
Abstract
To compare pain management outcomes in postoperative patients from an American hospital and a Chinese hospital. A convenience sample of 244 patients in the United States and 268 patients in China with similar surgical sites completed the American Pain Society Patient Outcome Questionnaire-Revised (APS-POQ-R) and the Pain Management Index (PMI) was calculated on their first postoperative day. Patients in the United States reported a higher score on the “perception of pain management” subscale of the APS-POQ-R and a higher proportion of adequate treatment as measured by the PMI (85.2% vs. 39.0%, p < .001). Patient education and degrees of pain relief predicted patient satisfaction with pain management (item in APS-POQ-R) in patients from both countries. A higher level of compliance with pain management guidelines has contributed to a higher level of perception in patients in the United States. Establishing procedure-specific protocols and clinical pathways may improve pain management outcomes for Chinese patients.
Pain management has been identified as an important human right by many international organizations (Brennan et al., 2019). Optimal pain management is also a fundamental component of enhanced recovery after surgery; it improves the quality of recovery, promotes early mobilization, and contributes to clinical and economic outcomes (Ljungqvist et al., 2017; Nimmo et al., 2017; Tan et al., 2015). Pain management outcomes, including patient satisfaction with pain management, have been evaluated for over two decades with the purpose of quality improvement (Gordon et al., 2010). However, little is known about comparisons of pain management outcomes among different countries and ethnicities, which may provide valuable clues for quality improvement.
Major advances in pain management have been initiated during the last three decades, including the advocacy of pain assessment as the “fifth vital sign,” the establishment of acute pain service teams, and innovations in analgesic medications and techniques, such as patient-controlled analgesia (PCA) and multimodal analgesia (Chou et al., 2016; Pasero et al., 2016; Prabhakar et al., 2014). These developments have been widely incorporated into clinical guidelines in pain management, which constitute one of the most important resources available to help clinicians make decisions and stay informed of updated evidence (Chou et al., 2016). The first operative pain management guidelines were established in Australia (1988) and the United Kingdom (1990) (Tawfic & Faris, 2015). Clinical practice guidelines for postoperative pain management in the United States were composed by the American Pain Society and American Society of Anesthesiologists in 1992 and have been updated many times since then (American Society of Anesthesiologists, 2012; Chou et al., 2016). However, limited relevant resources are available in China. The first expert consensus on postoperative pain management was published by the Chinese Society of Anesthesiology in 2010 in the Chinese language (Xu et al., 2010), approximately two decades later than in Western countries. The Chinese guideline offers pain management goals determined by maximum pain relief, minimum side effects, the best physical and psychological functions, and the best quality of life and patient satisfaction, but does not include a numerical scale for more precise measurements. Frequently used pain medications have been identified with recommended doses and specific multimodal analgesia methods targeting different anticipated postoperative pain severities (Xu et al., 2010).
Multiple reasons help explain the delayed development of pain management in China. A systematic review examining Chinese cancer patients revealed several factors that have impaired the development of pain management strategies, namely, misbeliefs by patients and families (e.g., fatalism, desire to be good, fear of addiction), performance by health professionals (such as poor communication, ineffective management of pain), and barriers related to the healthcare system (including limited access to analgesics, lack of health insurance) (Xu et al., 2018). Similar barriers have also been reported in postoperative patients who have undergone surgery; 72.6% of these patients knew nothing about morphine, while 18.5% strongly rejected morphine because of its notorious reputation in Chinese history (Weiran et al., 2013).
A report on clinical pain management in China indicates that approximately half of patients (48.3%) with acute pain are prescribed analgesics, while only 27.1% of patients with severe pain receive strong opioids (Xiao et al., 2018). In postsurgery patients, 51.6% receive no treatment at all (Weiran et al., 2013), while 80.9% to 86% experience moderate to severe pain after surgery (Shen et al., 2008; Weiran et al., 2013). The most common nonpharmacological methods applied for pain management are tolerating pain (84.4%), repositioning (83.7%), and family support (81.9%); family support has been reported as the most effective method (Shen et al., 2008). All these findings may indicate that pain management has not been identified as a priority in Chinese clinical practice in part due to patient attitudes about pain (Shen et al., 2008; Yin et al., 2011).
Although a comparison of analgesic medications between different countries has been reported (Kaafarani et al., 2020; Li et al., 2018), few have compared pain management outcomes among different countries. Recent research has reported that patients in the United States are prescribed alarming high amounts of opioids after surgery when compared with patients in other countries (Kaafarani et al., 2020; Li et al., 2018). It has been reported that 91% of postoperative patients in the United States receive post-discharge opioids, while no Chinese patients are prescribed any post-discharge opioids (Kaafarani et al., 2020). However, after major head and neck surgeries, Hong Kong patients receive similar doses of nonsteroidal anti-inflammatory drugs (NSAIDs) as that given to such patients in the United States (Li et al., 2018).
Outcomes of health care measure the effectiveness of services and the impact on patients and have been widely accepted as indicators of the quality of health care (Donabedian, 2005). To measure the quality of pain management, the most commonly used outcome indicators include changes in pain severity, physical, and emotional function, adverse effects of pain treatment and patient satisfaction (Gordon et al., 2010). The American Pain Society Patient Outcome Questionnaire (APS-POQ), first published in 1995 with the aim of quality improvement, incorporates most of these indicators. It was revised (APS-POQ-R) in 2010 and remains the most widely used instrument for examining pain management outcomes around the globe (Gordon et al., 2010; Shen et al., 2008). The Pain Management Index (PMI) is another validated method used to evaluate the adequacy or quality of pain treatment by combining both pain intensity and pharmacologic therapy, which could reflect consistency between the medical order and practice guidelines (Deandrea et al., 2008).
In this comparative study, we explored the differences in postoperative pain management outcomes (defined by APS-POQ-R and PMI) and postoperative pharmacologic treatments by comparing a well-developed country (the United States) and a developing country (China) with regard to pain management. Predictors of patient satisfaction on the APS-POQ-R were also explored in both countries using other items from the APS-POQ-R, the PMI, and demographic and surgical information (Gordon et al., 2010). The present study can provide valuable information to clinical professionals seeking to improve pain management quality.
Methods
Participants and Procedures
The present study was a descriptive comparative study. Ethical approval was provided by the School of Nursing in Peking Union Medical College, Chinese Academy of Medical Sciences in China and the School of Nursing, University of North Carolina at Chapel Hill in the United States. Patients were conveniently recruited from two hospitals, namely, an 803-bed hospital located in the southeast region of the United States and an 1860-bed hospital located in a major city in eastern China. Both hospitals are large not-for-profit academic teaching hospitals and among the top-ranked hospitals in their locations. Additionally, both hospitals are urban locations and serve patients from a wide geographical area.
The inclusion criteria were as follows: adult inpatients aged 18 to 90 years and patients who were on their first postoperative day after elective surgery and were conscious and sufficiently alert to respond to and communicate with researchers. Pregnant women and those who underwent cesarean sections were excluded.
Five units admitting postoperative patients at the hospital in the United States were all included for sampling, except intensive and critical care units, from January to May. To achieve a similar proportion of patients with different surgical sites, 15 units caring for postoperative patients at the Chinese hospital were identified for participant recruitment from March to September in the same year, with the elimination of units admitting patients with thoracic, vascular, obstetrics, cosmetic, and otolaryngological surgeries. The percentage of patients with different surgical sites in the United States was calculated to provide a reference for sampling in each unit in China.
Data were collected in each country by recruiting nursing students and providing standardized data collection training by the primary researcher. Patients were selected by the data collectors in consultation with the unit’s charge nurse and according to the inclusion criteria on the days designated for data collection.
Data collection was performed using a questionnaire administered face-to-face using a standardized procedure. Verbal consent was obtained from all participants with an invitation letter. Consent was read aloud per protocol to avoid literacy concerns. Following consent, all questions on the questionnaire were then read aloud by the data collector who then recorded each response. Data collectors then reviewed medical records to record demographic, surgical, and postoperative analgesia information.
Instruments
Pain management outcomes: APS-POQ-R and PMI
Patient management outcomes were measured by the APS-POQ-R and the PMI. The APS-POQ-R includes 23 items, 18 of which are rated using a numeric rating scale ranging from 0 to 10 and comprising five subscales: pain severity and sleep interference, affective interference, interference with activity, adverse effects, and perception of pain care (including degree of pain relief, involvement in decision making, and satisfaction with pain care). The patients were then asked to rate the helpfulness of the pain-related information they had received (if they had received any) using a numeric rating scale (ranging from 0 to 10). The application of nonmedical methods and how often patients were encouraged to use them were also surveyed (Gordon et al., 2010). The psychometric characteristics of the APS-POQ-R have been verified in many countries, including China (Botti et al., 2015; Schwenkglenks et al., 2014; Wang et al., 2017). The Cronbach’s alpha for the continuous items was .86 in patients in the United States (Gordon et al., 2010) and .73 for those in China (Wang et al., 2017).
The PMI was calculated by subtracting the strongest pain category score from the analgesics score (Cleeland et al., 1994; Deandrea et al., 2008). The “worst pain” intensity scored by patients on the APS-POQ-R was used to define the pain category score: 0 (no pain), 1 (mild pain, 1–3), 2 (moderate pain, 4–7), and 3 (severe pain, 8–10). Analgesics were retrieved from the patient’s postoperative medical orders and coded according to World Health Organization analgesic ladders (0 = no analgesic medication, 1 = nonopioid analgesics, 2 = weak opioids, 3 = strong opioids) (Cleeland et al., 1994). The result ranges from −3 (when a patient suffering severe pain received no analgesics) to +3 (when a patient receiving strong opioids reported no pain); a score of 0 (when analgesics were prescribed according to analgesic ladders) and higher indicates adequate analgesic treatment in terms of the analgesic category (Deandrea et al., 2008). The PMI does not account for analgesic doses in pain management; however, it does quickly evaluate the adequacy of pain management (Deandrea et al., 2008). While the PMI was originally designed to evaluate the adequacy of pain management in cancer patients, its validity in applying to patients with acute pain, including postoperative patients, has been well established (Shen et al., 2008).
Pharmacological treatments
Pain-related pharmacological treatment orders (including the name of the medication, dose, time, and route of administration) prescribed postoperatively before the interview were retrieved from the patients’ medical records.
Surgical and demographic information
Surgical and demographic information was obtained from the patients’ charts (electronic version in the United States and paper version in China), including their physical status according to the American Society of Anesthesiologists (ASA), surgical type (endoscopic or open), surgical name, surgical site (head and neck, breast, abdomen, orthopedics, and others), diagnosis after surgery (cancer or noncancer), and analgesics prescribed after surgery. Two researchers coded the patients’ surgical procedures into three categories (minor, medium, and major) according to evidence-based anticipated pain levels after surgery (Peters et al., 2007). For instance, thyroidectomy was placed into the minor surgery group, while cholecystectomy and colorectal surgery were defined as intermediate surgeries, and hepatectomy and a combination of different bowel surgeries were defined as major surgeries (Peters et al., 2007). If we could not validate the anticipated pain level for a surgical procedure, we referenced another similar procedure in the list, achieving 96% agreement and clearing up inconsistencies by discussions with an anesthetist in our research group.
Data Analysis
Data were analyzed using IBM SPSS statistics version 22.0 for Windows. Descriptive statistical analyses were used to describe the characteristics of the participants, pain treatments, and pain management outcomes. Comparisons between countries were made using independent samples t-tests and Pearson’s chi-squared tests according to the nature of the variables. Stepwise regression was applied to determine the predictors of patient satisfaction with the results of pain management in generalized linear models. Patient satisfaction is an item measured in the APS-POQ-R; the potential risk factors included in the stepwise regression consisted of other items from the APS-POQ-R (except “patient satisfaction”), the PMI, and surgical and demographic factors that were significantly associated with patient satisfaction in a univariate analysis. The significance level was set at p < .05.
Results
Sample Characteristics
A total of 244 eligible patients in the United States and 268 patients in China were ultimately recruited. The participants in the United States were mainly white (71.3%, N = 174) or black (22.5%, N = 55), while 97.4% (N = 261) of the patients in China were identified as Han, which is the main race in China. The American sample had a higher body mass index (BMI) (31.38 ± 9.52 vs. 23.89 ± 3.71, p < .001) and a more severe ASA physical status (p < .001) than their counterparts. Compared to patients in China, more patients in the United States reported a history of surgery (88.1% vs. 51.9%, p < .001), chronic pain lasting longer than 3 months (46.3% vs. 28.7%, p < .001), and cancer diagnoses (29.5% vs. 20.9%, p = .026). No differences were found between the two countries in regard to age, sex, surgical site, or surgery categories (minor, medium, and major) (Table 1).
Comparison of Sample Characteristics in the United States and China.

Note. Continuous variables are presented as the mean ± standard deviation. Other variables are presented as number (%). Independent t-test, Pearson’s Chi-squared test or analysis of variance (ANOVA) were used for statistical analysis as appropriate. BMI = body mass index.
p < .001.
Pain Management Outcomes
APS-POQ-R
Only two items of the APS-POQ-R (interference with out-of-bed activities and falling asleep) were comparable in the two countries. All other items were reported to be significantly higher in American patients than in Chinese participants, as were the subscale scores (Table 2). More patients in the United States (74.2%, N = 181) had received pain-related information than in China (25.0%, N = 67, p < .001), and the participants in the United States rated that information as being more helpful than did the participants in China (8.68 ± 2.17 vs. 6.80±2.91, p < .001). Approximately 59.8% (N = 146) of the patients in the United States and 23.9% (N = 64) of the patients in China had tried nonmedication methods (p < .01). More Chinese patients (82.5%, n = 221) than American participants (56.1%, n = 137) reported that they had never been encouraged to use nonmedical methods to address their pain (p < .001). The most reported methods among the participants from the United States were prayer (47.9%, N = 70), deep breathing (43.2%, N = 63) and distraction (40.4%, N = 59), whereas distraction (54.7%, N = 35) and massage (32.8%, N = 21) were the most reported methods by the patients in China.
Comparison of Patient Outcomes in APS-POQ-R Between the United States and China.
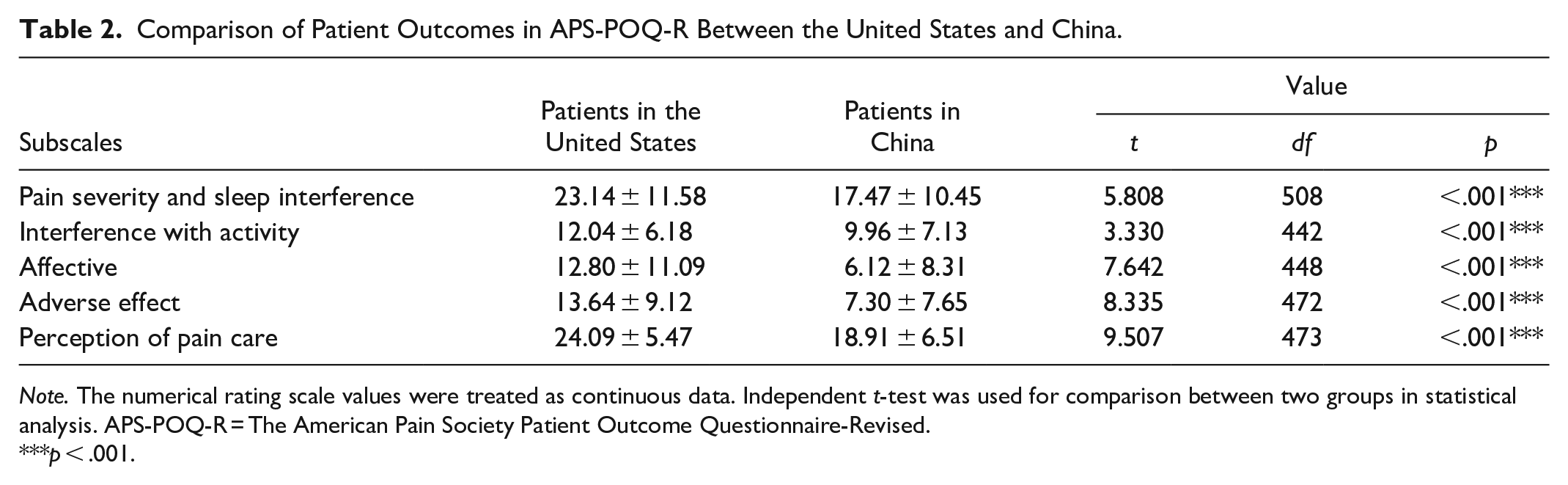
Note. The numerical rating scale values were treated as continuous data. Independent t-test was used for comparison between two groups in statistical analysis. APS-POQ-R = The American Pain Society Patient Outcome Questionnaire-Revised.
p < .001.
PMI
Based on the PMI, 85.2% of patients in the United States reported adequate pain management, which was a much higher results than that for the patients in China (39.0%, p < .001). The PMI calculations differed widely; more than half (61.5%) of the patients in the United States were treated appropriately with a PMI of 0, while in China, the highest percentage of PMI was -2 (29.2%).
Pharmacological Treatments
In China, more than half of the patients (54.5%, N = 146) reported not using any analgesic method after surgery, whereas only one American patient (0.4%) reported no analgesic use. In the United States, 95.5% (N = 232) of the patients reported using multimodal analgesia, whereas 6.5% (N = 8) of patients in China reported using combined pain medications or analgesic techniques. PCA use differed, with half (56.5%, N = 138) of the patients in the United States reporting PCA use and only 31.0% (N = 83) of the patients in China reporting such use.
The most common type of non-PCA medication order was pro re nata (PRN), with 79.1% of patients in the United States reporting being under this order, whereas in China, the most common was a single order (72.3%). The main routes of administration in the United States were oral (54.1%) and intravenous (IV) (45.9%), while in China, the predominant route was intramuscular (IM) (59.6%), followed by IV (21.3%), and oral (19.1%) administration. The most frequently prescribed type of medication was strong opioids (45.2%) in the United States compared to NSAIDs (51.1%) in China. Meperidine was the most commonly used strong opioid (38.3%, N = 18) prescribed in China, at 94.4% (N = 17).
Prediction of Patient Satisfaction
Risk factors significantly associated with patient satisfaction in univariate analysis were included in multiple linear regression, including gender, diagnosis (cancer), and chronic pain history, as well as all other items from the APS-POQ-R (except “patient satisfaction”) and the PMI. However, in Chinese participants, the item of “helpfulness of the information” was not included because only 25% (N = 67) of the patients reported that they had received pain-related information; therefore, the patients who did not receive pain-related education were not asked to score the item. Stepwise regression showed that the helpfulness of pain management information was the most important predictor in the United States, accounting for 29.9% of the total variance. The other predictor in the United States was the degree of pain relief, which was the most significant predictor in China, accounting for 17.9% of the variance. The models accounted for 34.5% and 27.0% of the total variance in the United States and China, respectively (Table 3).
Predictors of Patient Satisfaction in Pain Management in the United States and China.

Note. Stepwise regression was applied in multiple linear regression. Dependent variable: patient satisfaction. Independent variables include gender, diagnosis (cancer), and chronic pain history, as well as other items in APS-POQ-R. APS-POQ-R = The American Pain Society Patient Outcome Questionnaire-Revised.
p < .01. ***p < .001.
Discussion
The patients in the United States rated a higher score on “perception of pain management” than did the Chinese patients, despite reporting higher levels of postoperative pain levels, interferences, and side effects. A similar phenomenon has been debated for decades (Gordon et al., 2010; Schroeder et al., 2016) and can perhaps be explained by the predicting factors of patient satisfaction, which have been verified in both countries, including pain-related information and the degree of pain relief influencing overall patient satisfaction.
The helpfulness of pain management information only explained up to 29.9% of the variance in patient satisfaction in the United States. This outcome is consistent with guidelines addressing patient education, as well as discharge plans that promote the quality of pain management (American Society of Anesthesiologists, 2012). A study in Jordanian patients reported that the item of “the patient was told about the importance of reporting pain” was positively associated with patient satisfaction, while pain intensity and interferences were not significantly predictive factors (Darawad et al., 2014). However, in China, only 45% of the patients reported being informed that pain management was very important after surgery (Shen et al., 2008). In another survey in China, even though 51.0% of the participating hospitals provided pain management education, most patients (66.0%) were educated preoperatively; only 5.0% of the patients reported being instructed postoperatively by ward nurses, while only 1.0% reported being instructed by the acute pain service group during ward rounds (Liu et al., 2016).
The role of acute pain services in promoting pain management outcomes has been widely accepted, but challenges remain in regard to practical implementation (Rawal, 2016). For instance, the lack of professional resources, busy nursing schedules, and pain management are low nursing priorities in Chinese clinical practice (Rawal, 2016; Shen et al., 2008; Yin et al., 2011). One practical solution is to upgrade the role of ward nurses to be proficient in different acute pain service models (Rawal, 2016). Furthermore, education regarding pain management in nursing schools remains inadequate (Fang et al., 2017), which leads to less confidence in pain management in Chinese nurses than in American nurses, for whom pain management education is emphasized (Cong et al., 2014).
The study findings are consistent with a previous study in Europe in which the degree of pain relief contributed to patient satisfaction (Schwenkglenks et al., 2014). Patients’ perception of pain management (e.g., expectations for treatment, involvement in decision making, efforts made by health care professionals, the desire to receive more treatment), and pain experience (worst pain intensity) were also associated with patient satisfaction with pain management (Schwenkglenks et al., 2014). Thus, the process of pain management, rather than the results, may be the most important (Botti et al., 2015; Gordon et al., 2010). Compared with the participants in the United States, the patients in China received fewer services and information about pain management and were less involved in their pain management, which led to relatively low levels of patient satisfaction. Furthermore, physicians in China prescribe fewer opioids for their patients (Li et al., 2018), which has been deeply embedded in Chinese clinical practice and culture (Xu et al., 2018). The finding that approximately half (51.6%) of the patients in China received no analgesics for their postoperative pain (Weiran et al., 2013) may reflect conservative pain management beliefs, education and practices among both professionals and patients.
Compared with the patients in the United States, the patients in China were treated by fewer of the advanced strategies recommended by pain management guidelines, such as multimodal analgesia and PCA (American Society of Anesthesiologists, 2012; Chou et al., 2016; Xu et al., 2010). Multimodal analgesia has been strongly recommended because of its additive effects and opioid-saving mechanisms (American Society of Anesthesiologists, 2012; Chou et al., 2016). In the United States, the prevalence of multimodal analgesia is as high as 95.5%, showing high compliance with the guidelines. However, only 6.5% of Chinese patients reported using multimodal analgesia. PCA is also strongly recommended when the parenteral route is needed to administer systemic analgesia (Chou et al., 2016). As early as 1993, 78.1% of the hospitals in Australia and New Zealand were prescribing PCA use (Goucke & Owen, 1995). However, Liu et al. (2016) reported that postoperative PCA use in China is prescribed in only 43.0% of hospitals. In this study, PCA was reported by 31.0% of the Chinese patients compared with 56.6% of the American patients. Moreover, a recent study in China showed that 22.9% of patients discontinued PCA use on the first postoperative day, primarily due to the side effects (60.0%) and worrying about the side effects (Xu et al., 2015). Again, providing continuous education to professionals and patients is vital for improving pain management outcomes (Chou et al., 2016).
Clinical guidelines discourage the prescription of meperidine and the IM method because of their disadvantages, such as additional pain during the injection and the unstable absorption of the drug (American Society of Anesthesiologists, 2012; Chou et al., 2016). However, in this survey, up to 94.4% of the strong opioids administered in China were meperidine, and 59.6% of non-PCA prescriptions were given via the IM route. A recent study in China also showed this trend; only 48.33% of the patients with acute pain were administered analgesics, and meperidine (90.22%) was the most commonly used pain medication (Xiao et al., 2018).
There are differences in analgesic administration between the United States and China, as indicated by single medication orders and the avoidance of the use of opioids. Of the non-PCA prescriptions for Chinese participants, 72.3% were single doses, although 32.2% of the Chinese patients who had no pain treatments reported severe pain. This outcome may reflect concerns about addiction to opioids that have been deeply embedded in the Chinese culture and restrictive drug laws (Liu et al., 2007). A similar phenomenon has been reported in other countries with poor pain management, such as Eastern Poland, where pain management guidelines are available; 59.07% of patients report moderate to severe pain, but only 4.9% receive strong opioids (Borys et al., 2018). An Ethiopian hospital reported that 89.29% of its analgesic orders were single doses, while 21.9% were intramuscular orders; in addition, the hospital reported that the majority of its patients never requested pain medication or changes in pain medications (Woldehaimanot et al., 2014).
Although inadequate pain assessment and deficits in professional knowledge have been widely recognized as reasons for poor pain management, this view may be too simplistic (Brown & McCormack, 2005). Pain recognition, assessment, and management are performed within a particular organizational culture; they are not individual cognitive activities (Dowding et al., 2016). Tolerating pain and being embarrassed to report pain are parts of Chinese philosophy, and these attitudes have obstructed the development of pain treatment in China (Liu et al., 2007). Only 30% of postoperative patients in the United States sample were concerned about becoming addicted to narcotic medications (Gan et al., 2013). However, approximately 65.7% of Chinese patients preferred to tolerate their pain without treatment, and 40.1% of those who refused pain management reported having a fear of addiction and other adverse effects related to opioids (Xiao et al., 2018).
More important barriers may come from the culture or context of the facilities, such as the empowerment of nurses, the nursing workload, and the potentially unmeasurable characteristics of health institutions (Alaloul et al., 2017). Continuing education programs, collaboration with anesthesiologists and other physicians, and the incorporation of multimodal analgesia into early recovery and clinical pathways after surgery are strategies that can emphasize the priority of pain management (Rawal, 2016) and help health professionals recognize the importance of pain management (Tan et al., 2015). Moreover, since pain management guidelines tend to be general principles, developing procedure-specific evidence-based recommendations is more practical for improving clinical implementation (Joshi et al., 2019).
Brink-Huis et al. (2008) identified three effective organizational models for cancer pain management in hospitals, namely, institutionalization models, clinical pathways, and pain consultation services, which are complementary to each other. The first step in pain management improvement is the institutionalization model, which defines organizational policies and protocols. Clinical pathways provide continuous pain interventions, including assessment, patient education, interdisciplinary cooperation, and referring patients to the consultation service, which could provide case management, as well as discharge planning (Brink-Huis et al., 2008). Pain management models and programs should be incorporated across the organization to promote maximum pain management outcomes (Brink-Huis et al., 2008; Rawal, 2016). To promote pain management quality improvement in postanesthesia care, the establishment of a clinical pathway that incorporates multimodal analgesia and targets different patients can be promoted with educational programs (Naqib et al., 2018).
Even though more advanced pain management strategies were reported by the patients in the United States, their levels of pain intensity and interference of the pain were significantly higher. One possible explanation for this phenomenon is ineffective PRN medications and management. A national survey of postoperative inpatients in the United States reported that 57% had scheduled medication orders for pain management, while 16% had to ask for pain treatment when needed (Gan et al., 2013). As a result, 75% of patients experience moderate to extreme pain after surgery (Gan et al., 2013), in part because nurses do not always administer all available medication to patients who are in pain (Taylor, 2009). Nworah (2012) found that the evaluation and documentation of pain as the fifth vital sign and the effectiveness of PRN medications failed to improve patient outcomes because prompt interventions and treatments were not promoted. Only 44.3% of nurses report that the pain management in their units is well managed (Cong et al., 2014). A second explanation may be because of early ambulation on the day after surgery, which may contribute to severe pain in patients in the United States (Ljungqvist et al., 2017). Further explanations may include attitudes from professionals; adherence to procedures that affect patients’ reports of pain intensity and their expectations and tolerance of pain (Eriksson et al., 2016); and ethnic differences in pain management. White patients are more willing to report pain (Wandner et al., 2012) and consume significantly more analgesics than are Asian patients (Campbell & Edwards, 2012).
Limitations
The goal of the current study was to compare pain management outcomes in postoperative patients in both the United States and China, but the reality is that differences exist in the recruited participants from both countries. For example, the patients in the United States had a higher BMI than the patients in China. A higher number of patients in the United States had more severe conditions compared to the patients in China, as suggested by their ASA status, chronic pain conditions, and cancer diagnosis. This finding is consistent with a comparison of stroke patients between the United States and China, which shows that Chinese patients have a lower prevalence of comorbidities than their counterparts in the United States (Wangqin et al., 2018). In terms of surgery-related information, no difference was found in the two countries, including surgical category, surgical sites, and surgery type coded by expected pain; this makes the comparison of the patients reasonable.
The participating hospitals were selected by convenience sampling; therefore, caution is warranted in regard to generalizing the findings. Hospitals or units with a different pain management culture might have quite different patient outcomes, since the beliefs and concerns of patients and health professionals, the priority rank of pain management, and the feasibility of analgesics dramatically influence pain management outcomes (Xu et al., 2018). For instance, nurses in tertiary hospitals have a better education and beliefs than those in secondary hospitals (Li et al., 2019). However, the majority of the postoperative patients in the two participating hospitals were cared for in units selected for our research, and all the eligible patients were invited to participate during the data collection period. Despite the above mentioned limitations, these study parameters captured a localized picture of the two countries and revealed perceptions of similar problems, as seen in other areas and countries.
The numeric rating scale system was unfamiliar to some patients. The interpretation of a score of 10 (worst pain possible) was different among patients based on their previous experiences. The same pain intensity might be categorized into different severity categories, depending on the patient’s potential pain-rating schema (Frey-Law et al., 2014). Additionally, high-rating patients tend to rate all pain intensity significantly more severely than low-rating patients (Frey-Law et al., 2014). Pain is subjective and defined by the patients’ experience; therefore, it is important to have a rating system that allows for consistent interpretation by all patients (van Dijk et al., 2016). As a solution, the Changhai Pain Scale, which combines a numerical rating scale with a verbal rating scale, is a more precise assessment than using a numerical or verbal rating scale alone (Zhang et al., 2008).
Approximately 61.1% of the Chinese patients in this survey were treated inadequately according to the PMI, which only captures the balance between pain intensity and medication type and ignores other important factors, including dosage, which is a determining factor in pain relief (Gan, 2017). Therefore, the pain management outcomes may be worse than those reported herein. Ethnic differences in pain sensitivity have also been reported in previous studies; Asian-American individuals tend to have a more sensitive pain perception and lower pain tolerance than white Americans (Ahn et al., 2017). It may be that Chinese patients tolerate a higher pain intensity than they reported, which could lead to a false phenomenon in pain management outcomes. These assumptions need further research in the future.
Conclusions
Patients’ perceptions of pain management outcomes in the United States were better than those reported in China. Multiple modes of analgesia, scheduled analgesic orders, the amount of provided information and patient involvement in decision making contribute to higher levels of perception in the United States. The reluctance to prescribe strong opioids and the low priority of pain management in clinical practice have significantly impaired patient outcomes in China. Patient education and the degree of pain relief are the most important predictors of patient satisfaction in both countries. To develop and promote a safe and effective pain management environment, organizational structures and multidisciplinary cooperation, especially the involvement of pain management experts or anesthesiologists, are highly recommended (American Society of Anesthesiologists, 2012; Chou et al., 2016). More primary obstacles to pain management may originate from the culture or context of the facilities (Alaloul et al., 2017) and from the opportunity (or lack thereof) to implement changes by applying evidence to practice (Brown & McCormack, 2005). A successful pain management program relies on clear policies and effective support from a multidisciplinary team that is backed by leadership support (Tsao & Hsieh, 2015). Individualized pain risk assessment and stratified pain management protocols are promising trends for improving patient outcomes and efficacy in pain management (Peng et al., 2019). Establishing procedure-specific evidence-based recommendations and incorporating pain management in daily clinical pathways may improve patient pain outcomes in China by improving the priority level of pain management and reinforcing compliance with guidelines (Joshi et al., 2019; Rawal, 2016). Furthermore, given the high consensus for opioid addiction worldwide, any pain management program should increase their emphasis on nonpharmacological interventions to relieve postoperative pain.
Footnotes
Acknowledgements
We would like to acknowledge the China Scholarship Council for supporting the living expenses of the first author during visitation at UNC-Chapel Hill. We would also appreciate the participation of the surveyed hospitals, patients, and data collectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the School of Nursing in Peking Union Medical College, Chinese Academy of Medical Sciences and the School of Nursing, University of North Carolina at Chapel Hill (UNC-Chapel Hill).