
Abstract
Social drivers of health (SDOH) play a critical role in influencing health outcomes, including those related to cognitive dysfunction in patients with cirrhosis. Cognitive dysfunction, which can significantly impact the quality of life and health outcomes in patients with cirrhosis, may be influenced by various SDOH factors. This scoping review aims to synthesize current evidence on the association between SDOH and cognition among patients with cirrhosis. A systematic search of the literature was conducted from inception through March 2024 using PubMed, Cochrane Library, and Embase databases. Studies that examined the relationship between SDOH and cognition, as measured by neuropsychological tests, were identified. SDOH were categorized into the five Healthy People 2030 SDOH domains. A total of 31 studies were included in the review; however, many of the studies did not primarily focus on examining the relationship between SDOH and cognition. Cognition was primarily assessed using the Psychometric Hepatic Encephalopathy Score. Education was the most frequently investigated SDOH, followed by employment. Higher levels of education and employment were generally associated with better cognitive performance. The SDOH domains of social and community context and healthcare access and quality were not addressed in the included studies. This review highlights the potential link between SDOH and cognition among patients with cirrhosis but also reveals that existing research is limited, especially beyond education. Future research should address these understudied SDOH factors to inform strategies to identify at-risk patients and improve health outcomes in patients with cirrhosis.
Introduction
Cirrhosis is the progressive, often irreversible scarring of hepatic tissue that represents the final stage of chronic liver disease (Ginès et al., 2021). Although it is preventable through early detection and effective management of underlying liver diseases, the prevalence of cirrhosis in the United States (US) is 2.6% (Younossi et al., 2025). The primary causes of cirrhosis vary geographically, but most commonly include chronic alcohol consumption, chronic viral hepatitis (Hepatitis B and C), and metabolic dysfunction-associated steatotic liver disease. The clinical course of cirrhosis is broadly classified into two stages: compensated cirrhosis, wherein hepatic function is impaired yet preserved sufficiently to maintain essential physiological processes; and decompensated cirrhosis, marked by significant hepatic dysfunction and complications such as variceal hemorrhage, ascites, and hepatic encephalopathy (HE; Garcia-Tsao et al., 2010). In both stages, impaired liver function leads to the systemic accumulation of neurotoxins such as ammonia, which can disrupt brain function and contribute to cognitive dysfunction (Butterworth, 2003).
Cognition refers to any mental or thinking processes, including perceiving, remembering, and applying knowledge (APA Dictionary of Psychology, 2018). It encompasses several interrelated domains, including attention (sustaining focus while ignoring distractions), executive function (planning, problem solving, cognitive flexibility, and information manipulation), learning and memory (storing and retrieving factual and procedural knowledge), visuospatial abilities (perceiving and navigating spatial environments), and language (understanding and producing verbal communication) (Harvey, 2019; Possin, 2010; Siddiqui et al., 2023). Impairments in these domains can reduce independence in daily activities and impair judgment, ultimately diminishing the quality of life and contributing to poorer health outcomes (Stites et al., 2018). Cognition is commonly evaluated using neuropsychological tests that measure global cognition or specific cognitive domains, along with standardized screening tools such as the Mini-Mental State Examination.
Approximately 40% of patients with cirrhosis exhibit cognitive dysfunction (Lv et al., 2023), although it widely varies across studies, particularly due to different neuropsychological tests used. Cognitive dysfunction in this population could be a symptom of hepatic encephalopathy, a brain dysfunction characterized by neuropsychiatric abnormalities ranging from minimal HE (MHE), which involves subtle cognitive changes without clinical symptoms, to overt HE (Vilstrup et al., 2014). While treatments are available, MHE remains challenging to diagnose clinically and can recur, increasing the risk of progression to overt HE (Bajaj et al., 2009). HE can particularly impair cognitive domains of attention, visuospatial abilities, and executive function (García-García et al., 2018; Nardelli et al., 2017; Weissenborn et al., 2001). Beyond HE, cognitive dysfunction in cirrhosis could also be related to neurodegeneration or cerebrovascular dysfunction induced by metabolic and vascular comorbidities (Kjærgaard et al., 2021). Individuals with cognitive dysfunction tend to report poorer daily functioning (Bajaj et al., 2007) and quality of life (Bajaj et al., 2020). They also have up to a twofold higher risk of experiencing hospitalizations due to overt HE (Bajaj et al., 2007), falls (Soriano et al., 2012), and mortality (Kim et al., 2019; Tapper et al., 2021) compared to those without cognitive dysfunction.
Unfavorable social drivers of health (SDOH), including low income, limited education, lack of healthcare access, and neighborhood deprivation, can influence the onset and progression of cirrhosis and associated cognitive dysfunction. Patients with lower socioeconomic status or unemployment at diagnosis are more likely to present with advanced liver disease and experience poorer survival (Koutny et al., 2023; Stroffolini et al., 2020; Vaz et al., 2020). Cirrhosis-related mortality is also significantly higher in rural than urban areas, potentially reflecting limited access to specialty care (Ha et al., 2022). Stigma associated with alcohol-related liver disease can also delay care-seeking, further exacerbating disease progression and outcomes (Vaughn-Sandler et al., 2014). Moreover, low socioeconomic status is associated with higher rates of HE and HE-related hospitalizations (Helzberg et al., 2021), partly due to challenges in affording treatment and receiving timely specialist referrals (Tapper et al., 2022).
Clarifying the role of SDOH in cognitive dysfunction among patients with cirrhosis may support future strategies to identify those at risk. Although prior studies have examined SDOH in relation to cognition, a comprehensive understanding of these relationships remains limited. The purpose of this scoping review was to identify the SDOH factors studied in relation to cognition and to synthesize available evidence on their associations among patients with cirrhosis. Findings may guide future research and highlight key gaps that need further investigation.
Methods
Study Design
This scoping review followed the five-stage methodological framework developed by Arksey and O’Malley (2005) to guide the review process. These stages included the following: (a) identifying the research question, (b) identifying relevant studies, (c) study selection, (d) charting the data, and (e) collating, summarizing, and reporting the results. This structured approach ensured transparency and consistency throughout study identification, selection, and data synthesis. As recommended, we incorporated consultation with AK and FDG, which contributed to the refinement and validation of our findings. The review also followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines of Scoping Reviews to guide reporting (Tricco et al., 2018).
Search Strategy
The search strategy was developed in consultation with a health sciences librarian who has expertise in systematic literature searches. Literature searches were conducted in March 2024 using PubMed, Cochrane Library, and Embase. The PubMed search strategy, with no filters on the year of publication, was:
("Cognition"[Mesh] OR “Hepatic Encephalopathy”[Mesh] OR ”Cognitive Dysfunction"[Mesh] OR “Attention“[Mesh] OR “Executive Function”[Mesh] OR “Learning”[Mesh] OR “Orientation”[Mesh] OR “neuropsychol*”[Mesh] OR “neuropsychol*”[tiab] OR ”cognitive" [tiab] OR "cognition" [tiab]) AND ("End Stage Liver Disease"[Mesh] OR "Liver Cirrhosis"[Mesh] OR "Liver Cirrhosis, Biliary"[Mesh] OR "Liver Cirrhosis, Alcoholic"[Mesh] OR "liver failure" [tiab] OR "hepatic failure" [tiab] OR "cirrhotic" [tiab] OR "cirrhosis" [tiab] OR "liver dysfunction" [tiab]) AND ("Social Determinants of Health"[Mesh] OR "Health Equity"[Mesh] OR “Cognitive Reserve”[Mesh] OR "Socioeconomic Factors"[Mesh] OR "Health Disparate Minority and Vulnerable Populations"[Mesh] OR "Health Inequities"[Mesh] OR "socioeconomic" [tiab] OR "disparit*" [tiab] OR "social determinants" [tiab] OR “Education”[tiab] OR “Employment”[tiab] OR “race”[tiab] OR “enthnicity”[tiab] OR “Income”[tiab] OR “job”[tiab] OR “housing”[tiab] OR “health insurance”[tiab] OR “social support”[tiab]) NOT (animals [mh] NOT humans [mh])
The PubMed strategy was customized for other databases to acquire relevant search results. We exported all search results from the three databases and imported them into Rayyan, a web-based, user-friendly tool that facilitates collaboration of reviewers and expedites the initial screening of abstract and title for literature reviews (Ouzzani et al., 2016).
Inclusion and Exclusion Criteria
Studies were included if the target population included patients with cirrhosis aged 18 years or older, cognition was assessed using a validated neuropsychological test, and the relationship between SDOH and neuropsychological test results was examined. Studies were excluded if they (a) were review papers, case reports, protocols, editorials, commentaries, or book chapters, (b) only included patients with non-cirrhotic liver diseases, or (c) did not specifically report the relationship between SDOH and neuropsychological test results. After removing duplicate articles across the three databases, two reviewers independently assessed the titles and abstracts of studies during the initial screening, followed by a full-text screening of the included articles to determine whether they met the inclusion criteria. If there were disagreements about eligibility, the last author (DK) was consulted for discussion until consensus was reached.
Quality of Studies Assessment
We critically appraised the quality of the included studies using the tools of the Joanna Briggs Institute (JBI) (Aromataris et al., 2024) because they offer a comprehensive range of tools for appraising different study designs. Two reviewers independently evaluated all included studies for methodological quality and for measures taken by the studies to address bias. If there were disagreements about the quality, the last author (DK) was consulted for discussion until consensus was reached.
Data Synthesis
One reviewer designed a data-charting template in an Excel spreadsheet to identify the relevant variables for extraction. Two reviewers independently charted the data. Each reviewer charted half of the studies, then cross-reviewed each other’s data-charting forms, discussed their findings, and refined the form through an iterative process. Extracted data included study purpose, sample, design, location, tools used to assess cognition, SDOH variables, measures of SDOH, and findings on the relationship between SDOH and cognition. SDOH variables were categorized into the five Healthy People 2030 domains: economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context (Healthy People 2030, n.d.).
Results
Study Selection
The initial database search yielded 3,585 articles. After de-duplication and full-text screening of 175 articles, 31 articles were included for data extraction and synthesis (Figure 1). All studies met the methodological quality criteria of JBI critical appraisal tools (Table 1).
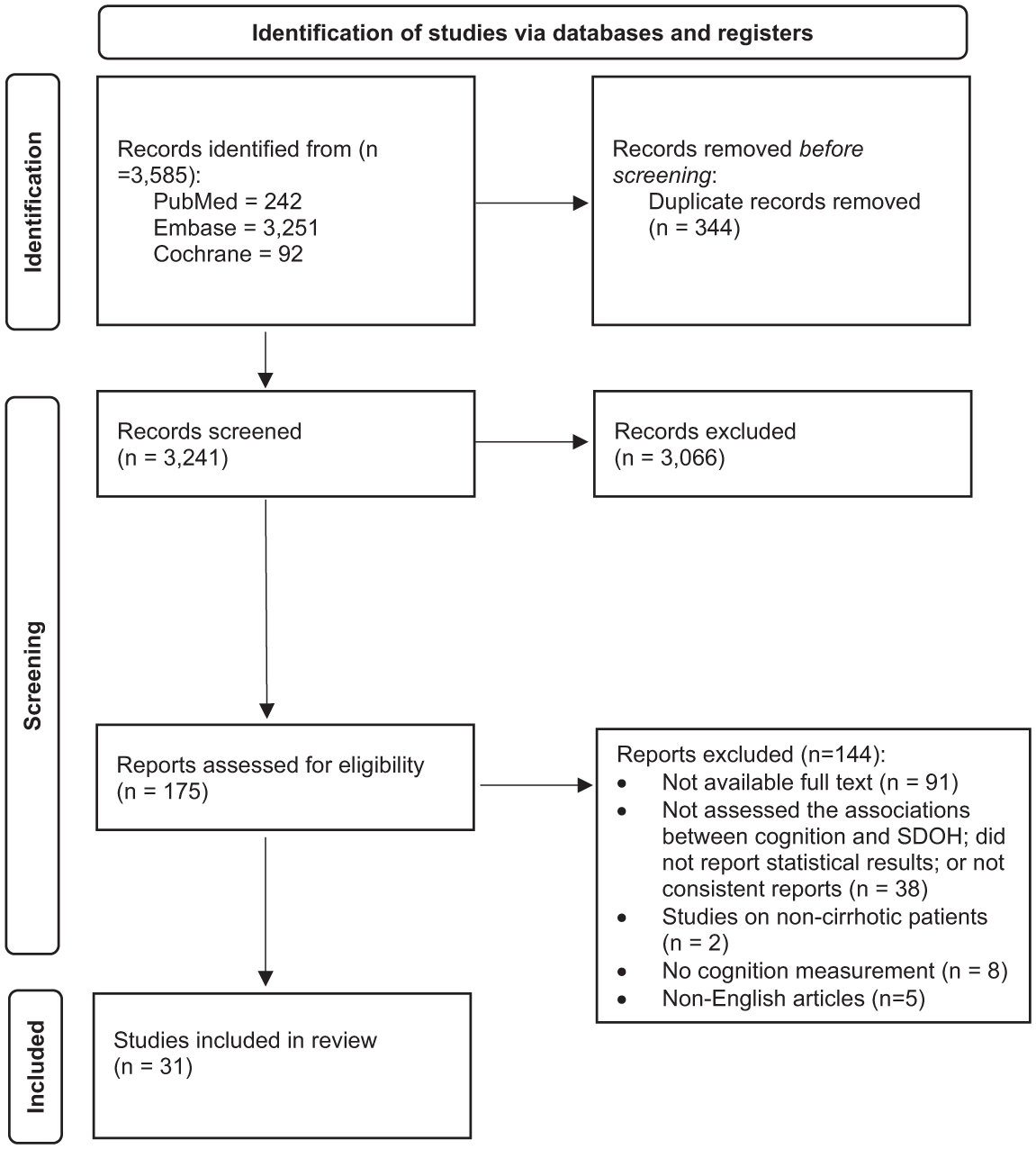
Flow diagram of study selection.
Quality Assessment of the Included Studies.
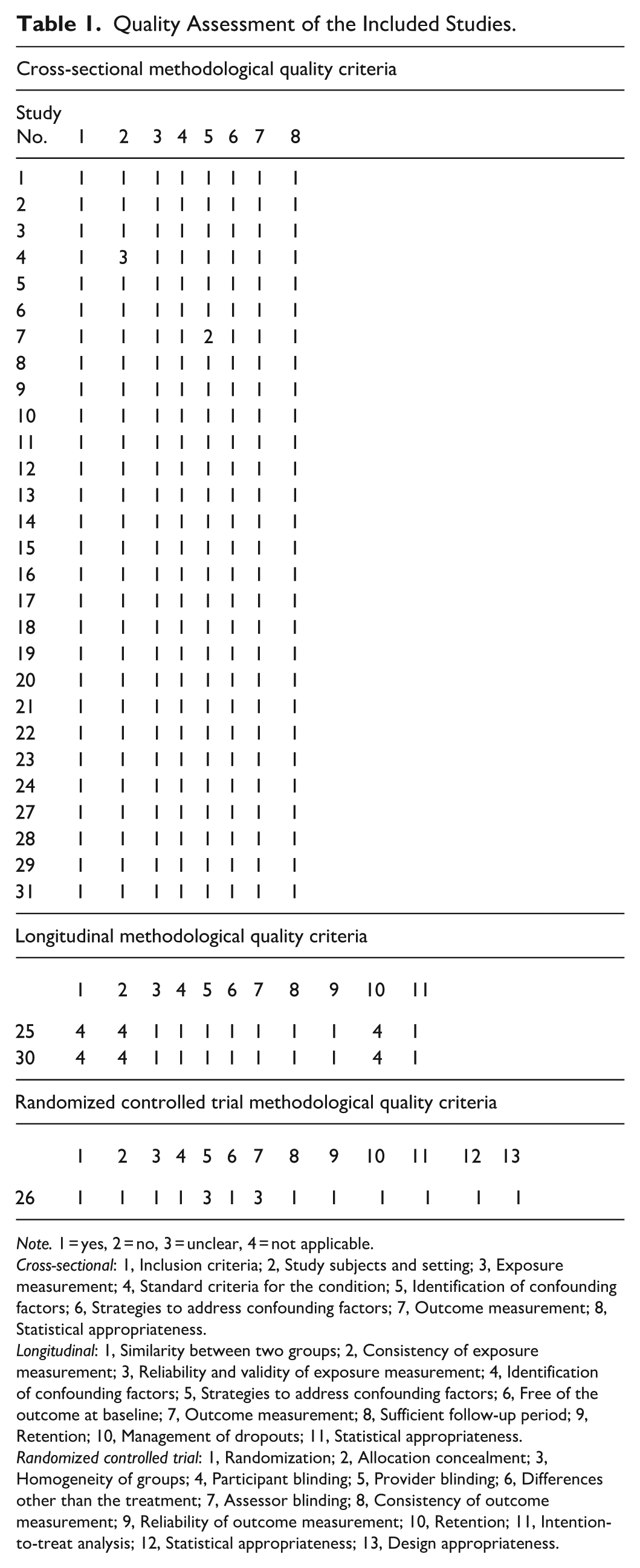
Note. 1 = yes, 2 = no, 3 = unclear, 4 = not applicable.
Cross-sectional: 1, Inclusion criteria; 2, Study subjects and setting; 3, Exposure measurement; 4, Standard criteria for the condition; 5, Identification of confounding factors; 6, Strategies to address confounding factors; 7, Outcome measurement; 8, Statistical appropriateness.
Longitudinal: 1, Similarity between two groups; 2, Consistency of exposure measurement; 3, Reliability and validity of exposure measurement; 4, Identification of confounding factors; 5, Strategies to address confounding factors; 6, Free of the outcome at baseline; 7, Outcome measurement; 8, Sufficient follow-up period; 9, Retention; 10, Management of dropouts; 11, Statistical appropriateness.
Randomized controlled trial: 1, Randomization; 2, Allocation concealment; 3, Homogeneity of groups; 4, Participant blinding; 5, Provider blinding; 6, Differences other than the treatment; 7, Assessor blinding; 8, Consistency of outcome measurement; 9, Reliability of outcome measurement; 10, Retention; 11, Intention-to-treat analysis; 12, Statistical appropriateness; 13, Design appropriateness.
Study Characteristics
The characteristics of the included studies are summarized in Table 2. Most studies were cross-sectional (n = 28, 90%) and published in the past 10 years (n = 20, 64%). Eight studies (26%) focused on identifying factors, including SDOH, that influence cognition, while others primarily aimed to establish normative values for neuropsychological tests (n = 10, 32%) or to estimate the prevalence of MHE in cirrhosis (n = 4, 13%). Studies were most commonly conducted in the United States (n = 7, 22%) and China (n = 7, 22%), with a few studies from Poland and Mexico (each n = 2, 6%) and one international multicenter study across the United States and Italy (#31). All studies reported a mean or median participant age of approximately 50 years or older. Education was reported in 28 studies (90%), with a mean or median of 14 years or less.
Summary of Included Studies.
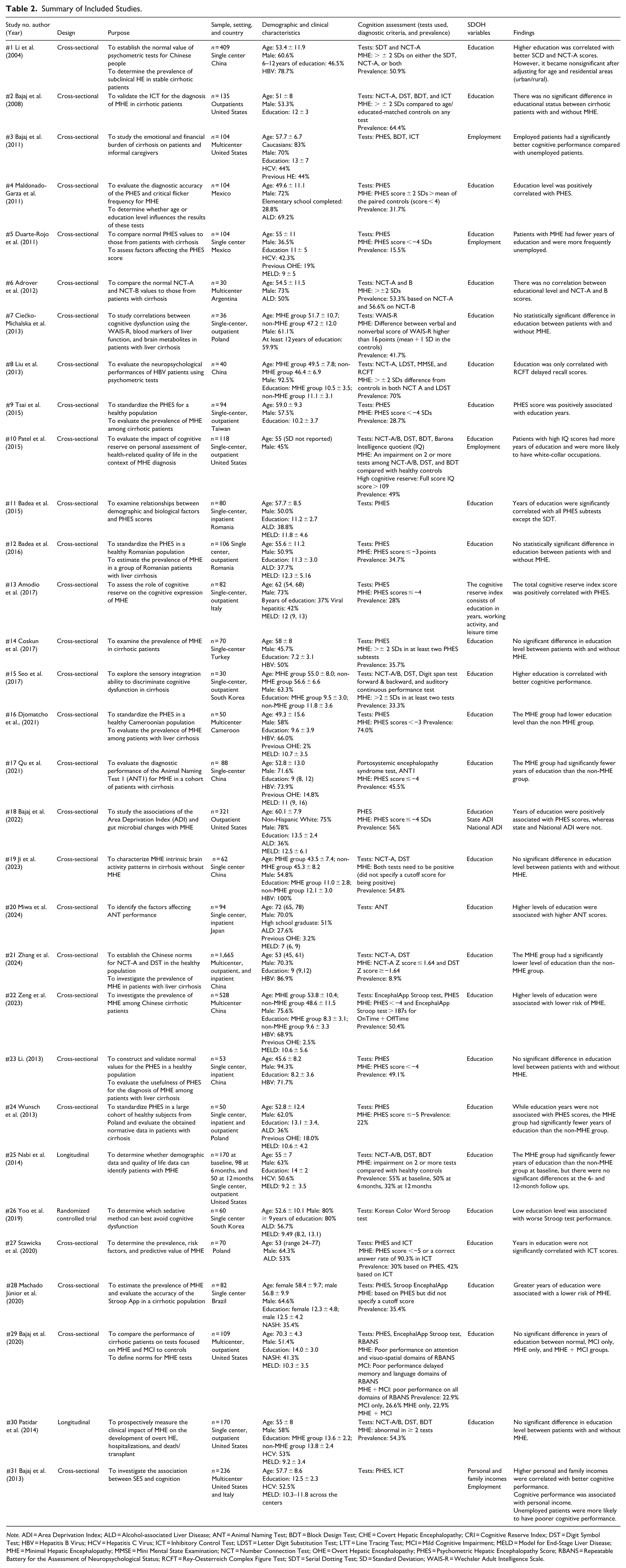
Note. ADI = Area Deprivation Index; ALD = Alcohol-associated Liver Disease; ANT = Animal Naming Test; BDT = Block Design Test; CHE = Covert Hepatic Encephalopathy; CRI = Cognitive Reserve Index; DST = Digit Symbol Test; HBV = Hepatitis B Virus; HCV = Hepatitis C Virus; ICT = Inhibitory Control Test; LDST = Letter Digit Substitution Test; LTT = Line Tracing Test; MCI = Mild Cognitive Impairment; MELD = Model for End-Stage Liver Disease; MHE = Minimal Hepatic Encephalopathy; MMSE = Mini Mental State Examination; NCT = Number Connection Test; OHE = Overt Hepatic Encephalopathy; PHES = Psychometric Hepatic Encephalopathy Score; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; RCFT = Rey-Oesterreich Complex Figure Test; SDT = Serial Dotting Test; SD = Standard Deviation; WAIS-R = Wechsler Adult Intelligence Scale.
Cognition
Cognitive dysfunction was considered a component of HE in 30 studies (97%), with MHE identified solely based on abnormal neuropsychological test scores. Many studies (n = 24, 77%) did not specify whether they intended to assess global cognition or domain-specific cognition. The neuropsychological tests used and their corresponding cognitive domains, based on descriptions provided in the articles or identified from the literature, are summarized in Table 3 (George et al., 2022; Lezak et al., 2012; Siddiqui et al., 2023). Most tests primarily assess attention, executive function, and visuospatial abilities, domains commonly impaired in HE. The Psychometric Hepatic Encephalopathy Score (PHES), which includes five subtests (digit symbol test [DST], number connection test-A [NCT-A], number connection test-B [NCT-B], serial dotting test [SDT], and line tracing test [LTT]), was the most frequently used measure (n = 18, 58%). Half (n = 16, 51%) of the studies used more than one neuropsychological test. Reported MHE prevalence varied widely, ranging from 8.9% to 74%.
Neuropsychological Tests and Cognitive Domains Used in Assessment in Included Studies.
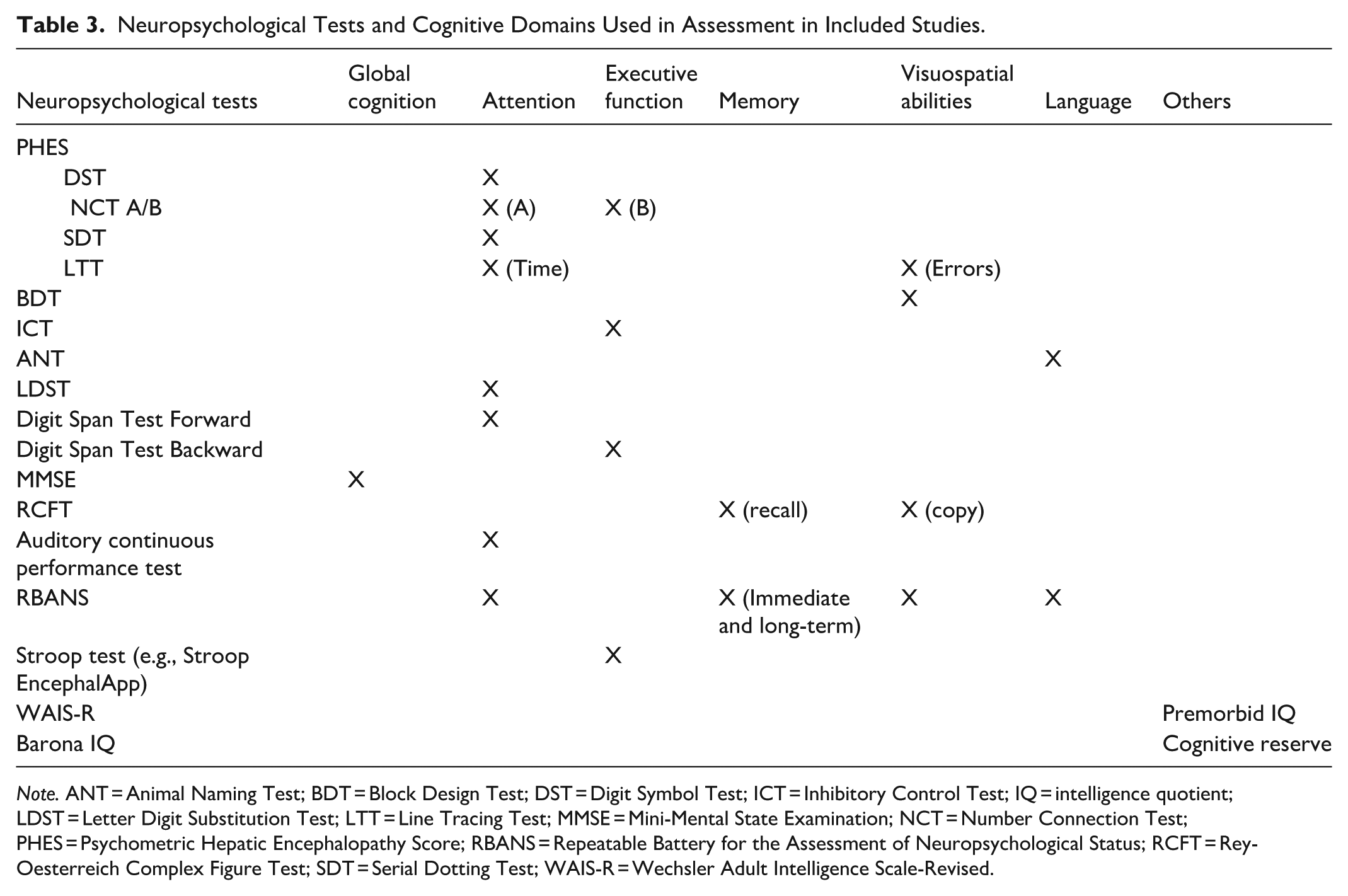
Note. ANT = Animal Naming Test; BDT = Block Design Test; DST = Digit Symbol Test; ICT = Inhibitory Control Test; IQ = intelligence quotient; LDST = Letter Digit Substitution Test; LTT = Line Tracing Test; MMSE = Mini-Mental State Examination; NCT = Number Connection Test; PHES = Psychometric Hepatic Encephalopathy Score; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; RCFT = Rey-Oesterreich Complex Figure Test; SDT = Serial Dotting Test; WAIS-R = Wechsler Adult Intelligence Scale-Revised.
Social Drivers of Health
Education was the most frequently examined SDOH (n = 28, 90%), followed by employment (n = 4, 13%), income (#31), and neighborhood socioeconomic status (#18). Most studies focused on a single SDOH factor (n = 26, 83%). The cognitive reserve index, which evaluates cognitive reserve through a combination of education, employment, and leisure time, was assessed in one study (#13).
According to the Healthy People 2030 SDOH domains, education falls under the education access and quality domain, employment and income under the economic stability domain, and socioeconomic conditions of the neighborhood under the neighborhood and built environment domain. The cognitive reserve index spans multiple domains, including education access and quality, economic stability, and social and community context. None of the SDOH variables studied in the included articles fell under the healthcare access and quality domain.
Relationship Between SDOH and Cognition
The majority of studies (n = 23, 74%) did not primarily aim to investigate associations between SDOH and cognition. Of the 28 studies (90%) that examined education in relation to cognition, 18 reported significant associations, indicating that higher levels of education are associated with better neuropsychological test scores. For example, two studies (#4, #9) reported bivariate correlations of .33 (p = .001) and .32, (p = .002), respectively, while two others (#22, #28) reported a reduced risk of MHE, with odds ratios of .89 (95% CI [.83, .95]) and .88 ([.78, .99]), respectively.
Six studies (19%) analyzed SDOH factors other than education. All three studies (#3, #5, and #10) that assessed employment reported a significant positive correlation between employment status and cognition, indicating that employed patients were more likely to have better neuropsychological test scores. Higher personal and family incomes were associated with better neuropsychological test scores (#31). The cognitive reserve index also showed a significant positive relationship (r = .35, p < .01) with cognition (#13). However, the association between neighborhood socioeconomic status, as measured by the Area Deprivation Index, and neuropsychological test scores was not significant (#18).
Discussion
This scoping review synthesized findings from 31 studies on the relationship between SDOH and cognition among patients with cirrhosis. While many studies did not examine this relationship as their primary aim, they consistently demonstrated associations between education, employment, and cognition. Current literature has predominantly focused on the SDOH domain of education access and quality, while limited evidence is available in the domains of economic stability, neighborhood and built environment, healthcare access and quality, and social and community context. These gaps highlight the need for further research to comprehensively understand how various SDOH influence cognition in this population.
The associations between education, employment, and cognition among patients with cirrhosis are consistent with evidence from the general population. Higher educational attainment and employment, particularly in intellectually demanding occupations, are associated with better cognitive performance and lower risk of cognitive dysfunction (Hughes & Ganguli, 2009; Livingston et al., 2020; Richards et al., 2019). These associations are often attributed to cognitive reserve, the brain’s ability to maintain functionality despite brain aging, pathology, or damage (Reserve, Resilience and Protective Factors PIA Empirical Definitions and Conceptual Frameworks Workgroup, 2020). Cognitive reserve varies based on educational and occupational experiences and cognitively enriching activities, such as physical exercise and social engagement.
In patients with cirrhosis, variation in education and employment may contribute to differences in cognition, potentially through their influence on healthcare access and disease progression. Those with lower education or who are unemployed at diagnosis have been shown to present with more advanced liver disease and experience poorer survival outcomes (Koutny et al., 2023; Stroffolini et al., 2020; Vaz et al., 2020). Employment is often limited in this population due to disability, yet individuals with a college degree have greater odds of remaining employed (Stepanova et al., 2017). Education and employment may also be linked to wealth, which influences access to health care (Zajacova & Lawrence, 2018). Limited financial resources can delay or prevent necessary treatments (Zajacova & Lawrence, 2018), potentially worsening cirrhosis prognosis (Nguyen et al., 2024) and increasing the risk of cognitive dysfunction (Acharya et al., 2021; Zeng et al., 2023). Notably, one study in this review found that higher cognitive reserve, as measured by education, employment, and intellectually and socially engaging leisure activities, was associated with better neuropsychological performance (Amodio et al., 2017).
However, the influence of SDOH on cognition extends beyond education and employment (Livingston et al., 2020; Majoka & Schimming, 2021). SDOH factors, such as low income, food insecurity, social isolation, and living in low-resource neighborhoods, are linked to chronic stress and comorbid conditions such as diabetes and hypertension, each a known risk factor for cognitive dysfunction (Livingston et al., 2020; Majoka & Schimming, 2021). These SDOH factors are interconnected and collectively impact health (Bronfenbrenner, 1977; Dahlgren & Whitehead, 2021). Despite this, few studies in this review examined SDOH beyond education. Most studies were limited to describing demographic characteristics of patients with cognitive dysfunction, rather than investigating broader SDOH factors. Identifying underexplored SDOH factors and integrating them with clinical factors associated with cognitive dysfunction in cirrhosis, such as the Model for End-Stage Liver Disease score and comorbidity (Acharya et al., 2021; Zeng et al., 2023), could inform the development of clinical tools to better screen and prioritize at-risk patients. Expanding the scope of future studies to include a broader range of SDOH may ultimately enhance our understanding of how these factors contribute to cognitive dysfunction in cirrhosis.
Although SDOH are increasingly recognized as key contributors to health in the US, only 23% of the studies in this review were conducted in US populations. Certain racial and ethnic groups may be more likely to experience adverse SDOH, such as living in lower-resource neighborhoods with limited access to quality education and employment opportunities. However, only two U.S.-based studies in this review examined cognition by race and ethnicity, and their findings were inconsistent. One study reported that White patients were more likely to exhibit high cognitive performance (Patel et al., 2015), while the other found no significant relationships (Bajaj et al., 2022). Moreover, some U.S.-based studies did not report the race and ethnicity of participants. These findings highlight a gap in research examining the intersection of race, ethnicity, and SDOH in relation to cognition.
This review also identified methodological limitations in the assessment of cognition. Most studies used HE-specific neuropsychological tests that primarily measure attention, executive function, and visuospatial abilities, leaving other cognitive domains, such as memory, largely unexplored. Given that cognitive dysfunction in cirrhosis is not solely attributable to HE (Kjærgaard et al., 2021), broader cognitive assessments are essential to fully characterize cognitive dysfunction in this population. Although all included studies met methodological quality criteria, the predominance of cross-sectional designs and small sample sizes (fewer than 200 participants) limits generalizability. The longitudinal studies lacked comparison groups, and the randomized controlled trial did not clearly report blinding procedures.
While this scoping review identified gaps in knowledge through a comprehensive literature search across multiple databases, it has a few limitations. We included studies that described SDOH in their abstracts; therefore, studies that investigated SDOH but only reported it in the full text may have been excluded. We limited our review to studies published in English. The heterogeneity of study designs and methodologies among the included studies prevents direct comparison of results. In addition, publication bias, favoring the publication of statistically significant findings in certain domains of SDOH and cognition, may further limit our understanding. Since most of the included studies used a cross-sectional design, the associations between SDOH and cognition do not indicate cause and effect.
Conclusions
In conclusion, this scoping review found that education and employment were consistently associated with cognitive performance, primarily in the domains of attention, executive function, and visuospatial abilities, among patients with cirrhosis. Clinicians may consider cognitive screening for patients with limited educational attainment or those who are unemployed and offer tailored support as needed. This review also highlighted the need for additional research in underexplored SDOH domains to better understand their influences on the risk of developing cognitive dysfunction in cirrhosis. Furthermore, it is crucial to explore how these factors influence cognition across different racial and ethnic groups. Addressing these identified gaps in future research will enhance our understanding of the relationship between SDOH and cognition and inform the development of future interventions aimed at mitigating cognitive dysfunction in cirrhosis.
Footnotes
Acknowledgements
The authors thank Philip Espinola Coombs, a health science librarian at Northeastern University, for his support in developing the search terms.
Author Contributions
NGS: literature search and screening, data extraction, analysis, writing—original draft preparation, review and editing; SW: literature screening, visualization; AK: data interpretation, writing—review and editing; FDG: data interpretation, writing–review and editing; DK: conceptualization, methodology, literature screening, data extraction, analysis, interpretation, and writing—original draft preparation, review and editing. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable.
Author Biographies
Dami Ko, PhD, RN, is an Assistant Professor in the School of Nursing at Northeastern University. Her program of research focuses on advancing health outcomes in patients with liver disease.