
Abstract
The aim of this study was to investigate the impact of COVID-19 infection on disease management among individuals with type 2 diabetes and to explore their perspectives on COVID-19. This descriptive qualitative study included patients with diabetes, with a sample of 15 patients meeting the study criteria. The data were analyzed using code groups, which were then further categorized into main themes and subthemes. The main themes were: initial contact with the SARS-CoV-2 that is associated with COVID-19 illness changes in diabetes self-management behaviors; attempt at maintaining diabetes selfmanagement behaviors; and problems with accessing diabetes care. The study findings revealed several significant insights. Individuals with diabetes exhibited a fear of contracting SARS-CoV-2, which led to reduced levels of exercise and difficulties in managing blood sugar levels and insulin adjustments. Moreover, due to anxiety about COVID-19 infection, they postponed health check-ups, resulting in experiencing diabetes-related complications.
Introduction
The COVID-19 pandemic has significantly impacted people worldwide, especially those with chronic conditions like type 2 diabetes mellitus. Individuals with type 2 diabetes are at a higher risk of contracting SARS-CoV-2, the virus responsible for COVID-19 illness, and developing severe pneumonia. and developing severe pneumonia (Guo et al., 2020; X. Wang et al., 2020). During this pandemic, maintaining proper glycemic control becomes even more crucial as it can lower the risk of infection and mitigate the severity of the disease. Attaining good glycemic control is fundamental in managing type 2 diabetes and essential for reducing the risk of diabetes-related complications (Grabowski et al., 2021). Self-care practices are paramount in the management of this disease, with healthy eating, medication adherence, regular physical activity, and consistent blood sugar monitoring forming the core of these practices (American Diabetes Association [ADA], 2018; Chamberlain et al., 2016).
The restrictions imposed in numerous countries during the COVID-19 pandemic have the potential to disrupt the self-care practices of individuals with diabetes (Grabowski et al., 2021; Ruiz-Roso et al., 2020; Singhai et al., 2020; Yan et al., 2020). These individuals already face ongoing concerns about managing their diabetes, maintaining glycemic control, and dealing with potential complications in their daily lives. The added challenges posed by the pandemic may exacerbate the psychological burden on them. Several studies have documented increased levels of anxiety and worry among diabetic individuals during this pandemic (Joensen et al., 2020).
While each country handles the pandemic and delivers healthcare services differently, individuals with diabetes have encountered similar challenges across nations. Like other chronic patients, individuals with diabetes have been confined to their homes during the pandemic, leading to disruptions in their routine and emergency check-ups. This emphasizes the importance of a global effort to comprehend how disease management strategies for this group have been adapted under pandemic conditions.
In this context, the objective of this study is to explore the experiences and challenges faced by individuals with type 2 diabetes in Turkey during the COVID-19 pandemic from a qualitative perspective. The study aims to gain deeper insights into how the pandemic has impacted self-care behaviors in diabetes management and how these individuals have navigated through this unprecedented pandemic.
Methods
Study Design
Phenomenology defines the shared meaning of individuals’ experiences related to a phenomenon or concept and aims to reveal the essence of perceptions regarding these experiences. Descriptive phenomenological research designs are proposed methods to identify factors related to the phenomenon and to evaluate their impact on individuals (Creswell & Poth, 2016; Rodriguez & Smith, 2018). Therefore, this study follows a phenomenological qualitative approach, aiming to delve into the lived experiences of individuals with type 2 diabetes during the COVID-19 pandemic.
Place and Time of the Study
The interviews for this study were conducted at the Diabetes Clinic of Akdeniz University Faculty of Medicine Hospital, Department of Endocrinology and Metabolism, between August and September 2021.
Participants
The participants in this study were patients who had received treatment at the Diabetes Clinic of the Endocrinology and Metabolism Clinic. These individuals had come together for a COVID-19 training program organized at the clinic. Those who expressed interest in sharing their experiences during the COVID-19 pandemic were invited to participate in the study. The purpose and details of the study were explained to the potential participants before their inclusion.
The selection of participants followed a purposive sampling approach based on specific inclusion criteria. To be eligible for the study, participants had to meet the following criteria: (1) have type 2 diabetes for more than 1 year, (2) be able to speak and communicate effectively in Turkish, and (3) voluntarily agree to take part in the study. Patients with type 1 diabetes and those younger than 18 years old were not included in the study.
Upon conducting interviews with 15 individuals with type 2 diabetes, the study team determined that these in-depth interviews yielded valuable insights into the participants’ disease management behaviors and their perspectives on COVID-19. The collected information was sufficient to reach data saturation, ensuring a comprehensive understanding of the participants’ experiences (Townsend, 2013).
Data Collection
Data collection for this study involved face-to-face individual in-depth interviews using a semi-structured interview format. Participants were provided information about the research’s purpose, and interviews were conducted with those who willingly agreed to participate. The interviews took place in the patients’ clinic rooms, and, on average, they lasted approximately 40 minutes. All the interviews were audio-recorded and transcribed from the semi-structured interview form on the same day as the interview.
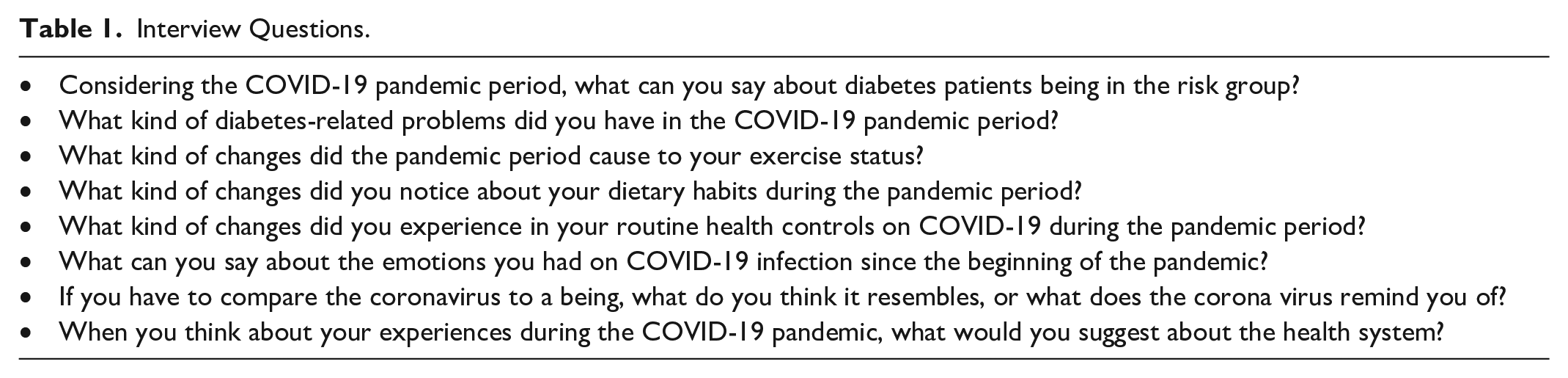
The interview questions were organized into two sections. The first section included questions about the participant’s age, gender, duration of diabetes, the reason for hospitalization, any comorbidities, and their self-measurement of blood glucose. The second section consisted of open-ended questions listed in Table 1.
Interview Questions.
Analysis and Interpretation of Data
Colaizzi’s seven-step content analysis method was employed to evaluate the data gathered from the interviews: (1) carefully reading each text to gain a general understanding of the entire content and overall perception of the participants’ experiences; (2) identifying the important statements related to phenomenology; (3) creating formulated meanings; (4) grouping the formulated meanings into clusters of themes; (5) integrating the results of the phenomenon and writing a comprehensive description; (6) comprehensive definition of the concept’s basic structure; and (7) providing feedback to participants with the results of the analysis (Colaizzi, 1978). The quotations extracted from the interviews were thoroughly read by two authors and categorized into semantic units. These semantic units were then further organized into code groups, encompassing self-management practices and daily life experiences during the curfew.
The code groups were subjected to comprehensive analysis, dividing and reassembling them to identify the main themes and subthemes that emerged from the data. To ensure the clarity and transparency of the analysis, the themes were meticulously reviewed, compared, and cross-interpreted.
To assess the consistency of the coding process, two external experts, who had no prior knowledge of the study, were asked to independently code the data. “Cohen’s kappa coefficient” was used for this assessment, as there were two coders involved in the study. The kappa coefficient measures agreement between raters, with values ranging from 0 to 1. A value of 0 indicates no agreement beyond chance, while a value of 1 represents complete agreement. Typically, a kappa value of 0.8 to 1.0 is considered excellent agreement, 0.6 to 0.8 good agreement, 0.4 to 0.6 moderate agreement, 0.2 to 0.4 slight agreement, and below 0.2 poor agreement (Viera & Garrett, 2005).
In this study, the kappa value was determined to be 1.0, signifying excellent agreement between the coders in their interpretation of the themes.
Ethics
To conduct this study, the necessary approvals were obtained from various authorities. Approval was granted by the Ministry of Health Scientific Research Platform on May 27, 2021. Ethical approval was obtained from the Akdeniz University Medical Faculty Clinical Research Ethics Committee with the reference number KAEK-518. Furthermore, legal permission was acquired from the relevant hospital to conduct the research.
Informed consent was an essential aspect of the study, and all participants were provided with a comprehensive explanation of the study’s purpose. They were informed about the details of their participation, including their rights as study subjects. In addition, participants were given clear information about whom to contact for any inquiries or questions related to the study.
Results
Characteristics of Participants
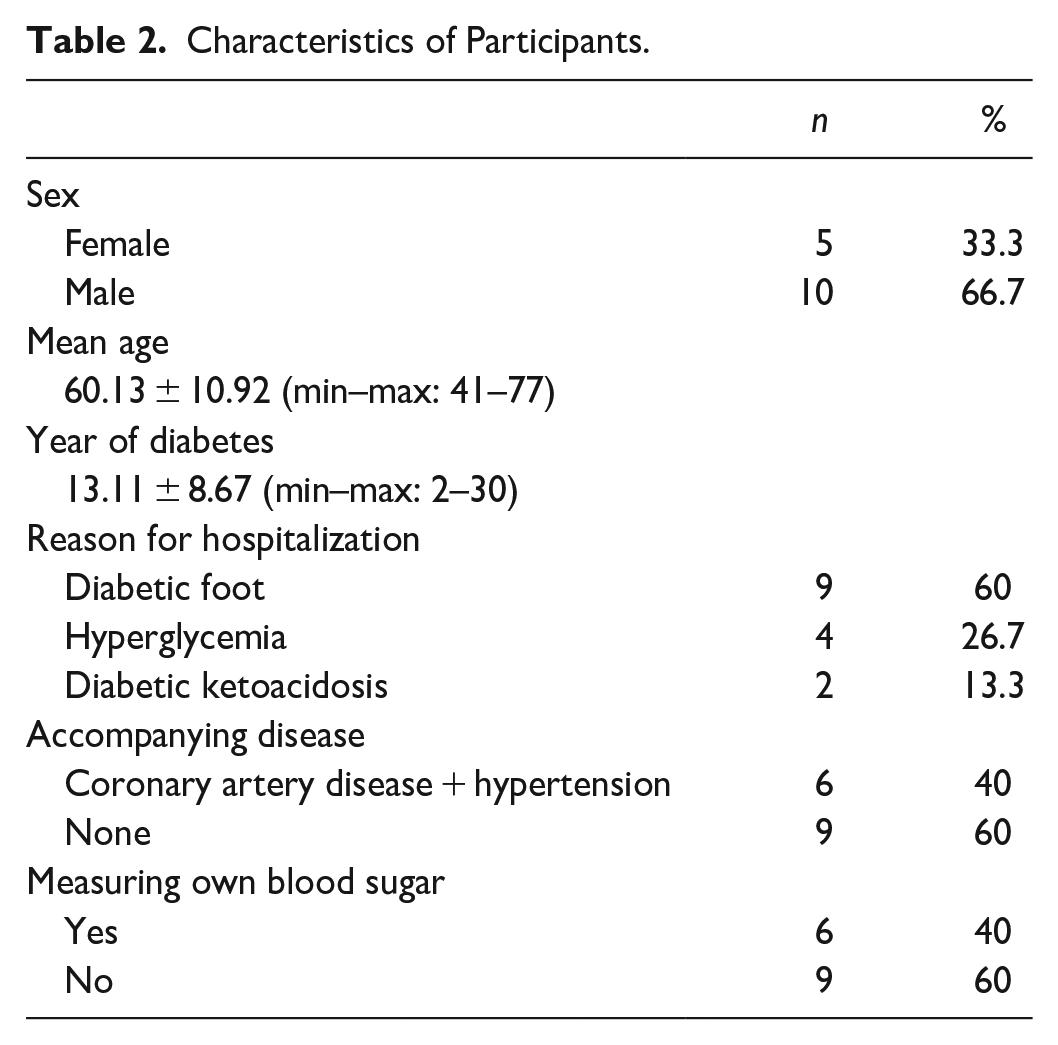
In all, 15 participants took part in this study, with 10 (66.7%) being male and 5 (33.3%) females. The participants’ ages ranged from 41 to 77 years, with a mean age of 60.13 ± 10.92 years. The duration of their diabetes varied from 2 to 30 years, with an average of 13.11 ± 8.67 years.
The hospitalization reasons for the participants were diabetic foot for nine participants (60%), hyperglycemia for four participants (26.7%), and diabetic ketoacidosis for two participants (13.3%). In addition, it was found that nine participants did not regularly measure their own blood sugar, and six participants had both hypertension and coronary artery disease as comorbidities.
A detailed summary of the participants’ characteristics is found in Table 2.
Characteristics of Participants.
Themes and Subthemes
The analysis of the patient interviews resulted in the identification of 4 main themes and 10 subthemes, as presented in Table 3.
Themes and Subthemes Determined with Disease Management Experiences of Individuals with Type 2 Diabetes.

Theme 1: Initial Contact with SARS-CoV-2 (COVID-19 illness)
Subtheme 1: Fear and anxiety
One of the key findings of this study is that individuals with diabetes experience fear and anxiety during the pandemic, much like the general population. Several participants expressed their feelings of fear and uneasiness related to the uncertain nature of the pandemic: I am afraid of suffering; I think I cannot tolerate it. (P 13) It made me worry about the future. (P 10) We were agitated, had fear and uneasiness. (P 5) We experienced fear at first, I knew it would be a big problem, then we started to get used to it. (P 11)
The participant who expressed being cautious in response to the fear and anxiety during the pandemic made the following statements: No, I thought if I was afraid, I could contact it. I devoted myself to protection. (P 4) I constantly warned to protect both my family and myself. (P 3)
Subtheme 2: Staying at home with the awareness of being in risk group
During the study, some participants mentioned adopting stricter isolation measures due to considering themselves at higher risk: I was afraid, I did not meet with anyone, I stayed in the house, but thankfully I did not have any signs of illness. I had my normal vaccinations. (P 1) I protected myself, I did not meet with anyone, I did not walk around without a mask, I did not go out. I had 2 doses of vaccines. I am having a safe process. (P 3) We stayed closed at home, protected from everything. I took my precautions because I knew myself, I was not worried. (P 4)
One participant, on the other hand, expressed the following to explain their perspective on considering themselves in the risky group and staying at home, which ultimately led to a negative outcome: I thought it was risky, I never went out. We retreated to the house, we were afraid, we closed ourselves in the house. I had a wound, we said it would get better, but it came to this. (P 13)
Subtheme 3: An ambiguous entity
Participants in the study attempted to explain the nature of SARS-CoV-2 (COVID-19 illness) using various analogies: It is a terrible thing. It is like waiting to die alive at home. Insolubility, tardiness. (P 6) It is like an insect. An invisible danger. (P 7) How electric energy is invisible and intangible but shows itself with its works, the coronavirus is something like that. (P 11)
Theme 2: Change in Diabetes Self-Management Behaviors
In the interviews with participants, it was observed that the COVID-19 pandemic brought about various changes to diabetes self-management practices, with differences observed in both the ways and degrees of these changes.
Subtheme 1: Inability to exercise due to curfew
Participants stated that their physical activity decreased significantly due to the curfew and social distancing measures. A male participant who owns a small grocery store described his level of physical activity as: Earlier, I was more active. I used to go to the store. Now I cannot walk due to weakness and fainting due to sugar drop. I stagger. I cannot walk much for fear of falling. I fell once and broke my leg. (P 8)
Another participant described as: I could not take walks, so my blood sugar started to rise. I had to make an additional dose of insulin. (P10)
Subtheme 2: Irregular medicine use
Participants reported that they did not encounter any issues with the regular use of oral antidiabetic medications. However, they had diverse experiences when it came to managing their insulin doses. A patient who was undergoing treatment for diabetic foot shared their perspective: I could not use insulin regularly. I used it on my way. I did not use insulin when my sugar was low; I used it when it was too high. As a result, I had an abnormal situation. (P 11)
Another patient, who was receiving treatment for diabetic ketoacidosis, stated: My appetite was up and down. When I felt faint, I ate too much, and in response, I increased the insulin dose. However, this led to a loss of control over my blood sugar levels. I struggled with an unbalanced diet. (P 8)
Subtheme 3: Unmanaged diabetes complications
All patients included in the study were undergoing hospital treatment for diabetes-related complications (diabetic foot n = 9; hyperglycemia n = 4, and ketoacidosis n = 2). It was noted that some patients experienced confusion resulting from blood sugar irregularities, which made it challenging for them to make appropriate decisions about their diabetes management: You know this diabetes thing? It is like a seesaw. It goes down, it goes up. It decreased to 50, it has also increased to 290. (P1) My blood sugar level increased. The biggest problem was going to the hospital and back. My blood sugar level was too high. I came here with 460. This is the problem I have the most frequently. I did not have any other problems. (P2) During this period, I had ketoacidosis, my blood sugar level increased. I had a very intense stress; I think it increased due to this. (P9) There experienced a lot of decreases and increases in my blood sugar levels. I even fell into a coma 3-4 times. I went to the hospital. There was a change in my diabetes medication. (P 5)
Patients experiencing irregular blood sugar levels alongside diabetic foot problems expressed feelings of both frustration and hopelessness: My blood sugar level did not increase very much; it went up to 200. But my intermediate blood sugar level dropped, all the way to 50 and 60. Now I have a wound on my foot. (P 13) I also had a wound on my foot, that is why I came. It happened 3 months ago and it still continues. . . I did not know what to do, it seemed to be healing, but it did not. (P 11) I came here with a blood sugar level of 387 because the wound on my foot deteriorated halfway up my knee, it was infected. Therefore, my insulin dose also increased. (P 3)
Theme 3: Attempts of Maintaining Diabetes Self-Management Behaviors
It was noted that some participants viewed the pandemic period as an opportunity and actively, tried to adapt to their current conditions.
Subtheme 1: Unchanged dietary habits
Two participants, who were vigilant about their diabetic nutrition during the pandemic, shared the following statements: I was paying attention to my diet. I am alone at home anyway, so I paid attention because I was not working during the pandemic. (P 9) I was careful. I did not eat anything sweet. (P 7)
Subtheme 2: Unchanged exercise routine
Despite the limitations imposed by the pandemic, some participants made an effort to continue exercising, albeit on a limited scale: I continued exercising without interruptions. There is a large park near our house with a 1 km walking track. I went out once every 3 days and had a walk. (P 15) When I could not go out because of the curfew, I was walking around the house. (P 13)
Theme 4: Problems with Accessing Diabetes Care
Subtheme 1: Requesting patient tracking system
Most of the patients expressed the importance of continuous follow-up by health professionals for individuals with diabetes. They emphasized the need to meet their specific needs and ensure their convenience in the healthcare process: There has to be a good tracking system. Patients should be monitored—are they nourishing adequately, taking or using their medications? Make a list if necessary. You are my patient; I will see you twice a year. Patients should be cared for individually. (P 1) Some convenience could be provided to ensure patients in the risk group who cannot leave the house are tested. (P 9) They should have come home when we made a call or we could have a video chat. We are dealing with these diseases now because we were not informed at the time. (P 6)
Some participants also mentioned positive experiences regarding access to health care during the pandemic, such as pharmacies delivering medicines to their homes, making it more convenient for them to manage their conditions: During the coronavirus pandemic, pharmacies were bringing my medicines home. It was a very positive thing. In terms of the hospital, maybe patients were going to the hospital to give blood. Health personnel could come home to give blood. (P 10) There was also a WhatsApp service of the hospital. We sent a message about the daily sugar level measurements, they directed us. We were very pleased with this situation. (P 5)
Subtheme 2: Postponing health check-ups due to the fear of contracting SARS-CoV-2 (COVID-19 illness)
Most of the patients mentioned that they avoided routine health checks, postponed their physical examination dates, and resorted to self-medication at home due to the fear of contracting SARS-CoV-2 (COVID-19 illness). Unfortunately, these actions led to negative outcomes for their health: Of course, we were afraid that we would go to the hospital and get sick. We came when the infection in the foot suddenly deteriorated. (P 7) Full closures caused this foot to become like this. We couldn’t come because we would get a penalty on the way. (P 6) We postponed coming to the hospital for the health check, so we were late in coming to the doctor, that’s why my foot got injured like this. If we had come back then, this wouldn’t have happened. If we had not experienced fear, we would have come to the hospital earlier. (P 8)
Discussion
With the onset of the COVID-19 pandemic, the entire world faced an extraordinary challenge posed by a previously unknown and highly contagious viral disease. Among the risk groups, individuals with chronic diseases like diabetes became even more vulnerable, necessitating a heightened focus on disease management. Existing evidence on diabetes management during the COVID-19 pandemic recommends measures such as monitoring glycemic control, maintaining a balanced and healthy diet, engaging in 1 hour of daily exercise at home, and adhering to medication and social distancing requirements (Wicaksana et al., 2020). In light of this, the authors aimed to determine the impact of the COVID-19 epidemic on the disease management of individuals with type 2 diabetes in this study.
The majority of participants in this study described the COVID-19 infection as an ambiguous and fearsome entity, leading them to feel worried and confined to their homes. This perception is closely related to the pathophysiological changes in individuals with diabetes, which can increase their vulnerability to infectious diseases and worsen COVID-19 symptoms (Peric & Stulnig, 2020). Being classified as a high-risk group due to their diabetes is considered the primary reason for their decision to stay at home. In support of this relationship, Yan et al. conducted a study comparing individuals with and without diabetes and found that people with diabetes expressed greater concerns about contracting SARS-CoV-2 (COVID-19 illness) and had a higher perceived risk of infection compared to those without diabetes (Yan et al., 2020). Other studies also highlighted the intense level of concern among people with diabetes regarding COVID-19 (Khader et al., 2020; Nachimuthu et al., 2020).
The impact of the COVID-19 pandemic has added complexity to the lives of individuals with diabetes, compounding the existing challenges of managing their condition. During the interviews, participants expressed disruptions in their daily routines and the need to adapt to both the pandemic and new diabetes management practices. Many interviewees reported adopting a more sedentary lifestyle, leading to a decrease in physical activity levels. This change was attributed to factors such as curfew restrictions, fear of COVID-19 infection, and social isolation, all of which negatively affected their ability to engage in regular physical activities. Studies investigating lifestyle changes in people with diabetes during curfew periods consistently found low exercise levels as a common outcome (Ghosh et al., 2020; Ruiz-Roso et al., 2020). For instance, a study conducted with individuals with type 2 diabetes reported that 69% of participants experienced a decrease in physical activity (Khader et al., 2020). Furthermore, a systematic analysis that assessed the impact of COVID-19 quarantines on physical activity and sedentary behavior revealed that 64 out of the 66 studies examined observed a decrease in physical activity and an increase in sedentary behavior (Stockwell et al., 2021).
This study demonstrated that COVID-19 curfews had a negative impact on the drug administration of individuals with diabetes. Another significant finding was that most participants did not regularly measure their blood glucose levels, and they adjusted their insulin dose randomly or based on their food intake. The participants also did not adhere to recommendations for diabetic nutrition, leading to disruptions in their blood sugar regulation and difficulties in adjusting their insulin dose accordingly. Notably, all participants were already receiving treatment at the hospital for complications related to diabetes, indicating that they were not following a diabetic diet even before the pandemic, which contributed to the development of diabetes-related complications.
Some participants in the study mentioned that they continued to uphold their diabetes self-management behaviors. The importance of proper glycemic control has been emphasized not only as the gold standard in diabetes management but also as a crucial factor in reducing the risk of COVID-19 infection and disease severity (Gupta et al., 2020; Pal & Bhansali, 2020; A. Wang et al., 2020). Several studies have investigated the impact of COVID-19 quarantine on various diabetes parameters (Ghosh et al., 2020; Grabowski et al., 2021; Nachimuthu et al., 2020). The literature reflects two common views on this matter. On one hand, numerous studies have shown that the majority of participants with both type 1 diabetes and type 2 diabetes continued to adhere to their routine diabetes behaviors, such as diet and exercise (Nachimuthu et al., 2020; Pal et al., 2020; Verma et al., 2020). On the other hand, some studies have reported an increase in snacking, the number of daily meals consumed, and the intake of sugary and general food during the pandemic (Bennett et al., 2021; Ghosh et al., 2020; Moynihan et al., 2015; Ruiz-Roso et al., 2020).
After the initial period of the pandemic, many hospitals reduced their outpatient capacity to minimize the potential spread of the virus. This change has had a significant impact on individuals with diabetes, as they are more susceptible to hospitalization for glycemic control and insulin management (Peric & Stulnig, 2020). The majority of individuals with diabetes who participated in our study mentioned that they perceived hospitals as unsafe environments and avoided routine check-ups or postponed appointments. Unfortunately, during the study, many of these participants ended up being hospitalized due to diabetes complications, with diabetic foot being particularly prevalent. It is challenging to precisely measure the full impact of COVID-19 on diabetes complications since the pandemic is still ongoing with varying severity across different regions. However, based on the limited data available, it is reasonable to assume that this situation will lead to an increase in acute and chronic complications for diabetes patients in the post-COVID-19 era. This surge in diabetes-related complications could place additional burdens on the healthcare system and may also raise the risk of COVID-19 infections in individuals with blood sugar irregularities (Ghosal et al., 2020). Given the circumstances, it is crucial to prioritize the treatment of diabetic complications, especially foot care, as it holds significant importance in preventing subsequent amputations (Peric & Stulnig, 2020).
In the study, the majority of participating patients emphasized the importance of continuous follow-up and meeting the needs of individuals with diabetes while also ensuring their convenience. Interestingly, some participants found WhatsApp services to be a positive and helpful tool. During the pandemic, one of the most effective methods for monitoring diabetes patients at home was through remote communication of their glucose measurement results to healthcare professionals, who could then adjust their antidiabetic drug doses accordingly (Kısa Mencütekin & Gençtürk, 2021). To facilitate remote diabetes care, tele-nursing services have been implemented, allowing for practices such as (Alromaihi et al., 2020) remote monitoring and “virtual visits” for individuals with diabetes (Hartmann-Boyce et al., 2020). In this context, nurses play a crucial role in managing diabetes treatment from a distance (Waizinger et al., 2021). It is worth noting that different countries have established their guidelines for routine diabetes care during the COVID-19 pandemic, resulting in variations in approaches and protocols (Polat Topçuoğlu & Ünsal Avsal, 2021). This highlights the importance of adapting healthcare services to the unique challenges and circumstances presented by the pandemic while ensuring that diabetes patients receive the necessary care and support remotely.
This study revealed the significant impact of the COVID-19 pandemic on the daily lives of diabetes patients. Interestingly, the participants reported not receiving adequate guidance on how to adapt their self-management of diabetes during the curfew periods. Consequently, they had to independently devise strategies to cope with the changes in their daily routines. As a result of these challenges, it became evident that each participant managed their diabetes at different levels, leading to a range of diabetes-related complications experienced by the individuals involved in the study.
Conclusion
Just like everyone else, individuals with diabetes faced the challenges of the pandemic and long-term curfews for the first time. During this period, it became evident that providing comprehensive information and support to patients was crucial for successful diabetes management. One effective approach to offer comprehensive care in diabetes management is by establishing integrated clinics that adopt a multidisciplinary approach. By doing so, patients can receive a well-rounded and holistic care experience. Optimal glucose control remains the gold standard in preventing acute and chronic complications, and incorporating technologies like remote individual patient monitoring systems can be a promising strategy. This approach is particularly beneficial for experienced diabetics who are adept at using technology, as it allows for easy adjustment of insulin doses without the need for face-to-face contact. For patients less familiar with technology, simpler methods like mobile phone calls and text messages can also be explored. Interestingly, the strategies developed during the constraints of the pandemic crisis have the potential to become new standards of diabetes treatment in the future. Therefore, it is essential to capitalize on the lessons learned from the COVID-19 pandemic and use this crisis as an opportunity to create innovative management strategies for patients with diabetes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.