
Abstract
One and a half million cardiac surgeries are completed worldwide each year where undertreated postoperative pain increases the risk of patient morbidity and mortality. Patient-centered pain management is recommended to improve patient outcomes but there is insufficient information regarding how the patient views their role. The objective of this study is to explore cardiac surgery patients’ perspectives on their role in postoperative pain management. This study used an interpretive phenomenological design and convenience sampling. Six participants who had undergone cardiac surgery were recruited from a cardiac rehabilitation program in Western Canada. The first author conducted semi-structured digitally recorded interviews. Sociodemographic characteristics and measures of anxiety and depression were also collected. Emergent thematic analysis of the qualitative data generated three themes: attitude, coping and care, and communication. The findings of this study address a gap in the literature with regard to patients’ perceived roles in pain management. There is a complex relationship between patient attitude, coping and care, and communication which, in turn, influences how patients view their role within the pain management continuum. These themes contribute to the development of the patient role within the pain management continuum and form an integrated feedback loop. The patient’s attitude contributes to their ability to cope with pain and participate in pain assessment and management. Furthermore, their ability to cope and desire to participate influences the development of their attitude. These findings may enhance providers’ understanding of the patient’s perspective and improve pain management outcomes.
Cardiac surgery is a widely accepted treatment modality for heart disease in Canada and around the world with approximately 1.5 million surgeries performed annually worldwide (Tai et al., 2021). The complex nature of cardiac surgery can result in nociceptive pain from tissue injury (Tai et al., 2021). It is acknowledged that postoperative pain contributes to complications associated with increased length of stay, increased readmission rates, higher morbidity and mortality (Jayakumar et al., 2019), persistent postsurgical pain (Katijjahbe et al., 2021; Sethares et al., 2013), and persistent opioid use (Lanzillotta et al., 2018). Literature indicates that moderate to severe pain is reported following cardiac surgery (Boitor et al., 2017; Lanzillotta et al., 2018) with rates of up to 74% of patients reporting significant levels of pain after discharge (Gan et al., 2014; Jayakumar et al., 2019). Complications may be mitigated by improved postsurgical management of pain with evidence supporting that the key is a patient-centered focus (Pomey et al., 2015). As pain assessment is an acknowledged crucial first step in pain management (Wooldridge & Branney, 2020), and self-report is the gold standard for assessment (Gordon, 2015), it is clear that the patient perspective is critical to pain management.
How do Cardiac Surgery Patients View Their Role in Pain Management?
Existing literature on pain management has focused on investigating patient characteristics and risk factors to develop approaches to manage anxiety, depression, and acute pain in the postoperative phase (Aternali et al., 2022; Pagé et al., 2017). However, there remains a paucity of information regarding the patient’s perception of their role in pain management. A recent scoping review of pain management highlighted aspects of the surgical patient’s pain experience (Walton et al., 2023).
Purpose
A significant knowledge gap on how patients view their role in the interactions within pain management was revealed, including those individuals undergoing cardiac surgery. Therefore, this study aimed to explore the cardiac surgery patients’ perspective regarding their role in pain management.
Methods
The methodological orientation for this study was interpretive phenomenology. A qualitative study was carried out with cardiac surgery patients with recruitment from a cardiac rehabilitation program in Western Canada. Volunteer participants were recruited via telephone over 6 months from May 2021 to October 2021, using convenience sampling. Participants had undergone cardiac surgery via sternotomy approach in the previous 6 months and were able to speak and understand English. Verbal consent was obtained. The study included semi-structured interviews via telephone and the use of a voice recorder. The duration of interviews ranged from 35 to 50 minutes. The interviews employed an interview guide developed by the authors based on current literature as well as anxiety (Generalized Anxiety Disorder assessment GAD-7) (Spitzer et al., 2006) and depression (Brief Depression Severity measure PHQ-9) (Kroenke et al., 2001) scales, and a researcher-developed sociodemographic survey inviting information related to age, education level attained, employment status, and relationship status.
Eight individuals were recruited for participation and a total of six participants were interviewed. The two individuals who declined to participate cited time constraints as the reason. Recruitment during COVID-19 protocols which included lockdowns was challenging and resulted in reduced ability to recruit. All particpants were male and had undergone cardiac surgery within the last 3 weeks to 5 months. Transcribed interviews were read in their entirety, and the digital recordings were reviewed to ensure that their meaning was understood in the manner intended by the participant. An emergent interpretive phenomenological analysis of the data was completed by the lead author, reviewed by (DM), and subsequently validated by all authors. Themes were developed through standard coding practices (Braun & Clarke, 2006). Data and codes were managed by Atlas Ti software. Trustworthiness was enhanced using multiple data sources, demographics, transcribed interviews, and a reflective journal which included field notes taken at the time of the interviews. Anonymized data were reviewed by (LW) and confirmed by all authors for thematic validity to increase rigor. Lastly, participant validation was employed with a 50% response rate. Ethics approval was received from the University of Manitoba Ethics Board in May of 2021 with a designated approval number of HS 24917.
Results
The participants all identified as male and were between the ages of 56 and 76 years (mean 68 years). They were all in a committed relationship (either marriage or common law). Two individuals were still actively employed at the time of the interviews with the other four being retired. The participants had varying levels of education with two having less than high school, two with bachelor’s degrees, and one having attended trade school.
Three overarching themes with identified subthemes were generated from the interview data. First was the theme of attitude toward pain assessment and management which encompassed the subthemes of expectations, prior experience, and beliefs.
Expectations
Patients expressed a desire to be able to exceed the perceived expectations placed on their recovery and performance as patients: I try to exceed what is expected of me and I was out of hospital in 4 days, I wanted to be out in 3. (P0937) I want to get back to playing with my fellow musicians. (P1524)
Prior Experience
Prior experience helped reduce anxiety and familiarity with the environment assisted in confidence with participation in pain management. Participants indicated that prior pain experiences facilitated awareness of their body’s response to pain and how to approach the management of the pain: This was not my first rodeo. (P1524) I was not in a foreign environment. (P1226) Chronic pain is not who I am and that helps me. (P0937)
Beliefs
Beliefs regarding spirituality assisted with recovery. Beliefs regarding the safety and efficacy of treatments contributed to the patient’s attitude. Finally, a belief in their responsibility regarding participation in pain management was noted: I am spiritual . . .. I feel a destiny. (P1602) Some miracle of sorts. (P1524) I never really took any drugs because I figured it was going to numb the pain and make it worse after. . .cause more injuries. (P0929)
Member check-in validated the belief in individual responsibility regarding active participation in pain management. This contributed to the overall attitude toward the patient’s role in pain management: My job is to do the things I can do, and Our job is to do the part of the recovery we can do. (P1602) This is your like, your body so you have to take care of it. (P0937)
The second theme was coping, with the subthemes of mindfulness or distraction, social interaction, and knowing yourself. Some participants focused specifically on methods that assisted in coping, while with others it was implied.
Mindfulness or Distraction
Technical aspects of the surgery or devices employed during care provided a distraction while other participants used mindfulness strategies: A pacemaker is a gizmo, I’m a gizmo guy. (P1602) Mindfulness helps me quite a bit. (P0937) You have to relax. (P1524)
Social Interaction
Engaging members of the healthcare team in playful or humorous banter assisted with coping. In addition, interaction with family and friends as well as the use of social media was important for coping: If I didn’t have people close to me. . .I wouldn’t be able to do it alone. (P1602) I try to use a bit of wit and a little bit of humour. (P1602) I had a friend come over. (P0929)
Knowing Yourself
Participants noted that knowing their limits and pacing themselves assisted them in being able to cope: You have to listen to your body. (P1602) You have to be able to adapt. (P1524) I’ve been taking it easy, like I don’t overextend. (P0957) You have to be in tune with your body. (P0937)
The final theme was care and communication which was composed of the subthemes of pain assessment interaction, pain education, and empathetic care communication. The participants’ perceived ability to participate in pain management was explored.
Pain Assessment
Participants noted the challenges inherent in pain assessment due to the subjective nature of pain and also indicated that being clear and honest is crucial in achieving effective pain management. Participants expressed that pain assessment interactions made them feel cared for: How do you feel someone else’s pain? (P0929) You have to be clear in your communication with your providers. (P1602) I am an open book. (P1226) If you don’t tell them all the facts, they can’t figure out what needs to be done. (P0937)
Education
Education regarding pain assessment and management was valued by participants. In addition, the right to stop the flow of information held importance. One noted education gap was sufficient information about pain assessment anchors for the numeric rating scale and how the assigned value was relayed to the patient experience: By the time it came around I knew exactly what to expect. (P1226) Finally, I said I don’t want to know any more. (P1524) . . .yeah, I really don’t know the number scale because I’ve never had any education on what a 10 would be. (P0929)
Significantly, participants also received information from individuals outside of the healthcare team. Information from friends and relatives who had similar experiences to share was sought, while others spoke to fellow patients to discover information. Member check-in revealed that one participant had explored information online using peer-reviewed journals and physician-recommended websites to help build their “toolbox” of knowledge. Conversely, one participant explained that he benefited from educating a friend scheduled for heart surgery, solidifying information that he received concerning his recovery: It kind of helped me as well because I had to express it in clear terms. (P1602)
Empathetic Care
The participants noted that empathetic care was integral to developing trust and fostering feelings of well-being which assisted with coping: The care made me feel comfortable. (P1524) Trust is what you develop through the interchange. (P1602) I was very reassured. . .I was calm as I could be because I knew I was in good hands. (P1226)
Discussion
Exploring the question of how the patient views their pain management role, our findings support that patients do not specifically identify that they occupy a role in pain management, nor do they define what is that role. Rather, participants described aspects of this role in terms of expectations, responsibilities, and beliefs which contribute to an overall attitude that forms the basis of their participation in care and communication within the healthcare team. In addition, their experience of participation regarding pain assessment and management forms a feedback loop to the attitude they hold toward their role (see Figure 1).
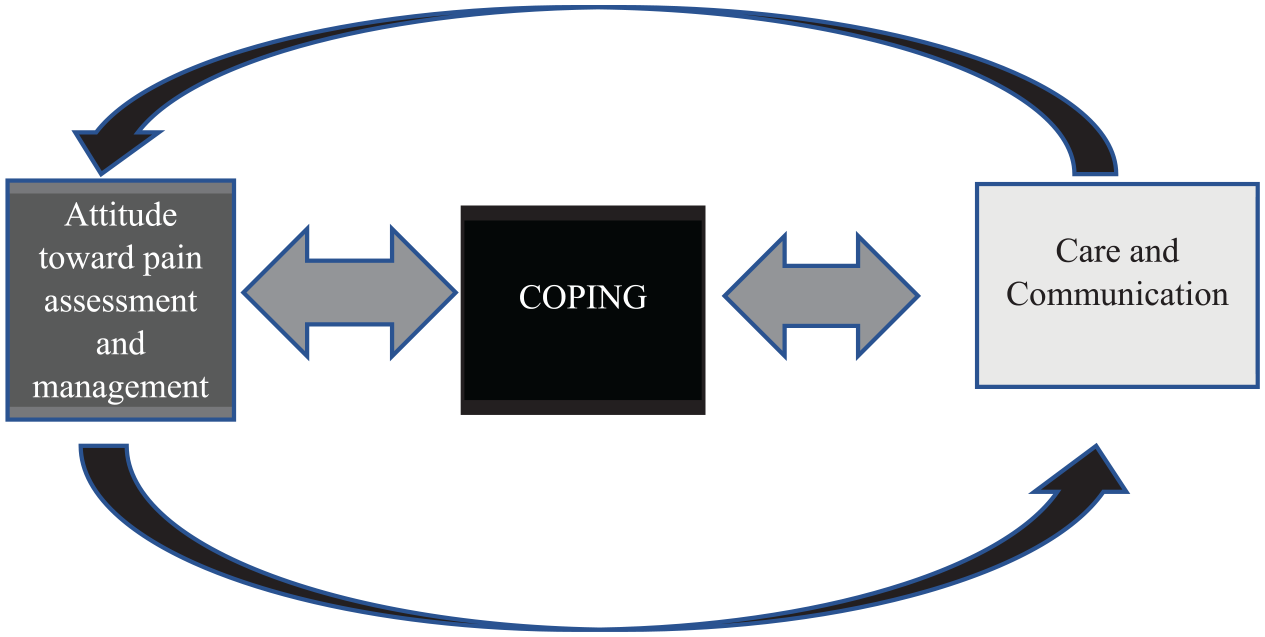
Attitudinal coping and care interaction model.
The results from this study are consistent with prior research which indicates that patients have expectations about how they will perform in the recovery stages after surgery and what will be the final outcomes of surgery (Hansen et al., 2016). In a narrative study exploring recovery from cardiac surgery (Hansen et al., 2016), most participants, both male and female alike, expected to return to “normal life” after surgical intervention (p. 1102). This was reflected in our findings within the subtheme expectations where participants expressed they desired and expected a return to prior activities. Similar to the findings of Angelini et al. (2018), this current study identified that patients who had prior experience with postoperative pain tended to have lower levels of postoperative anxiety and lower levels of acute pain.
The current study identified patients’ beliefs about the risks and benefits of pain medications and reinforced prior evidence that patients were “overwhelmingly misinformed regarding . . .the risks involved in taking medications to control pain” (Cogan et al., 2014. p. 576). Participants were reported to express that less pain medication is preferable to avoid not being aware of the pain and causing injury is similar to a study exploring misconceptions (Cogan et al., 2014). This belief may present challenges in the management of acute postoperative pain with patients desiring to avoid medications due to misconceptions.
Spiritual belief was identified as a contributing factor with respect to patients’ roles within the themes of this study. This finding supports previous research that the spirituality belief may encourage patient empowerment and reduce complications due to the focus on an “internal locus of control” related to belief in a higher power (Ai et al., 2012, p. 1102). One Heideggerian study examining the existential aspects of the cardiac surgery patient awaiting surgery demonstrated that some patients can experience existential anguish related to the unknown aspects of their futures which was the same for both male and female participants (Gomes et al., 2018). Our study examined the post-surgical aspects of the cardiac surgery experience and found strong spiritual beliefs appeared to foster coping. The empowered patient may be strongly positioned to take responsibility within the pain management interaction.
In addition, this work aligns with a previous report that patients should be encouraged to move beyond passive interactions and feel empowered to engage actively in pain management. These opportunities may not be explicit but rather implied (Hansen et al., 2016). Empowerment, whether defined as an outcome (Acuña Mora et al., 2022) or a process (Falk-Rafael, 2001), is associated with increased awareness, knowledge, and skills supporting improved health outcomes. Our study found that patients believe they have a responsibility to participate and to be active advocates, reflecting expressions of empowerment.
This study found that similar to prior investigations, humor and mindfulness could be employed as important coping tools (Boezeman et al., 2016). A novel finding of this study was the discovery that coping contributed to the participant’s overall attitude toward pain management and their role as a patient. The ability to cope facilitated a more positive attitude toward pain management, including assessment. The wide variety of coping strategies employed by participants demonstrates the need for individualized care and opportunities for patients to practice mindfulness, socialize, and be self-aware.
Our findings further reinforced the research evidence which demonstrates the subjective nature of pain and the resulting challenges associated with self-report (Kaptain et al., 2017). In addition, the need for improved education regarding pain assessment tools and the associated anchor points has been noted previously and was reaffirmed with the outcomes of this research (Gordon, 2015).
The participants in our study reported very low levels of anxiety and depression which is contrary to much of the literature on patient factors thought to influence pain management and cardiac surgery recovery (Aternali et al., 2022; Bjørnnes et al., 2018; Sethares et al., 2013). This may have been related to the high level of confidence, self-efficacy, and self-awareness that these patients exhibited as they self-selected for participation in the study.
Lastly, this study provided support for the body of literature which indicates that empathetic caring, which goes beyond routine assessment and patient education and extends to the general provision of care, is critical to the satisfaction and overall well-being of the patient (Mubita et al., 2020). However, of note in this study was the extent to which participants indicated the impact of these interactions on their attitude and ability to cope with pain and the extent to which this encouraged them to participate in pain management.
Participants did not express that there was an explicit role they occupied in pain management. Instead, they spoke of their approaches and attitudes to various aspects of pain management. Therefore, our findings demonstrate that the patient’s role in pain management is poorly defined from the perspective of cardiac surgery patients. With acknowledgment of the need for patient and care-provider partnerships to improve outcomes and effective utilization of resources, it is crucial to understand the perspective of the patient and the complexities of how patient attitudes impact this role, its development, and what clinicians can adapt to improve outcomes. Further studies in pain management exploring patient perception, awareness, and interpretation of their role with explicit attention to expectations and triggers for participation should be undertaken. Our study is the only study that we are aware of that specifically explored the patient perception of their role in pain management after cardiac surgery. While recruitment was open to both males and females, our study participants were all self-identified males, raising questions about whether these views are relatable to a more gender-diverse cardiac population. Although there is a dearth of literature related to gender and the perceived role in pain management within the cardiac surgery literature, it is notable that some work has explored the relationship of gender within the cardiac postoperative experience (Bellet et al., 2017; Kemp et al., 2021; Sethares et al., 2013). In their phenomenological study, Kemp et al. (2021) reported that the demographics of the eight participants (7 male, 1 female) were similar to the overall cardiac surgery patient population and that statements regarding how the participants viewed their experience were similar across genders. Another study explored the impact and experience of pain for male and female participants. This exploration of the interference of pain and strategies employed by postoperative patients during their recovery, noted that while the female participants rated their pain higher on a numeric rating scale for the 12 weeks of the study, there was no difference in pain interference (Sethares et al., 2013). However, a study by Bellet et al. (2017) found that being female was a risk factor for a higher prevalence of pain and shoulder disability after cardiac surgery. Unfortunately, none of these studies explored the patient’s perception of pain or disability as it related to their role as a patient, nor how it may have impacted their attitude and ability to participate actively in their pain management.
Limitations
Qualitative interpretive phenomenological research intends to gain knowledge of the situated participant. However, it is acknowledged that this study was conducted at a single cardiac rehabilitation site. Second, all participants identified as male based on convenience sampling. This may limit the transferability of the findings. Future studies should explicitly explore the perspective of both male and female patients undergoing cardiac surgery to determine how these perceptions may vary with gender to facilitate a more robust understanding of the role. In addition, these interviews were conducted only in English with participants who self-identified as Caucasian. Future studies should consider the influencing factors of language and culture. Therefore, there should be the possibility of varying the language utilized for the interviews and consider consulting with patient advocates from a variety of cultural backgrounds to improve the questionnaire guide to enhance generalizability.
Conclusions
This qualitative study exploring the role of the patient in pain management following cardiac surgery found a complex relationship between patient attitude, coping and care, and communication which, in turn, influences how patients view their role within the pain management continuum. Issues with congruence in pain assessment and lack of participation in treatment decisions may contribute to the continued issue of undermanaged postoperative pain. Future research should focus on further investigation into the development of the patient role and its impact on participation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Manitoba Centre for Nursing and Health Research grant (Grant # 54893) and the University of Manitoba College of Nurses Endowment fund.
Ethics Approval
University of Manitoba Ethics Review Board, May 2021 approval number HS24917