
Abstract
Estimates of 10-49% of patients may experience ongoing symptoms after COVID-19, including dyspnea. Respiratory muscle strength training has been used to reduce dyspnea in other respiratory diseases, thus, it may be a viable option for individuals with post-COVID-19 symptoms. The objective of this review was to evaluate the evidence for the effectiveness of respiratory muscle strength training for individuals with post-COVID-19 dyspnea. A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. CINAHL, Web of Science, PubMed, EMBASE, Google Scholar, and Scopus databases were searched from 2020-2023. Eleven articles met the inclusion criteria. Pulmonary measures were improved in all but one study, and dyspnea, physical capacity and quality of life measures achieved statistical significance. Outcomes improved following respiratory muscle strength training as a standalone intervention, or with aerobic and peripheral muscle strength training.
Keywords
COVID-19-related symptoms can be persistent, estimating approximately 10%–49% of patients experiencing ongoing symptoms 3 months after resolution of the acute infection (Fortini et al., 2021; WHO, 2021; Wittmer et al., 2021). The most frequently reported post-COVID-19 symptoms include shortness of breath, fatigue, and cognitive disturbances, regardless of the severity of the acute phase of illness (Chen et al., 2022; WHO, 2021; Zhang et al., 2021). While the exact etiology of lung impairment for COVID-19 remains unclear, evidence suggests that prolonged inflammation, alveolar epithelial and endothelial cell injury, fibroproliferation, and chronic vascular and alveolar remodeling may be responsible (Siso-Almirall et al., 2021; Zhang et al., 2021). Radiologic evidence of lung fibrosis, pulmonary scarring, and interstitial changes have been associated with persistent dyspnea in Long COVID-19 (Yong, 2021). Recent studies hypothesize that the COVID-19 infection may specifically cause damage, resulting in weakness in the respiratory musculature (Severin et al., 2022).
Respiratory muscle strength training may prove to be a viable option for individuals with persistent dyspnea following COVID-19 infection. Respiratory muscle strength training is known to lead to improved respiratory muscle efficiency, allowing for a reduction in the amount of oxygen needed to perform the work of breathing (Held & Pendergast, 2014). The resulting reduction in muscle fatigue, sympathetic nervous system activation, and lactate levels as a result of respiratory training lessens the vasoconstriction that otherwise occurs during physical activity (Illi et al., 2012).
Varying approaches designed to strengthen the respiratory muscles by stretching and resistance training that targets the respiratory muscles have been detailed in patients with respiratory weakness (Basso-Vanelli et al., 2016; Sapienza, 2008). Inspiratory and expiratory muscle strength training have demonstrated improvements in dyspneic symptoms and quality of life (QoL) in other chronic respiratory illnesses (Budweiser et al., 2006; Graur et al., 2022; Lu et al., 2020), and in more recent studies of patients post-COVID-19 (Del Corral et al., 2023a; Liu et al., 2020) but the protocols are inconsistent, hindering comparison for effectiveness. While traditional pulmonary rehabilitation programs can be helpful, there are limitations to program access due to the strain the COVID-19 pandemic has placed on these resources (Dixit et al., 2021). Lastly, the gold standard for the most effective pulmonary exercise strategy remains unestablished. Home-based programs that overcome barriers to access may be an important strategy for managing persistent dyspnea following COVID-19 infection (Dixit et al., 2021).
Objective
The aim of this systematic review was to evaluate the evidence for the effectiveness of respiratory muscle strength training for patients post-COVID-19. This review draws upon interventional studies focused on this population, to determine the most current evidence for respiratory muscle strength training. We address the respiratory muscle strength protocols and the reported outcomes for pulmonary measures, dyspnea, physical capacity, and QoL.
Methods
This review was performed according to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (Page et al., 2020) and has been registered as CRD42022361676 under PROSPERO.
Search Strategy
A three-step search strategy was used with the support of the University librarian. An initial search of PubMed was carried out, as well as an analysis of the text words in the titles and abstracts. A second search was conducted using the identified keywords and index terms across six databases including CINAHL, Web of Science, PubMed, EMBASE, Scopus, as well as Google Scholar. Only studies published in English were considered for inclusion, and the search included studies conducted from 2020 to 2023. The search strategies used for the databases are detailed in Appendix 1. The reference lists of articles selected for appraisal were searched for additional studies.
Study Selection
Once duplicates were removed, two investigators independently screened the titles and abstracts against the inclusion criteria. The full texts of 102 potentially eligible studies were retrieved and assessed in detail against the inclusion criteria by two independent reviewers. Full-text studies that did not meet the inclusion criteria were excluded. Any disagreement that arose between the reviewers was resolved through discussion.
Inclusion and Exclusion Criteria
Studies were included if they (1) focused on individuals with post-COVID-19 and dyspnea, (2) were randomized controlled trials, quasi-experimental, prospective, cohort studies, or observational studies, (3) used a pulmonary rehabilitation intervention that included respiratory muscle strength training, (4) reported pulmonary, dyspnea, physical capacity, or QoL outcomes, (5) over the age of 18 years, (6) written in English, and (7) published between the years of 2020 to present. Studies were excluded if they did not involve a respiratory muscle strength training intervention that included pulmonary, dyspnea, physical capacity, or QoL outcomes in adults, not written in English, reviews, or secondary data analysis reviews.
Assessment of Methodological Quality
Studies meeting the inclusion criteria were assessed by two independent reviewers using standardized critical appraisal instruments for randomized and non-randomized controlled trials. The quality assessment tool for quantitative studies by the effective public health practice project (EPHPP) (Thomas et al., 2004) was used as the assessment tool to evaluate the methodological quality of the studies selected for this review. This instrument provides a standardized method to evaluate study quality. An overall quality rating using a scale of high, moderate, and weak in seven areas (i.e., selection bias, study design, confounders, blinding, data collection methods, and withdrawals and drop-outs) is scored. The Oxford Center for Evidence-Based Medicine Levels of Evidence (OCEBM) instrument was used to evaluate the level of evidence for each study. The OCEBM tool was designed to be able to rate the level of evidence in the research studies for therapeutic effects, on a scale of 1 through 5 (Howick et al., 2011). Level 1 indicates the highest level of evidence, which is a systematic review, to a 5 which indicates mechanistic thinking. Two independent reviewers evaluated the data, and discrepancies were resolved through discussion with a third reviewer.
Data Extraction
One reviewer extracted data from included papers using an adapted data extraction tool, while a second reviewer cross-referenced the extracted data. The data extracted included patient characteristics, study methods, outcomes of significance, and details of the study interventions. Any disagreements that arose between the reviewers were resolved through discussion.
Data Analysis
Data analysis was carried out using a method of constant comparison where data were examined in categories to allow visualization of the outcomes. The included studies were grouped by randomized versus non-randomized study designs within the evidence tables, and further grouped into three broad outcome categories: pulmonary function and dyspnea, physical capacity, and QoL. Home-based respiratory muscle strength training versus facility-based rehabilitation settings that included aerobic and peripheral muscle strength training were grouped to compare outcomes. Although the heterogeneous nature of the interventions and measurement tools used precluded the use of meta-analysis, the synthesis of data outcomes was assessed where appropriate.
Results
Study Inclusion
A total of 6,328 articles were identified in the search. After the exclusion of 3,642 duplicates, non-English, or non-respiratory-focused articles, 2,686 articles were screened by title and abstract. Four additional articles were obtained from reference lists. In all, 102 articles were full text reviewed. In all, 91 articles were excluded because they did not include respiratory muscle strength training within the interventions, or they were not measuring the specific variables; pulmonary measures and dyspnea, physical capacity, and QoL. In all, 11 studies were ultimately included in this review (Figure 1).
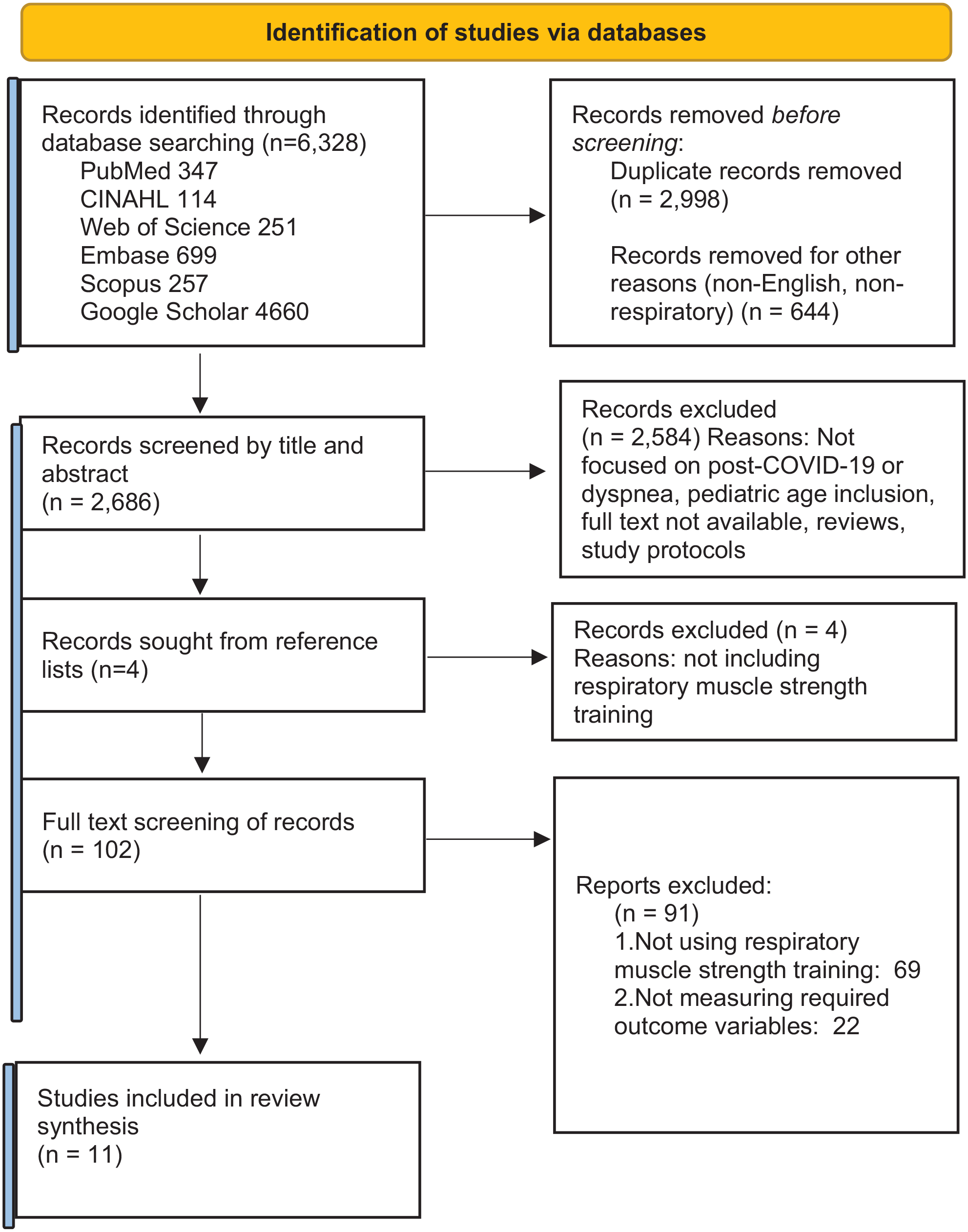
Flow diagram of literature search.
Methodological Quality
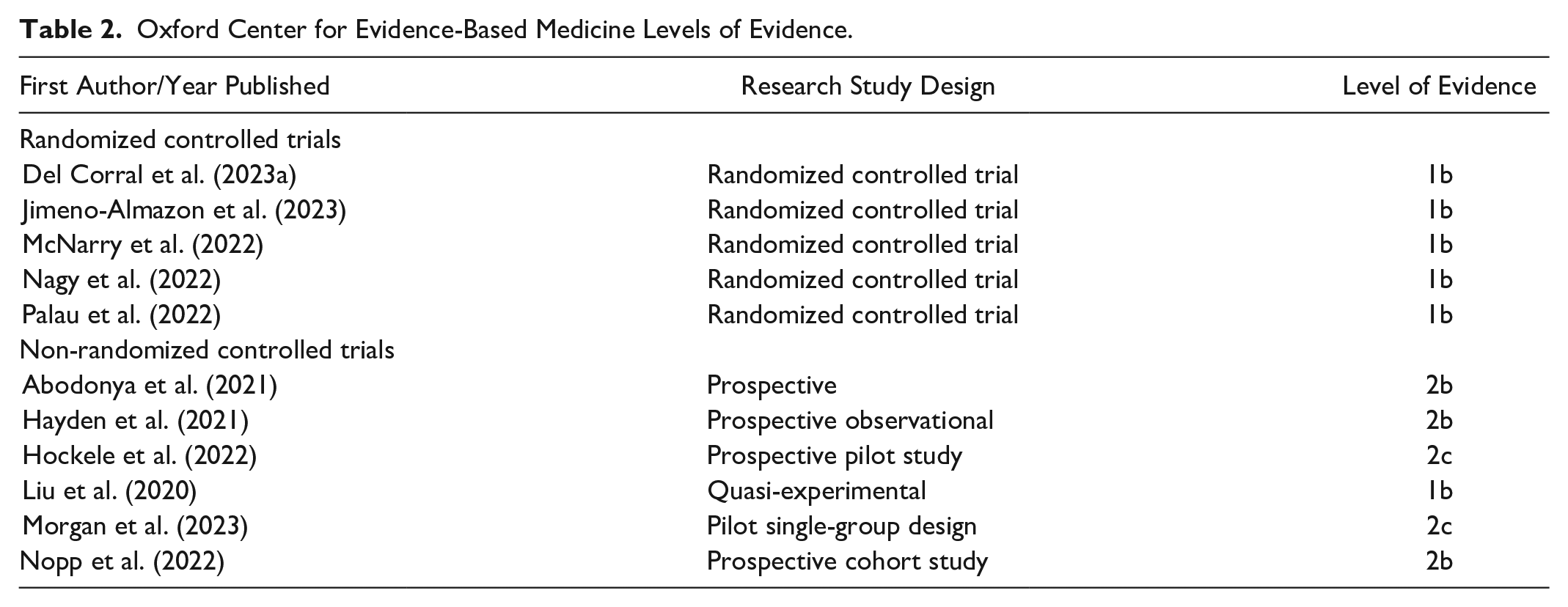
Using the EPHPP tool, 4 (36%) of the studies received strong ratings, and 7 (64%) received moderate ratings. Some studies did not mention or have blinding processes related to study design, leading to n/a ratings in this category (Table 1). Using the OCEBM instrument to evaluate the level of evidence for each study, six of the studies had a 1b level of evidence (Del Corral et al., 2023a; Jimeno-Almazan et al., 2023; Liu et al., 2020; McNarry et al., 2022; Nagy et al., 2022; Palau et al., 2022), three had a 2b level of evidence (Abodonya et al., 2021; Hayden et al., 2021; Nopp et al., 2022), and two had a 2c level of evidence (Hockele et al., 2022; Morgan et al., 2023) (Table 2). These relatively high levels of methodological quality led to the inclusion of these studies in the review.
Qualitative Assessment Tool for Quantitative Studies, Effective Public Health Practice Project.
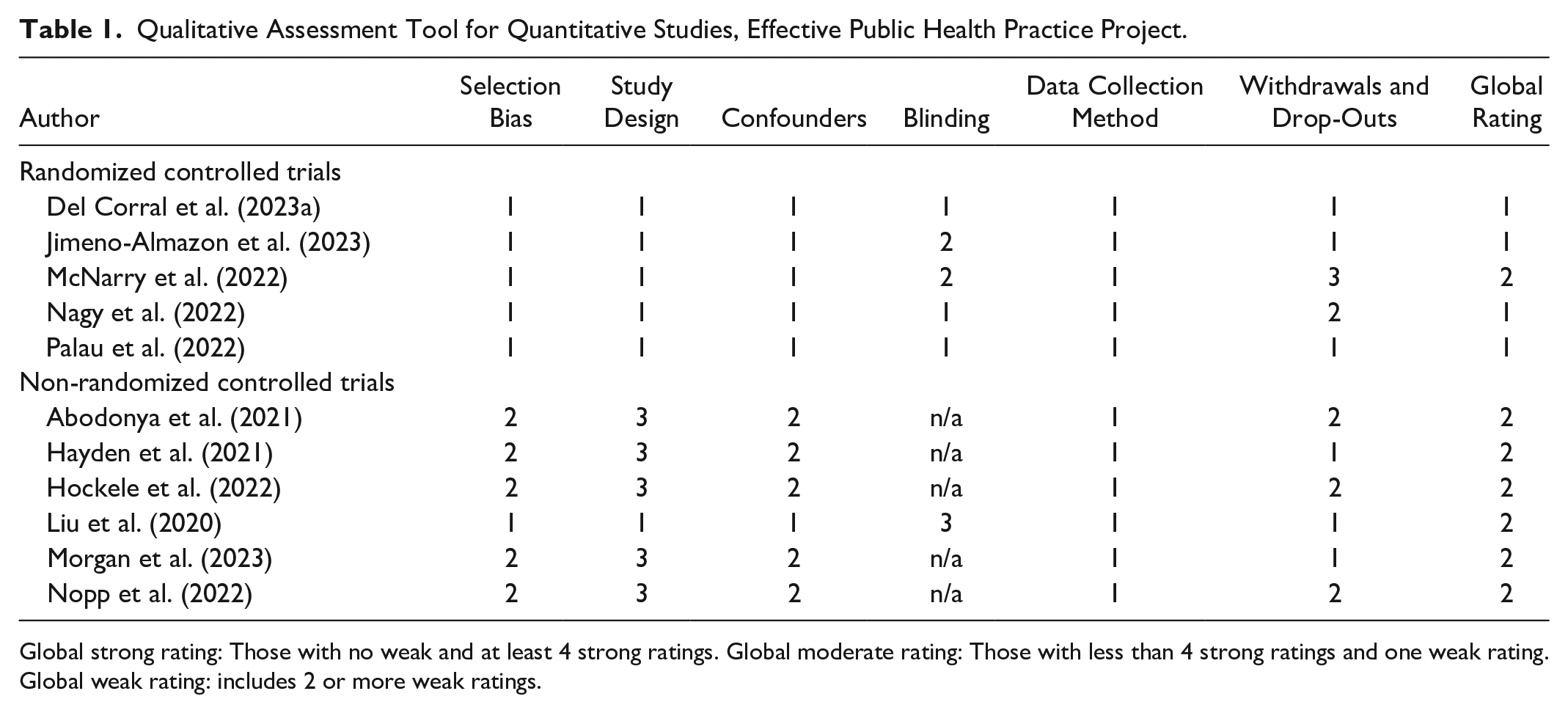
Global strong rating: Those with no weak and at least 4 strong ratings. Global moderate rating: Those with less than 4 strong ratings and one weak rating. Global weak rating: includes 2 or more weak ratings.
Oxford Center for Evidence-Based Medicine Levels of Evidence.
Characteristics of Included Studies
Among the 11 included studies, five were randomized controlled trial studies (Del Corral et al., 2023a; Jimeno-Almazan et al., 2023; McNarry et al., 2022; Nagy et al., 2022; Palau et al., 2022), one was quasi-experimental (Liu et al., 2020), and five were prospective (Abodonya et al., 2021; Hayden et al., 2021; Hockele et al., 2022; Morgan et al., 2023; Nopp et al., 2022). All of the studies focused on respiratory muscle strength training in individuals experiencing post-COVID-19 symptoms, with four including an aerobic or peripheral strengthening exercise component in the intervention (Hayden et al., 2021; Hockele et al., 2022; Liu et al., 2020; Nopp et al., 2022), and one including a diaphragmatic release intervention (Nagy et al., 2022).
In total, 855 individuals were included in this analysis, covering nine countries. All participants were adults, with an average age of 51.09 years. There was little consistency among studies in relation to research design, interventions, and the measurement instruments used. Duration of the study interventions ranged from 2 to 12 weeks, while performance frequency of the respiratory interventions included daily, twice daily, or three times per week (Table 3). Therefore, the main findings of this systematic review were synthesized and grouped into three main themes related to participant outcomes following respiratory muscle-strengthening interventions:
(1) Pulmonary function and dyspnea
(2) Physical capacity
(3) QoL
Characteristics, Interventions, and Outcomes of Included Studies by Study Design.
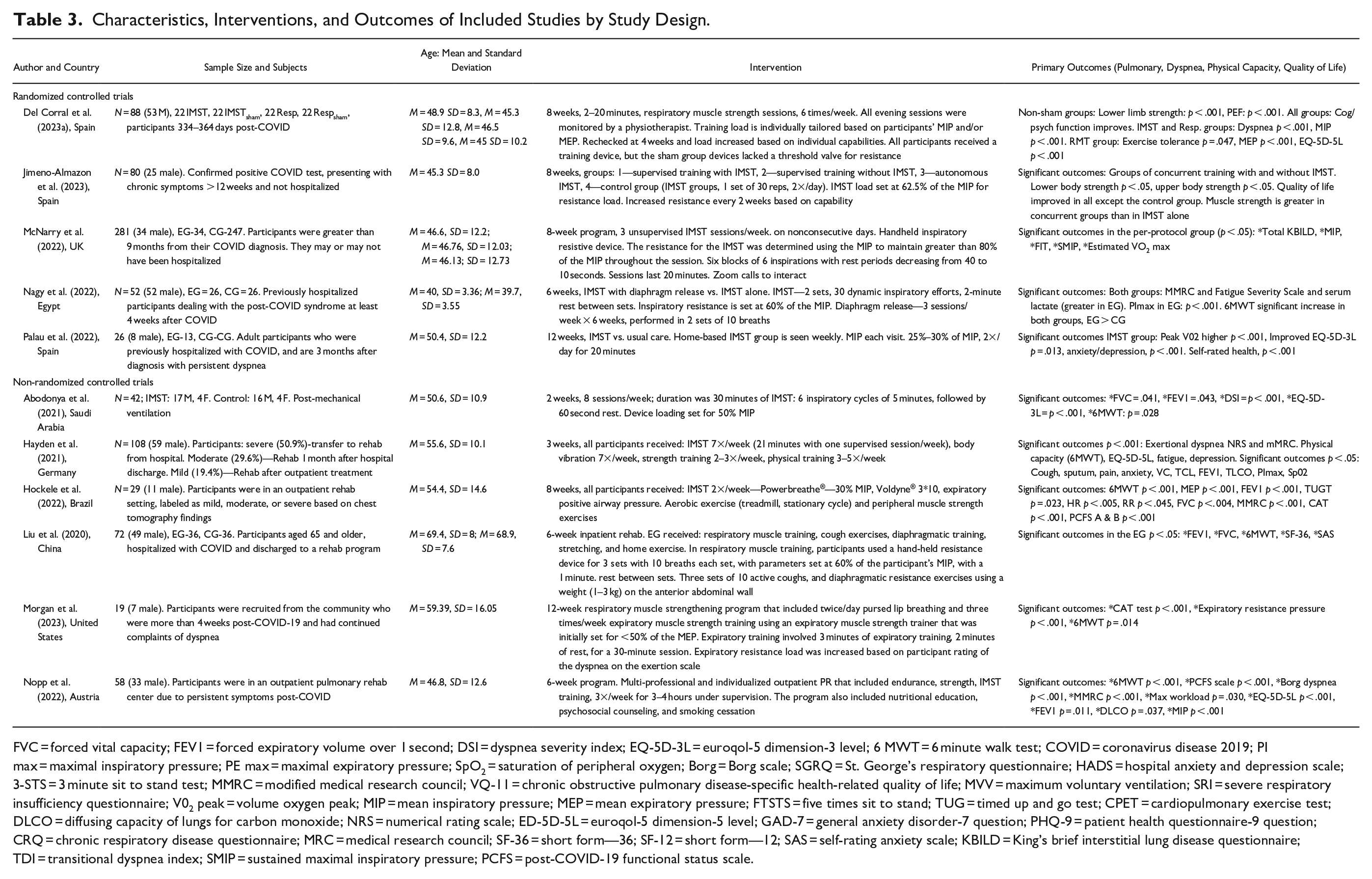
FVC = forced vital capacity; FEV1 = forced expiratory volume over 1 second; DSI = dyspnea severity index; EQ-5D-3L = euroqol-5 dimension-3 level; 6 MWT = 6 minute walk test; COVID = coronavirus disease 2019; PI max = maximal inspiratory pressure; PE max = maximal expiratory pressure; SpO2 = saturation of peripheral oxygen; Borg = Borg scale; SGRQ = St. George’s respiratory questionnaire; HADS = hospital anxiety and depression scale; 3-STS = 3 minute sit to stand test; MMRC = modified medical research council; VQ-11 = chronic obstructive pulmonary disease-specific health-related quality of life; MVV = maximum voluntary ventilation; SRI = severe respiratory insufficiency questionnaire; V02 peak = volume oxygen peak; MIP = mean inspiratory pressure; MEP = mean expiratory pressure; FTSTS = five times sit to stand; TUG = timed up and go test; CPET = cardiopulmonary exercise test; DLCO = diffusing capacity of lungs for carbon monoxide; NRS = numerical rating scale; ED-5D-5L = euroqol-5 dimension-5 level; GAD-7 = general anxiety disorder-7 question; PHQ-9 = patient health questionnaire-9 question; CRQ = chronic respiratory disease questionnaire; MRC = medical research council; SF-36 = short form—36; SF-12 = short form—12; SAS = self-rating anxiety scale; KBILD = King’s brief interstitial lung disease questionnaire; TDI = transitional dyspnea index; SMIP = sustained maximal inspiratory pressure; PCFS = post-COVID-19 functional status scale.
Pulmonary Function and Dyspnea
All but two studies used a pulmonary function measure as an indicator, comparing pre- and post-intervention means (Jimeno-Almazan et al., 2023; Palau et al., 2022). The included studies reported at least one significant pulmonary outcome measure post-intervention, except one (Morgan et al., 2023).
Forced Vital Capacity
Three studies reported significant improvements in the forced vital capacity (FVC) (Abodonya et al., 2021; Hockele et al., 2022; Liu et al., 2020). One of these studies was a 2-week, home-based inspiratory muscle strength training (IMST) program that focused on respiratory muscle strength training alone, in participants who had previously been mechanically ventilated (Abodonya et al., 2021), while the other two studies used IMST combined with aerobic exercise and peripheral muscle strength training (Hockele et al., 2022; Liu et al., 2020).
Forced Expiratory Volume Over One Second
Five studies reported significant increases in the forced expiratory volume over one second (FEV1) (Abodonya et al., 2021; Hayden et al., 2021; Hockele et al., 2022; Liu et al., 2020; Nopp et al., 2022). All five of these studies utilized IMST within their interventions, and four also included aerobic and peripheral muscle strength training (Hayden et al., 2021; Hockele et al., 2022; Liu et al., 2020; Nopp et al., 2022).
Maximal Inspiratory Pressure
Four studies reported significant outcomes in maximal inspiratory pressure (MIP) (Del Corral et al., 2023b; McNarry et al., 2022; Nagy et al., 2022; Nopp et al., 2022). All four studies incorporated IMST with two studies using IMST alone A recent randomized controlled trial reported a minimally clinical important difference (MCID) value of 18 cm H20 for the MIP within the post-COVID-19 population in an attempt to assess whether the improvements noted in MIP are clinically meaningful (Del Corral et al., 2023b). In this review, all four studies exceeded the reported MCID for MIP.
Maximum Expiratory Pressure
Two studies reported statistically significant increases in maximum expiratory pressure (MEP) (Del Corral et al., 2023a; Hockele et al., 2022). MEP was found to have the largest effect outcome (0.8 ≥ d) in the randomized controlled trial group that performed both IMST and expiratory muscle strength training (EMST) (Del Corral et al., 2023a).
Dyspnea
Dyspnea was measured in all but three of the included studies (Liu et al., 2020; Morgan et al., 2023; Palau et al., 2022). The MCID for patient-reported dyspnea has not yet been established for the post-COVID-19 population, but for the five studies that used the modified Medical Research Council Dyspnea Scale (Hayden et al., 2021; Hockele et al., 2022; Jimeno-Almazan et al., 2023; Nagy et al., 2022; Nopp et al., 2022), outcomes exceeded the MCID of −1 that is reported in the chronic obstructive pulmonary disease (COPD) population (Ammous et al., 2023). All studies that reported dyspnea scores reported statistically significant improvements in dyspnea ratings in the respiratory muscle strength training groups (Table 3).
Physical Capacity
The physical capacity of participants was found to be significantly improved post-intervention in the included studies. Three different physiologic measurement strategies were used to determine physical capacity. Seven of the studies used the 6-minute walk test (6MWT) (Abodonya et al., 2021; Hayden et al., 2021; Hockele et al., 2022; Liu et al., 2020; Morgan et al., 2023; Nagy et al., 2022; Nopp et al., 2022), three measured cardiorespiratory fitness (Del Corral et al., 2023a; Jimeno-Almazan et al., 2023; Palau et al., 2022), and one used V02 max (McNarry et al., 2022). The MCID for the 6MWT has not yet been established for the post-COVID-19 population. However, in those studies that used the 6MWT to measure physical capacity, outcomes ranged from 42.1 to 119.1 m post-intervention, which exceeds the reported MCID of 30 m for the 6MWT in those with chronic lung disease (Singh et al., 2014). Five studies used a home-based respiratory muscle-strengthening exercise as a standalone intervention (Abodonya et al., 2021; Del Corral et al., 2023a; McNarry et al., 2022; Morgan et al., 2023; Palau et al., 2022).
Quality of Life
Health-related QoL instruments were used to measure the impact of respiratory muscle strength training on QoL in all but one study (Nagy et al., 2022). A recently published randomized controlled trial placed participants into four different groups. These groups included a supervised rehabilitative training program with IMST, without IMST, IMST alone, or a control group in which participants received a pamphlet. QoL scores were significantly improved in all post-interventional groups, but not the control group. In addition, the groups that included rehabilitative training with and without IMST reported the largest QoL effect sizes (Jimeno-Almazan et al., 2023). Another recent randomized controlled trial placed participants in one of four groups (IMST alone, sham IMST, IMST plus EMST, and sham IMST plus EMST training). Both the IMST alone and the IMST plus EMST groups demonstrated a significant improvement in QoL when compared to the sham groups. However, the combined IMST and EMST training group reported the largest clinically important increase in QoL outcomes (Del Corral et al., 2023a). The two studies that measured QoL using the COPD assessment test reported statistically significant improvements post-intervention that were greater than the established MCID of four that had been established in the COPD population (Hockele et al., 2022; Morgan et al., 2023). One randomized controlled trial that measured QoL outcomes using King’s brief interstitial lung disease questionnaire did not find significant outcomes in the total QoL score following the intervention; however, statistically significant improvements were found in the breathlessness and activities and psychological domains (McNarry et al., 2022). Despite the variability of the study designs and the health-related QoL tools that were used, studies that measured QoL reported statistically significant improvements in QoL scores post-intervention (Table 3).
Discussion
The purpose of this systematic review was to examine the effect of respiratory muscle strength training in individuals with post-COVID-19 dyspnea. Based on the methodological quality of the included studies, there is a high level of confidence in these findings. Despite the heterogeneity of the interventions, measurements, and study designs, the outcomes demonstrated improvements post-intervention.
The pulmonary function measures examined in this review demonstrated positive effects in those participants who received the respiratory muscle-strengthening intervention in all but one study (Morgan et al., 2023). In this home-based pilot study, there was no difference in the FEV1 following the EMST intervention. This may be attributed to the small sample size, and that the intervention included EMST with pursed lip breathing only. Inspiratory rib cage muscles actively promote rib cage expansion; thus, focusing training on the inspiratory muscle groups as well as expiratory muscle groups may be more effective in achieving significant pulmonary function outcomes (Illi et al., 2012). IMST has been shown to reduce the impact of the respiratory metaboreflex in other respiratory conditions, thereby increasing exercise tolerance and respiratory muscle strength (Witt et al., 2007), which may describe the positive pulmonary function outcomes reported in participants with post-COVID-19 who received IMST. It is important to note that improved pulmonary function outcomes occurred whether the IMST interventions were used alone as a home-based intervention, or if aerobic and peripheral muscle strength training was included.
Persistent dyspnea is a major concern for individuals suffering from post-COVID-19 symptoms (Fortini et al., 2021; Siso-Almirall et al., 2021). Dyspnea is linked to respiratory muscle weakness such that when respiratory muscles are weakened, the additional effort required to perform the work of breathing triggers the increased feeling of breathlessness (Fukushi et al., 2021). Respiratory muscle exercise training has been found to improve energy conservation, decrease muscle fatigue, and improve oxygen saturation and blood flow (Dixit et al., 2021). IMST specifically has been reported to improve respiratory muscle strength and blood oxygenation in patients with COPD, which, in turn, reduces dyspnea (Mehani, 2017). A recent literature review that included patients with post-COVID-19 symptoms who underwent pulmonary rehabilitative strategies that included breathing exercises, peripheral strength training, and respiratory muscle training reported significant improvements in self-reported dyspnea (Kolodziej et al., 2021). This coincides with the studies in this review that respiratory muscle strength training that includes IMST alone, or in combination with aerobic and peripheral muscle strength training, reduces persistent dyspnea in individuals with post-COVID-19.
All included studies in this review reported statistically significant improvements in physical capacity. Respiratory muscle strength training is known to increase the work efficiency of the respiratory muscles, reducing blood supply competition to the lower extremities (Held & Pendergast, 2014). Subsequently, reduced respiratory muscle fatigue can improve overall physical capacity (Illi et al., 2012). Respiratory muscle strength training in patients with chronic obstructive lung disease has historically demonstrated improved exercise tolerance and endurance by targeting the diaphragmatic and intercostal muscles (Mehani, 2017). More specifically, IMST improves respiratory muscle strength, endurance, and exercise capacity in patients with COPD (Dixit et al., 2021) and interstitial lung disease (Dowman et al., 2021). A meta-analysis of three studies involving patients with post-COVID-19 pooled the distance walked in the 6MWT following a respiratory training intervention. A statistically significant improvement was found, regardless of the variability in duration, population, and intensity of the respiratory interventions used (Chen et al., 2022). Similarly, the included studies in this review demonstrated significantly improved physical outcomes following the use of respiratory muscle strength training as a standalone intervention, or in combination with aerobic and peripheral muscle strengthening interventions.
Although all included studies that measured QoL reported statistically significant improvements, one study did not achieve statistical significance in the total QoL score. Attrition and protocol concerns may have impacted the total score outcomes (McNarry et al., 2022). A recent systematic review of patients post-COVID-19 following pulmonary rehabilitation described significant QoL improvements post-respiratory rehabilitation (Fugazzaro et al., 2022). QoL improvements have also been reported in patients with COPD (Tout et al., 2013), interstitial lung disease (Dowman et al., 2021), bronchiectasis (Pehlivan et al., 2019), and asthma (Renolleau-Courtois et al., 2014), following respiratory muscle-strengthening exercise. Individuals experiencing persistent dyspnea, exercise intolerance, fatigue, and decreased pulmonary function may experience a reduction in QoL. Thus, it is reasonable to consider that physiologic improvements related to respiratory muscle strength training can improve health-related QoL outcomes.
Implications for Clinical Practice
Current evidence suggests that there are benefits associated with the performance of respiratory muscle strength training in the post-COVID-19 population. The number of randomized controlled trials being published related to post-COVID-19 symptomology is increasing with growing evidence that supports targeting the respiratory musculature with exercise to reduce dyspnea. Home-based studies that used respiratory muscle strength training as a standalone intervention found statistically significant improvements in pulmonary function and dyspnea, physical capacity, and QoL measures. Thus, respiratory muscle strength training may be an efficient and efficacious treatment that can be used to reach individuals experiencing persistent dyspnea. However, additional research is recommended to determine the optimum dose and duration.
Strengths and Limitations
A strength of this systematic review was using the PRISMA guidelines to support the data collection and appraisal process, including only studies published in peer-reviewed journals, registration of the study in PROSPERO, and the large number of participants evaluated. Specified inclusion and exclusion criteria helped to drive consensus on data extraction, appraisal, and summarizing of the findings. Another strength of this review was the methodological quality of the included studies. The level of evidence in the included studies in this review ranged from moderate to strong. However, the wide heterogeneity of the intervention protocols and measurement instruments limited the analysis. Less than half of the included studies were randomized controlled trials; thus, the lack of control groups, randomization, and blinding of patients and assessors within some of the studies may have undermined the reliability and validity of the results.
Conclusion
The findings of this review suggest that respiratory muscle strength training demonstrates clinical improvements in pulmonary function, dyspnea, physical capacity, and QoL in individuals post-COVID-19. In addition, home-based rehabilitation programs that use respiratory muscle strength training demonstrate beneficial outcomes and may serve to increase the ability to reach patients who might otherwise be unable to receive rehabilitation.
Supplemental Material
sj-docx-1-cnr-10.1177_10547738231201994 – Supplemental material for Respiratory Muscle Strength Training in Patients Post-COVID-19: A Systematic Review
Supplemental material, sj-docx-1-cnr-10.1177_10547738231201994 for Respiratory Muscle Strength Training in Patients Post-COVID-19: A Systematic Review by Sandra P. Morgan, Constance Visovsky, Bini Thomas and Aimee B. Klein in Clinical Nursing Research
Footnotes
Acknowledgements
The content is solely the responsibility of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Conduct of Research
This is a systematic review article and does not require institutional review board approval.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.