
Abstract
Background
Brain-computer interfaces (BCIs) are technologies that may allow children to operate assistive devices by translating their brain signals into commands for the devices. BCI technology requires specific user skills for successful operation. However, the cognitive demands remain relatively unexplored, particularly in pediatric populations, where developmental differences and cognitive variability significantly influence usability and performance.
Objective
This review explores what has been reported on the cognitive requirements for using BCIs, with a focus on the pediatric population.
Methods
A systematic search was conducted across six databases (Scopus, Web of Science, Embase, MEDLINE, PsycINFO, and CINAHL) for original research studies involving children aged 5–18 using BCIs for control purposes. Inclusion criteria focused on studies reporting cognitive factors relevant to BCI performance. Data extraction and analysis followed the PRISMA-ScR guidelines.
Results
Seven studies met the inclusion criteria, highlighting attention, motivation, and processing speed as key factors influencing BCI performance. However, the limited pediatric research suggests significant gaps in understanding the cognitive factors involved in BCI performance.
Conclusions
Further research is necessary to tailor BCI systems implementation to the unique cognitive and developmental needs of children. Addressing these gaps will enhance BCI usability and effectiveness, promoting greater independence for children with motor disabilities.
Introduction
Play is a fundamental activity through which children learn and explore their environment. It contributes significantly to the development of social, cognitive, motor, and linguistic skills, promoting learning, adaptability, creativity, problem-solving and self-expression. 1 Beyond its developmental benefits, play serves as a medium for children to interact with the world, acquire new skills, and engage in social activities.
For children with motor disabilities, the opportunity to participate in play is often limited due to restricted motor control. Many lack the ability to use conventional access technologies such as switches or eye gaze systems effectively. 2 These challenges may place them at risk of learned helplessness, where repeated failures to interact meaningfully with their environment impact their motivation. 3 Brain-computer interfaces (BCIs) have the potential to address these challenges by enabling children to engage in interactions and exercise control over their environments, thereby improving autonomy.
BCIs are technologies that offer individuals with significant motor disabilities new opportunities for participation in various activities, including communication, learning, and interaction with their environments. BCIs function by detecting and interpreting neural signals from the brain to control external devices, bypassing the need for physical motor input. 4 Non-invasive BCIs use sensors placed on the scalp to measure brain activity, such as electroencephalography (EEG). There are two primary types of brain activity used in EEG-based BCIs. First, sensorimotor rhythms, which are induced by either executing or imagining movement, that is, motor imagery (MI). 5 Changes in frequency in the brain signal power in the sensorimotor area can be detected and used to control devices. Second, evoked potentials, which are brain responses to external stimuli. In the P300 evoked potential a peak occurs in the brain signal 300 ms after a visual, auditory or tactile stimulus. In the Steady State Visual Evoked Potential (SSVEP) pyramidal neurons resonate at the same frequency as a flickering visual stimuli. 5 Through signal analysis it is possible to distinguish the user’s focus and make a desired action.
Using BCI requires specific user skills, competencies, and attitudes for successful operation. 6 Several studies with adults have demonstrated the effect of specific cognitive functions on BCI performance. 7 For instance, the role of working memory, general intelligence, motivation and attention has been confirmed in P300 BCI performance.7–9 However, there is limited understanding of how these demands align with the developmental capacities of children.
Children’s cognitive, emotional, and developmental needs differ significantly from those of adults, necessitating a tailored approach to the design and implementation of BCIs. Additionally, many children with motor disabilities experience cognitive impairments related to their underlying conditions, such as cerebral palsy (CP) or neuromuscular disorders. 10 These impairments may include difficulties with executive functioning, memory, and processing speed, which could influence their ability to learn and use BCI systems effectively.
There have been some reviews of how BCI has been used with children, and while they illuminated some challenges, their aims were not specifically around examining required cognitive skills.11–13 Most studies covered in the reviews focused on BCIs for characterizing neurotypical brain signals or remediating attention disorders. Of the studies where BCI was used for control of devices, there were only a few where children with motor impairments were participants, and they controlled robots 14 and computer games.15,16 Five studies with neurotypical children were done in anticipation of the systems being used with children with disabilities, and children-controlled robots 17 or computer games,18,19 performed target selection 20 or cursor control and drove a remote-controlled car. 21 Mikołajewska and Mikołajewski 11 summarized their observations from their own research listing several special preparations that are needed for working with children, such as having pleasant child-friendly room décor and toys/games, ensuring they are positioned for optimized comfort and to prevent BCI headset movement artifacts, and making assessments and training procedures motivational. Orlandi et al.’s 13 systematic review noted challenges such as fatigue, visual annoyance or impairments, and distraction and trouble reproducing signals.
Despite the growing interest in pediatric BCI research, there is still limited knowledge about the specific cognitive requirements for effective system use among children. Most existing reviews have focused on technical feasibility, system adaptations, or clinical implementation, without addressing the underlying cognitive skills that may influence performance. Addressing this gap is critical for advancing the development of BCIs that are not only accessible and functional but also developmentally appropriate for pediatric users. Understanding the cognitive factors that influence children’s ability to engage with and control BCI systems can guide the development of training methods and interfaces, which could increase the number of people who can effectively use the BCI and enhance the accuracy of BCI performance for existing users.
This paper seeks to answer the question: What is the current evidence on the cognitive requirements necessary to use BCI technologies in the pediatric population? By examining existing research, this review aims to identify key cognitive considerations, highlight gaps in knowledge, and provide recommendations for future usage of BCI systems tailored to the needs of children.
Methods
Search strategy
Line-by-line search strategies on the six databases.
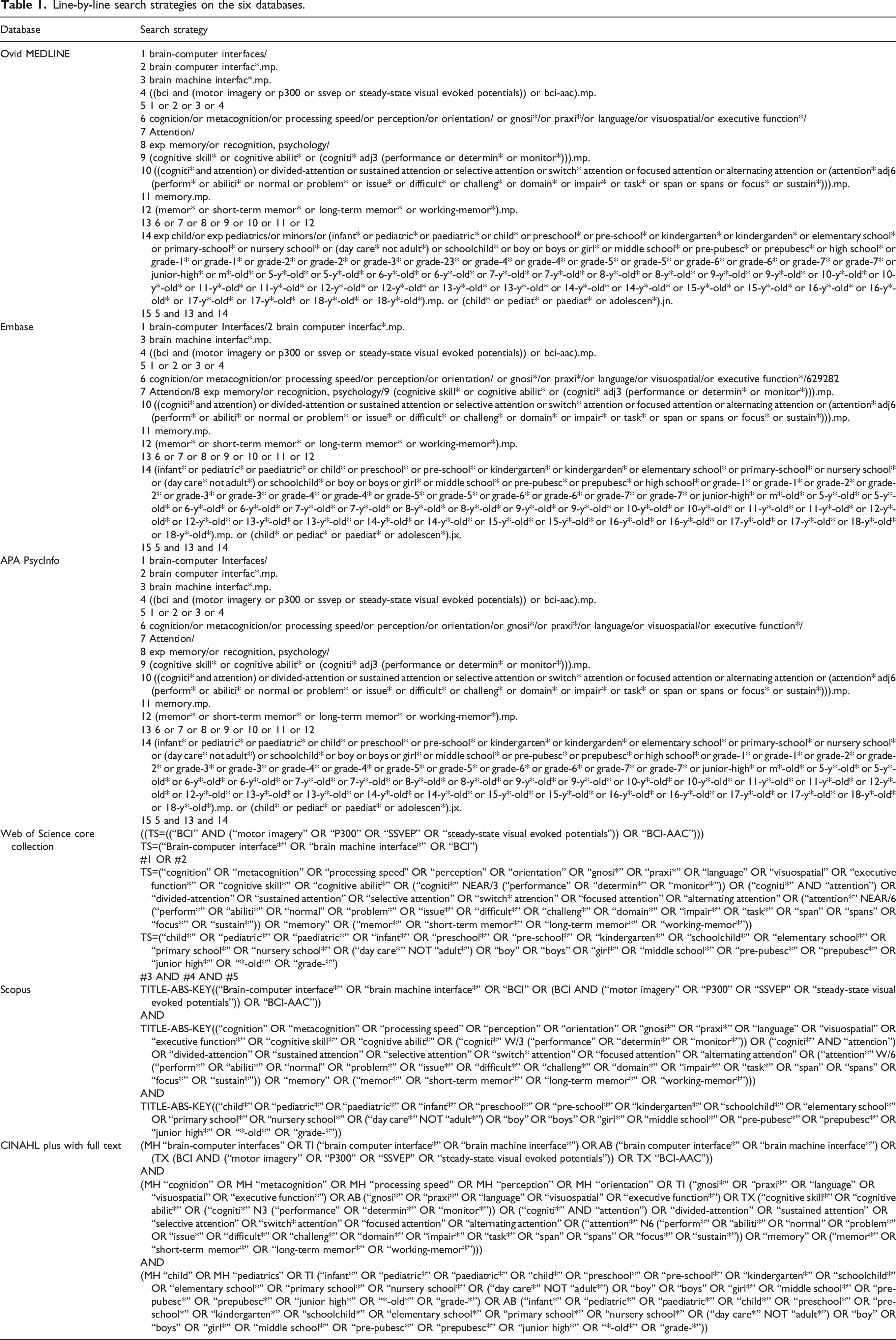
Eligible studies included articles published from each journal’s inception through December 2024. Search results were exported to Covidence, a web-based systematic review software (Veritas Health Innovation, Melbourne, Australia; https://www.covidence.org), where articles were screened for eligibility and duplicates were removed.
Selection of studies
Articles were eligible for inclusion if they met the following requirements: (1) children at or below age 18; (2) included both typically developing children and those with disabilities, such as brain injury or cerebral palsy; (3) focused on BCIs used for control purposes, including P300, SSVEP, or MI-based BCIs; (4) mentioned cognitive factors affecting BCI performance, such as working memory, attention, intelligence, or motivation; (5) original research studies employing quantitative, qualitative, or mixed-method designs; (6) published in English; and (7) published in peer-reviewed journals.
Articles were excluded from the review if they: (1) were reported as abstracts, reviews, or protocols; (2) were published but the full text was not accessible; (3) focused solely on EEG signal analysis or the technical development of BCIs without discussing user requirements; (4) involved BCIs used exclusively for training or cognitive assessment in conditions like Attention Deficit Hyperactivity Disorder (ADHD) or Autism Spectrum Disorder (ASD) without broader control applications.
Screening of studies
After duplicates were removed using Covidence, two reviewers (JRO and KA) carried out the screening and review process. First, they independently assessed the titles and abstracts of the retrieved studies to determine their eligibility. Inter-rater reliability during the title and abstract screening phase was assessed using Cohen’s kappa coefficient and indicated fair agreement (κ = 0.38). Any disagreements about eligibility were resolved through discussion and reviewed by a third reviewer (AL). Next, full-text articles were independently evaluated to confirm final inclusion. Inter-rater reliability during the full-text review phase indicated substantial agreement (κ = 0.76). Finally, data from each included study were extracted and organized for analysis.
Data analysis and synthesis
The extracted data were categorized into several key elements, including (1) age of participants, (2) type of participants (e.g., neurotypical, diagnosed with a specific condition), (3) participant description, (4) cognitive areas reported, (5) hardware used, and (6) BCI paradigms. The data was organized into a summary table to present the results concisely.
Results
The database search results are presented in the PRISMA diagram (Figure 1). Initially, 724 articles were obtained. Following the removal of duplicates, 446 articles were screened and 420 articles were excluded as they were not focused on BCI, children and cognition, not published full-text, or not original research studies. The full-text review of the remaining 26 articles led to the exclusion of 19 that did not meet the inclusion criteria (see Figure 1 for details). In total, seven articles met the inclusion criteria and were summarized in Table 2. Study selection flowchart. The flow diagram describes identification, screening, eligibility, and inclusion procedures. List of studies reporting cognitive factors in BCI. Abbreviations: EEG: Electroencephalography, mVEP: Motion-onset Visual Evoked Potentials MI: Motor Imagery, VI: Visual Imagery, CP: Cerebral Palsy, GMFCS: Gross Motor Function Classification System, ITR: Information transfer rate. NASA TLX: is a tool for measuring and conducting a subjective mental workload (MWL) assessment, PPVT-4: Peabody Picture Vocabulary Test. aSub-study contributing to the cohort reported in Huggins et al. (2022). bMotivation, interest, engagement, and fatigue were reported as modulators of BCI performance, not cognitive factors.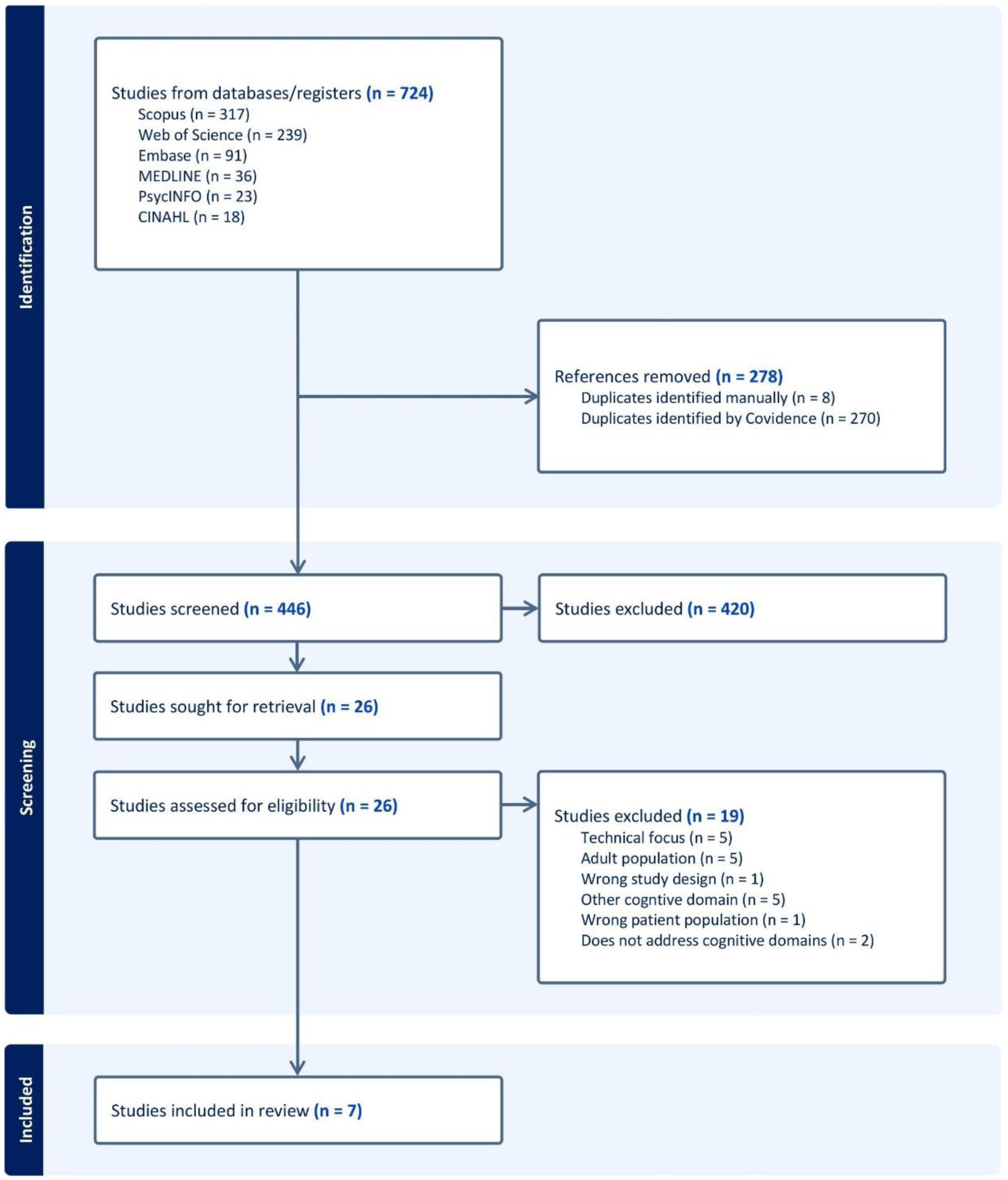
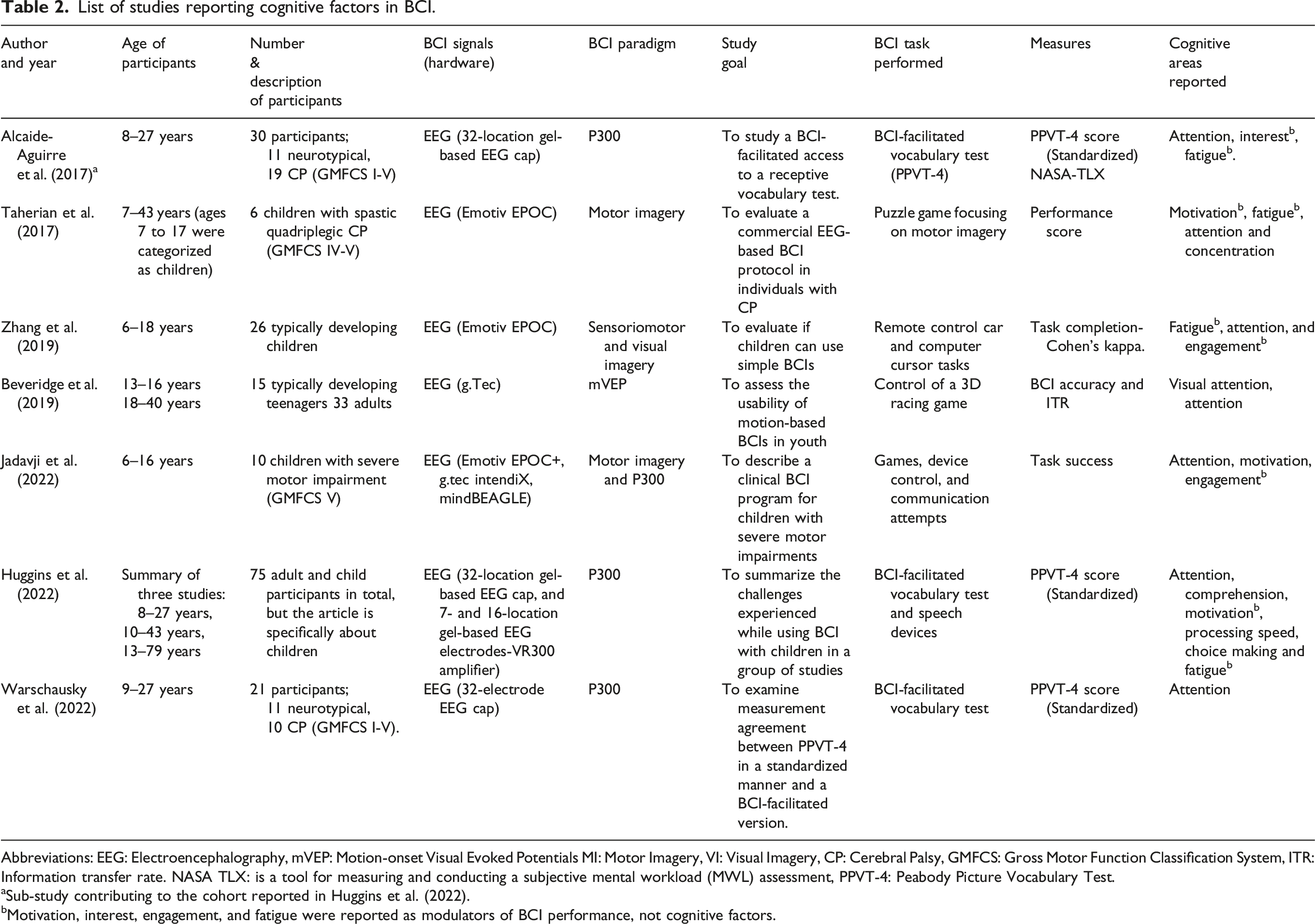
This review focused on children, with studies including participants aged 6 to 18 years. Participants were from two groups: (1) neurotypical children and (2) children with disabilities (primarily CP). Studies involving neurotypical children included Zhang et al. 21 and Beveridge et al. 19 Studies focusing on children with disabilities included Taherian et al., 15 Alcaide-Aguirre et al., 23 Warschausky et al., 24 Jadavji et al., 25 and Huggins et al. 26 The functional abilities of participants with CP were commonly described using the Gross Motor Function Classification System (GMFCS), with most participants classified as levels IV or V, indicating significant motor support needs.
The activities children participated in were diverse. Huggins et al. 26 summarized challenges seen in three studies when children used a P300-based BCI-facilitated cognitive assessment, the Peabody Picture Vocabulary Test - Version 4. 27 Children used this system in Alcaide-Aguirre et al. 23 and Warschausky et al. 24 Several studies used the Emotiv MI-BCI for various play activities, such as revealing puzzle pieces, controlling a remote-controlled car and a computer cursor, 21 and accessing computer games, robots, iPads, and environment control. Children also did spelling using a P300 based BCI. 25 Beveridge et al. 19 examined the use of mVEPs, which are elicited when an individual focuses their attention on a moving display item, to control a car race computer game. The main findings regarding cognition relevant to this review were needing customized systems to meet needs and motivation of children, using pictorial displays for those with limited or emerging literacy skills, and suggesting that children have access to BCI as early as possible.
Cognitive areas relevant for BCI
Attention was the primary cognitive area mentioned in the reviewed studies, highlighting its essential role in BCI operation. Other aspects, such as concentration and processing speed were also noted as influencing performance, although they received comparatively less emphasis. Motivation and fatigue, while not classified as cognitive domains, were frequently referenced as psychological or physiological factors that can impact BCI performance by modulating performance. Each of these cognitive areas is presented in greater detail below.
Attention and concentration
Attention is a critical cognitive factor in BCI operation, particularly in paradigms like P300, which require users to selectively focus on specific stimuli to generate detectable brain responses. To support attentional engagement and align users with the timing of stimulus presentation, strategies like “counting the flashes” are commonly used. 26 However, this approach may be challenging for children who have difficulty with mental counting. 26
Generating reliable P300 signals requires users to identify and monitor specific stimuli while sustaining attention throughout the task. Warschausky et al. 24 observed attention difficulties among their participants and cited Thompson et al., 28 who reported that such difficulties can negatively affect BCI signal detection. Huggins et al. 26 further emphasized the importance of task comprehension and sustained focus during lengthy sessions. Prolonged setup and calibration periods, often exceeding an hour, can surpass a child’s attention span, especially when the stimuli are not inherently engaging. Alcaide-Aguirre et al. 23 observed that some children interacted with the BCI for only a few seconds before becoming distracted or engaging with their parents. Children struggling with attention and interest frequently reported feelings of fatigue, boredom, and a desire to stop the test.
Zhang et al. 21 reported that younger children face additional challenges in sustaining attention during BCI tasks, adolescents often experience performance declines during prolonged sessions, possibly due to fatigue or waning focus. These trends align with findings that adults tend to perform better than children in tasks requiring prolonged visual processing and sustained attention. 19
Finally, Taherian et al. 15 observed that factors such as physical design limitations of devices like the Emotiv EPOC for individuals with disabilities, unengaging or ineffective software design, and physical illness may negatively impact users’ ability to stay concentrated throughout the BCI task, resulting in an inability to effectively use BCI.
Processing speed
Individuals with slower processing speeds may struggle with the timing and pace of BCI tasks. 26 Lower processing speed can be especially problematic in synchronous BCI systems where the timing of stimulus presentation and response detection is fixed. Thus, BCI systems may require adjustments to stimulus duration, where the system waits for user confirmation of a predicted target rather than automatically proceeding to the next target selection.
Motivation and engagement
Multiple sources emphasized the role of motivation in BCI performance. Individuals who are motivated and engaged in the task are more likely to perform well. For instance, Jadavji et al. 25 observed that participants showed greater engagement during MI tasks for play compared to P300 spelling tasks, potentially due to the more engaging feedback and shorter training involved. Similarly, Taherian et al. 15 noted that participant motivation and concentration significantly influenced the user performance.
Zhang et al. 21 further noted that children achieved higher performance on a car control task compared to a cursor control task, potentially due to increased engagement when interacting with a visually stimulating, dynamic toy rather than a static, less engaging cursor. Moreover, they found that the GO strategy that they asked children to use worked better than the classic MI task of imagining moving a limb. In the GO strategy, children directly imagined the car (or cursor) moving. 21 These findings underscore the importance of task design in influencing user motivation and performance. Intuitive, engaging, and age-appropriate tasks are essential to optimize BCI effectiveness.
Fatigue
Both mental and physical fatigue can impact the usability and performance of BCIs. In the study evaluating the Emotiv MI/VI -based BCI, participants reported experiencing mental fatigue during the final 10 min of their sessions. 21 Prolonged setup and calibration periods may contribute to physical fatigue. For instance, children with CP perceived the BCI-facilitated PPVT-IV test as having a higher physical demand compared to the standard version, despite the lack of required physical movement. This was attributed to fatigue from prolonged sitting during setup. 23 Flashing visual stimuli used in VEP-based BCIs can also induce visual fatigue with extended use. 19 Fatigue in its various forms may impact cognitive functions necessary for BCI performance, including attention and processing speed.
Additional considerations
Neuroimaging was recommended to “confirm diagnosis, absence of additional neuropathology, and presence of fundamental neuroanatomy consistent with the reported level of cognitive potential and potential for EEG-based BCI applications.” 25 In children with cerebral palsy, neuroimaging is particularly important, as studies have shown abnormal brain anatomy in 80%–90% of cases. 28 These findings are relevant to BCI research, especially when considering neurodevelopmental differences that may influence electrode placement. This underscores the dual importance of neuroimaging in both adapting BCI systems to individual neuroanatomy and understanding the cognitive challenges faced by children with neurodevelopmental conditions.
Hardware used
The reviewed studies utilized a range of non-invasive EEG systems for BCI signal acquisition. The Emotiv EPOC/EPOC was employed in studies such as Taherian et al., 15 Zhang et al., 21 and Jadavji et al. 25 g.Tec systems, known for their high-resolution signal acquisition, were utilized by Beveridge et al. 19 High-resolution systems, such as 32-location gel-based EEG caps, were used in studies like Alcaide-Aguirre et al., 23 Warschausky et al., 24 and Huggins et al. 26 Additionally, Jadavji et al. 25 used specialized systems such as the g.tec mindBEAGLE to measure vibrotactile and auditory evoked potentials, potentially expanding the scope of BCI applications to individuals with visual impairments.
BCI paradigm
The studies reviewed utilized three primary brain signal paradigms across their research. MI was employed by Taherian et al., 15 Zhang et al. 21 and Jadavji et al. 25 P300 event-related potentials, a widely adopted paradigm, were utilized in multiple studies, including Alcaide-Aguirre et al., 23 Warschausky et al., 24 and Huggins et al. 26 Motion-onset visual evoked potentials (mVEPs) were implemented in neurogaming applications, particularly in the study by Beveridge et al. 19 Collectively, these paradigms reflect the diverse methodologies employed across the seven studies to explore the capabilities and applications of BCIs.
Discussion
The goal of this scoping review was to examine cognitive factors associated with successful BCI use in pediatric populations. Drawing on developmental theory and prior research in adult BCI applications, it was anticipated that cognitive domains such as attention, concentration, and working memory would emerge as particularly relevant. This review sought to systematically map existing evidence in this area and highlight knowledge gaps to inform future research and system development. After the screening process, only seven studies met the inclusion criteria, reflecting the limited research available on this topic. Despite this, the included studies provided valuable insights into the cognitive factors influencing BCI use in children, particularly attention, concentration, and processing speed. However, the small number of studies emphasizes the need for further research to deepen our understanding of these factors and their impact on pediatric BCI applications.
This review highlights the role of attention in BCI research, particularly in paradigms like P30023,26 where sustained focus is essential for generating reliable signals. Among the cognitive factors considered, attention and its modalities were the most mentioned, reflecting its central importance in BCI use. While this focus is expected, it also highlights a broader gap in research addressing other cognitive domains, such as working memory, processing speed, or executive functions, particularly in pediatric populations.
The study by Huggins et al. 26 stands out for directly addressing the cognitive demands of BCI use, offering valuable insights into the relationships between task comprehension, attention, processing speed and BCI performance. In contrast, the other studies mentioned cognitive requirements as secondary observations rather than primary objectives. This reflects the early stage of BCI research in pediatric populations and underscores the need for more focused and intentional investigations into cognitive factors affecting BCI use in children.
In adult populations, research shows that BCI performance is strongly influenced by cognitive variables such as working memory, attention, and general intelligence.7,9 For instance, Sprague et al. 9 found that working memory and general intelligence are related to BCI performance, with higher working memory capacity associated with greater accuracy. Furthermore, Carelli et al. 7 emphasized that cognitive load and attentional resources significantly modulate BCI usability and performance.
Although studies in adult populations provide a strong foundation, translating these findings to pediatric populations requires careful consideration of developmental differences. Children’s executive functions, attention span, and working memory capacity are still maturing, in line with the ongoing anatomical and functional development of the prefrontal and parietal cortices throughout childhood and adolescence. These maturational processes may contribute to greater variability and distinct cognitive performance compared to adults. Tasks and paradigms designed for adults, as noted by Beveridge et al., 19 may not align with the cognitive abilities or interests of younger users. For example, researchers such as Orlandi et al. 13 have questioned the feasibility of MI tasks for children with congenital movement conditions, noting that those who have never functionally moved their limbs may struggle to understand or perform these tasks. 29
Thus, while overlapping cognitive factors (e.g., attention) are relevant across age groups, the developmental stage introduces unique considerations that would impact pediatric BCI application. To address these challenges, it is essential to develop intuitive, engaging, and age-appropriate tasks, complemented by adaptive feedback mechanisms.26,30 These measures are necessary for improving usability and ensuring that BCI systems are effectively tailored to the needs of pediatric populations.
Moreover, although cognitive factors such as attention, memory, and concentration are relevant for effective BCI use, not all influencing factors are strictly cognitive. Elements like motivation, engagement,8,31 and fatigue32,33 also play a significant role in BCI implementation.
Neuroimaging is crucial for advancing BCI research, particularly when accessible to clinicians. For children with CP, it provides vital insights into neuroanatomy, helping to guide electrode placement and tailor systems to individual needs. Knowing the significant neuroanatomical differences in children with CP, as reported by Korzeniewski et al., 28 is essential during the initial stages of BCI implementation. This knowledge can also aid in assessing cognitive potential, optimizing residual skills, identifying areas for targeted training, and exploring alternative strategies, ensuring BCIs effectively address the unique challenges of children with CP.
Our results extend this understanding to children with CP, emphasizing the relevance of these factors in a pediatric context. This distinction underlines the importance of considering age-specific challenges and responses when designing and implementing BCI systems.
Clinical and technical implications
These findings have important practical implications for the future development of pediatric BCI systems. Clinically, considering that attention, concentration, and processing speed were frequently identified as relevant cognitive abilities associated with BCI use, and motivation, engagement and fatigue were also reported as influential factors, pediatric users may benefit from a progressive familiarization process. This approach could include early exploration of the equipment, simple attention-based games, and gradually more complex tasks. This not only helps manage cognitive load and reduce fatigue but also creates optimal conditions for neuroplasticity. 34 As children’s brains are especially receptive to experience-driven change, this process might be particularly effective in enhancing both BCI control and broader cognitive development. Additionally, neuroimaging could play a crucial role in assessing the potential for EEG-based BCI applications, particularly in pediatric populations.
From a technical perspective, intuitive, visually engaging, and developmentally appropriate interfaces can help children focus their cognitive resources on task performance rather than system navigation. Additionally, systems should account for variations in processing speed by allowing sufficient time for users to perceive, process, and respond to stimuli. Incorporating adaptive difficulty, real-time feedback, and gamified elements may also support sustained attention and engagement while reducing the risk of cognitive overload and fatigue during long sessions, as stated by Pitt et al. 35
Limitations and future work
The current review has several limitations that should be acknowledged. First, it was restricted to English-language articles, potentially excluding relevant studies in other languages. Second, this review focused on attention, concentration, and processing speed, which represent only a subset of the broader cognitive factors that may influence BCI use. Cognitive functioning is a broad and multifaceted area, and this review may not encompass all aspects, particularly those less frequently reported or indirectly studied. As such, the findings do not fully capture the complexity of cognitive requirements for pediatric BCI use. Third, variations in participants’ demographics, BCI paradigms, and hardware across studies limited our ability to draw clear conclusions or generalize findings. Additionally, the limited number of included studies further restricts the generalizability of the results.
Future research should prioritize exploring cognitive factors across specific populations, hardware, and paradigms. These approaches will help advance the field by addressing gaps in knowledge and refining BCIs for pediatric populations with diverse needs.
Conclusion
This scoping review highlights the limited but growing body of evidence regarding the cognitive and psychological factors involved in pediatric BCI use. Attention, concentration, and processing speed consistently emerged as relevant cognitive demands, while motivation, engagement, and fatigue were also frequently mentioned as modulators of performance. However, these factors were not typically the primary focus of the studies reviewed, and their impact was often reported anecdotally rather than assessed. In contrast, adult BCI research has more explicitly examined the role of psychological and cognitive variables, such as working memory and motivation, within specific paradigms. It is recommended that future pediatric studies adopt a similarly focused approach, assessing these factors to better understand how they contribute to BCI performance in children.
Recommendations for the future use and development of pediatric BCI systems include using a progressive familiarization training process and designing engaging, adaptive, and developmentally appropriate interfaces in order to enhance readiness, motivation, and reduce fatigue. Collaborative efforts among clinical and technical professions are essential to create BCI systems that are not only technically feasible but also optimized for diverse cognitive profiles and needs of pediatric users.
Footnotes
Author Contributions
Conception: JRO and KA.
Performance of work: JRO and KA.
Interpretation or analysis of data: JRO, KA, and AL.
Preparation of the manuscript: JRO and KA.
Revision for important intellectual content: JRO, KA, and AL.
Supervision: KA and AL.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Johana Rios Ortegon was supported by the Natural Sciences and Engineering Research Council of Canada Collaborative Research And Training Experience in Sensory Motor Rehabilitative Technology (NSERC SMART-CREATE) Program at the University of Alberta.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.