
Abstract
Keywords
Introduction
Compression hosiery (CH) aims to reduce swelling and pain of the limbs in patients with various diagnoses, including lymphoedema, lipalgia, varicose veins, venous insufficiency, chronic wounds, and post-thrombotic conditions. 1 In the Netherlands, 2% of the population wears CH. CH belongs to the top five assistive products. 2 In Germany, as many as 10% of the population uses CH. 3 To our best knowledge, there are no published reliable international prevalence figures for CH.
Despite the positive physical effects of CH, adherence to wearing CH every day or nearly every day is low. Reported rates of non-adherence in the literature vary between 33% and 52%.4,5 Non-adherence carries a high risk of complications such as chronic wounds, erysipelas, reduced mobility, and pain, thereby decreasing autonomy and quality of life and increasing healthcare costs. 6 The main factors contributing to non-adherence are physical limitations, health literacy, discomfort, financial issues, psychosocial factors, and problems with donning and doffing CH.7,8 Sippel et al. 9 found that 27% of CH wearers cannot don and doff CH independently. In addition to the high costs of home care assistance, this results in a loss of autonomy for CH wearers. 8
Most wearers of CH could be independent in donning and doffing CH if they used appropriate assistive products for donning and doffing CH (hereafter abbreviated as APD). 9 However, people who wear CH often do not obtain any APD or have an APD that does not fully match their needs.10–12 Currently, APD are not used to their full potential.8,10 This is mainly a consequence of the organisation of the current provision process for CH and APD, which is described for the Netherlands in Textbox 1. To our best knowledge, no study has yet been conducted on the improvements needed to facilitate optimal use of APD in CH wearers.
This study aimed to optimise the provision process of APD to ensure that every wearer of CH has access to the most suitable APD and the appropriate care required to achieve independence in donning and doffing CH. Therefore, three research questions were formulated: (1) What bottlenecks are perceived in the provision process of APD by representatives of interested parties (patient, care professionals, and health insurers)? (2) What principles are considered important in this provision process according to these representatives? (3) What solutions do representatives of interested parties propose to address the bottlenecks, and how can these solutions be translated into concrete actions and tools to implement an optimal provision process? Care related to compression therapy in the Netherlands is described in the quality standard Compressiehulpmiddelenzorg,
13
which is based on the principles of stepped care. For the provision of assistive devices, the focus is on the patient’s intended functioning rather than on diagnosis, as governed by the Health Insurance Act. Within this quality standard, however, little attention is paid to donning and doffing CH and to the provision of APD. In the Netherlands, CH is most often prescribed by general practitioners, dermatologists, and vascular surgeons. Patients are subsequently referred to a compression therapist (CT), usually at a different location from the prescribing physician. Despite their title, CTs are commercial providers who fit and supply CH and can claim reimbursement for the product from health insurers. CTs are not permitted to claim reimbursement for treatment. Often, the required CH is in stock, allowing patients to receive it immediately. If not, the CH is ordered and provided during a second appointment. In some cases, one pair of CH is supplied initially and, if it performs well, a second pair is provided later. After several weeks, most CTs evaluate the performance of the CH, often by telephone. CTs also provide APD but are not reimbursed for the time required to practise donning and doffing with these devices. Simple APDs, such as slip-on aids, may be provided directly. These devices are sometimes discounted by health insurers within the reimbursement that CTs are allowed to claim for CH. For more expensive or complex devices, such as arm extension frames and electrical devices, patients are referred to an occupational therapist (OT) for advice. Without advice from an OT, most health insurance companies will not reimburse these devices. Range of available APDs is extensive, with more than 30 different devices marketed by various manufacturers and importers.
Textbox 1: Provision process of CH and APD in the Netherlands
Method
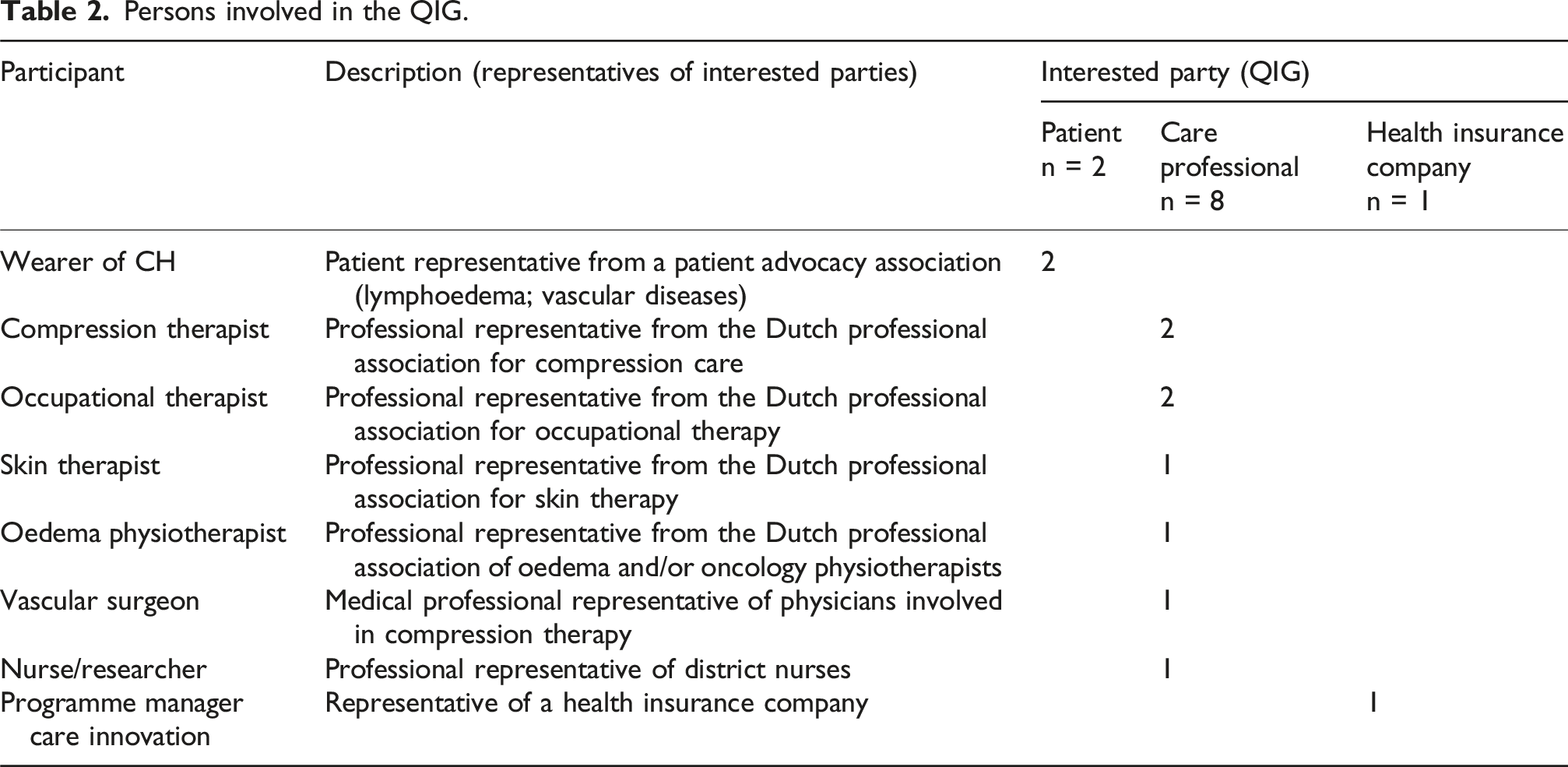
The study employed an experience-based co-design approach using a participatory design. In experience-based co-design, academics collaborate with representatives of interested parties to identify key moments in a process, generate knowledge, and co-design care pathways. 14 In this study, patients, practitioners, CTs, OTs, skin therapists, oedema physiotherapists, and healthcare insurers collaborated in defining the problems and developing interventions. This approach ensured that diverse perspectives were integrated, aligning quality improvements with the preferences of representatives of interested parties and fostering effective implementation. 15 Experience-based co-design research comprised a discovery phase, in which bottlenecks in a process were identified, and a co-design phase, in which a quality improvement group (QIG) of patients and professionals optimised the process. 15
Procedure
Based on Bate and Roberts, 15 the experience-based co-design study was conducted in two phases.
CH: compression hosiery; APD: assistive products for donning and doffing compression hosiery; CT: compression therapist; OT: occupational therapist
Persons involved in the QIG.
The study was conducted from January 2022 to September 2022. The Generic Quality Framework Care for Assistive Products,
16
in particular the Process Description Medical Devices
17
(Figure 1), was used as a template to describe the optimal provision process of APD. This framework is commonly used in the Netherlands to describe provision processes for assistive products. Process Description Medical devices (Nictiz, 2009).
17
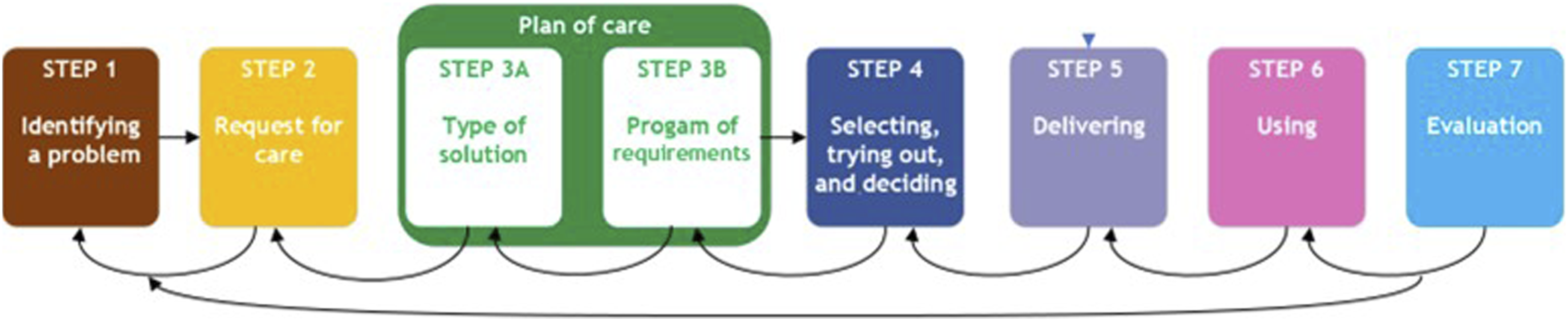
The co-design phase comprised six meetings. At the start of the initial meeting, participants were asked to share their interests in the provision process from the perspective of the interested parties they represented. By openly addressing the issues at hand and the occasionally conflicting interests, a conducive environment was established, fostering constructive discussions in which all opinions were acknowledged and respected. The initial meeting focused on whether the identified bottlenecks were recognisable and which were considered most significant. In addition, the important principles of the provision process of APD were established during this meeting. Across the six meetings, each step of the provision process, was elaborated, except for steps 1 and 2, which were discussed together during the first meeting. For each step, the four-D cycle (Discover, Dream, Design, Destiny) of appreciative inquiry was followed. 18 The current situation and associated bottlenecks were discussed. Subsequently, each participant wrote three memos outlining their desired situation, which elements of the current provision process should be maintained, and which elements should disappear or be changed. These memos were placed on three large posters. The individual input was discussed within the group, and advantages and disadvantages were considered. Taking these aspects into account, the aim was to identify the most optimal provision process for all participants while acknowledging their diverse interests. In addition, the roles and responsibilities of all interested parties involved in each step were discussed. During each meeting, the QIG strived to reach consensus on the content and direction of the respective step within the framework. Participants also brainstormed potential tools to support caregivers and patients in performing according to the optimal provision process. The researchers documented the consensus reached during each meeting in a single working document describing the optimal provision process of APD, which was expanded step by step. This document was emailed to all participants after each meeting. Participants discussed the document with the groups they represented, and each subsequent meeting started with feedback from these constituencies. Based on this feedback, joint decisions were made on whether adjustments were desirable and feasible. The next step of the Process Description Medical Devices was then discussed following the same approach. After the final meeting, the description of the optimal provision process was completed and submitted to patient advocacy associations, professional associations, and industry associations. Finally, the optimal provision process was presented to and adopted by the steering group of the HASHTEK study to facilitate commitment. Supporting tools were subsequently developed in small working groups consisting of participants with relevant expertise, supplemented by a researcher. Where applicable, existing tools were assessed and further developed when necessary.
Data processing
Notes and audio recordings were made during each meeting by one of the researchers (EH), with the consent of the participants. The audio recordings were re-listened to by one researcher and processed together with the meeting notes to produce a discussion report. Specific decisions were extracted by the research team and documented in the concept document describing the optimal provision process. The existing quality standard on care for compression therapy 13 was used as a basis to ensure the possibility of seamless integration into a unified quality standard in the future. Member checking was conducted after each meeting. The concept document was shared with all participants, who discussed it with their respective constituencies. Feedback was brought to the subsequent meeting, where adjustments were made if necessary.
Quality criteria
The description of the quality criteria was based on the framework proposed by Frambach et al. 19 The two researchers jointly processed the results of the discussions and the decisions regarding the optimal provision process, thereby ensuring investigator triangulation (credibility). Notes and audio recordings were made during the meetings, and both sources were incorporated into the analysis to prevent misinterpretation (confirmability). The resulting document was distributed to all participants by email approximately 1 week after each meeting to ensure persistent observation (confirmability and credibility). Participants discussed this document with their respective constituencies after every meeting (member checking) to enhance credibility and dependability. Following completion of the preliminary draft of the optimal provision process, the document was submitted to the study’s steering group and to the participants’ constituencies for additional member checking (credibility). The feedback received was discussed during the sixth meeting, with the aim of reaching consensus. One of the researchers (EH) wore CH and was trained as an OT. This enabled her to view the process through a similar ‘lens’ to that of representatives of patient associations and OTs, and to ask probing questions to obtain more in-depth information. To enhance confirmability, she exercised caution to ensure that her personal experience did not influence the process and reflected critically on her role throughout the research process to ensure reflexivity. The other researcher (LvdH) did not have this personal experience and acted as chairperson, moderating the meetings. This division of roles within the research team was consistent with the recommendations of Moser and Korstjens. 14
Transferability of both the method used to develop an optimal provision process for assistive devices and the results of this research to other APD provision processes was enhanced by providing a detailed description. This enables readers from other countries who may wish to adopt the method to assess its suitability for their specific context.
Results
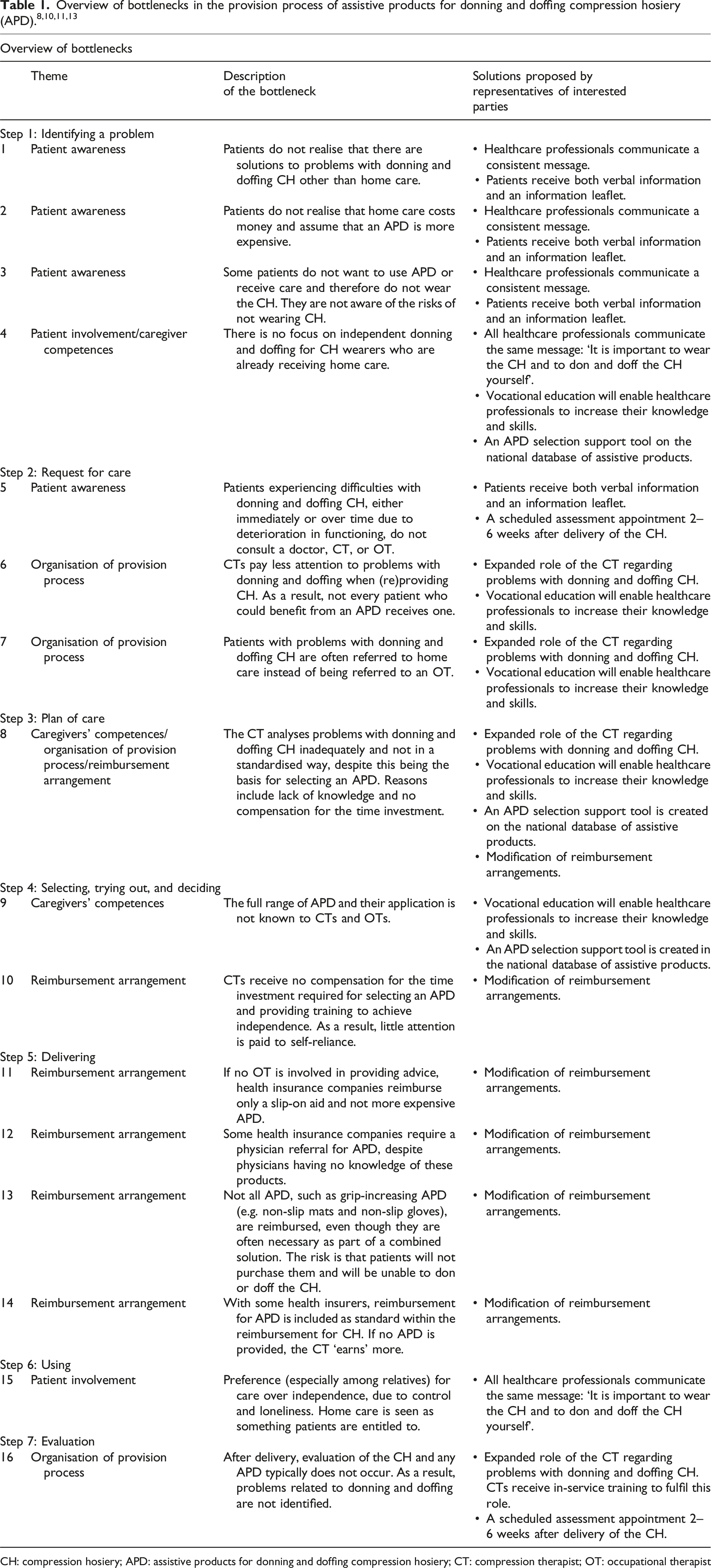
What bottlenecks were perceived by interested parties in the provision process of APD?
All bottlenecks identified in earlier studies were confirmed by both the steering group of the HASHTEK study and the participants of the QIG. These bottlenecks were addressed by changes to the provision process of APD, as well as by the development of supporting tools.
What are important principles in this provisioning process according to representatives of interested parties?
Principles for the provision process were proposed by participants in the QIG, partly informed by obligations in legislation and by societal trends. Participants discussed their viewpoints on these principles and reached consensus as a basis for the optimal provision process: (1) Treatment by a single healthcare professional as much as possible. This was the preference of CH wearers and was adopted by the other representatives of interested parties. Involvement of an additional professional inevitably results in delays in the process, and the need to provide repeated explanations is a source of frustration for patients. (2) Assistance is only provided when individuals are unable to don or doff CH independently, even when using an APD, and when there is an absence of informal caregivers who are able to provide such assistance. This principle is particularly relevant in the context of staff shortages in home care organisations and the high costs associated with care provision. (3) For the provision of assistive devices, the focus is on the patient’s intended functioning rather than on diagnosis. Intended functioning is defined as the activities that the patient wishes to perform, can perform, and is permitted to perform from a care perspective. This principle is governed by the Health Insurance Act in the Netherlands. (4) Stepped care, which is standard practice in the Netherlands, is applied in the selection of APD. Stepped care entails offering patients the most effective, least burdensome, and least costly assistive device possible, taking into account the nature and severity of the problem.
According to representatives of interested parties, what is the optimal provisioning process for APD to achieve independence of the CH wearer in donning and doffing CH?
Based on the formulated findings, the optimal provision process was designed by the QIG. Previously, care as usual entailed that patients with problems with donning and/or doffing CH were automatically referred to an OT. In line with principle 1 (preference for treatment by a single healthcare professional as much as possible), it was determined that patients with problems with donning and/or doffing CH should no longer be automatically referred to an OT. Instead, the CT – whom all patients encounter early in the process because they provide the CH – also pays attention to maintaining self-reliance, selects an APD if necessary, and practises its use with the patient. For this purpose, the CT describes the functional diagnosis, consisting of the diagnosis, prognosis, limitations, and the activities that the patient wishes to perform, can perform, and is permitted to perform from a care perspective, as well as the programme of requirements for the patient’s intended functioning (principle 3). Based on these requirements, the CT selects an APD in accordance with the principles of stepped care (principle 4). First, the most basic or least expensive tool that appears appropriate is tried. If self-reliance is not achieved after a maximum of three practice sessions, the patient is referred to an OT for additional training or for a second opinion on the choice of APD. The OT also provides advice with a focus on intended functioning (principle 3) and stepped care (principle 4). This procedure ensures that as many patients as possible are treated by a single healthcare professional and that waiting lists for OTs, due to shortages, are avoided as far as possible. To ascertain the effectiveness of donning and doffing in practice, evaluation is essential. The agreed timing for evaluation is 4–6 weeks after delivery of the APD, and this evaluation can be conducted concurrently with the evaluation of the performance of the CH. In the optimal process, CTs are instructed to refer patients to an OT rather than to home care, in order to ensure that individuals only receive home care when they are unable to don and doff CH independently, even with an APD, and when no informal caregivers are available (principle 2). If the OT concludes that self-care is not feasible, the patient is referred to home care. Only in cases of very complex problems (e.g. advanced dementia or paralysis of the upper extremities), where it is evident that self-reliance is not feasible, can a patient be directly registered for home care. If a patient is already receiving home care for other conditions, the home care worker should still attempt to achieve self-reliance with regard to donning and doffing CH. If this is unsuccessful, an OT is consulted and the standard procedure is followed. In all situations, the CT delivers the APD. The flowchart (Figure 2) illustrates the procedure from three different initial situations. The optimal provision process is further described in a document outlining the roles, tasks, and responsibilities of all interested parties at each step of the process. Flowchart of the optimal provision process for APD.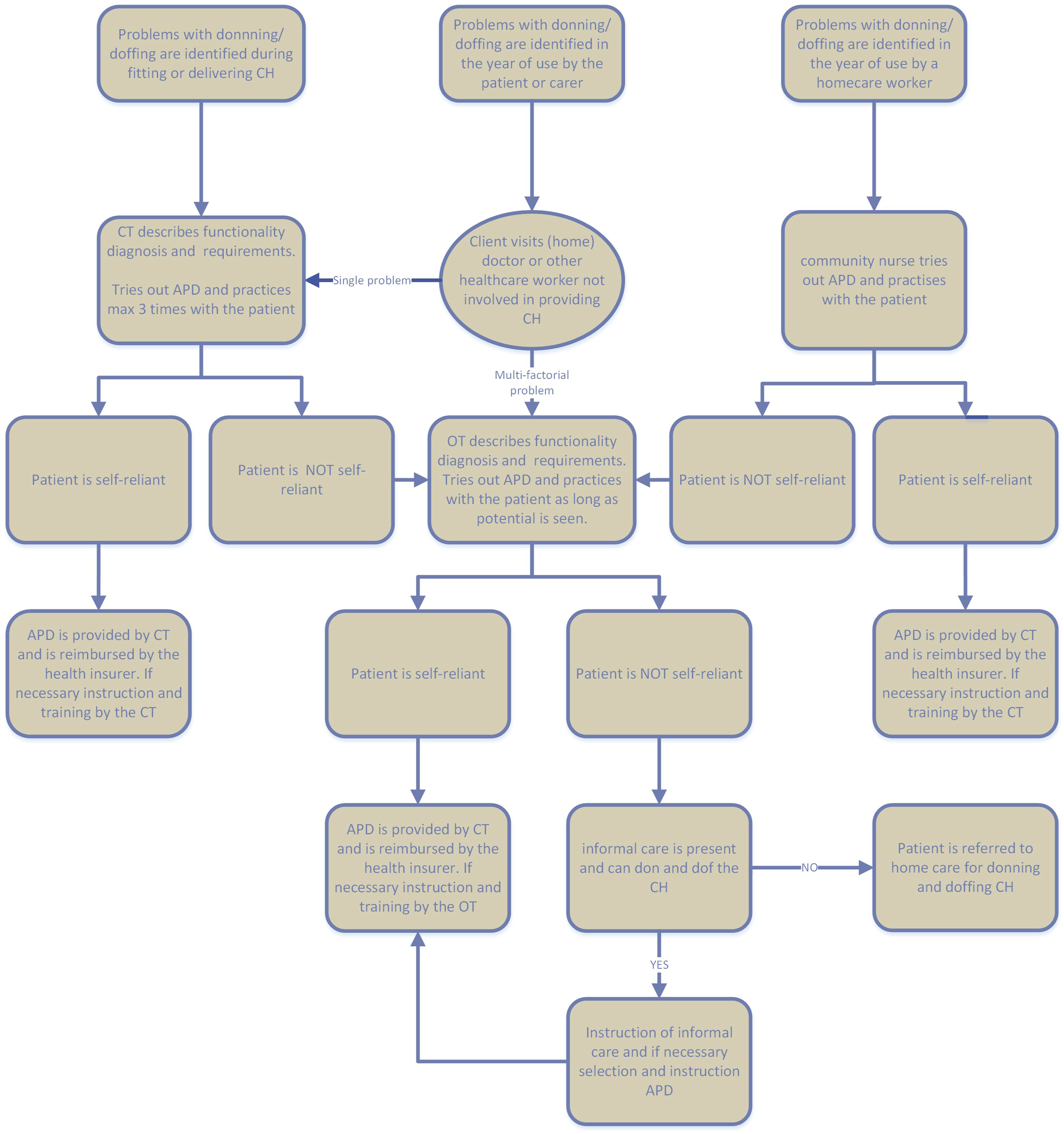
What solutions do representatives of interested parties see to solve the bottlenecks, and how can these be translated into concrete actions and tools to implement an optimal provision process?
To address the identified bottlenecks in service provision and to better meet patients’ needs, representatives of interested parties proposed the following solutions: (1) The CT should take on an expanded role, addressing problems with donning and doffing and, where necessary, selecting an appropriate APD and practising its use with the patient. (2) The OT should be involved prior to referral to home care (bottlenecks 6–8, 16). (3) A follow-up assessment 2–6 weeks after delivery of the CH should be scheduled to identify any problems with donning and doffing CH (bottlenecks 5, 16).
To enable CTs to perform this expanded role effectively: • The CT should receive in-service training in APD selection, clinical reasoning, motivational interviewing, and training strategies. • Other healthcare professionals should be informed about the expanded role of the CT.
To enhance patient awareness: (1) Patients should receive clear and comprehensive information during consultations with all involved healthcare professionals. (2) To reinforce verbal communication, the CT should provide an information leaflet at the time of CH delivery. The leaflet highlights the importance of wearing CH and maintaining independence, instructions for donning and doffing, the availability of APDs, and procedures for addressing related problems. (3) Healthcare professionals should convey a consistent message (bottlenecks 1–3, 5).
Patient independence can only be enhanced if all healthcare professionals involved (practitioners, CTs, OTs, nurses, and physiotherapists) communicate a consistent message: ‘It is important to wear the CH and to don and doff it independently. Home care support is limited and should be reserved for situations in which self-management is not possible, even with an APD. Moreover, independence offers clear benefits, such as avoiding reliance on home care and allowing greater flexibility in daily routines’ (bottlenecks 4, 15).
Attention should be paid to strengthening the competences of all professionals involved, particularly CTs, OTs, and home care workers (bottlenecks 4, 8, 9). Vocational training can enhance their knowledge and skills. To support APD selection, a brand-independent decision-support tool was developed. In addition, a standardised recommendation form was developed to support justification of APD selection to health insurers.
The reimbursement structure requires modification: (1) To support the expanded role of the CT, reimbursement should cover the additional time required for training in the use of APDs (bottlenecks 8, 10–14). This requires changes by health insurers, as CTs are currently reimbursed only for the product (CH or APD) and not for treatment or training. (2) Reimbursement should include all APDs necessary to achieve patient independence, even if this involves two relatively costly electric devices (for donning and doffing), as well as low-cost aids such as non-slip gloves or mats. Without reimbursement for these essential items, patients may remain dependent on others or discontinue CH use, resulting in higher follow-up care costs than would arise from reimbursing low-cost APDs.
Implementation of the optimal provision process will be carried out through patient organisations, professional associations, and the health insurance branch association. In the future, this process will be incorporated into the quality standard Compression Therapy Care (Compressie Hulpmiddelenzorg).
Participants in the QIG emphasised the importance of supporting both patients and professionals in adopting the new APD provision process. The tools described below were developed to facilitate this transition: • Patient information leaflet – covering the importance and maintenance of CH, solutions for problems with donning and doffing, reimbursement information, and the benefits of self-reliance. • Vocational training – for CTs, OTs, and optionally home care workers, focussing on motivational interviewing, clinical reasoning, functional assessment, translation of functional to technical requirements, knowledge of APDs, patient training, reporting to health insurers, and APD evaluation. Regular CT and OT curricula should also include guidance on the use of APDs. • Selection support tool – providing independent, brand-neutral information via the Dutch national assistive products database (Vilans Hulpmiddelenwijzer). • Standardized forms – for (a) functional assessment and APD selection and (b) APD evaluation.
All tools are available in Dutch via www.compressiehulpmiddelenzorg.nl and https://www.hulpmiddelenwijzer.nl/activiteit/persoonlijke-verzorging/aan-en-uitkleden/steunkousen-aan-en-uittrekken/keuzehulp-bij-steunkousen-aan-en-uittrekken.
Discussion
In this study, an optimal provision process for APD was systematically developed, informed by evidence and with careful consideration of the concerns of key interested parties. The role of the CT was expanded to include assessment, instruction, training, and follow-up related to APD. Owing to the co-design approach, consensus was reached efficiently despite the substantial nature of the proposed changes. Employing participatory action research through experience-based co-design enabled the establishment of basic principles for the provision process, the generation of solutions for identified bottlenecks, and the proposal of changes to tasks and roles of interested parties within the APD provision process, as well as to the reimbursement of CH, APD, and CT services.
Participatory action research was essential in this study because it enhances scientific rigour by incorporating diverse experiential and contextual knowledge. This strengthens relevance and allows for triangulation of findings. The approach gave voice to patients and aligns with the slogan ‘Nothing about us without us’, which conveys the principle that no policy should be adopted without the full and direct involvement of those affected by it. 20 Patient representatives (CH wearers) were engaged as full collaborators in this research. They expressed a strong preference for treatment by a single healthcare provider and were able to justify this effectively. This represented a significant shift from the traditional approach, in which individuals with difficulties in donning or doffing CH were referred by the CT to an OT. Without participatory action research—where all interested parties, including patients, discussed the benefits and consequences of the proposed changes – this shift would likely not have emerged. This finding is consistent with Cusack et al., 21 who describe the added value of participatory action research, particularly its potential to generate results that might otherwise be unattainable. Interestingly, a comparable study conducted in the Netherlands during the same period 22 recommended that CH wearers should always be referred to an OT when experiencing problems with donning and/or doffing CH. That study employed the Delphi method, in which relevant representatives of interested parties were consulted individually, without group discussion. The contrasting findings suggest that both the chosen methodology and the selection of representatives can substantially influence outcomes. They also highlight the potential value of including individuals who, beyond representing their own interests or those of their stakeholder group, are able to adopt a broader societal perspective, demonstrate openness to change, and articulate a forward-looking vision. Participatory action research relies on methods that accommodate diverse viewpoints and encourage discussion of solutions, whereas the Delphi method emphasises quantification and majority opinion without facilitating dialogue.
An optimal provision process for assistive products supports effective implementation and sustained integration into daily life. Previous research shows that insufficient information and limited attention to instruction and integration of CH into daily routines lead to non-use.23,24 When funding is allocated solely for the acquisition of an assistive product without addressing the practical barriers that hinder its use, such devices often remain underutilised, calling the investment into question. 25 Non-use of APD may lead to non-use of CH, which is a well-established and effective intervention that is fully reimbursed by Dutch health insurance. Consequently, the original problem may persist or worsen, potentially resulting in complications and/or unnecessary reliance on home care. Similar patterns have been observed with other assistive products, for which reimbursement often covers the device itself but not the associated services required for effective use, such as assessment, adjustment, instruction, or user training. 25 The lack of attention to instruction, training, and integration is particularly striking given the increasing emphasis on self-reliance, a priority reinforced by staff shortages in healthcare driven by population ageing and declining workforce inflow. 26 Addressing this gap through structured and targeted investment in services accompanying assistive devices, as developed in this study, represents a feasible strategy towards more future-proof long-term care delivery.
Thanks to the co-design approach and the consensus achieved, there is immediate national support for implementation of the new provision process. Successful implementation is further supported by the expectation that all interested parties will benefit from the revised approach. 27 Increased self-reliance enhances the autonomy of CH wearers, allowing them to organise their daily activities without dependence on care providers. For CTs, the new provision process broadens and enriches professional practice, while potentially reducing waiting lists for OTs. Home care organisations benefit by promoting self-reliance, improving clients’ autonomy and well-being, addressing staff shortages, and reducing physical strain on care workers. By supporting patient independence, health insurers may reduce healthcare costs while optimising quality of care and quality of life. Despite these advantages and the consensus among interested parties regarding the optimal provision process, successful implementation is not guaranteed. Without modification of the current financial compensation system, implementation is likely to fail. CTs will only invest additional time in supporting patient independence if they are reimbursed for this effort. Because the Dutch Health Insurance Act currently defines CTs as suppliers who are not permitted to charge for treatment, amendments to the Act are required. Reimbursement structures must actively incentivise CTs to support self-reliance. Although care for CH may initially become more costly, long-term costs are expected to decrease due to reduced reliance on home care. Additional barriers to implementation include the potential shortage of CTs following task expansion, and the possibility that not all CTs are willing or able to take on these additional responsibilities.
Strengths and limitations
A key strength of this study is the deliberate creation of a respectful and safe dialogue culture among representatives of interested parties, who were delegated by different professional and interest groups and were often unfamiliar with one another. This is particularly important in experience-based co-design research. 28 Because some interested parties had potentially conflicting commercial or organisational interests, the approach – guided by lessons from earlier studies 29 – explicitly emphasised openness, transparency, and the primacy of patient interests. This safe environment facilitated open and constructive discussions and encouraged participants to look beyond their own organisational perspectives, reducing the risk of biased or compromise-driven outcomes and supporting the development of a genuinely patient-centred provision process.
Another strength is the use of an established and previously validated approach 29 to describe the optimal provision process for APD, grounded in the Generic Care Quality Framework for Assistive Devices 16 and the Process Description Medical Devices. 17 This structured methodology proved efficient and capable of generating clear, actionable results within a relatively short timeframe, making it a valuable approach for designing or revising provision processes. Furthermore, the resulting process aligns with international recommendations for assistive device delivery, 30 supporting the robustness and relevance of the proposed approach.
A limitation of this study concerns uncertainty regarding the extent to which representatives of interested parties consistently consulted their constituencies during the co-design process. Although delegates were expected to report back to their organisations after each meeting, no formalised feedback mechanism was defined, and there is no evidence that this occurred systematically. As a result, the perspectives incorporated may reflect those of the QIG participants rather than the broader groups they represented. This may have led to underrepresentation of divergent or minority viewpoints, thereby narrowing the overall perspective. 31 This risk was partially mitigated by presenting the final working method to the advisory group, where all interest groups were represented at board level; nevertheless, the lack of a structured consultation procedure remains a limitation.
Conclusion
This study demonstrates that addressing bottlenecks in the APD provision process requires expansion of the CT’s role to include APD selection, instruction, and user training, thereby supporting the principle that care should be delivered by a single healthcare professional whenever possible. APD selection should be guided by the patient’s functional abilities and follow a stepped-care approach to ensure alignment with core principles. When CTs are unable to support patients in achieving independence, OTs assume responsibility for more comprehensive assessment and training. This approach ensures that home care is reserved for individuals who, even with appropriate APD support and adequate training, remain unable to don and doff CH independently and lack an informal caregiver. To enable implementation of this optimal provision process in practice, tailored information materials were developed for patients and healthcare professionals, CTs and OTs require additional training, and reimbursement structures must be adapted accordingly.
Footnotes
Acknowledgements
We would like to thank the following individuals and organisations: The participants of the QIG for candidly sharing their experiences and perspectives. NLNet, Harteraad, NVCZ, EN, and NVFL for their assistance with recruiting participants for the QIG and for providing feedback on the preliminary draft. Artificial intelligence (AI)-assisted technologies were used for writing assistance.
Ethical considerations
Author contributions
Conceptualisation: Edith Hagedoren-Meuwissen, Loek van der Heide, Uta Roentgen, Sandra Zwakhalen, Ramon Daniëls.
Formal analysis: Edith Hagedoren-Meuwissen, Loek van der Heide.
Funding acquisition: Edith Hagedoren-Meuwissen, Uta Roentgen, Loek van der Heide, Ramon Daniëls.
Investigation: Edith Hagedoren-Meuwissen, Loek van der Heide.
Methodology: Edith Hagedoren-Meuwissen, Loek van der Heide, Uta Roentgen, Sandra Zwakhalen, Ramon Daniëls.
Supervision: Uta Roentgen, Sandra Zwakhalen, Ramon Daniëls.
Writing – original draft: Edith Hagedoren-Meuwissen.
Writing – review & editing: Uta Roentgen, Sandra Zwakhalen, Ramon Daniëls.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZonMw (project number 10310042110001). ZonMw funds research and innovation in health, healthcare, and well-being, encourages the use of knowledge, and highlights knowledge needs (![]() ). The grant was awarded to the participating organisations rather than to individual researchers. The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
). The grant was awarded to the participating organisations rather than to individual researchers. The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All meeting reports, presentations, and other study-related documents are available from the DataVerseNL database (![]() ).
32
).
32