
Abstract
The aim of this study was to estimate the prevalence of metabolic syndrome (MetS) in a Spanish rural population and assess differences in prevalence according to loneliness level, social isolation, and social support. This is a cross-sectional study of 310 patients. MetS was defined by National Cholesterol Education Program–Third Adult Treatment Panel. The UCLA (University of California, Los Angeles) Loneliness Scale, Multidimensional Scale of Social Support, and Lubben Social Network Scale were used to assess loneliness, perceived social support, and social isolation. Almost half of the participants fulfilled MetS diagnosis criteria. Subjects with MetS showed significantly higher levels of loneliness, less social support, and greater social isolation. Systolic blood pressure was significantly higher in socially isolated rural adults. Environmental factors may play a key role in the prevalence of MetS, so specific screening and prevention programs could help health professionals prevent the increasing rates of MetS in rural populations under these socially specific conditions of vulnerability.
Introduction
Metabolic syndrome (MetS) comprises a group of at least three of five cardiometabolic abnormalities: high blood pressure, central obesity, insulin resistance, elevated blood triglycerides, and atherogenic dyslipidemia (Rojas et al., 2021). This syndrome is a complex pathological state with incidence similar to that of a global epidemic. In Europe, the prevalence of MetS is 41% in men and 38% in women, whereas, in Spain, it has been estimated at nearly 31% of all adults (Gallardo-Alfaro et al., 2020; Ling et al., 2020). This is especially relevant since MetS increases the risk of all-cause mortality by 1.5 and also represents a risk factor for the onset of chronic non-communicable degenerative diseases, including cardiovascular diseases (CVD), type 2 diabetes mellitus, chronic kidney disease, and some types of cancer (Gallardo-Alfaro et al., 2020; Rojas et al., 2021). Complex interactions between the genetic and epigenetic makeup of an individual with environmental factors are reported to be responsible for the pathophysiology of MetS (Ramzan et al., 2021; Tsao et al., 2020). However, the exact etiology underpinning the development of MetS remains to be fully established (Ramzan et al., 2021).
MetS is now both a public health concern and a clinical problem (Tsao et al., 2020). For this reason, patient diagnosis is important to improve the outcomes of the disease by applying lifestyle and risk factor modifications (Ahmed et al., 2022). Numerous studies in the United States, South Africa, Korea, and China have identified a higher prevalence of MetS among rural populations (Lan et al., 2018; Nowicki et al., 2021). The Prospective Urban and Rural Epidemiological Study, Poland found that within the group of people with MetS there were more rural residents (Czekajło et al., 2019). Similarly, Nowicki et al. found that people residing in rural areas had an approximately 30% higher probability of developing MetS compared to urban residents (Nowicki et al., 2021).
In parallel with the epidemic of metabolic disorders, loneliness and social isolation are also being recognized as epidemics within our societies due to their rapid increase. Loneliness and social isolation occur in approximately one-third or more of older adults, with 5% often or always feeling lonely (Iamtrakul & Chayphong, 2022). People in rural areas may be at particular risk of loneliness. In addition to many rural areas being physically and socially isolated, rural residents are more likely than urban residents to report being in fair or poor health and are more likely to have certain chronic health conditions (Abshire et al., 2022). In this line, recent studies have highlighted the adverse effects that social isolation and loneliness have on the health and quality of life of subjects, leading to a clear deterioration of both (Hernández-Ascanio et al., 2022).
The terms social isolation and loneliness are interrelated but describe different concepts. Social isolation has been defined as “the objective characteristics of one’s relationships and refers to shortcomings in the size of their social network,” whereas loneliness has been described as “the distressing subjective experience of lacking relationships or missing a certain level of quality in them” (Winterton et al., 2020). Living in a remote or rural location has been found to be a substantial risk factor for social isolation and loneliness, with many rural residents experiencing intense and chronic feelings of loneliness. Risk factors can be exacerbated by the geographic challenges inherent in accessing services due to inflexible or limited public transport links (Kelly et al., 2019).
It is well established that less social support, loneliness, and social isolation are risk factors for all-cause morbidity and mortality with outcomes comparable to other risk factors such as smoking, lack of exercise, obesity, and high blood pressure (Fakoya et al., 2020). A lack of social support and social disengagement or feelings of loneliness are closely linked to CVD, depression, dementia, disability, cognitive decline, and mortality (Mehrabi & Béland, 2020). Interestingly, a few recent studies evidence that environmental factors such as social support, loneliness, and social isolation may affect the prevalence of MetS (Badcock et al., 2019; Kim et al., 2021; Winterton et al., 2020).
In this context and considering that MetS represents a major public health concern that may be influenced by environmental factors such as loneliness, social isolation, and low levels of social support, the aim of this study was to estimate the prevalence of MetS in a rural population in Spain and to investigate the differences in prevalence according to loneliness levels, social isolation, and social support, specifically in a rural population.
Material and Methods
Study Population
This cross-sectional study was conducted using residents in a rural area of Spain (Nerpio, Castilla la Mancha) from October 2021 to April 2022. A total of 350 patients >18 years of age were screened for participation after nursing consultations. In all, 19 patients were deemed ineligible and 21 patients declined to participate. A flow diagram of participant recruitment is shown in Figure 1.
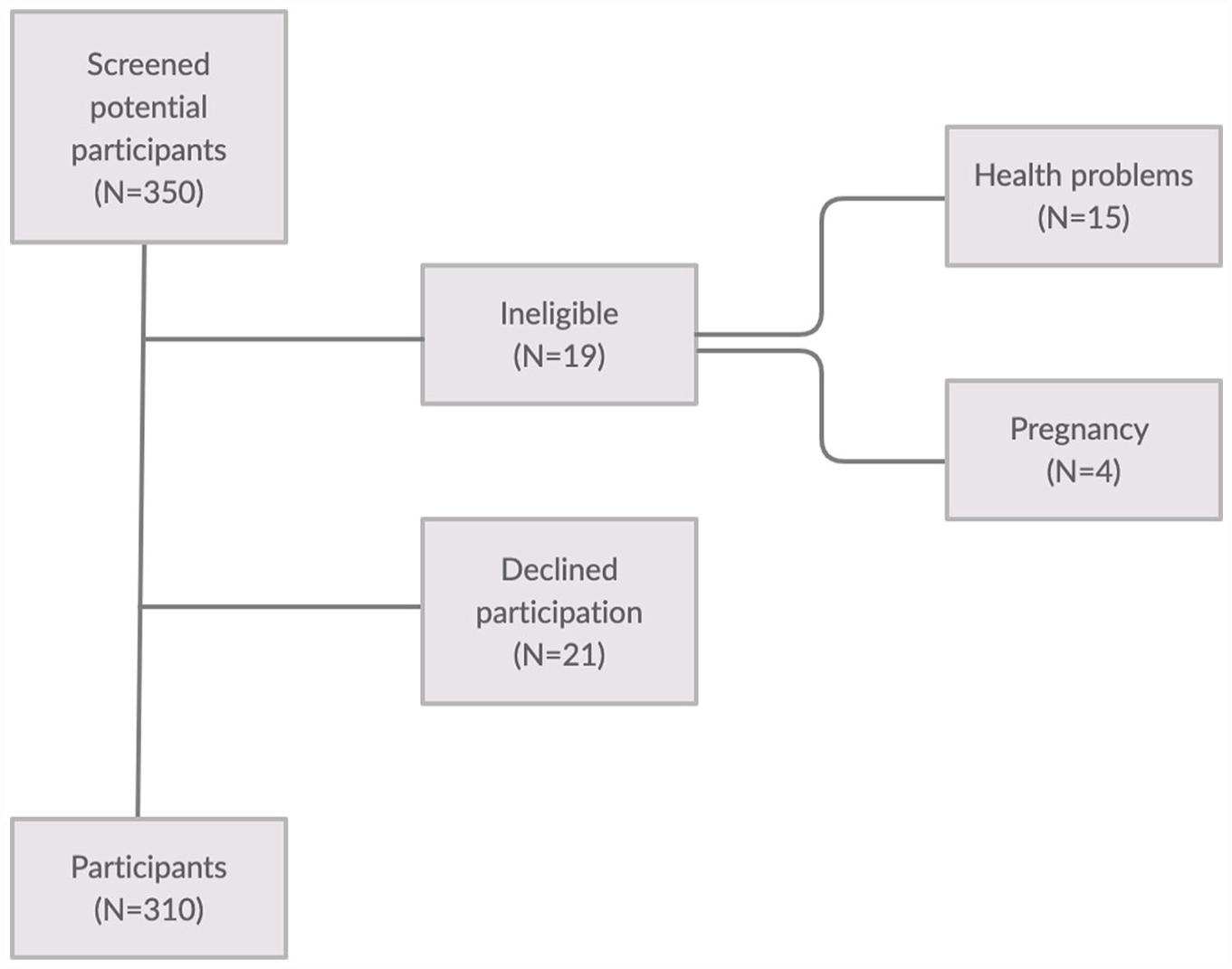
Flow diagram of participant recruitment.
The inclusion criteria were as follows: (a) being a resident in the rural area of Nerpio and (b) being >18 years old. The following exclusion criteria were fixed: (a) pregnancy, (b) terminal disease, and (c) mental illness or cognitive disorders which do not allow the assessment to be completed (e.g., dementia). Inclusion and exclusion criteria were self-reported by patients and confirmed by checking their medical records in nursing consultation. After receiving verbal and written information, a total of 310 patients who met the aforementioned inclusion criteria gave their written consent for participation. The local ethics committee approved the study protocol (September 14, 2021), which was conducted in agreement with the Declaration of Helsinki. The study was carried out following the STROBE reporting checklist for observational research.
Sociodemographic Characteristics
First, each participant completed a structured questionnaire on their sociodemographic characteristics, including gender, age, civil status, socioeconomic status, and educational level.
MetS Diagnostic Criteria
According to the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III), persons meeting at least three of the following five criteria qualify as having MetS: higher fasting glucose level, elevated blood pressure, lower high-density lipoprotein cholesterol (HDL-C) level, higher triglyceride level, or abdominal obesity (James et al., 2020). These are defined below:
(1) Elevated blood glucose: fasting blood glucose ≥110 mg/dL or a diagnosis of diabetes;
(2) Elevated blood pressure (systolic blood pressure [SBP] ≥130 mmHg and/or diastolic blood pressure [DBP] ≥ 85 mmHg) or a history of hypertension;
(3) Low HDL-C: serum HDL-C concentration <40 mg/dL for males and <50 mg/dL for females;
(4) Elevated triglyceride: serum triglyceride concentration ≥150 mg/dL;
(5) Abdominal obesity: a waist circumference (WC) of ≥102 cm for males and ≥88 cm for females, as measured to the nearest 0.1 cm at the level of the navel, using a flexible steel tape.
Anthropometric Data
After completing a general information questionnaire, participants were instructed to wear light clothing (e.g., a t-shirt and shorts) for the physical examination. Once the subjects were barefoot and, in their underwear, their body weight (kg) was measured using an electric scale (Tanita® BC-420-MA®, Tokyo, Japan). Their height was measured with a portable stadiometer (Seca® 213, Hamburg, Germany). Body mass index was calculated as kg/height (m2), and classified according to the World Health Organization (WHO) criteria (WHO, 2000) (normal: 18.5–24.9 kg/m2; overweight: 25.0–29.9 kg/m2; and obese: ≥30 kg/m2). WC was determined using the average of two measurements taken with a tape (Lufkin W606PM®, Parsippany, NJ, USA) at waist level (midway between the last rib and the iliac crest).
Blood Pressure Measurements
Blood pressure was taken using an automatic monitor (Omron® Healthcare Europe B.V., Hoofddorp, the Netherlands) following the recommendations of the European Heart Society: the patient’s blood pressure was taken on the right arm, with the participants in a supine position and after 10 minutes of rest (Mancia et al., 2013).
Blood Collection Analysis
For blood measurements, participants were instructed to fast for at least 8 hours prior to the test, and abstain from exercise training, caffeine, nicotine, and alcohol for 12 hours before the clinical examination; they continued to take their regular medication. Capillary blood samples (40 µL) were collected to determine serum biochemical parameters, including fasting glucose and total cholesterol (TC) using portable Cardiocheck® equipment (Mexglobal SA, Parsippany, NJ, USA).
Loneliness Assessment
The validated Spanish version of the UCLA Loneliness Scale was used to evaluate loneliness (Vázquez & Jiménez, 1994). This scale is a widely used unidimensional measure of loneliness showing significant correlation with other measures of loneliness (Deol et al., 2022). The UCLA Loneliness Scale comprises 20 items such as “Do you feel close to people?” and “Do you feel left out?” Patients rated each item on a 4-point scale, ranging from 1 (never) to 4 (always). Higher scores represent higher levels of loneliness (Chen et al., 2021).
Social Support Evaluation
The validated Spanish version of the Multidimensional Scale of Perceived Social Support (MSPSS) was used to assess perceived social support (Landeta & Calvete, 2002). MSPSS is a 12-item scale that measures the perceived adequacy of social support from three domains: family, friends, and significant others. It has a three-factor structure, with each subscale comprising four items that address practical help, emotional support, the availability to discuss problems, and help in decision-making (Ercole et al., 2018; Grey et al., 2020). The participants were asked to indicate their agreement with items on a seven-point Likert-type scale, ranging from very strongly disagree to very strongly agree, yielding a score range from 12 to 84. (Grey et al., 2020).
Social Isolation Evaluation
To assess social isolation, the validated Spanish version of the Lubben Social Network Scale (LSNS-6) was administered (Granero et al., 2020). This consists of two sets of questions on family and friendship ties, with three items in each set, including the number of relatives/friends that the subject sees or hears from at least once a month, the number of relatives/friends they feel able to call for help, and the number of relatives/friends they feel able to talk to about private matters. Each item is scored from 0 to 5. The total score is an equally weighted sum of the 6 items, ranging from 0 to 30. Higher scores indicate larger social networks. Individuals with a score of less than 12 were classified as socially isolated, meaning that, on average, there were fewer than two individuals available for the social network aspects assessed (Lubben et al., 2006; Röhr et al., 2021; Wu & Sheng, 2021).
Statistical Analysis
IBM SPSS version 24 was used for all the analyses (IBM Statistical Program for Social Sciences SPSS Statistic, Corp., Armonk, NY, USA). All the analyses were carried out by a blinded researcher. A descriptive analysis was developed to summarize the sociodemographic and clinical characteristics of the participants. Continuous variables were expressed as the mean ± the standard deviation, and categorical variables were recorded as numbers and percentages. The normal distribution of the variables was checked using the Kolmogorov–Smirnov test. All the variables had non-normal distributions so Mann–Whitney U and Fisher’s exact test were employed. A comparison by sex of the baseline demographic and clinical data was made using the Student’s t-test for continuous variables, or the chi-square test for categorical variables, with their nonparametric homologues, the Mann–Whitney U and Fisher’s exact test being used as appropriate. The Kruskal–Wallis test was also used when outcomes did not reach normality. An analysis of covariance was used to examine the association between MetS prevalence, loneliness level, and social support, adjusted for sex, age, race, educational level, and monthly income. To analyze the differences in the MetS components according to loneliness level and social support, the participants were divided according to their median values for each variable. The cohort was therefore categorized into high levels of loneliness (UCLA ≥ 54.61) and low levels of loneliness (UCLA < 54.61); low levels of social support (MSPSS ≥ 69.12) and high levels of social support (MSPSS < 69.12); and individuals who were socially isolated (LSNS-6 < 12) or not socially isolated (LSNS-6 ≥ 12). A 95% confidence interval was established, and significance was set at p < .05.
Results
The main characteristics of the study population according to gender are shown in Table 1. No significant differences were observed for age, civil status, educational level, or household income between men and women. As expected, anthropometric data including weight, height, and WC were higher in men than women. In terms of cardiovascular risk factors, significant differences between men and women were found for the presence of dyslipidemia, acute myocardial infarction, stroke, smoking status, and being a former smoker. Compared with women, men had significantly higher levels of TC, HDL-C, glucose, SBP, and DBP. Among medications currently being taken, antidyslipidemic agents and uric acid treatments were significantly more common in men (p = .01, p = .005, respectively); nonetheless, the prevalence of thyroid treatment was significantly higher in women (p = .001).
Sociodemographic and Clinical Characteristics According to Sex (N = 310).
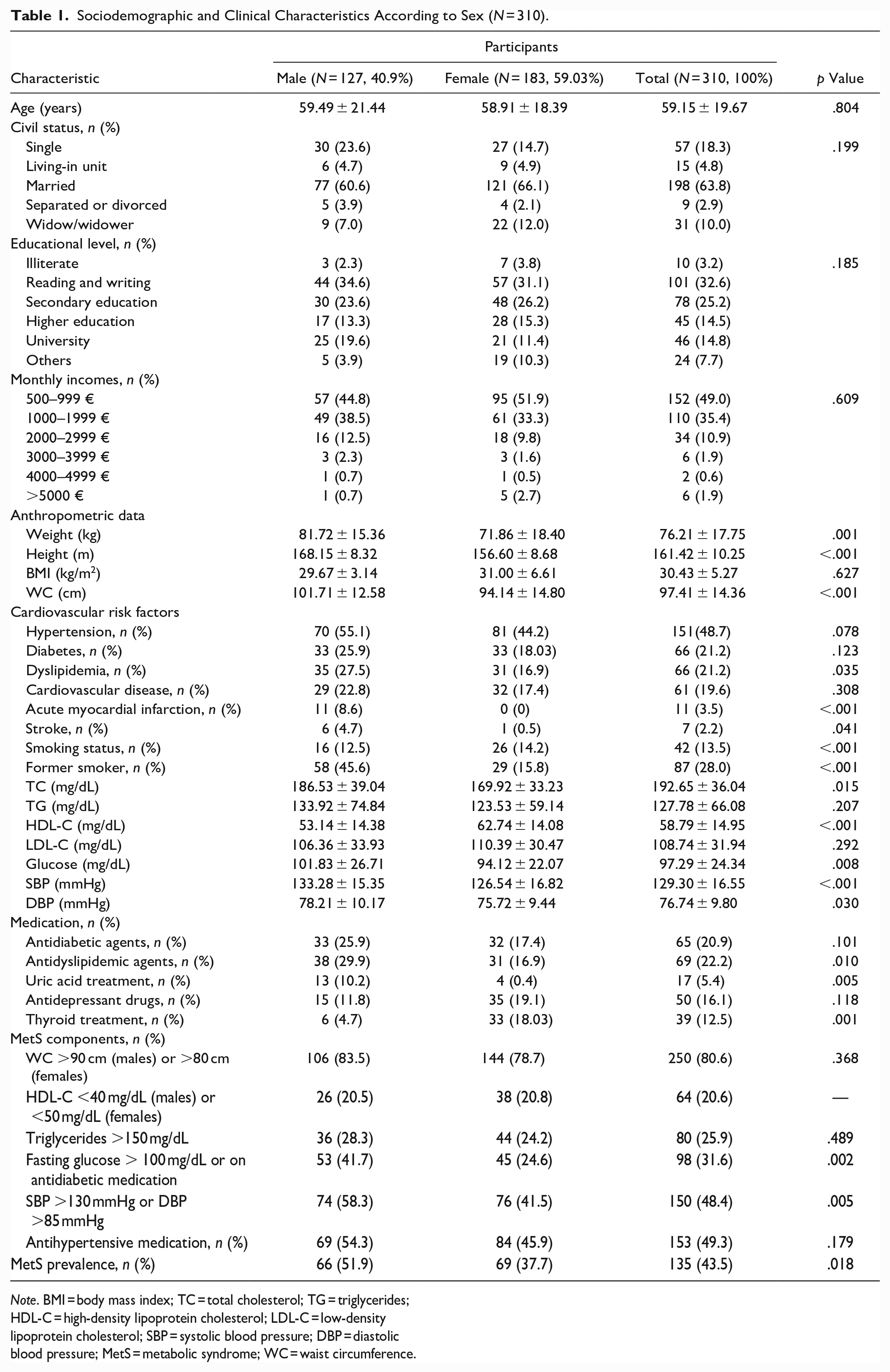
Note. BMI = body mass index; TC = total cholesterol; TG = triglycerides; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; SBP = systolic blood pressure; DBP = diastolic blood pressure; MetS = metabolic syndrome; WC = waist circumference.
With regard to metabolic parameters, 80.6% of the subjects had an increased WC, 20.6% had low HDL cholesterol levels, 25.9% had high triglyceride levels, 31.6% had increased fasting glucose, and 48.4% had systolic hypertension. It was found that 43.5% of the study sample fulfilled the diagnosis criteria for MetS. Also, men presented significantly higher values for fasting glucose and hypertension, and the prevalence of MetS was significantly higher in men than women (51.9 vs. 37.7%; p = .018)
Table 2 shows loneliness level, social support, and social isolation according to MetS prevalence in the study cohort. The analysis of covariance showed that subjects with MetS had significant higher levels of loneliness (p = .001), less social support (p = .032), and greater social isolation (p = .005) after adjusting by sex, age, race, educational level, and household incomes compared to subjects without MetS.
Loneliness Level, Social Support, and Social Isolation According to MetS Prevalence (N = 310).
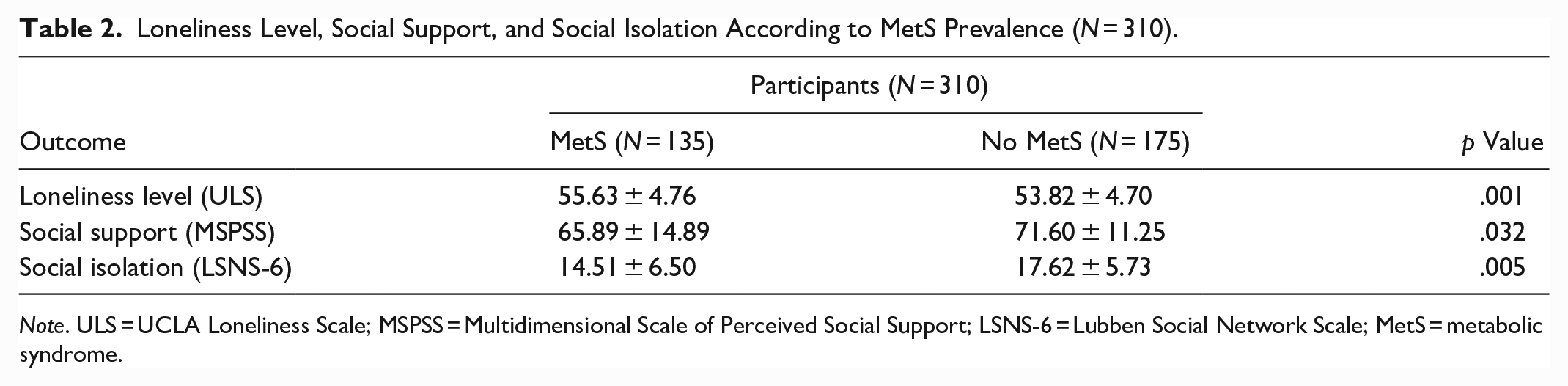
Note. ULS = UCLA Loneliness Scale; MSPSS = Multidimensional Scale of Perceived Social Support; LSNS-6 = Lubben Social Network Scale; MetS = metabolic syndrome.
Differences in MetS components according to loneliness level, social support, and social isolation are presented in Table 3. SBP was significantly higher in rural adults who were socially isolated than non-socially isolated individuals (131.52 ± 17.06 vs. 128.35 ± 16.27; p = .004). No significant differences among MetS components were observed for loneliness and social support.
Differences in MetS Components According to Loneliness Level and Social Support (N = 310).
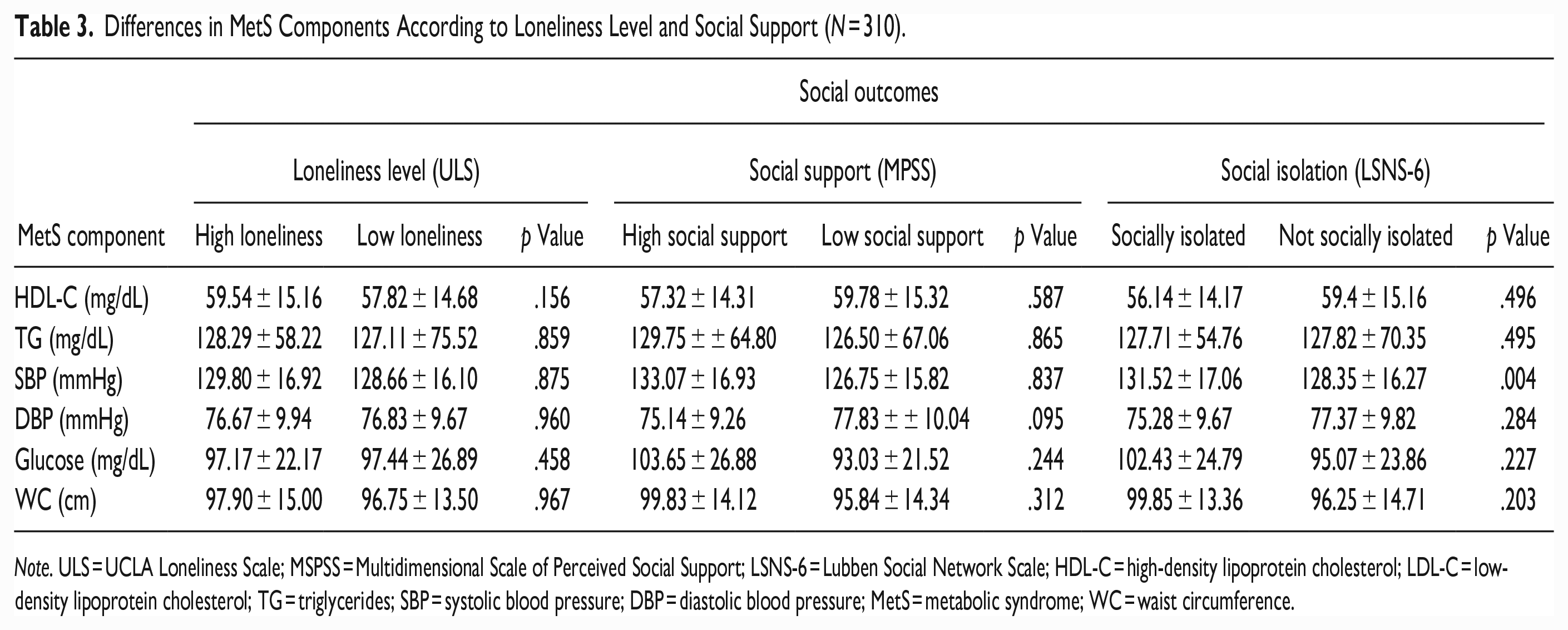
Note. ULS = UCLA Loneliness Scale; MSPSS = Multidimensional Scale of Perceived Social Support; LSNS-6 = Lubben Social Network Scale; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; TG = triglycerides; SBP = systolic blood pressure; DBP = diastolic blood pressure; MetS = metabolic syndrome; WC = waist circumference.
Discussion
In this study, we found that adults from a rural area with MetS had significantly higher levels of loneliness, less social support, and greater social isolation, supporting the hypothesis that these environmental factors may play a key role in the prevalence of MetS. Moreover, we identified that almost half of the rural population studied fulfilled the MetS diagnosis criteria.
Several previous studies have proposed that loneliness and social isolation might be risk factors for the development of cardiometabolic abnormalities (Badcock et al., 2019; Cacioppo et al., 2015; Valtorta et al., 2016). Longitudinal research in human and animals concludes that loneliness is a potent social stressor that leads, inter alia, to an increased morning rise in cortisol and decreased glucocorticoid receptor sensitivity, indicating increased activity in the hypothalamic–pituitary–adrenocortical axis (Badcock et al., 2019; Cacioppo et al., 2015). These processes may increase the risk of lonely individuals developing MetS (Valtorta et al., 2016). Nevertheless, the mechanism by which social isolation impacts health outcomes is unclear for a number of reasons. First, social isolation is associated with general morbidity and mortality rather than with the etiology of any specific disease. Second, the effects of social relationships on long-term morbidity and mortality take years to unfold and many cross-sectional studies do not take this into account (Winterton et al., 2020).
Interestingly, we also found that SBP was significantly higher in socially isolated rural adults compared to non-socially isolated individuals. These findings are in line with previous work (Yang et al., 2013, 2016). In two studies, including 4323 participants aged 50 and older from the United States and 1571 participants aged 57 to 85 of African-American or Hispanic ethnicity, Yang et al. reported a negative association between social integration and poor physical functioning and SBP (Yang et al., 2013, 2016). It has therefore been proposed that possible mechanisms through which social isolation may influence blood pressure levels include psychological stress and social contagion (behavior spread through a social network via the diffusion of information or the transmission of behavioral norms) (Nakagomi et al., 2022).
In addition, our findings showed that the rate of MetS according to the NCEP ATP III was 43.5%, suggesting that the prevalence of MetS continues to increase in line with the dramatic rise in the prevalence of obesity. The observed prevalence is similar to that identified in studies of rural populations in Mongolia (Kim et al., 2021), Korea (Lee et al., 2018), and Poland (Czekajło et al., 2019). However, other studies in rural areas of China showed a prevalence of MetS ranging from 14.3% (Guo et al., 2017) to 24.2% (Ling et al., 2020), somewhat lower than in this study. Also, it should be highlighted that we observed a higher prevalence of MetS in men than in women, similar to that observed in other European populations (Gao et al., 2008). Nevertheless, previous studies conducted in rural areas of China and Iran (Guo et al., 2017; Hosein et al., 2020; Naghipour et al., 2021; Ying et al., 2021) showed the opposite trend. These differences in prevalence can be attributed to differences in lifestyle, genetic factors, or age.
This study has some limitations that should be mentioned. First, it was a cross-sectional study and, as such, was subject to the limitations inherent to this type of design. Longitudinal prospective research is needed to address the impact of loneliness, social support, and social isolation on MetS. Second, our study was carried out in a delimited geographic area; our findings will therefore require replication in further studies of populations of older adults from other areas and communities with different geographic and demographic profiles. Despite its limitations, this study provides novel information. To our knowledge, this study is the first to investigate the relationship between the MetS and its components, and social health in a rural Spanish population, providing reliable data that can be helpful to understand the status of MetS according to social health in other similar rural areas with similar socioeconomic factors and lifestyle.
In conclusion, adults from a rural area with MetS had significantly higher levels of loneliness, less social support, and greater social isolation, supporting the hypothesis that these environmental factors may play a key role in the prevalence of MetS. Future research is warranted to support these preliminary findings.
Relevance for Clinical Practice
Our findings suggest that social health might influence the metabolic health of a rural Spanish population. This, together with previous reports, highlights the relevance of considering social isolation and loneliness important factors to be screened for and assessed in clinical practice by healthcare professionals in general and nurses in particular.
The use of specific clinical practice guidelines and screening programmers focused on the social health of target populations would allow, first, the early detection of patients in situations of diminished social health who might be at a higher risk of developing MetS. In this way, individualized and tailored interventions could be implemented to ameliorate social isolation and loneliness, which would also would improve metabolic health in these populations considering their specific socioenvironmental conditions. It would also facilitate quality health education in good lifestyle behavior and the creation of robust healthcare team–patient support networks, tasks in which the nursing profession, as part of a multidisciplinary team, play a key role.
Footnotes
Acknowledgements
The authors express their gratitude to the participants for taking part in this study. This manuscript is part of a PhD thesis developed by DelOlmo-Romero Sara (Doctoral Programme in Clinical Medicine and Public Health, University of Granada, Granada, Spain).
Author Contributions
Study design: DelOlmo-Romero Sara, Correa Rodríguez-María, Rueda-Medina Blanca.
Data collection: DelOlmo-Romero Sara, Sánchez-Martínez M. Cristina.
Data analysis: DelOlmo-Romero Sara, Correa-Rodríguez María, Rueda-Medina Blanca, Sánchez-Martínez M. Cristina, Gil-Gutiérrez Rocío, Ortego-Centeno Norberto.
Manuscript writing: DelOlmo-Romero Sara, Correa-Rodríguez María, Rueda-Medina Blanca.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the local Ethics (Helsinki) Committee of Albacete (Spain) (2021-78).
Data Availability
The datasets used and analyzed during the study are available from the corresponding author on reasonable request.