
Abstract
This study investigated the pattern of weight variability over 8 weeks and its associations with achieving weight gain goals and five biopsychosocial factors among pregnant women. We conducted a secondary analysis of 117 weeks of data from 16 pregnant women with a body mass index (BMI) ≥25. Weight variability was calculated from the difference of ending and beginning and maximum and minimum weights in a week and percent of each difference from baseline weight. Loess smoother, repeated measures model, and compound symmetric covariance matrix were used for analysis. The variability measure of maximum-minimum weight (overall mean: 2.1 ± 0.4 lbs.) was greater than the ending-beginning weight measure (overall mean: 0.7 ± 0.6 lbs.). Weight variability was negatively associated with achieving weight gain goals but not with biopsychosocial factors. Assessing weight variability is important during pregnancy so that preventive measures or lifestyle counseling can be instituted immediately to prevent excessive weight gain.
Keywords
Approximately 50% of women gain excessive weight during pregnancy (Brannum et al., 2016). Pregnant women are advised to gain weight during pregnancy, but excessive weight gain can cause maternal (e.g., gestational diabetes, hypertension) and infant (e.g., preterm birth, large birth weight) adverse outcomes (Goławski et al., 2023; Santos et al., 2019). Empirical evidence gathered from non-pregnant individuals indicates that weight variability could elevate the likelihood of metabolic and cardiovascular diseases, as well as obesity. To effectively mitigate excessive gestational weight gain among expectant mothers, it is vital to include, within prenatal weight management counseling, not only guidance on the appropriate amount of weight to gain but also strategies to minimize weight fluctuations. Nonetheless, research on weight variability specifically within the pregnant population has been relatively scarce.
Weight variability is the fluctuation of the overall trend and pattern in body weight quantified from frequent weight measures (Turicchi et al., 2021). Weight variability and weight cycling are interchangeable terms used by researchers. Some researchers view weight cycling as a history of repeated weight fluctuations by volitional weight loss and weight regain over time (Lowe et al., 2015). Weight variability can predict cardiovascular and metabolic problems. In a previous study, people with the highest weight variability (3rd tertile), as compared to those with the lowest weight variability (1st tertile), had a 2.06-fold increase for high blood pressure, low high-density lipoprotein-cholesterol, and increased waist circumference over a 7-year follow-up period (Vergnaud et al., 2008). For individuals with diabetes, weight variability has been shown to increase their risks for cardiovascular events, myocardial infarction, and stroke (Bangalore et al., 2018; Nam et al., 2020).
Emerging evidence has also shown that weight variability among non-pregnant adults can impact weight outcomes. Using a weight measurement protocol of four times a day for 4 months in a weight reduction program, researchers found that patients with a weight variability in the 75th percentile before going to bed had higher body weight and abdominal visceral fat at 8, 12, and 16 months than those with a weight variability in the 25th percentile (Tanaka et al., 2004). Data from a weight maintenance program designed for adults with at least 5% prior weight loss showed that greater weight variability in the first 12 weeks predicted greater weight change at 6, 12, and 18 months (Turicchi et al., 2021). The relationship between weight variability and weight gain has also been observed in individuals who have not been in weight loss or maintenance programs (Benson et al., 2020; Lowe et al., 2015).
To date, research on weight variability among pregnant women and its associated factors remains scarce. A previous study found that pregnant women who gained excessive weight during pregnancy had a higher number of weight loss attempts before pregnancy than the women who did not gain excessive gestational weight (Nagpal et al., 2020). Other studies focused on excessive maternal gestational weight gain also examined weight cycling that occurred before pregnancy, not during pregnancy (Ölin & Rössner, 1996; Piccinini-Vallis et al., 2021).
A few previous studies found that diet and physical activity influenced weight variability (Field et al., 2009; Nagpal et al., 2020; Stafford et al., 1998); additional biopsychosocial factors associated with weight variability during pregnancy have not been explored. According to Engel’s (1977) Biopsychosocial Model, biological and psychosocial factors interact to affect health. In this study, we explored five biopsychosocial factors, including morning sickness, food cravings, sad mood, stress, and household food shortages, that are pregnancy-specific or intensified during pregnancy and thus have the potential to influence gestational weight gain. Morning sickness may occur throughout pregnancy and change pregnant women’s diet habits (Singh et al., 2023). Approximately 80% of pregnant women have reported food cravings, and 45% reported developing new cravings during pregnancy (Belzer et al., 2010; Farland et al., 2015). Lastly, studies suggest that depression, stress, and household food shortages, more notable during pregnancy, directly or indirectly influence healthy eating, physical activity, and weight gain (Chang et al., 2015; Kolko et al., 2017; Matthews et al., 2018; Shieh & Wu, 2014; Thomas et al., 2014).
In summary, weight variability could increase the risk for developing metabolic and cardiovascular health problems, overweight, and obesity. Pre-pregnancy weight variability has been reported to link to maternal excessive gestational weight gain. Weight variability occurring during pregnancy and its associated factors, however, have not been studied.
The purpose of this study was to assess patterns of weekly weight variability and its associations with achieving weight gain goals and biopsychosocial factors among pregnant women who participated in an 8-week weight management intervention. Specific aims included assessing (1) the patterns of weekly weight variability across 8 weeks, (2) the association between weekly weight variability and achieving weekly weight gain goals, and (3) the associations between weekly weight variability and five biopsychosocial factors, including morning sickness, food cravings, household food shortage, stress, and sad mood.
Methods
Design
This study reflected a secondary analysis of data from an 8-week one-group cognitive behavior weight management intervention conducted in 2014 to 2015, which was approved by an institutional review board for human subjects protection. Details about the trial were published elsewhere (Shieh et al., 2017). Briefly, study participants were given weekly goals for weight gain, food intake, and walking. They self-monitored their weight, food intake, and walking steps daily and the five biopsychosocial factors weekly. Using a provided digital weight scale, participants measured weight at home in the morning with light clothes on and no shoes. They mailed self-monitored data to the research office. During the 4- and 8-week meetings, data from previous weeks were reviewed individually with each participant by an interactionist, and barriers and strategies related to achieving goals were discussed.
Study Participants
Enrollment criteria for the original study included pregnant women who were at less than 20 weeks of gestation, had a pre-pregnancy BMI of 25 or higher, and had no history of cardio/metabolic or psychiatric diagnoses. In this secondary analysis, we included 16 pregnant women with at least 50% (4 weeks) of weight data (12 participants had 100% data, 1 had 87.5% data, 1 had 75% data, and 2 had 50% data) for a total of 117 weeks of data for analysis.
Measurements
Weight Variability
We used four measures of weekly weight variability, including the ending-beginning weight (weight difference between the first day and the last day of a week), maximum-minimum weight (difference between the highest and the lowest weight in a week), ending-beginning weight as percent of baseline weight, and maximum-minimum weight as percent of baseline weight.
Achieving Weight Gain Goals
We used the Institute of Medicine’s (2019) weight gain recommendations for pregnant women. The recommended weekly weight gain is 0.75 lbs. for women with a pre-pregnancy BMI of 25 to 29.99 and 0.5 lbs. for women with a pre-pregnancy BMI of 30 or higher. Participant were considered to have achieved their weight gain goals of the week when their weekly weight gain did not exceed the range based on their pre-pregnancy BMI.
Biopsychosocial Factors
Participants self-reported their weekly morning sickness, food cravings, stress, and sad mood (feeling sad) using response categories of “not at all,” “a little bit,” or “very strong.” They also self-reported food in the house as “enough,” “a little bit short,” or “totally not enough.” For the analysis, biopsychosocial factors were clustered as present or absent. We combined “a little bit” and “very strong” into one category of “having symptom” to distinguish participants who had the symptom from those who did not (“not at all”). Similarly, for household food, we combined “a little bit short” and “totally not enough” into one category of “having household food shortage” to distinguish participants who had household food shortage from those who did not (“enough”).
Data Analysis
To assess patterns of weight variability over time (aim 1), we plotted individual participants’ weight variability measures (ending-beginning weight, maximum-minimum weight, ending-beginning weight as percent of baseline weight, and maximum-minimum weight as percent of baseline weight) from the 8-week period. To better assess trends over time, we used a loess smoother, which allowed us to see fluctuations in average weekly weight variability over time.
From the plots, we saw that the patterns of weekly weight variability whether measured as differences or as percentages of baseline weight were similar, so for analyses of aims 2 and 3, we chose to only analyze weight variability measures as a percent of baseline weight.
To assess whether weight variability was associated with achieving weight gain goals (aim 2), we fit a repeated measures model of the two weight variability measures (i.e., percent of baseline weight). The model had independent terms of meeting the goal, week, and the interaction of meeting the goal with week. A compound symmetric covariance matrix was used. Differences in mean weekly weight variability between those who met the goal and those who did not were presented.
To assess whether weight variability was associated with biopsychosocial factors (aim 3), we fit models similar to that described above. Differences in mean weight variability between those having and not having a symptom and those having and not having household food shortage were presented.
Results
Study Participants
The average gestation of study participants upon enrollment was 17.2 ± 3.3 weeks, and the mean age was 29.3 ± 5.6 years. Of the 16 participants, 4 (25%) had a pre-pregnancy BMI of 25–29.99, and 12 (75%) had a pre-pregnancy BMI of 30 or higher. The majority were Black (75%), single (56%), had a high school or no high school diploma (44%), worked outside the home (63%), had a household income of less than $25,000 a year (50%), and had two pregnancies including the current one (75%). Other socioeconomic information of the study participants included that 56% (n = 9) and 50% (n = 8) were recipients of the Special Supplemental Nutrition Program for Women, Infants, and Children and the Supplemental Nutrition Assistance Program (formerly food stamps), respectively.
Patterns of Weekly Weight Variability
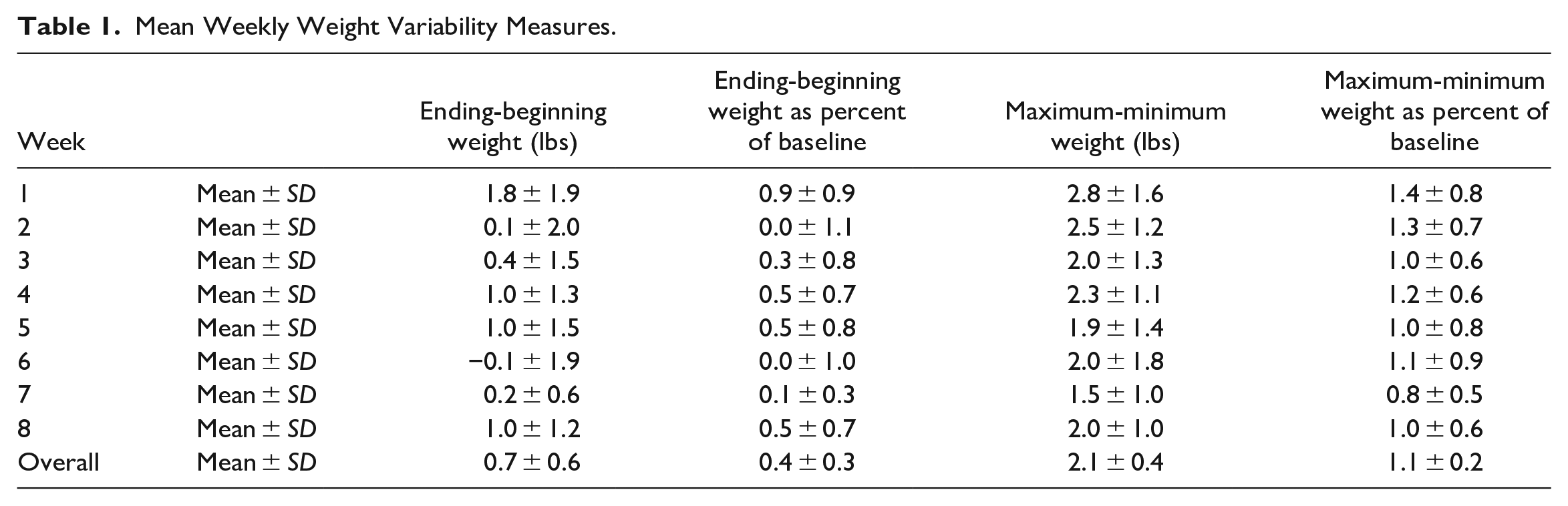
In general, maximum-minimum weight variability measure (overall mean: 2.1 ± 0.4 lbs.) was larger than the ending-beginning weight variability measure (overall mean: 0.7 ± 0.6 lbs.). The maximum-minimum weight as precent of baseline weight variability measure (overall mean: 1.1 ± 0.2%) was also higher than the ending-beginning weight as percent of baseline weight variability measure (overall mean: 0.4 ± 0.3%) (see Table 1).
Mean Weekly Weight Variability Measures.
Patterns of weekly weight variability over time were similar regardless of whether measures were the raw difference or the percent of baseline weight (Figures 1 and 2). In Figure 1, the pattern of ending-beginning weight difference decreased from weeks 1 through 3 but remained stable from weeks 4 through 8. In Figure 2, the maximum-minimum weight difference steadily decreased over the 8 weeks.
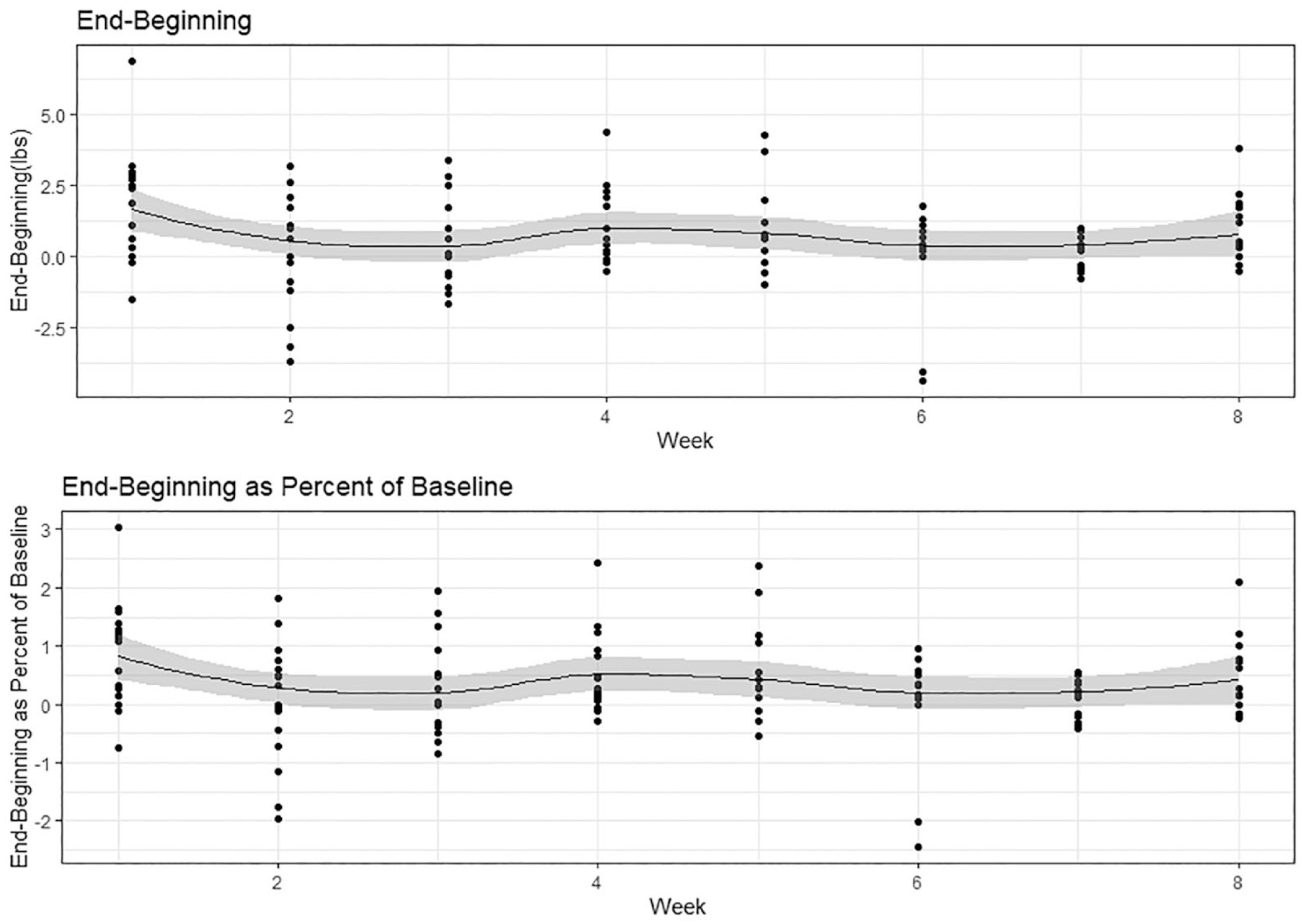
Average weekly weight variability over time based on ending-beginning weight and ending-beginning weight as percent of baseline.
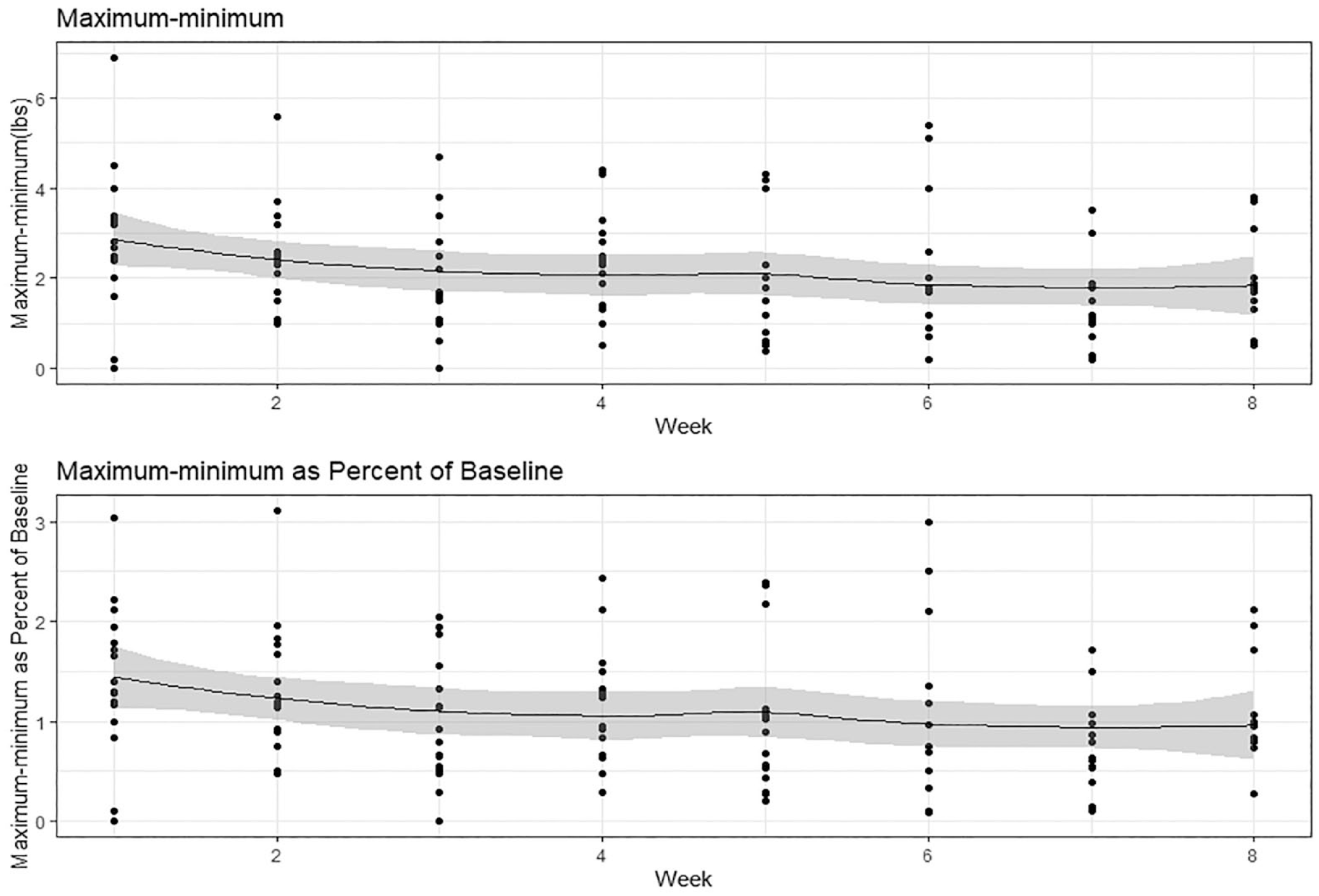
Average weekly weight variability over time based on maximum-minimum weight and maximum-minimum weight as percent of baseline.
Association Between Weekly Weight Variability and Achieving Weight Gain Goals
In Table 2, the main effect of achieving weight gain goals showed that those who achieved weight gain goals had, on average, significantly lower percent ending-beginning weight (p < .0001) and percent maximum-minimum weight (p = .0015) than those who did not achieve weight gain goals. Comparisons of weekly percent ending-beginning weight showed that for all weeks but one, average weight variability was significantly greater in participants who did not achieve weight gain goals than in those who achieved weight gain goals. When modeling percent maximum-minimum weight, we saw significantly greater weight variability in those who did not achieve weight gain goals in weeks 1, 5 and 8. Graphs in Figures 3 and 4 show the mean weekly weight variability measures of those who achieved and did not achieve weight gain goals over the 8 weeks.
Weekly Mean Weight Variability by Goal Met.
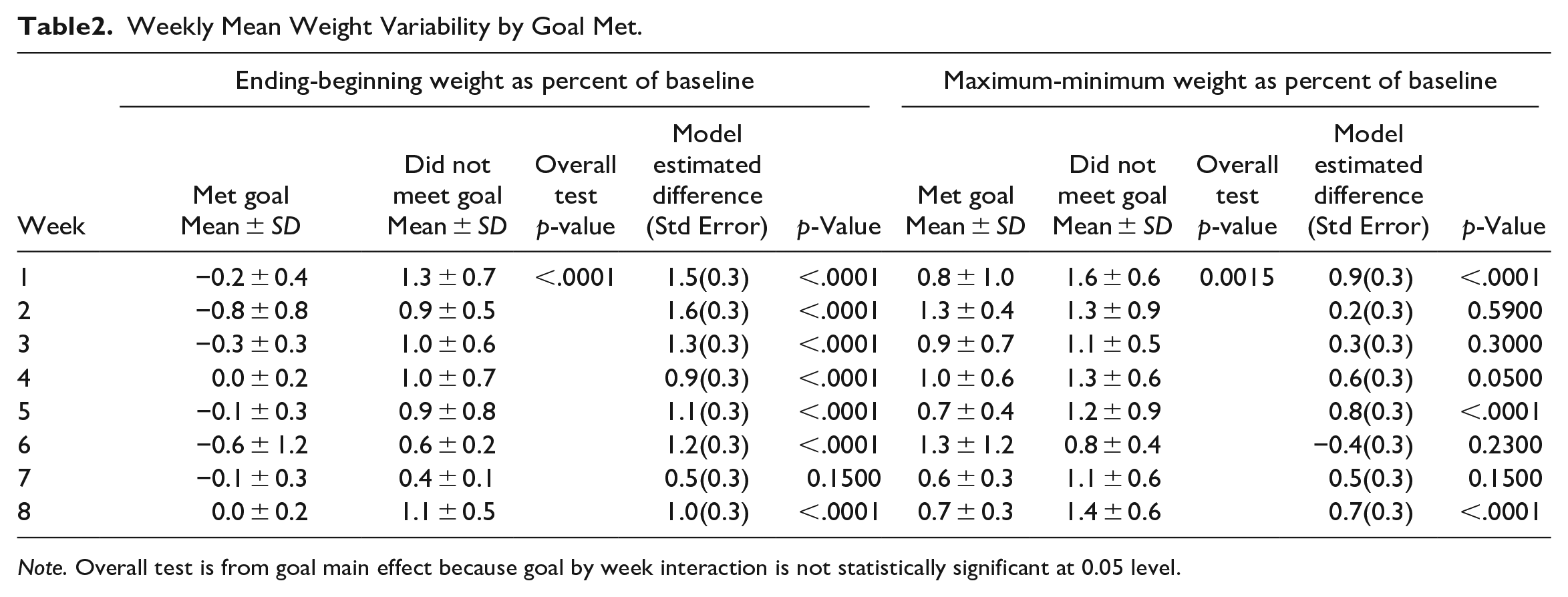
Note. Overall test is from goal main effect because goal by week interaction is not statistically significant at 0.05 level.
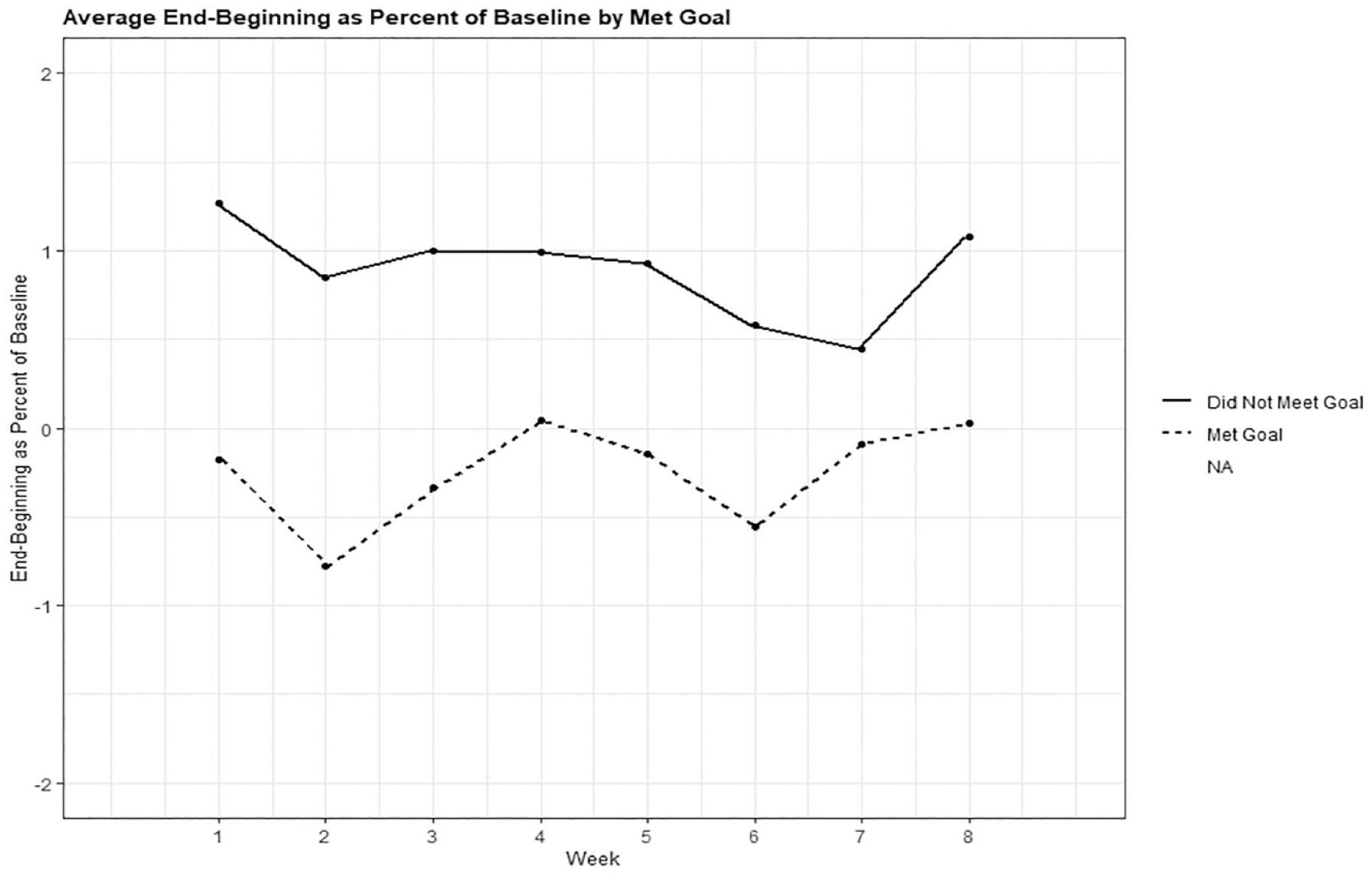
Association of weight variability as ending-beginning weight as percent of baseline and weight gain goals (goal met or not).
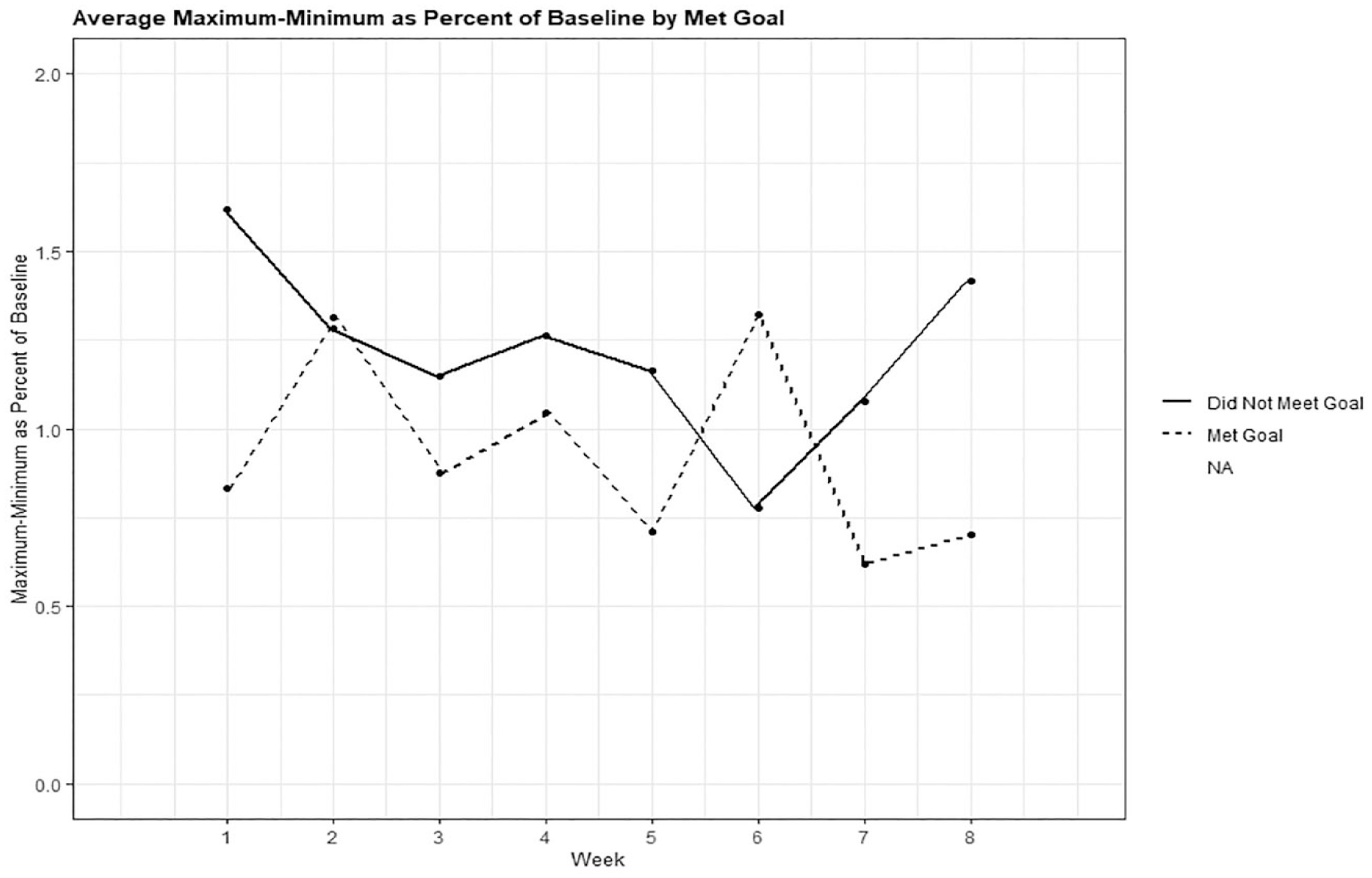
Association of weight variability as maximum-minimum weight as percent of baseline and weight gain goals (goal met or not).
Associations Between Weekly Weight Variability and Biopsychosocial Factors
Table 3 shows the results from models of ending-beginning weight as percent of baseline weight and maximum-minimum weight as percent of baseline weight and their associations with biopsychosocial factors. The only significant association was between ending-beginning weight as percent of baseline weight and sad mood (p = 0.0318), and weekly comparisons revealed that a significant difference was seen only in week 6 (p = .0018). In that week, those with a sad mood had significantly smaller mean ending-beginning weight as percent of baseline weight than those without a sad mood.
Estimated Mean Weight Variability (as Percent of Baseline) by Biopsychosocial Factors.
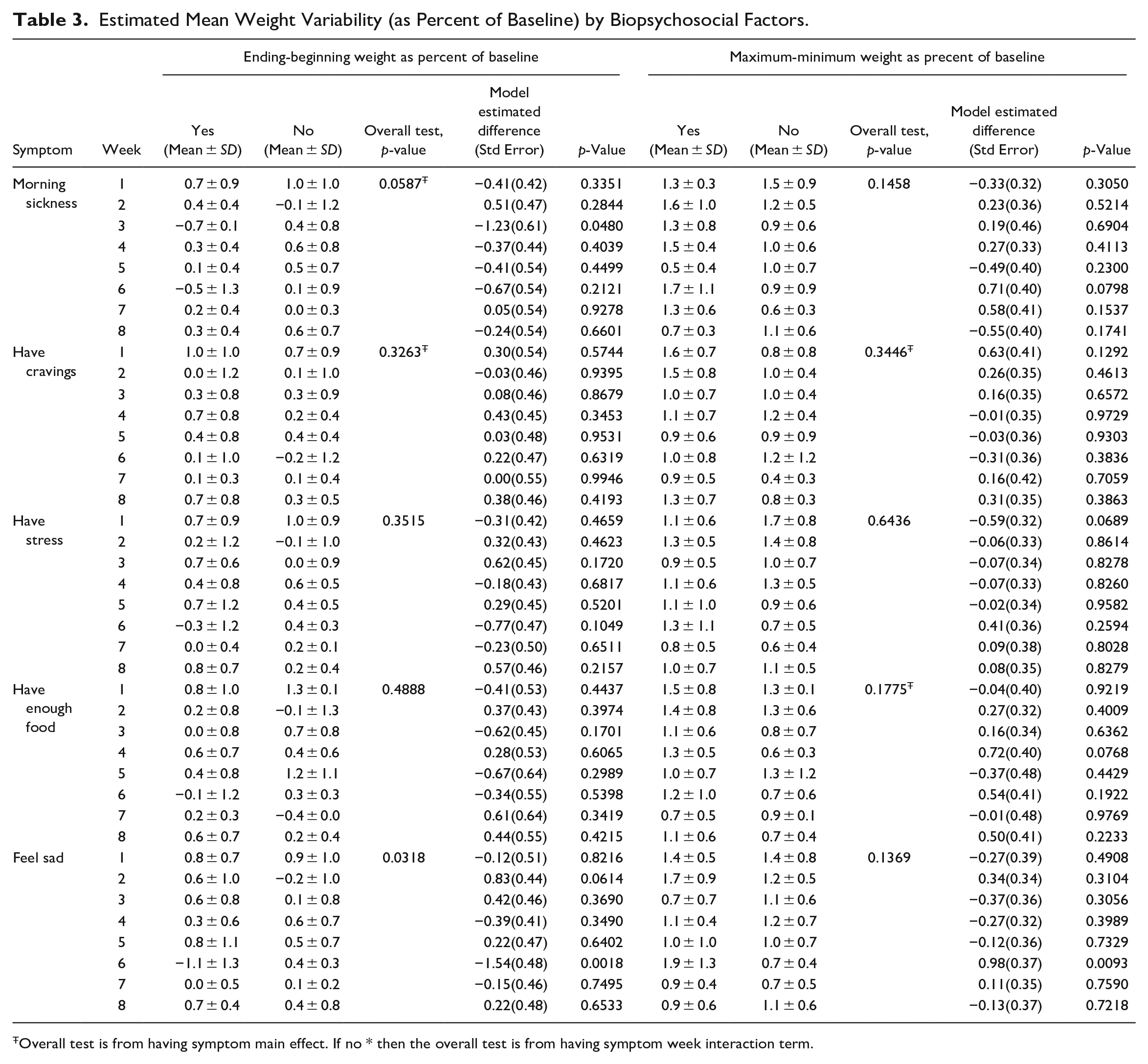
Overall test is from having symptom main effect. If no * then the overall test is from having symptom week interaction term.
Discussion
To our knowledge, this study was the first to investigate patterns of prenatal weight variability among pregnant women with overweight or obesity and associations of weight variability with achieving weight gain goals and biopsychosocial factors.
A major finding from our study was that weight variability was present during pregnancy and the average weekly weight variability was greater than the average weekly weight gain. Previous weight variability studies on non-pregnant adults assessed weight outcomes weeks or months after the intervention (Benson et al., 2020; Field et al., 2009; Lowe et al., 2015; Tanaka et al., 2004). We measured weight variability and weight outcome concurrently in the same week among pregnant study participants. Short- and long-term weight outcomes associated with weight variability are all important, but short-term weight outcomes can provide opportunities for timely modifications in weight management behaviors. Overall, our study findings support that weight variability can play a role in weight outcomes even for the pregnant population whose weight management goals are not to lose weight but gain the amount of Institute of Medicine recommended weight. Additionally, pre-pregnancy weight variability was found more prevalent among pregnant women who gained excessive gestational weight than those who did not gain weight excessively during pregnancy (Nagpal et al., 2020; Ölin & Rössner, 1996; Piccinini-Vallis et al., 2021). Our findings along with those from previous studies offer strong evidence that weight variability before or during pregnancy could influence maternal gestational weight outcomes.
Except for sad mood in week 6, there were no associations between weight variability and biopsychosocial factors. The absence of associations may be because the original trial targeted weight gain rather than biopsychosocial goals. It is difficult to explain why women in our study with sad mood symptoms in week 6 experienced significantly lower weight variability than those without sad mood symptoms. Among non-pregnant participants with overweight or obesity in a previous lifestyle change program, those with steady, moderate weight loss, compared to minimal-to-no or delayed-minimal weight loss, were less likely to experience depression (Romanelli et al., 2020). Our findings seem to align with this previous study. However, in our study, the association of weight variability and sad mood was not consistently positive or negative across the 8 weeks. We question whether sad mood or depression affects weight gain or variability in different directions depending on its severity level. Additional studies investigating weight variability and biopsychosocial factors in larger study samples are needed. Future studies addressing mediators or moderators that influence weight variability and depression are also recommended.
Our findings about the patterns of weight variability and its association with achieving weight gain goals have several implications. First, the weight variability measure of maximum-minimum weight was three times greater than that of ending-beginning weight. This difference could be a compensatory reaction or a self-correction of the body to regulate weight (Orsama et al., 2014). It could also mean that pregnant women experienced weight overgain and weight loss in a week. Both maximum-minimum and ending-beginning weights were associated with achieving the Institute of Medicine’s weight gain recommendations, which implies that assessing both the total weight gain and weight variability is important during pregnancy. Should a large variability be seen, preventive measures or lifestyle counseling can be instituted immediately to prevent excessive weight gain. Second, patterns of weight variability showed that over time the maximum-minimum weight variability decreased gradually, but the ending-beginning weight variability presented fluctuations. Traditionally, researchers have used the ending-beginning weight (weight difference between two time points) to evaluate the efficacy or effectiveness of weight intervention programs. Being able to reduce the magnitude of maximum-minimum weight could also serve as a matrix for intervention effects. Third, maximum-minimum weight has not been incorporated into maternal gestational weight gain research. There is a need to assess its relationships with pregnancy and infant outcomes and to establish clinical meaningful values associated with adverse outcomes. Future research may also direct attention toward investigating the influence of prenatal weight variability on postpartum weight outcomes, extending into the years following pregnancy, as well as exploring factors associated with post-pregnancy weight fluctuations, including the role of breastfeeding.
Practice Implications
Informing pregnant women of proper gestational weight gain amount based on the recommendations by the Institute of Medicine (2009) should be done by care providers during the first prenatal visit. In the subsequent prenatal visits, care providers should assess both total amount of weight gain and any weight fluctuations between two visits. Care providers may teach pregnant women to monitor their own weight at home and to report to care providers frequent weight loss and weight regain. Care providers need to educate pregnant women about the importance of keeping a steady weight gain and avoid weight fluctuations as weight variability makes it difficult to achieve the Institute of Medicine’s recommended weight outcomes. Moreover, in cases of weight variability, healthcare providers may collaborate with pregnant women to understand the reasons behind these weight fluctuations.
Limitations
This study had several limitations. Body weight and biopsychosocial data were self-reported. Study participants in our study might have overestimated or underestimated their self-reported data. We included only pregnant women whose BMIs were in the range of overweight and obesity and in a weight management intervention. The findings may not apply to other groups of pregnant women or those not in a structured weight management program. The associations of weight variability with achieving weight gain goals and biopsychosocial factors were assessed during the intervention, and thus, whether weight variability can predict weight outcomes post-intervention (e.g., at delivery or postpartum) remains unclear. Because of the secondary analysis design, we were limited to the variables originally collected in the parent study for our analysis. We did not have access to additional potential factors that could have helped explain the study findings.
Conclusion
We investigated four measures of weight variability and their associations with achieving weight gain goals and five biopsychosocial factors. Weight variability, expressed as the weight difference between the first day and the last day of a week and the difference between the highest and lowest weight in a week, was associated with achieving weekly weight gain goals. Except for sad mood in week 6, weight variability was not associated with biopsychosocial factors. The study’s findings offer evidence that both the total amount of weight gain and weight variability can impact a pregnant woman’s ability to achieve appropriate gestational weight gain. Assessing gestational weight gain and weight variability are equally important. Educating pregnant women about avoiding weight variability is crucial, as such variability may hinder their ability to reach their gestational weight gain goals.
Footnotes
Acknowledgements
The authors thank Dr. Tasneem Laila (Nina) Talib for her editorial assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.