
Abstract
Objective:
To determine if there is a correlation between objective nasolabial aesthetics assessment using the Cleft Aesthetic Rating Scale (CARS) and patient satisfaction.
Design:
Retrospective analysis of a generic satisfaction questionnaire and independent assessment by three cleft surgeons of the nasolabial area of these patients on 2D frontal photographs, using the CARS.
Setting:
The Vrije Universiteit Medical Center and The Academic Center for Dentistry Amsterdam.
Patients:
Thirty-nine 18-year old patients with a repaired complete or incomplete unilateral cleft lip, with or without a cleft palate, and a completed satisfaction questionnaire. Exclusion criteria were an incomplete questionnaire; a history of facial trauma; and congenital syndromes affecting facial appearance.
Main Outcome Measures:
The correlation between surgeon evaluation (on a 5-point Likert scale) and patient satisfaction (not, moderately or very satisfied) on nasolabial appearance was assessed using Spearman rho (ρ).
Results:
There was a negligible correlation between surgeon evaluation and patient satisfaction on nose assessment (ρ = 0.20) and a moderate correlation on lip assessment (ρ = 0.32).
Conclusions:
Most literature supports this discrepancy between different objective aesthetics evaluation methods and subjective patient-reported outcome measures, suggesting there are factors playing a role in patient satisfaction that are impossible to objectify with assessment methods. Therefore, a strong emphasis should remain on clear communication between the physician and patient regarding their expectations, perception, and satisfaction of surgery results.
Introduction
In the past 2 decades, the focus on the patients’ perspective of received health care using questionnaires, collectively referred to as patient-reported outcome measures (PROMs), has increased in importance to improve health-related quality of life (Wu et al., 2010; Jayadevappa and Chhatre, 2011). As PROMs evaluate outcomes that have direct relevance to the day-to-day functioning of the patient like perceived aesthetic results, speech, functionality, self-image, incorporation into society, and quality of life, they can be more meaningful than clinical measures alone (Wu et al., 2010; Eckstein et al., 2011). Assessment of the appearance is an essential component of the quality of life outcome and several PROMs for aesthetic evaluation have been developed (Al-Omari et al., 2005). However, a wide variety exists between PROMs and, until the recent development of the CLEFT-Q, none have been specifically validated for patients with cleft (Eckstein et al., 2011; Ranganathan et al., 2015; Tsangaris et al., 2017a; Wong Riff et al., 2017). Moreover, critics express 3 major concerns about patient-reported satisfaction: it actually captures some aspect of the patient’s current happiness, it could be confounded by satisfaction with the care process not directly associated with the facial appearance, and it may reflect the realization of the patient’s a priori desires (Manary et al., 2013). Nevertheless, inventorying patient experiences offers distinctive indicators of health-care quality and helps to improve treatment strategies (Wu et al., 2010; Manary et al., 2013).
Traditionally, the focus of outcomes research for cleft surgery has been on objective instruments such as anatomic measures, clinical photographs, morbidity, and mortality (Eckstein et al., 2011). For surgeons performing cleft lip repairs, achieving perfect symmetry of the nose and lip has always been one of the most important aims. Despite numerous assessment techniques to evaluate facial symmetry and nasolabial aesthetics on 2-dimensional (2D) photographs, 3-dimensional images, videographic assessment, and direct clinical assessment, no internationally accepted standardized rating method for the aesthetic evaluation of patients with cleft after cleft repair is recognized (Al-Omari et al., 2005; Sharma et al., 2012; Mosmuller et al., 2013). Besides, there appears to be a discrepancy between professional assessment of nasolabial aesthetics and patient satisfaction with their appearance (Mani et al., 2010; Keijser et al., 2016; Nadjmi et al., 2016; Pausch et al., 2016). It should be realized that professional assessment and patient satisfaction are 2 different modalities and they probably should be interpreted like this. Nevertheless, much is still to learn from comparing these assessments and from analysing patient questionnaires. Moreover, better understanding of the patient perspective is a key element in improving cleft care.
Recently, an easy to learn, quick, and reliable assessment method for rating nasolabial aesthetics on 2D-photographs has been developed: the Cleft Aesthetic Rating Scale (CARS) (Mulder et al., 2018). The CARS evaluates the nose and lip on a 5-point Likert scale by means of rules and a photographic reference scale. The primary objective of this study was to determine the correlation between the assessment of nasolabial appearance by cleft surgeons using the CARS and the patient satisfaction with their nasolabial appearance in patients with a repaired unilateral cleft lip. Further, correlations between questions in the patient questionnaire about nasolabial aesthetics, functionality, social problems, and a wish for surgical correction of the nasolabial area were examined. Our null hypothesis was that there was no difference in subjective and objective assessment of nasolabial appearance.
Methods
Participants
Generic satisfaction questionnaires completed by 41 patients with a repaired cleft lip and palate, aged 18 years during their last consultation at the VU Medical Center between October 2010 and June 2014 were retrospectively retrieved. Photographs that were taken on the day of consultation were selected from the database of the Academic Center for Dentistry Amsterdam. Inclusion criteria were 18-year-old patients; a complete or incomplete unilateral cleft lip, with or without a cleft palate (CL±P); and an available photograph of the frontal view with the face in neutral position, showing the nasolabial area according to our institutions standardized protocol. Exclusion criteria were an incomplete questionnaire; a history of facial trauma; and congenital syndromes affecting facial appearance.
The Medical Ethics Review Committee of VU Medical Center (2017.614) has confirmed that the use of anonymous patient data collected during routine patient care is in accordance with the Dutch law on medical research. The principles outlined in the Declaration of Helsinki were followed.
Methods of Measurement
Patients completed the generic questionnaire at home, before their last visit at our cleft lip and palate team. This questionnaire has been used by our department for the past 16 years, and contains questions about achievements on an academic level, problems with speech, hearing, teeth, and jaws. For this study, we focussed on questions if they were satisfied with their nose, lip, and overall face appearance (not satisfied, moderately satisfied, or very satisfied), if they experienced problems in their social life, functional nose problems, or nasal regurgitation (often, sometimes, or never), and if they would prefer any nasolabial surgical corrections in the future (yes or no). An example of the (Dutch) questionnaire can be requested from the corresponding author.
For the objective assessment of the nose and the lip, using Photoshop (Adobe systems, Inc, San Jose, California), the photographs of patients with a right-sided cleft were mirrored so all images showed a left-sided cleft and the photographs were cropped only leaving the nasolabial area visible (Figure 1). Three cleft surgeons, not involved in the treatment of these patients, independently scored the photographs using the CARS. The photographs were presented in a Microsoft PowerPoint slideshow on a MacBook Pro with Retina display (Apple, Inc, Cupertino, California). According to CARS protocol, the surgeons received a printed version and an oral explanation of the assessment rules and photographic reference scale. Next, a test trial of 10 photographs not included in this study was scored and immediately discussed with the author managing the PowerPoint slide advancement (Frans J. Mulder ) to familiarize the surgeons with the scale. Finally, the photographs were scored, showing every photograph for a maximum of 30 seconds, followed by a blank slide for at least 5 seconds before moving on to the next photograph. The nose was scored on a 5-point Likert scale from A to E, representing an excellent to poor result, respectively. For the lip, the same was done on a 5-point Likert scale from 1 to 5, representing an excellent to poor result respectively.
Cropped photograph of the nasolabial area.
Descriptive data (sex, race, cleft side, type of cleft, and surgical procedures) were collected from the patients’ medical records. If an additional correction to the nose, scar, or lip was performed after the initial lip repair (for instance during the palate repair, pharyngoplasty, or alveolar closure) it was counted as a secondary correction, in addition to separately scheduled secondary corrections.
Statistical Analysis
Demographic and cleft related population characteristics were expressed as percentages. During statistical analysis, the CARS letter scores of the noses were transformed into numbers (A = 1, B = 2, C = 3, D = 4, and E = 5). To determine if there was a difference in CARS scores between the different categories of patient satisfaction (not satisfied, moderately satisfied, or very satisfied), the Kruskall Wallis test was used. Using Spearman rho (ρ), the correlation between the mean CARS score of the surgeons and patient satisfaction was assessed. According to Hinkle et al. (2003), a correlation coefficient of 0.00 to 0.29 is considered negligible, from 0.30 to 0.49 weak, from 0.50 to 0.69 moderate, from 0.70 to 0.89 strong, and above 0.90 is considered a very strong correlation.
Results
Of the 41 patients, 39 met the inclusion criteria. Patients were on average 18.1 years old (standard deviation [SD] 0.26). Rotation advancement lip closure according to Millard (1964) was performed 3 to 4 months after birth (mean 3.8 months, SD 1.8 months). Twenty-four (62%) of the 39 patients were male and 16 (41%) originally had a right-sided cleft. Thirty-two patients were Caucasian (82%), 5 North African (13%), 1 South American (2.6%), and 1 Asian (2.6%). A post hoc G*Power 3.1 power analysis showed that 39 patients provide a power of 0.47 to detect a weak correlation (ρ = 0.30, α = 0.05), using a 2-tailed exact test for a bivariate normal model (Faul et al., 2009).
A negligible correlation was found between CARS score and patient nose satisfaction (ρ = 0.20) and a weak correlation for the lip (ρ = 0.32). No significant difference in surgeon assessment between different satisfaction groups for nose satisfaction (P = .46) and lip satisfaction (P = .14) was found (Figures 2 and 3).
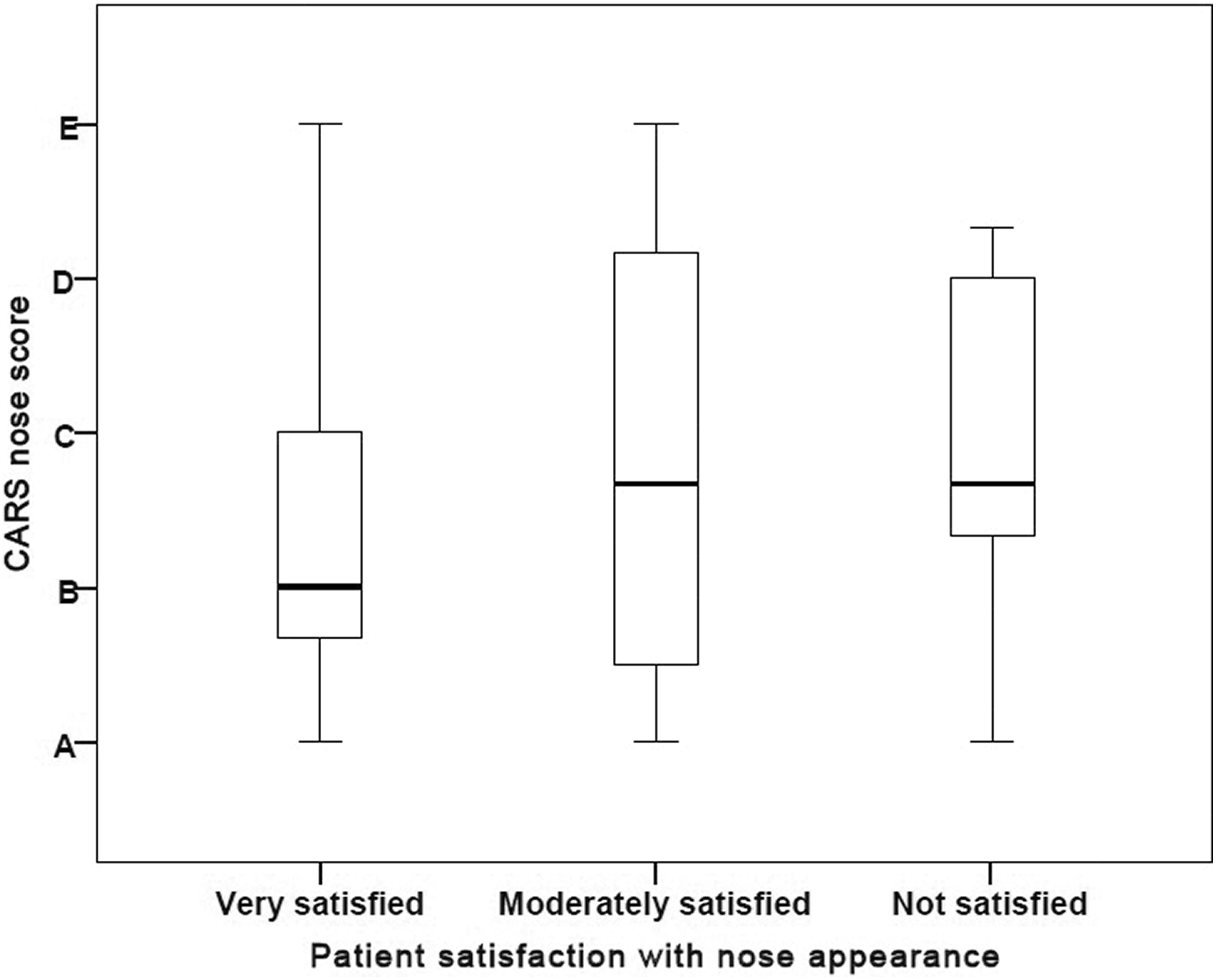
Patient satisfaction with nose appearance versus CARS score (A = excellent result, E = poor result), showing a negligible correlation (ρ = 0.20). CARS: Cleft Aesthetic Rating Scale.
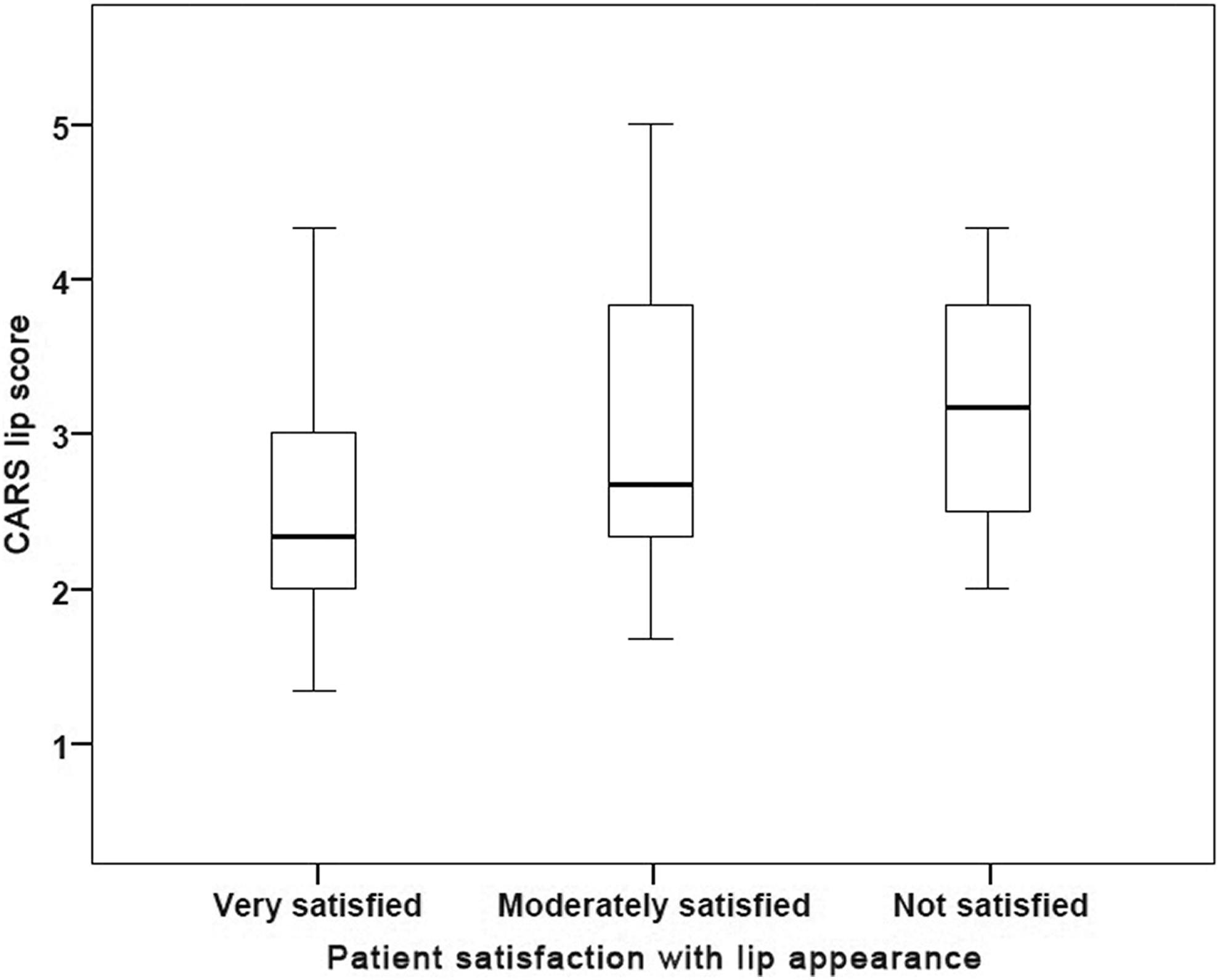
Patient satisfaction with lip appearance versus CARS score (1 = excellent result, 5 = poor result), showing a weak correlation (ρ = 0.32). CARS: Cleft Aesthetic Rating Scale.
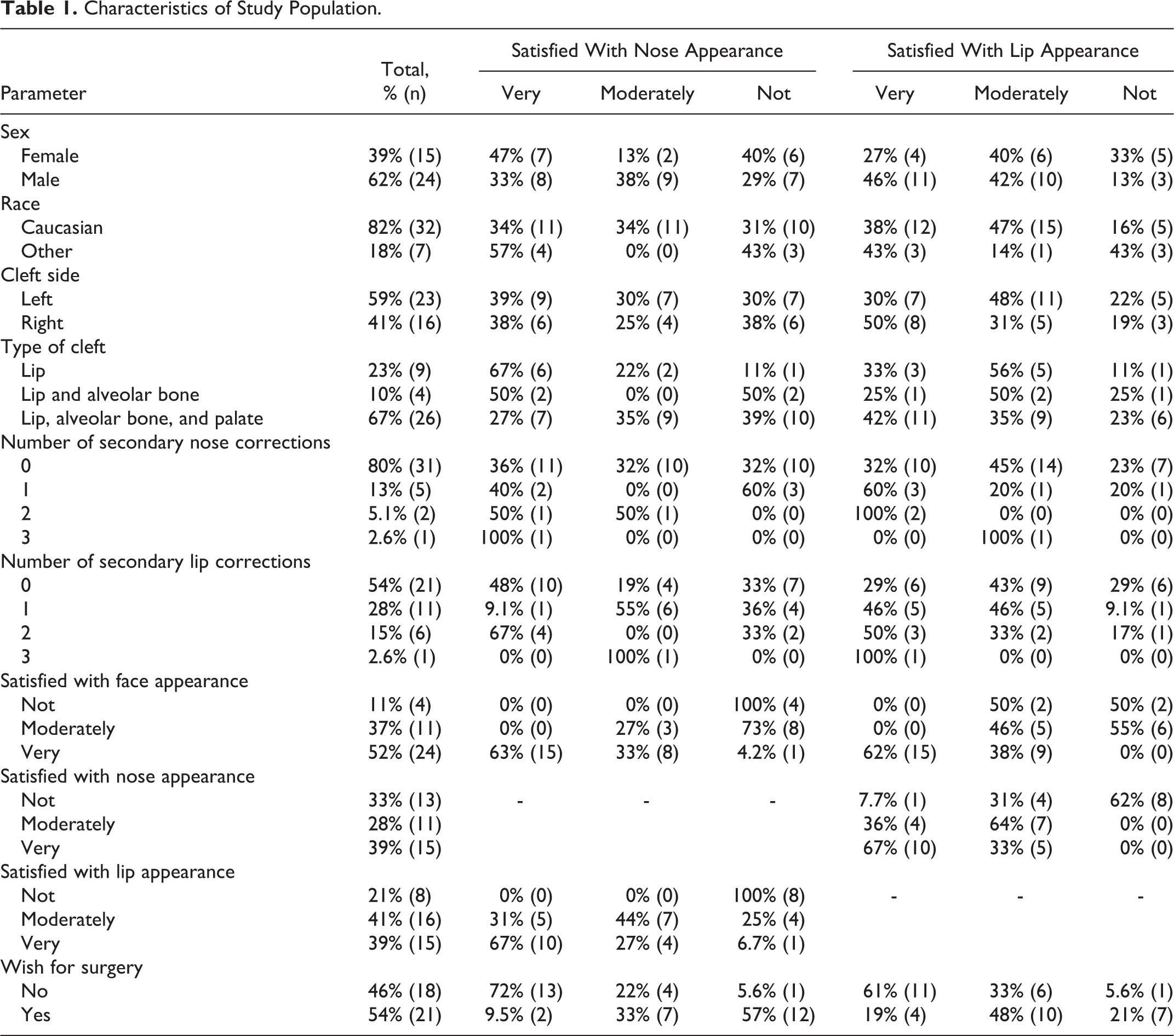
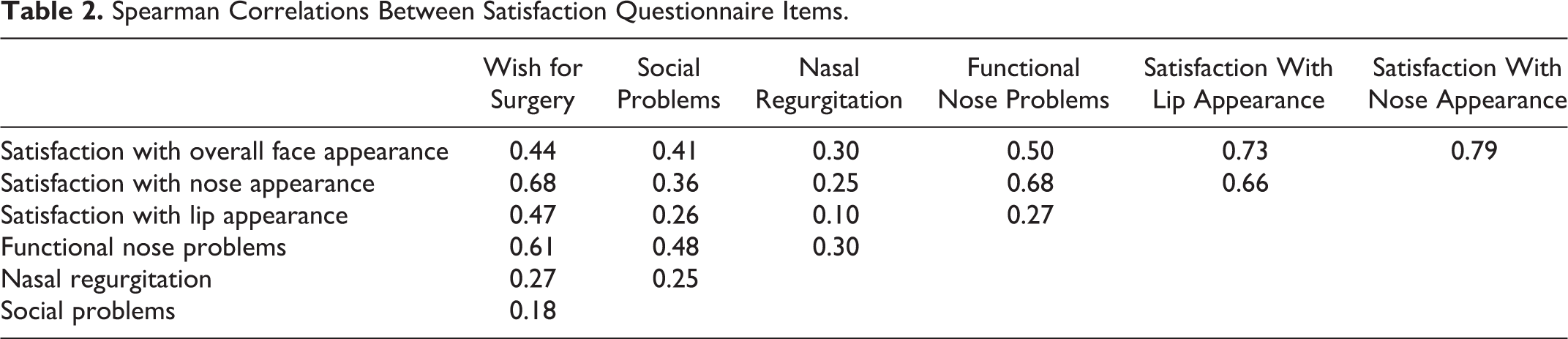
Patients who were very satisfied with their nose appearance were also very satisfied with their overall face appearance (strong correlation, ρ = 0.79) and lip appearance (moderate correlation, ρ = 0.66). Similarly, satisfaction with lip appearance was strongly correlated to overall face appearance (ρ = 0.73). All patients dissatisfied with their lip appearance were dissatisfied with the appearance of their nose as well (Table 1).
Characteristics of Study Population.
Experiencing social problems as a result of their cleft had a negligible to weak correlation to the aesthetic perception of their nasolabial area. The wish for a surgical correction of the nasolabial area was strongest correlated to the patients’ satisfaction with nose appearance (ρ = 0.68) and experiencing functional nasal problems (ρ = 0.61; Table 2). Of the 21 patients who preferred further surgical correction of the nose or lip, 81% were not satisfied or moderately satisfied with its appearance.
Spearman Correlations Between Satisfaction Questionnaire Items.
Discussion
This study showed a negligible correlation between patient satisfaction and nose assessment and a weak correlation with lip assessment of cleft surgeons using the CARS. There was a strong correlation between satisfaction with nose appearance and satisfaction with lip appearance and most patients who were not or moderately satisfied with their nasolabial appearance preferred surgical correction in the future.
The largest limitation of this study was that the patient group was too small for additional analysis, for example, to evaluate predictors for patient satisfaction (power of 0.47 to detect a weak correlation). Unfortunately, small numbers are generally a problem with CL±P research. Secondly, a fairly new rating system was used for objective aesthetics assessment: the CARS. Then again, for the aesthetic evaluation of cleft patients after cleft repair, no standardized rating method is internationally recognized (Al-Omari et al., 2005; Sharma et al., 2012; Mosmuller et al., 2013). Moreover, the CARS seems robust when the average judgement of 3 cleft surgeons is taken, as was shown in a previous study with a reliability of 0.77 for the lip assessment and a reliability of 0.85 for the nose assessment (Mulder et al., 2018).
Our results are in concordance with Keijser et al. (2016), who reported a negligible correlation (ρ < 0.20 for all variables) between nasal appearance evaluation by a professional panel using the Asher-McDade aesthetic index (AMAI) and self-assessment of nasal appearance by patients (mean age 32 years) using the Satisfaction With Appearance scale (SWA; Asher-McDade et al., 1991; Alsarraf et al., 2001). The AMAI evaluates 4 parameters of the nose and lip on a 5-point Likert scale of which a mean score is calculated. A recent systematic review about PROMs among CL±P children showed that aesthetic considerations are most commonly analysed using the SWA, reflecting satisfaction with cleft-related and noncleft-related aspects of speech, face, and overall appearance, and extra oral visibility of the cleft on a visual analogue scale from 1 to 10 (Ranganathan et al., 2015). Mani et al. (2010), however, found a weak-to-moderate correlation (ρ = 0.48-0.53 for all parameters) between these assessment methods in a similar patient group, suggesting that other factors than the nasolabial appearance itself contribute to the self-assessment of patients with cleft, emphasizing the importance of clear communication between health-care professionals and patients to optimize satisfaction with treatment (Table 3).
Nasolabial Assessment Tools for Patients With a Repaired Cleft Lip.
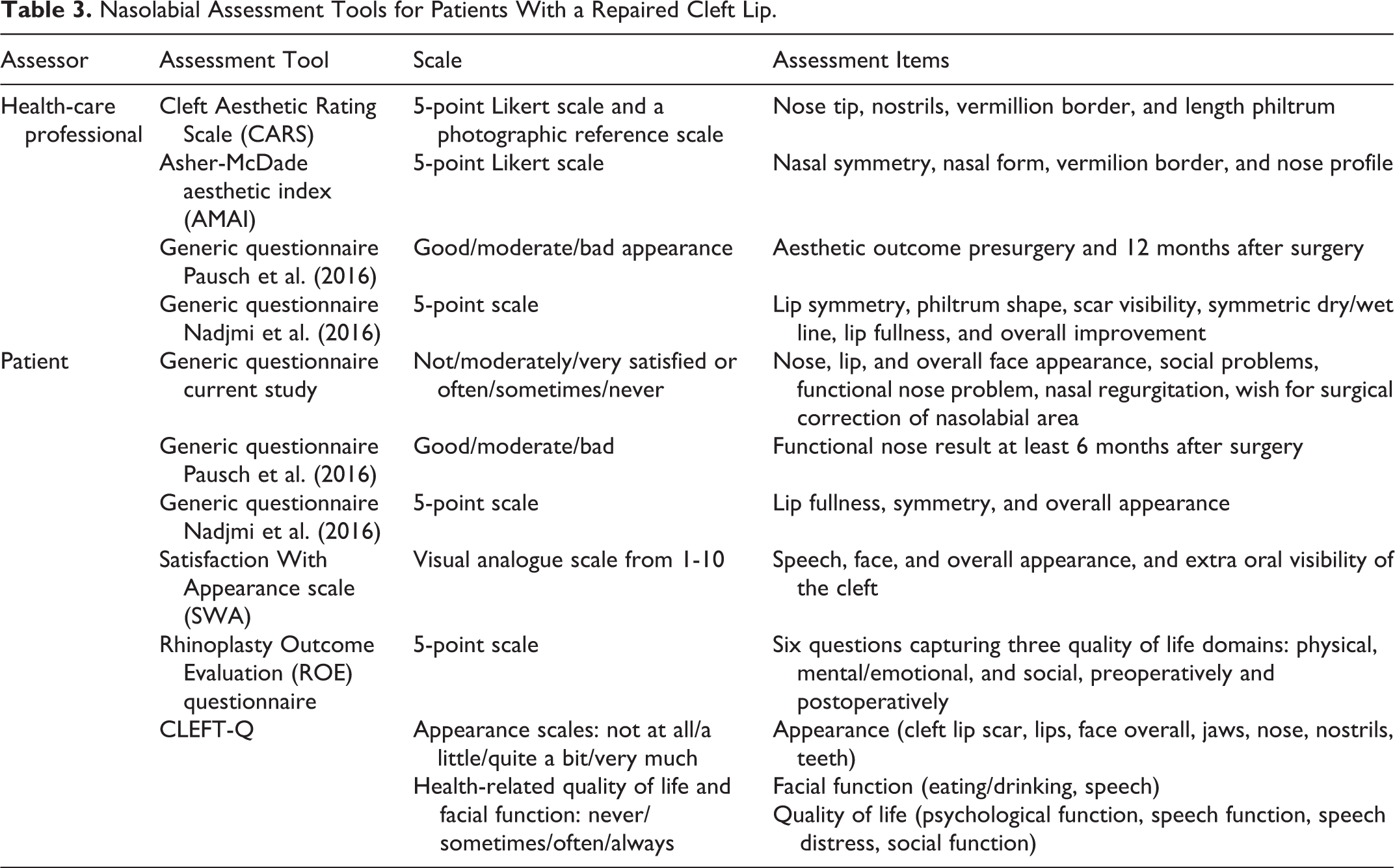
A commonly used evaluation method for nose satisfaction after rhinoplasty is the Rhinoplasty Outcome Evaluation (ROE) questionnaire, assessing the state of the nose preoperatively and postoperatively (Alsarraf et al., 2001). Byrne et al. (2014) and Roosenboom et al. (2014) both evaluated aesthetic outcome satisfaction using the ROE in a patient group with a mean age of 22 and 27 years respectively and compared it to the AMAI of a professional panel. Although both studies found a significant increase in patient satisfaction 1 year postoperatively, no correlation with the panel’s objective outcome was found (ρ = 0.054 and 0.21, respectively). They too, stressed the importance of factors other than technical skill to be important for patient satisfaction, like positive reactions of their environment after rhinoplasty and the communication skills of the surgeon, recognizing the patient’s expectations and provide a realistic prognosis of the expected results. Opposed to the abovementioned findings, Gassling et al. (2015) concluded the ROE and AMAI were largely compatible in their study (Table 3). However, they came to this conclusion because the subjective and objective outcomes were descriptively congruent, not because a statistical correlation was performed between the ROE and AMAI scores.
Some research groups describe the use of different scales for the subjective and objective analysis as a weakness of their study (Keijser et al., 2016). Similar to our study, Pausch et al. (2016) used a generic scale for patient satisfaction (good/ moderate/ bad appearance). They compared the aesthetic outcome before and after secondary rhinoplasty, having the professional panel use the same rating scale. Nonetheless, substantial differences between patient and professional assessments were found (Cohen κ = 0.39). This applies to Nadjmi et al. (2016) too, where a 5-point scale compared preoperative and postoperative results from secondary lip reconstruction for both patients and physicians. Though the physicians and patients both had high scores for postoperative satisfaction, they concluded no correlation between scores was found (no correlation coefficient displayed; Table 3). An explanation could be that professionals rate their satisfaction with the surgery technical result and the patients more what they find aesthetically pleasing. These studies reaffirm that satisfaction is not only captured by aesthetic results and might include factors that cannot be defined by objective scales. Therefore, using the same assessment method for subjective and objective evaluation seems faulty.
In the current study, patients and cleft surgeons mostly agree on a very satisfactory nose and lip appearance, as this category had the lowest CARS score (Figures 2 and 3). On the moderately and not satisfactory appearances, as judged by the patients, there was a less clear distinction between median scores. Moolenburgh et al. (2008) and Semb et al. (2005) found similar results, concluding the severity of deformity is no indicator for patient satisfaction. Our data signify the importance of a good nose result, not only aesthetically but functionally too, as the highest correlation to a wish for surgical correction of the nasolabial area was when the patient was less satisfied with their nose appearance or experienced functional nose problems more often. Some other studies, however, conclude that the lip is of more influence than the nose when assessing CL±P faces, because the lip is both functionally and aesthetically a dominant structure of the face (Deall et al., 2016; Nadjmi et al., 2016).
All these data support the need for a reliable PROM specifically designed for the different nuances applying to CL±P patients. In the last couple of years, such an instrument has been developed: the CLEFT-Q. The CLEFT-Q has been validated for patients aged between 6 and 29 years in different countries in North America, Europe, and Asia (Tsangaris et al., 2017a; Wong Riff et al., 2017). It consists of a total of 171 items, divided into 13 scales, evaluating the appearance, health-related quality of life, and facial function and each subdomain represents an independently functioning scale (Wong Riff et al., 2018; Table 2). Normative values of this rigorously developed instrument have recently been published, in addition to the translation and cultural adaptation of the CLEFT-Q to 3 Spanish language varieties (Tsangaris et al., 2017b; Klassen et al., 2018). Because of this elaborate validation, the CLEFT-Q has the potential of becoming the primary PROM for CL±P patients.
Conclusions
So far, no objective nasolabial appearance evaluation method has been created with a strong correlation to patient satisfaction with their nasolabial appearance in patients with a repaired unilateral cleft lip. Therefore, we evaluated the recently published CARS, as is used as a quick objective evaluation method with an equal weight on nose as on lip assessment.For the CARS as well, a negligible and weak correlation was found with patient aesthetics satisfaction for the nose and lip, respectively. Most literature supports this discrepancy, suggesting other factors play a role in patient satisfaction that are impossibly objectified with assessment methods. The recurrent advice is a strong emphasis should remain on clear communication between the physician and patient regarding their expectations, perception, and satisfaction of surgery results.
Footnotes
Authors’ Note
Dr. Mulder and Dr. Mosmuller are researchers, Prof. Dr. Ir. de Vet is a professor in clinimetrics, and Dr. Don Griot is a cleft surgeon.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.