrognathia, severe neonatal respiratory distress, glossoptosis, and cleft palate being major elements of this entity, burdens of treatment throughout infancy and childhood revolve around these features and their effects.
Upper airway obstruction, the first sign which requires urgent medical attention in neonates born with RS, and related feeding difficulties present in a heterogeneous manner. These may range from mild respiratory and feeding problems to severe crisis of asphyxia that can be fatal in the absence of immediate medical intervention (Evans et al., 2011). The severity of the compromised airway is usually assessed with endoscopic evaluation in order to determine the optimal intervention (Evans et al., 2011). These intervention methods include both conservative and surgical techniques. Prone positioning, allowing the mandible and tongue to be placed forward, is thought to be successful in at least half of children with RS (Sjolin, 1950; Pashayan & Lewis, 1984; Wagener et al., 2003; Evans et al., 2006). If this fails, other interventions can be used such as nasopharyngeal and endotracheal intubation (Stern et al., 1972; Wagener et al., 2003; Evans et al., 2011), positive pressure ventilation in the form of continuous positive airway pressure (CPAP; Van den Elzen et al., 2001), head braces or suspension caps (Dennison, 1965), or palatal plates and mandibular traction devices (Davis & Dunn, 1933; Callister, 1937; Pradel et al., 2009; Poets et al., 2019; Poets et al., 2021). In severe cases of persistent airway obstruction, surgical methods such as glossopexy in the form of tongue-lip adhesion (Argamaso, 1992; Evans et al., 2011), subperiosteal floor of mouth release (Caouette-Laberge et al., 2012), mandibular distraction osteogenesis (Dauria & Marsh, 2008; Cheng et al., 2011; Evans et al., 2011), and tracheostomy are indicated (Chigurupati & Myall, 2005; Cheng et al., 2011). Feeding difficulties are managed either by special nipples and cleft palate bottles or by nasogastric feeding tubes in 38% to 62% of infants with RS (Elliott et al., 1995; Li et al., 2002; Evans et al., 2006).
Patients with RS require long-term care, with management spanning a very long time from the neonatal period through infancy and childhood. Even after infancy, children can present problems in facial growth and development (Figueroa et al., 1991; Laitinen et al., 1997; Daskalogiannakis et al., 2001; Matsuda et al., 2006; Suri et al., 2006; Suri et al., 2010), obstructive sleep apnea (OSA; Anderson et al., 2011; Evans et al., 2011), auditory (middle-ear dysfunction) problems (Glynn et al., 2011), and speech problems (Thouvenin et al., 2013). It has been reported that children with nonsyndromic RS present bimaxillary retrognathism, mandibular deficiency, and a more hyperdivergent growth pattern when compared with unaffected children (Suri et al., 2010; Do et al., 2019). Patients who normalize their maxillomandibular discrepancy and even mandibular length were described in a recent systematic review (Purnell et al., 2019) to be the exception rather than the rule, indicating that some form of treatment will be required to correct existing dentofacial deformities. Orthodontic treatment, as well as orthognathic surgical intervention at skeletal maturity, when indicated, can improve the skeletodental malocclusions, facial, and dental esthetics.
The management of children with RS is challenging and requires interdisciplinary collaboration by many specialists. The existing literature contains publications related to identifying different aspects of the management at different stages of infancy and childhood but do not present a consolidated, longitudinal documentation of the institutional multidisciplinary treatment aspects each patient undergoes. Previous studies have focused predominantly on the methods of relieving airway compromise and feeding difficulties caused by RS during infancy. However, inadequate attention has been given to documenting the other interventions patients with RS undergo from infancy to their growth completion. Consequently, a consolidated report that documents the multidisciplinary institutional treatment aspects longitudinally in a cohort of patients is lacking. The purpose of this study was to examine, using a comprehensive retrospective longitudinal analysis, the overall institutional multidisciplinary treatment in children born with nonsyndromic RS, who underwent the treatment protocol at one craniofacial center.
Methods
The hospital’s Research Ethics Board approved this study prior to data collection. A retrospective chart review of children born with nonsyndromic RS from December, 1985, to January, 2012, was performed using patient records from The Hospital for Sick Children in Toronto, Canada. Inclusion criteria were the following:
– Children having a diagnosis of RS with cleft palate.
– Children having been followed longitudinally at the same institution from birth until early adulthood or the latest age at which data were available.
– Exclusion criteria were the following:
– Children with RS associated with a syndrome or other anomalies.
– Patients with incomplete or non-decipherable case notes pertaining to the intervention being documented.
– Children not having completed their follow-up examinations and treatments at the same institution.
– The information that was retrospectively collected for each of the included patients comprised:
– Demographic information,
– Airway management,
– Nutritional management,
– Audiological management,
– Any additional surgical interventions necessary, in relation to the diagnosis of RS (eg, pharyngeal flaps),
– Speech therapy,
– Presence of OSA and its management, and
– Orthodontic management.
Descriptive statistics were reported based on percentages of the sample that underwent the intervention being documented, within the age range described.
Available comparative data from other international centers regarding each of these interventions were also collected from publications in the peer-reviewed literature.
Results
Sample
A total of 117 children (55 boys and 62 girls) born between December, 1985, and January, 2012, with nonsyndromic RS and who were treated at The Hospital for Sick Children, Toronto, were included in the present study. Clinical data related to medical interventions we aimed to collect of their infancy period were available for almost all 117 children. Data were collected according to the intervention list described in Methods, till December, 2020, where available. There were 13.5% children whose data were available only below age 12 years, while for others, longitudinal data were available till later ages. Dental charts including orthodontic notes from the age of 5 years and older were available for 110 patients at different ages (described later). Data were analyzed in relation to the age-group at which interventions were typically performed. Almost 86% of the children whose cleft shape was recorded in the charts were seen to have a U-shaped palatal cleft while 14% had a V-shaped palatal cleft.
Airway Management
Airway obstruction was managed most commonly with prone positioning during infancy (in 91.5% of the sample). Other methods used, albeit more infrequently, were nasopharyngeal tube placement (5.7%), tracheostomy (1.9%), or mandibular distraction osteogenesis (0.9%; Figure 1). No patient underwent tongue lip adhesion or the placement of a palatal plate for airway management.
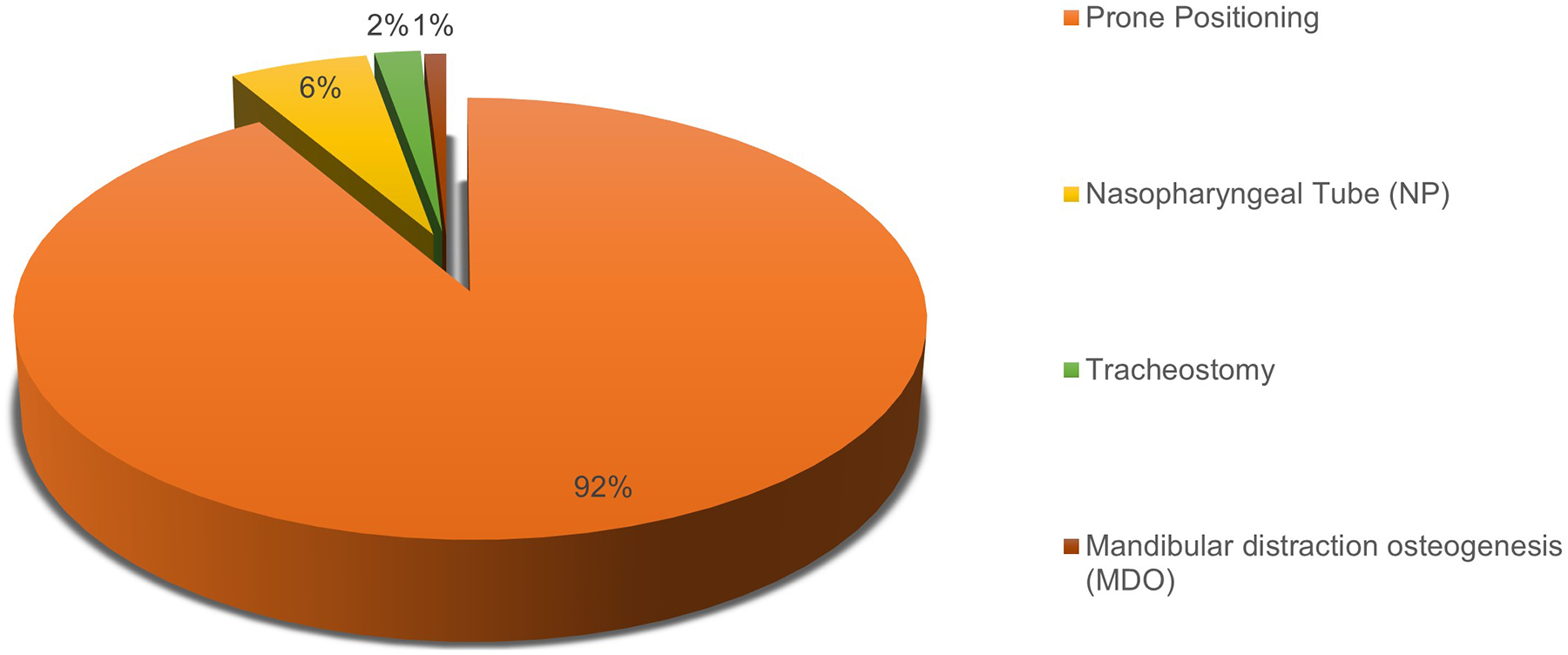
Neonatal and early infancy airway distress and/or obstruction management.
Nutrition
Nutritional management during infancy was most often by means of the Haberman feeder (53.3% of children). More invasive management methods were used in 43.8% of patients and this included the placement of nasogastric (NG-), gastrostomy (G-), or gastrojejunostomy tubes, with or without the addition of the Haberman feeder (Figure 2). Less than 6% of children were diagnosed with gastroesophageal reflux disease (GERD).
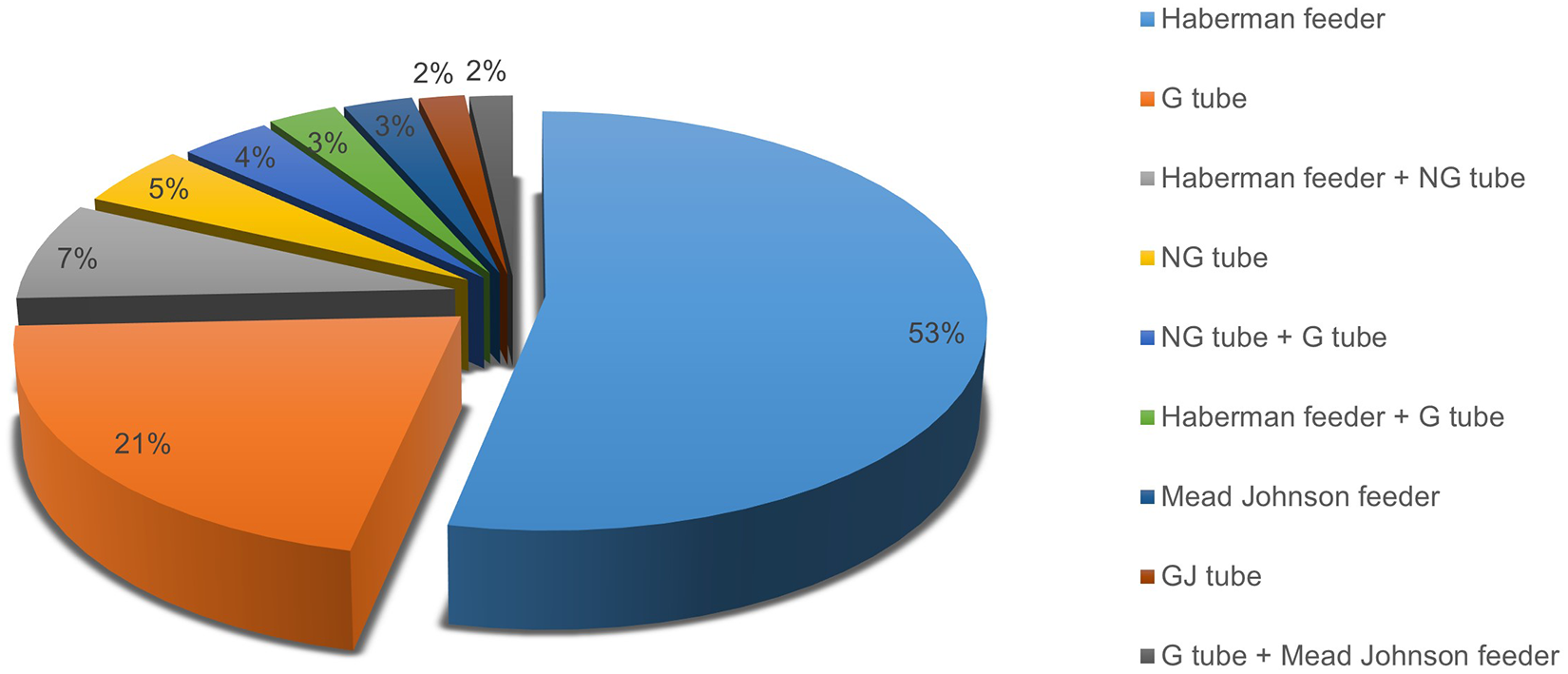
Nutritional management in infancy and early/middle childhood.
Audiology
Audiological management was necessary in 61.5% of infants and the younger children and this was via the placement of tympanostomy tubes. In many infants, tubes had to be replaced one or more times during childhood.
Additional Surgical Interventions
Primary palatoplasty was conducted at the mean age of 1.4 ± 0.5 years. Most children (62.4%) did not require any additional surgical interventions during early or middle childhood or in the earlier part of adolescence. Pharyngeal flap surgery for velopharyngeal insufficiency (VPI) was conducted in 22.2%, 11.1% underwent secondary palatal surgery, and 4.3% had adenoidectomy or adenotonsillectomy (Figure 3). Within the number of children who received pharyngeal flap surgery, 16.2% had a pharyngeal flap alone (with 4.3% requiring simultaneous fistula repair), 0.9% underwent a flap revision later, 4.3% underwent a second surgery later for fistula closure, and 0.9% required a second palatoplasty. Of the children who required secondary palatal surgery, 85% had this operation in order to treat VPI and 15% for fistula repair. Patients who required secondary palatal surgery underwent a Furlow palatoplasty.
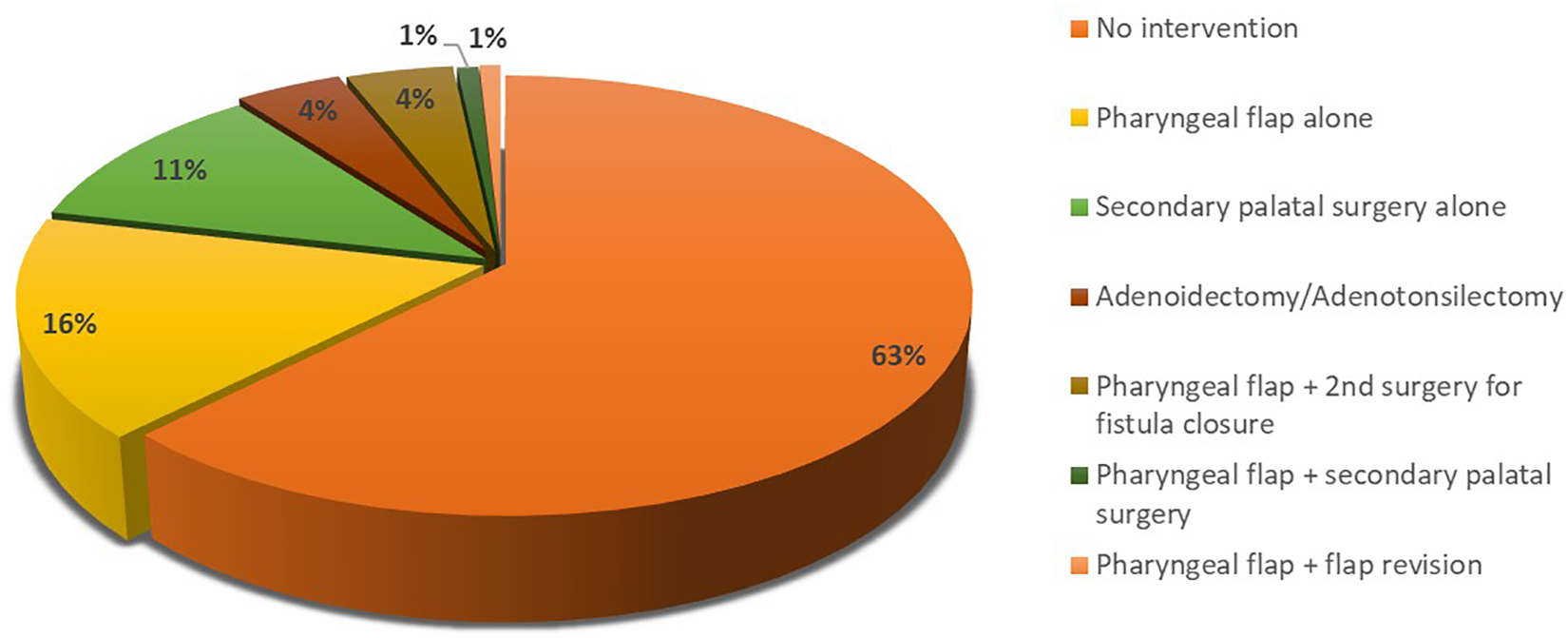
Additional surgical procedures employed for velopharyngeal or other otolaryngological indications.
Obstructive Sleep Apnea
About 18% of the included children were diagnosed with OSA, confirmed by polysomnography. Management was primarily with the use of CPAP or bilevel positive airway pressure.
Orthodontics
Orthodontic examination and treatment notes were available for 110 of the 117 patients aged 5 years and older. Analysis of data pertaining to the middle childhood and adolescent period showed that orthodontic treatment was conducted for most children for crowding, tooth agenesis of one or more permanent teeth, and to correct the skeletal and/ or dental dysplasia. Agenesis of one or more permanent teeth was frequently diagnosed, as well as severe crowding. Interceptive guidance of occlusal development was often performed through serial extractions of teeth. Treatment of Class II malocclusions and convex profiles was frequently noted. There were 51 patients with orthodontic notes available from the age of 15 years and older. Analysis of the orthodontic notes for these 51 children aged 15 years and older revealed the presence of Angle’s Class I malocclusion in 34%, Angle’s Class II malocclusion in 50%, and Angle’s Class III in 16% of the children. This age-group allowed examining the type of orthognathic surgery if it was conducted or was planned for the patients. The analysis revealed that only 4 (7.8%) of these 51 patients received orthognathic surgery involving osteotomies, which included mandibular advancement along with maxillary surgery (N = 2; 3.9%) and maxillary advancement with mandibular setback (N=2; 3.9%) for correcting a Class II and Class III malocclusion, respectively. A genioplasty with Medpor implant alone had been provided to augment the chin without mandibular surgery for 2 (3.9%) patients. There were 2 (3.9%) patients with Angle’s Class II malocclusion for whom surgery was considered as a possibility but not yet conducted and 1 (2.0%) patient was deemed to be indicated for a maxillary and mandibular surgery for Class III malocclusion, but it had not been conducted.
Discussion
A retrospective chart review of 117 children with nonsyndromic RS was conducted at one large institution, with acquisition of data regarding airway management, nutritional management, audiological interventions, orthodontic treatment, and additional surgical interventions needed. The Hospital for Sick Children, Toronto is a tertiary-care, referral, teaching hospital and has one of the world’s largest craniofacial centers. The present study is the first, to the best of our knowledge, to explore multidisciplinary interventions for nonsyndromic RS care longitudinally from infancy until growth completion. Longitudinal data of almost 87% of the children was available for the interventions we studied, including airway, nutritional, audiological, and surgical palatal management, thereby allowing a good longitudinal assessment of the interventions received by these patients. In addition, orthodontic examination and treatment notes were available for 51 children aged 15 years and older (mean age 17.8 ± 2.8 years, range 15-29.2 years), which provided an opportunity to examine their long-term orthodontic and orthognathic surgery outcomes. Data from previous studies have shed light on interventions for a specific management or issue but no comprehensive longitudinal multidisciplinary data as described in this study are available. It must be clarified that establishing specific treatment outcomes in various situations under different treatment modalities, although interesting, was beyond the scope of the current study.
When considering neonatal airway management, nonsurgical management of respiratory compromise was used in the majority (92%) of the patients. This percentage is somewhat higher than in other studies looking at airway management, which report frequencies between 45% and 75% (Caouette-Laberge et al., 1994; Van den Elzen et al., 2001; Li et al., 2002; Kirschner et al., 2003; Schaefer et al., 2004; Evans et al., 2006; Glynn et al., 2011; Izumi et al., 2012; Rathé et al., 2015; Table 1). On the contrary, tracheostomy was performed to a lesser extent (2%) than most other studies (2%-22%; Van den Elzen et al., 2001; Li et al., 2002; Evans et al., 2006; Glynn et al., 2011; Izumi et al., 2012; Filip et al., 2015; Paes et al., 2015; Rathé et al., 2015) and similarly the use of a nasopharyngeal airway (6% compared to 3%-23% in other studies; Evans et al., 2006; Glynn et al., 2011; Izumi et al., 2012; Filip et al., 2015; Rathé et al., 2015), mandibular distraction osteogenesis (1% compared to 3%-24% in other studies; Izumi et al., 2012; Paes et al., 2015; Rathé et al., 2015), or tongue lip adhesion (0% compared with 6%-27% in other studies; Li et al., 2002; Evans et al., 2006; Izumi et al., 2012; Paes et al., 2015; Table 1). When looking at neonatal airway management, differences between the present study and others may be due largely to the preferences of each individual center and represent perhaps a more conservative approach to management of the airway distress in early infancy followed at the hospital and craniofacial center where this study was based. How to choose the best intervention for an individual infant with RS, however, remains an unanswered question (MacLean, 2019) and depends upon a thorough clinical analysis of the nature and severity of respiratory distress in the neonatal and infancy period.
Comparative Data From Multiple International Centers Regarding Management of the Neonatal Airway Distress.a

Abbreviations: MDO, mandibular distraction osteogenesis; NPA, nasopharyngeal airway; TLA, tongue-lip adhesion.
a Values shown are percentages of the use of each specific procedure in the total RS population studied.
It is important to keep in perspective that Canada’s health care system is a publicly funded model of health care delivery with an interlocking set of 10 provincial and 3 territorial health systems and health care insurance plans. This “medicare” model provides access to a broad range of health services (Government of Canada, 2019). Under this system, all Canadian residents have reasonable access to medically necessary hospital and physician services without paying out-of-pocket. This may have contributed to the greater availability and access to longer periods of hospital stay and nursing support in early infancy that allowed conservative and nonsurgical approaches to be applied more frequently in the airway management during infancy.
Feeding difficulties during infancy and early childhood were managed nonsurgically (53%) with the use of Haberman feeders or occasionally Mead Johnson feeders. The placement of an NG-tube was carried out in 16% of children in this study, which was below the 41% to 77% range found in other studies (Van den Elzen et al., 2001; Li et al., 2002; Glynn et al., 2011; Paes et al., 2015), while the placement of a G-tube was carried out in 26% of 105 patients analyzed during infancy, early, and middle childhood which was within the range also seen in other studies (3%-43%; Van den Elzen et al., 2001; Kirschner et al., 2003; Evans et al., 2006; Table 2). The prevalence of GERD in infants and younger children noted in the present study (6%) was much lower than the 35% (Evans et al., 2006) to 83% (Monasterio et al., 2004) reported in previous studies.
Comparative Data From Multiple International Centers Regarding Nutritional Management of Neonatal Feeding Difficulties.a,b
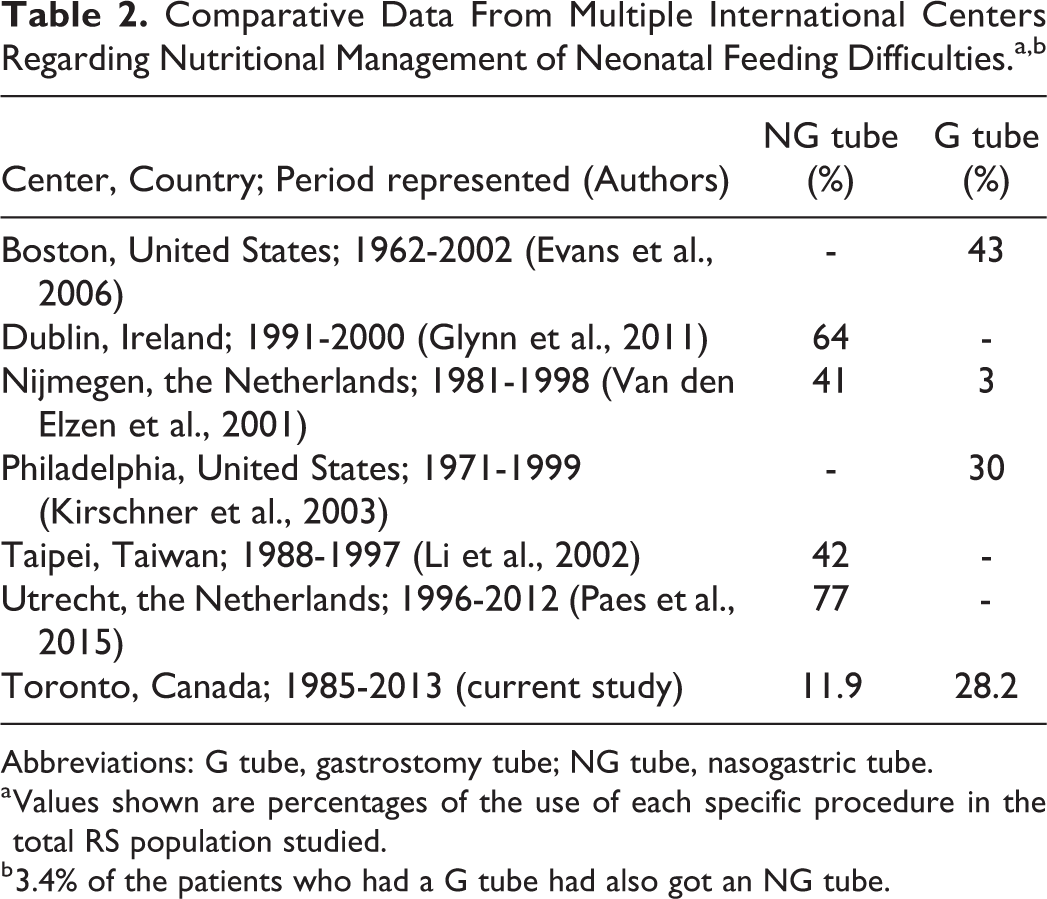
Abbreviations: G tube, gastrostomy tube; NG tube, nasogastric tube.
a Values shown are percentages of the use of each specific procedure in the total RS population studied.
b 3.4% of the patients who had a G tube had also got an NG tube.
The placement of tympanostomy tubes was required in 72 (62%) of the 117 children and infants with RS whose data were included for this part of the analysis in the present study. This is within the range from 35% (Glynn et al., 2011) to 64% (Li et al., 2002) reported in previous studies.
Analysis of longitudinal chart records of patients followed during the early, middle childhood periods, and early adolescent years revealed that the most common additional surgical intervention necessary was a pharyngeal flap for problems related to VPI, which was required in 22% of children with RS in this study. This figure is similar to 22% (Van den Elzen et al., 2001) and lower than 33% reported in other studies (Filip et al., 2015).
Orthodontic treatment was performed in most of the children in our study based on the longitudinal records of children whose data were available. This was due in part to the availability of orthodontic services within the same institution and, in part, to the availability of reimbursement benefits these children were entitled to through the Cleft Lip and Palate/Craniofacial Dental Program of the Ontario Ministry of Health and Long-Term Care. The province of Ontario in Canada has established The Ontario Cleft Lip and Palate/ Craniofacial Dental Program to financially assist and cover the expenses of the families of affected individuals for their specialized dental needs. The provincial Ministry of Health and Long-Term Care, through this program, covers up to 75% of the preapproved dental specialist treatment costs (eg, orthodontic treatment, dental implants, prosthetic treatment, and oral surgery) that cannot be covered by private dental insurance. This gives the opportunity for a larger number of affected individuals to receive specialist orthodontic and dental services, which allowed a bigger pool of data for the longitudinal analysis of the orthodontic problems and treatment plans.
Some of the characteristics of individuals with RS which require orthodontic treatment include mandibular retrognathia, bimaxillary retrognathia, tendency for a hyperdivergent facial pattern, maxillary constriction secondary to clefting, Class II malocclusion accompanied by severe crowding, and tooth agenesis (Hermann et al., 2003; Suri et al. 2006, 2010; Antonarakis & Suri, 2014; Andersson et al., 2015; Antonarakis et al., 2017; de Smalen et al., 2017; Cohen et al., 2017; Do et al., 2019). In the present study, the agenesis of one or more permanent teeth and severe crowding were common findings. Orthodontic treatment including serial extractions of teeth was used in most of the cases.
A small number of the children had undergone orthognathic surgery upon achieving skeletal maturity. Interestingly, little data are available in the literature describing the modalities of orthodontic treatment needed in children with RS as the focus is usually on the airway and feeding management during their first or early years of life and further multidisciplinary longitudinal management of the included children is mostly not described. The limited number of published case studies regarding the type of orthodontic treatment needed in RS includes serial extractions of teeth and mandibular incisor proclination to obtain a functional occlusion (Matsuda et al., 2006; Eliyahu et al., 2018). In both of those case studies, although not performed, orthognathic surgery by means of bilateral sagittal split osteotomy or genioplasty was suggested as the optimal treatment method to improve facial esthetics. In the current study, we noted that orthognathic surgery after reaching skeletal maturity was conducted in or deemed appropriate for 17.6% of the children whose orthodontic examination and treatment notes were available for 51 children aged 15 years and older. This relatively low number could be explained by the bimaxillary retrognathia seen in RS (Suri et al., 2010; Do et al., 2019). In this age-group, although 50% children in the current study had Angle’s Class II malocclusion and 34% children had Angle’s Class I malocclusion, it is noteworthy that 16% children had Angle’s Class III malocclusion. This could be explained by maxillary retrusion related to cleft palate, and therefore maxillary advancement was required in half of the children who received orthognathic surgery involving osteotomies. This calls attention to the fact that clinicians may expect to encounter and treat not only Class II and Class I malocclusions but also Class III malocclusion in RS. A cleft palate program in Los Angeles has reported an orthognathic surgery percentage of 39% in skeletally mature patients with RS, with the vast majority requiring mandibular advancement to correct a class II malocclusion (Pfaff et al., 2020). In their sample, however, 66% of the included patients had syndromic RS. The frequency of orthognathic surgery as reported in our analysis, however, does not allow us to comment on any potential mandibular “catch-up growth” in this cohort, as this study did not include a longitudinal cephalometric analysis of the patients to document and analyze growth increments.
Strengths of the present study include its relatively large sample size of a relatively rare entity, especially when compared with sample sizes in most other published studies in the field (Van den Elzen et al., 2001; Li et al., 2002; Kirschner et al., 2003; Wagener et al., 2003; Schaefer et al., 2004; Evans et al., 2006; Glynn et al., 2011; Izumi et al., 2012; Filip et al., 2015; Paes et al., 2015; Rathé et al., 2015), and the collection of longitudinal data through infancy, childhood, and adolescence, using a multidisciplinary approach with a broader perspective including interventions from several different specialties. Furthermore, the treatment setting was centralized which allowed for more accurate and less heterogeneous data collection. Although retrospective, the collection of data was consecutive, with minimal patient exclusion and minimal loss of information unless limited by the age of the children.
Limitations of this study include its retrospective nature. Due to the nature of such an investigation however, previous reviews of this kind (Filip et al., 2015) as well as the international studies, which reported on the interventions included in our comparative summaries (Caouette-Laberge et al., 1994; Van den Elzen et al., 2001; Li et al., 2002; Kirschner et al., 2003; Schaefer et al., 2004; Evans et al., 2006; Glynn et al., 2011; Izumi et al., 2012; Paes et al., 2015; Rathé et al., 2015), were also retrospective studies. Retrospective studies allow for the inclusion of a large sample, while reducing the significant ethical and financial constraints of a prospective study. Furthermore, for a study of this nature, the retrospective design allowed analysis of the prevailing protocol or care and multidisciplinary treatment rendered over a long period of time for a relatively large number of individuals affected by a relatively rare condition. While recall bias may be an issue, it was considered to be minimal in the present study as data retrieved were for the most part complete unless limited by the age of the children.
Selection-related bias was avoided as best as possible by including all patients who fulfilled the inclusion criteria. Only patients having a diagnosis of nonsyndromic RS with cleft palate were included. Recently, there has been consensus among multidisciplinary experts, in which cleft palate has not been included as a mandatory diagnostic criteria in the definition of RS (Breugem et al., 2016). During the operational period of data collected for this study, the hospital’s diagnosis of RS included the triad of mandibular micrognathia at birth, severe neonatal respiratory distress, and cleft palate. Including patients having a diagnosis of RS with cleft palate allowed us to investigate a homogeneous sample. There was no control group, although its value and significance in such a study is questionable. Data were not collected on surgical techniques used in primary palate repair as all children had cleft palate and had palatoplasties. While this analysis reflects multidisciplinary aspects of the treatment protocol of a large craniofacial center, it was beyond the scope of the current investigation to provide details of nuances of interventions or to include an analysis of the outcomes of effectiveness of the specific interventions that were documented. Finally, this study was based on treatment details available in the institutional records, and therefore it does not provide an analysis of the burdens of these treatment interventions on the families and individuals. The aim of the study was not to examine the individual and financial burdens and therefore those data were not within the scope of the investigation.
It should be clarified that although data were available for 117 patients during their infancy period, and for almost 87% of the sample at other times, while long-term orthodontic notes were available for 51 patients aged 15 years and older; this, however, was not equivalent of having a biased sample. It was to be expected considering (1) the limits of eligibility for inclusion (born between 1985 and 2012) and (2) the fact that some specific interventions are required at specific ages. For example, airway considerations are critical in the management of RS in early infancy and become less so as the infant thrives and grows into later infancy and early childhood periods. Therefore, analysis of interventions for airway management would be most valuable in the infancy period. On the other hand, orthodontic assessments and treatments are normally undertaken in the middle and later childhood years and adolescent years and therefore analysis of patients at that age would be important.
The results of the present study and comparative data about multidisciplinary interventions reported from other international centers are of significant clinical importance, as they may help in the development of cleft and craniofacial team treatment strategies for children born with RS, contributing to their optimal health care and long-term outcomes. Comparison with available data from other studies allows understanding the frequencies of usage of different approaches in the management of specific problems at different ages of affected children. Recent efforts have aimed toward creating treatment algorithms for children born with RS (Gómez et al., 2018; Hicks et al., 2018; Resnick et al., 2019), and data presented in the current study may be useful in developing international consensus treatment algorithms. The data may also help in planning the allocation of federally, provincially, or publicly funded, institutional and/or individual resources for children born with RS. Finally, these results may help in designing burden of care and quality-of-life studies for this patient population and their families, as the overall burdens of treatment interventions and care may show an association with such indices.
Conclusions
Institutional treatment of children with nonsyndromic RS involves multidisciplinary care at different ages and stages of their development. The types, frequencies, and extents of these interventions vary among international centers. With the treatment approach followed at the tertiary-care hospital in which this study was based, surgical intervention for airway compromise in the neonatal period and early infancy was used in only 7% of infants with nonsyndromic RS, and 92% were managed with prone positioning. Approximately 26% of the patients included in this study required feeding G-tube placement and approximately 62% required tympanostomy tube placement. In addition to the repair of the cleft palate, 22% patients required pharyngeal flap surgery and 11% received secondary palatal surgery. Obstructive sleep apnea was diagnosed and managed in 18%. Orthodontic and dentofacial orthopedic treatment was recommended and performed for most patients for malocclusions related to tooth agenesis, severe crowding, and relative mandibular retrognathia. Orthognathic surgery at the completion of facial growth was used or deemed appropriate in almost 18%.
Footnotes
Authors’ Note
This study was presented in part at the 2nd International Robin Sequence Consensus Meeting; Toronto; May, 2017.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by an American Association of Orthodontists Foundation Biomedical Research Award to Sunjay Suri.