
Abstract
Background:
The main goal of presurgical orthopedics (PSO) for patients with bilateral cleft lip and palate is to correct the protruded and/or twisted premaxilla. However, PSO is associated with the risk of uncontrolled development of the vomer, which has received little attention to date.
Solution:
We present a removable orthodontic device that can be used to keep or align the vomer and the premaxilla in the midline during preoperative molding of cleft segments independently and 3 dimensionally.
Keywords
Introduction
The management of a severely protruded, and/or twisted premaxilla, and a deviated vomer has always been a challenge for cleft surgeons. Postoperative uncontrollable tension on the cleft segments affects surgical outcomes, further growth, and even speech through nasal airway obstruction (NAO). Therefore, several techniques have been developed to align the premaxilla before lip and palate closure (Vyas et al., 2016). Among these, presurgical orthopedics (PSO) seems to be the gentlest method; clinically, it applies controlled forces, but mainly focuses on the premaxilla and lateral cleft segments, without considering the vomer (Hotz, 1969; Grayson et al., 1999). An exception is the Latham appliance, which was intensively discussed (Berkowitz, 1996), and has never been accepted worldwide.
In our experience, a vomer in the optimal position preoperatively, even without the premaxilla perfectly aligned between the lateral segments, makes the surgical procedure easier and shorter and produces better functional and aesthetic results.
With these considerations, we developed a removable customized premaxilla vomer plate (PMVP) based on 3D model operations to control the position of the vomer during preoperative molding of the cleft segments.
Methods
Initially, we take an impression with an individualized tray with C-silicones (Xantopren, Kulzer GmbH) to capture the cleft segments and the vomer, as cranial as possible, up to the septum. We prefer C-silicones because of their controllable viscosity, accuracy, elasticity, and dimensional stability. We decided for conventional impressions instead of intraoral scanner, because the undercuts of the vomer cannot be detected (Figure 1A).
Silicone impression.
The impression is digitized, and a computer 3D model is then created. A biometric analysis with computer-aided design simulates movement of the cleft segments from the initial to the final position for surgery. The computer divides the overall movement of the segments into single steps, each step can be up to 1 mm in all 3 dimensions (Autodesk). Up to 10 model operations may be necessary according to the severity of the cleft. Based on 3D models, each PMVP is manufactured with Dental LT Clear resin (V2) in 50-µm coating thickness, by a 3D printer (both from Formlabs, Formlabs GmbH). After 4 weeks, we take another impression to judge the growth and the position achieved for further planning (Figure 2A-F).
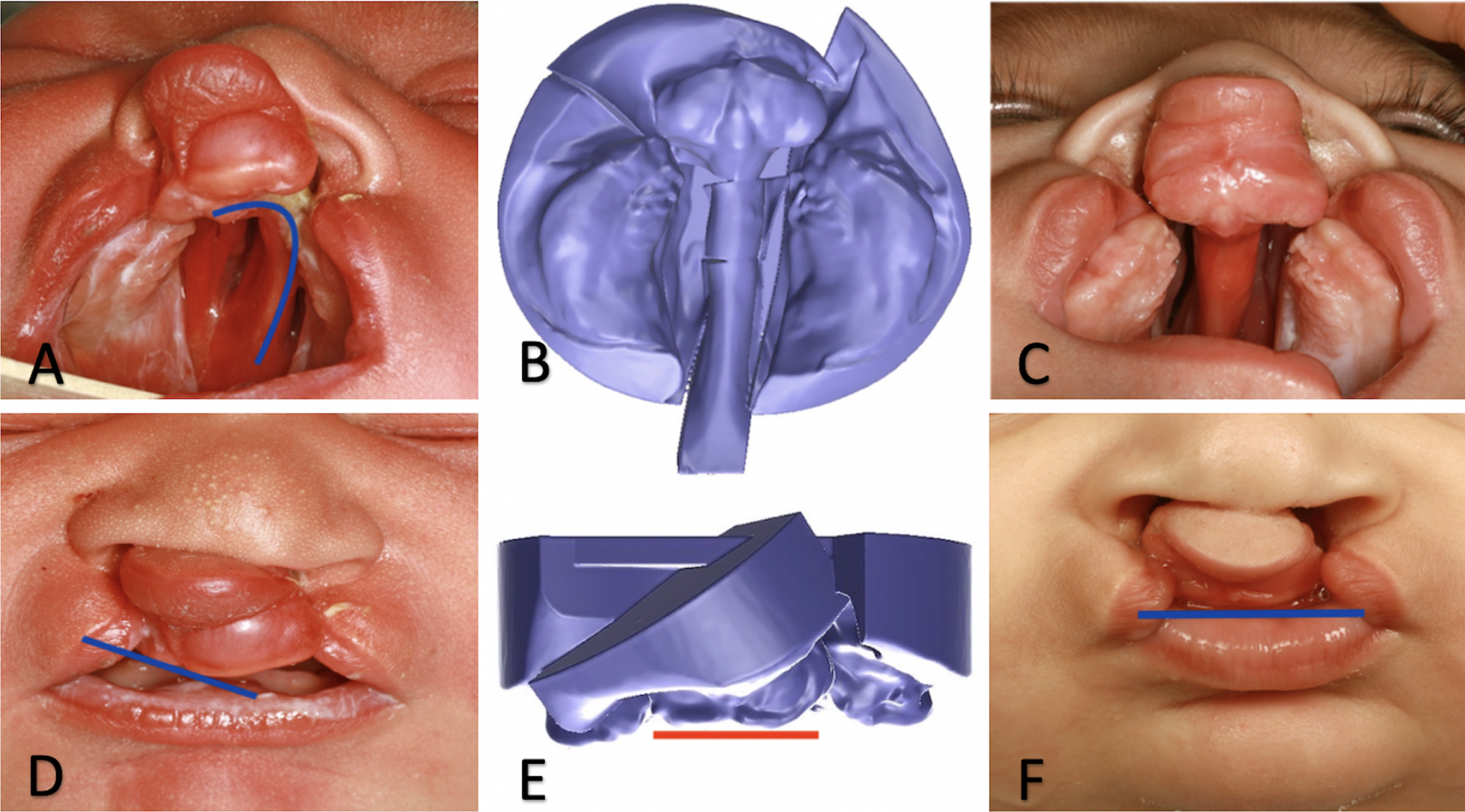
(A) Postnatal condition; (B) last model operation 10/10; (C) after 10 weeks; (D) postnatal condition; (E) last computer-aided design (CAD) model operation 10/10 in the front; (F) after 10 weeks.
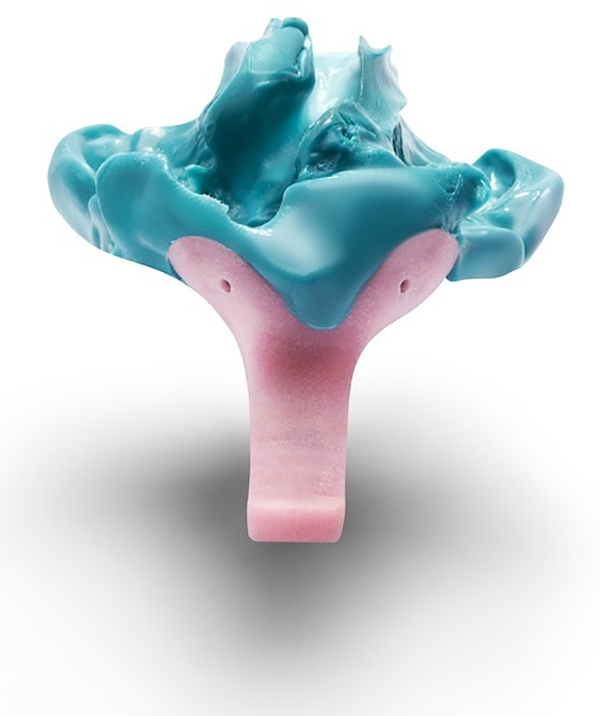
The key features of the PMVP are the 2 bars enclosing and shaping the vomer, and moving the cleft segments independently in different directions. The mechanism underlying the plate is based on the principle of the inclined plane, where the dorsal part of the maxilla and the bars are the active elements of the inclined plane. The first as well as each new PMVP has a gap of about 1 mm in the region of the tuber. The natural pressure of the tongue on the dorsal parts of the PMVP moves the plate to its final position within one week cranially/posteriorly. During this time, the inclined plane moves the cleft segments and shapes the vomer according to the model operation. The bars guide the movement and support the holding of PMVP in situ (Figure 3A and B).
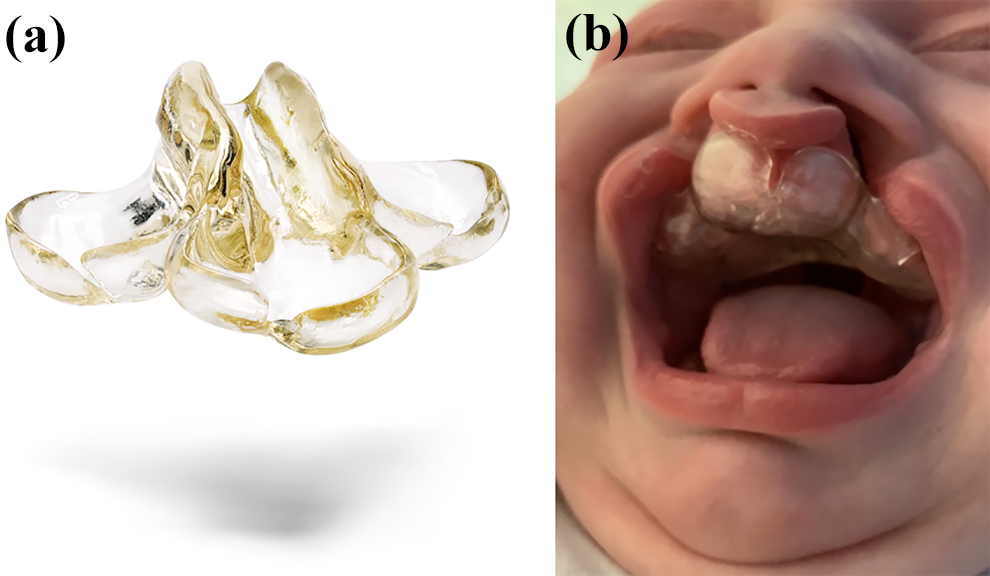
A, Premaxilla vomer plate. B, Inserted premaxilla vomer plate.
Discussion
The PMVP is recommended for the horizontal and vertical alignment of the premaxilla, without application of extra oral forces, as well as independent capturing and guiding of the vomer.
Cleft therapists are divided in their opinions for and against PSO. Although active appliances and extraoral forces are considered responsible for growth impairment, extensive tissue mobilization during closure of severe clefts bears the same risk. Considering both these aspects, we have developed a device, working with natural tongue pressure and reasonable positioning of the premaxilla, to provide an operable basis. That means a symmetrical constellation of all cleft segments to provide an operable basis for tension free closure and the possibility to bridge the gaps with like tissue.
Contrary to conventional PSO, the serial production of PMVP, with each modification prefabricated in the laboratory, does not require the presence of the patient for adjustment. This can spare clinical time and cost.
Conclusion
Symmetrical nasal floors, a prerequisite to prevent NAO, and fistula free closure of the hard palate with sophisticated lip and nose à la Millard, Mulliken, or Bitter are most likely possible when the vomer and cleft segments are in a tolerable position. Premaxilla vomer plate use does not aim for perfect alignment of the premaxilla, which is considered controversial (Spolyar, 2020); it is about creating better conditions for primary surgery with the support of orthodontists and medical engineers.
Footnotes
Authors’ Note
G.S. and C.M. contributed to conceptualization; C.M. contributed to use software; G.S. and C.M. contributed to writing—original draft preparation; M.H. contributed to writing—review and editing; C.M. contributed to visualization; G.S. and C.M. contributed to supervision; G.S. and C.M. contributed to project administration. All authors have read and agreed to the published version of the manuscript. Ethics approval and consent to participate our report is on a clinical innovation, that is, this was not a study, but an attempt to improve patient care, for which neither Ethical Approval nor written informed parental consent is needed; neither was thus obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.