
Abstract
The goal of this study was to examine current rates of resident deaths, Emergency Department (ED) use within the last year of life, and hospital deaths for long-term care (LTC) residents. Using a mixed-methods approach, we compared these rates across four LTC homes in Ontario, Canada, and explored potential explanations of variations across homes to stimulate staff reflections and improve performance based on a quality improvement approach. Chart audits revealed that 59% of residents across sites visited EDs during the last month of life and 26% of resident deaths occurred in hospital. Staff expressed surprise at the amount of hospital use during end of life (EOL). Reflections suggested that clinical expertise, comfort with EOL communication, clinical resources (i.e., equipment), and family availability for EOL decision making could all affect nondesirable hospital transfers at EOL. Staff appeared motivated to address these areas of practice following this reflective process.
Introduction
As the population ages, more people will die in long-term care (LTC) homes. In Canada, currently 27% of residents die in LTC annually (Jayaraman & Joseph, 2013; “Quick Stats: Continuing Care Reporting System,” 2014), with 62% to 71% of them being transferred to the hospital within the last year of their life (“Quick Stats: Continuing Care Reporting System,” 2014). Unfortunately, research has shown that palliative care is suboptimal in LTC, with pain and other symptoms being poorly managed especially for those with dementia (Teno et al., 2004); lack of attention given to advance care planning (Castle, 1997); issues of loss, grief, and bereavement (Waldrop & Kusmaul, 2011); widespread use of feeding tubes (Mitchell, Teno, Roy, Kabumoto, & Mor, 2003); and excessive reliance on hospitalizations (Menec, Nowicki, Blandford, & Veselyuk, 2009; Miller, Gozalo, & Mor, 2001). Given the growing demand for palliative care principles within LTC and the increased awareness of service inadequacies, frameworks to guide the implementation of palliative care practices within LTC have begun to emerge (Brazil et al., 2004; Sussman et al., 2016).
Many barriers to optimal palliative care in LTC homes have been identified, including a lack of knowledge, workload demands, and a failure to identify impending death and implement a timely end-of-life (EOL) care plan (Kaasalainen, Brazil, Ploeg, & Schindel, 2007; Kaasalainen, Sussman, Neves, & Papaioannou, 2016; Miller, Teno, & Mor, 2004). Unfortunately, decisions to implement such a plan are usually made after hospitalization of an LTC resident, rather than proactively and pre-emptively discussing these issues with the resident and family members prior to their onset. These decisions become even more complicated as most LTC residents die from noncancer conditions, such as co-occurring dementia, heart failure, and/or respiratory conditions, where prognostication is challenging (Berta, Laporte, Zarnett, Valdmanis, & Anderson, 2006; Doupe et al., 2011; Hirdes, Mitchell, Maxwell, & White, 2011). Burdensome interventions and hospitalizations negatively affect the quality of EOL care for residents, families, and staff (Mitchell et al., 2003). Yet, overreliance on hospitalizations at EOL are still commonplace in LTC environments (Hall, Schroder, & Weaver, 2002; Menec et al., 2009; Miller et al., 2001).
This substudy was embedded within a larger study that evaluated the Strengthening a Palliative Approach in Long-Term Care (SPA-LTC) program to improve the quality of living and dying for LTC residents and their family members. SPA-LTC aims to build capacity in LTC homes to pre-emptively involve residents and their family members in discussions about goals of care, including preferred location of death, to avoid unnecessary hospital use at EOL. This article reports on the baseline data that were collected and a quality improvement initiative conducted with staff to explore potential explanations of the baseline results regarding hospital use at EOL.
Specifically, the purpose of this substudy was to examine current rates of resident deaths, Emergency Department (ED) use within the last month and week of life, and hospital deaths for LTC residents. In addition, we compared these rates across four LTC homes in Ontario, Canada, and explored potential explanations of variations across homes based on a quality improvement approach.
Method
This study is informed by Participatory Action Research, which aims to pursue action (or change) and research (or understanding) within an emergent process (Dick, 2009). A mixed-method (qualitative and quantitative) multiple case study design (four LTC homes as “cases”) was used to address the study purpose (DiCenso, Hutchinson, Grimshaw, Edwards, & Guyatt, 2005; Morse & Niehaus, 2006; Yin, 2009). Case study designs are ideal for examining the interplay between process questions and outcomes (Yin, 2009). Chart audit data were collected and analyzed followed by a focus group held at each LTC site to allow staff to reflect on the chart audit data. Ethical approval was obtained at two university-affiliated ethics boards (McMaster University and McGill University).
Settings
Four LTC homes in southern Ontario were selected representing the mix of contexts found in LTC homes including for profit; not for profit; large (150 beds), medium (100-150 beds), and small (less than 100 beds); high turnover and low turnover; religious based versus secular (see Table 1; DiCenso et al., 2005). Site 1 was a 115-bed home, not-for-profit, that was religious based and employed two advanced practice nurses. Site 2 was a smaller, 64-bed home that experienced moderate turnover of administrators (i.e., four administrators over past 10 years). Site 3 was a large LTC home with 206 beds, employed the largest number of staff and also had moderate turnover of administrators. Site 4 was a medium-sized facility with 169 beds and had high ethnocultural diversity among residents and their family members.
Characteristics of Case Sites/LTC Homes.
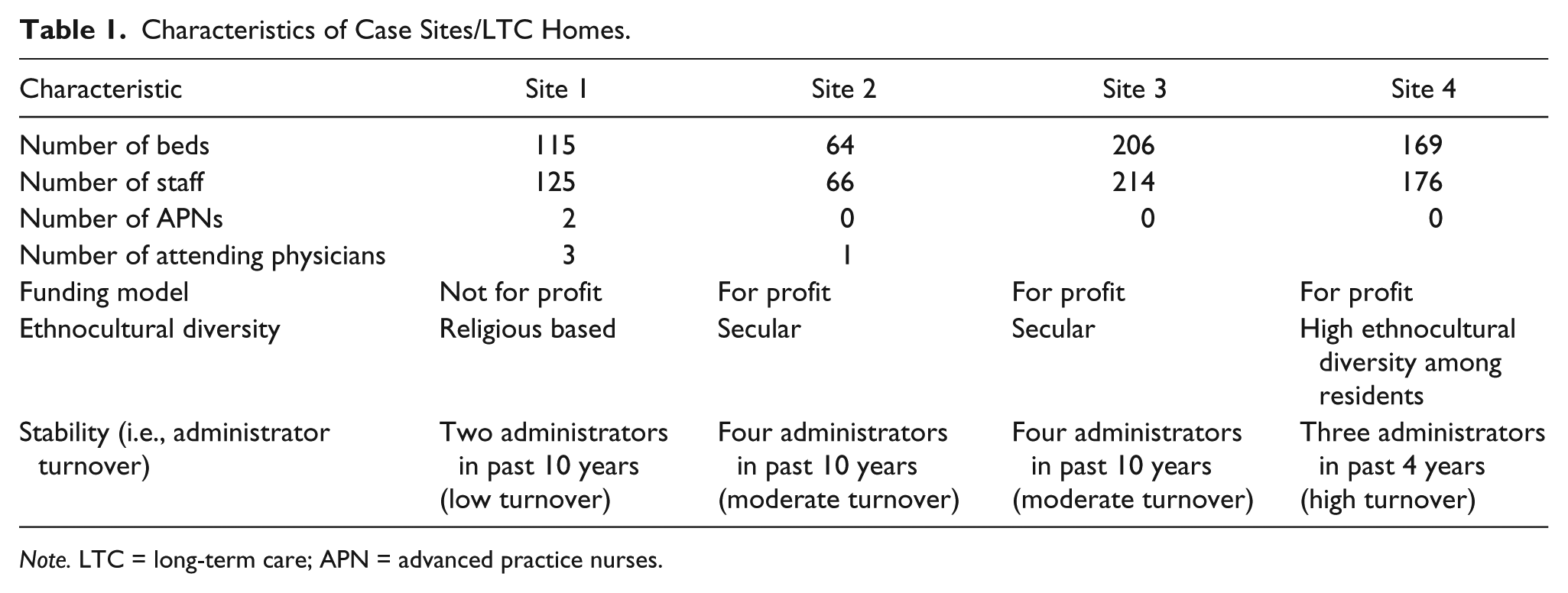
Note. LTC = long-term care; APN = advanced practice nurses.
Data Collection and Analysis
Chart audits
Administrative data were collected by a staff member from each LTC home for the following indicators over a 1-year period: (a) resident deaths; (b) deaths that occurred at the hospital versus LTC home; (c) ED visits in the last year, month, and week of life for each resident; (d) planned versus unplanned ED visits; and (e) ED visits that became hospital admissions. The decision to designate an ED visit as planned versus unplanned was determined by reviewing the resident chart data. Planned or appropriate ED visits were defined as those that were deemed medically necessary by the physician or charge nurse evidenced by diagnostic tests and/or sudden and severe onset of an illness and/or as a result of advance care planning decisions. Alternatively, an unplanned or inappropriate ED visit was determined as being at the request of the family (against the physician/nurse’s judgment) or because the physician was not comfortable treating the resident in the home (i.e., for certain pain management issues, poor intake). Chart audit data were analyzed using descriptive statistics (i.e., means, SDs, frequencies, percentages) for each home separately and then summarized across all four sites.
Focus groups
A focus group was held at each LTC home. Participants included members of the interdisciplinary site palliative champion team, ranging from three to seven staff in each focus group. Participants included nurse managers and other licensed nurses, social workers, physiotherapists, recreation staff, and dietary aides.
A summary of the chart audit findings for both the site-specific data and average across all sites was shared and discussed at a focus group meeting for each site. These chart audit findings were presented to staff at each site to raise awareness and stimulate reflections on local factors affecting hospitalization trends at EOL. Staff were probed to reflect on potential reasons why their home-specific findings were either higher, lower, or similar to the average rates across all four homes. All deliberations were audio recorded, transcribed, and thematically analyzed.
Questions were asked relating to their experiences, needs, strengths, and concerns providing (or receiving) palliative care in their organization.
Consistent with a case study approach, cross-site comparisons were conducted to distinguish site-specific themes from cross-site themes (Yin, 2009). Other factors that could help explain outcomes such as local contextual factors (community resources) and organizational features were also explored.
Results
Chart Audits
Chart audits revealed that 26% of LTC residents on average across all four sites died in the past year, with the majority of resident deaths occurring at the LTC home (71.5%; Table 2). Of these residents who died over the past year, 65.3% of them visited EDs during the last year of life: 45.8% with ED visits in their last month of life and 27.1% in their last week of life. The majority of residents had planned/appropriate ED visits (83%) and 89.4% of all residents who visited the ED over the past year were admitted to the hospital.
Chart Audit Results for All Sites.
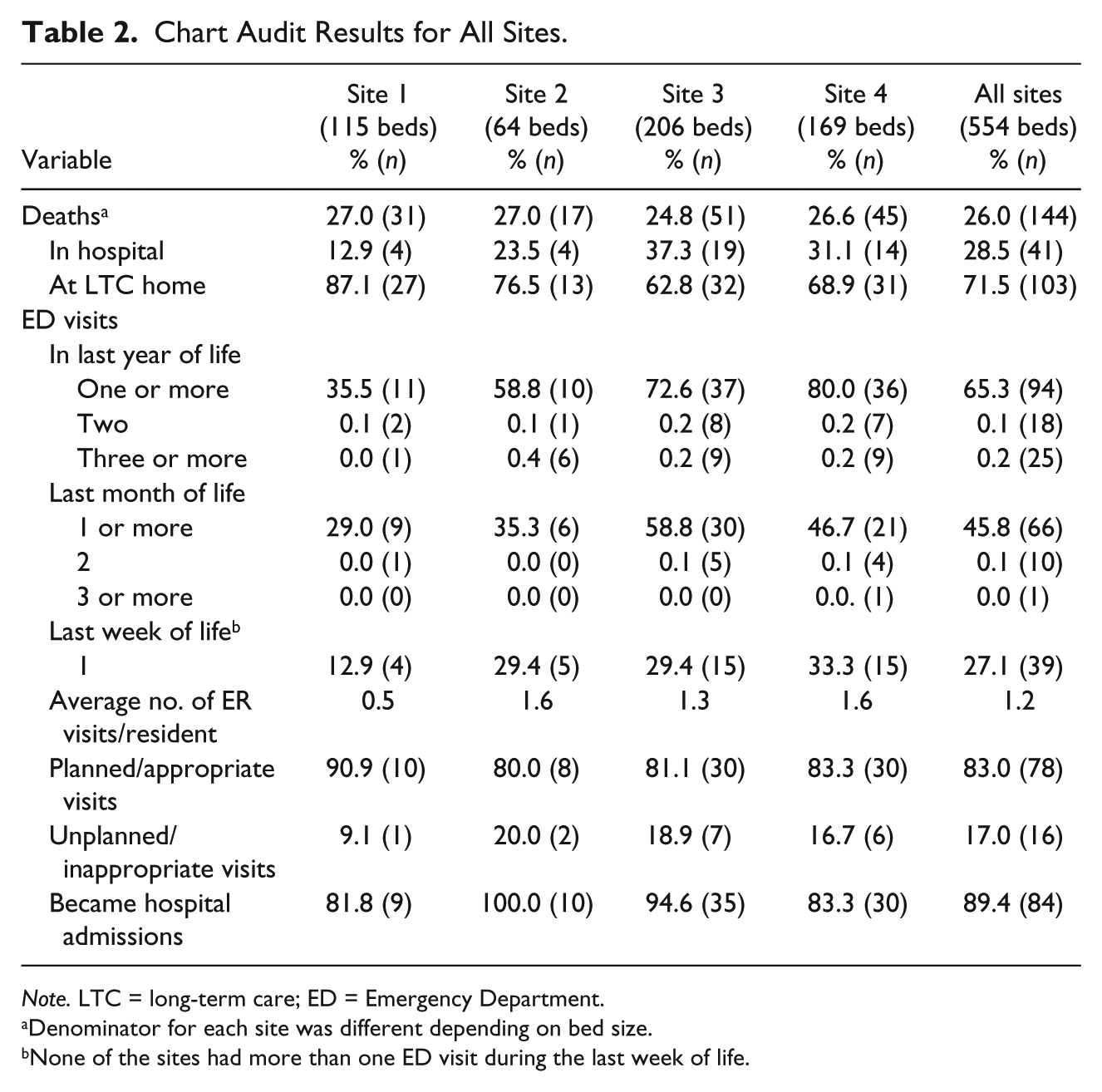
Note. LTC = long-term care; ED = Emergency Department.
Denominator for each site was different depending on bed size.
None of the sites had more than one ED visit during the last week of life.
Site 1 had the most residents die in their LTC home (87.1%) with the fewest ED admissions in the last year of life (35.5%). Sites 3 and 4 had above average rates of hospital deaths (37.3% and 31.1%, respectively) and ED visits during last year of life (72.6% and 80.0%, respectively).
Focus Groups
Characteristics of Participants
In total, 21 individuals participated in the focus groups (Table 3). Most of the participants were female (81%), were less than 44 years of age (76%), and were nurses (43%). Most of the participants were employed by the LTC home (80%) in a full-time position (86%), and had received some palliative training in the last year (81%).
Demographics of Focus Group Participants.
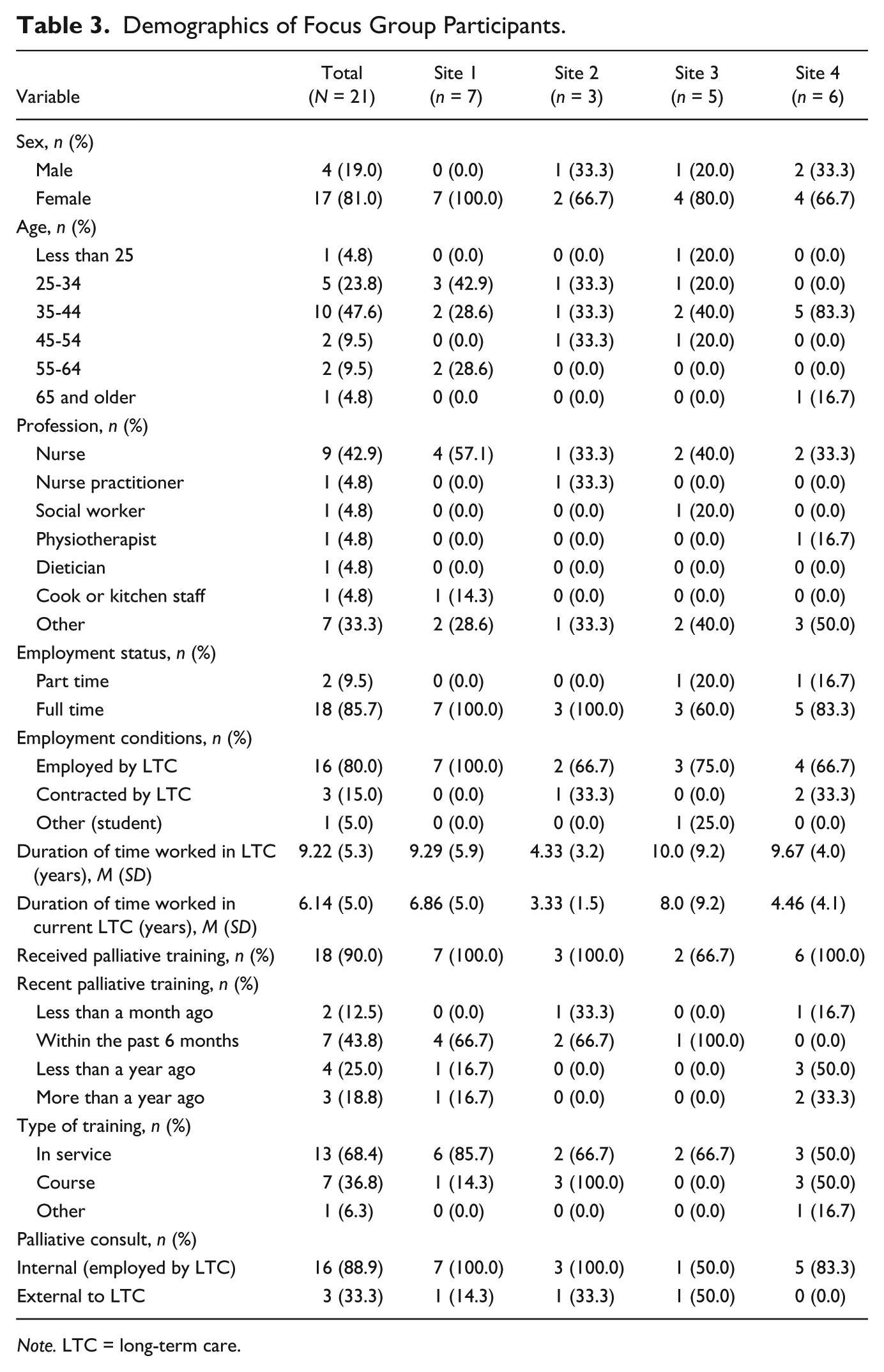
Note. LTC = long-term care.
Overview of Findings
Overall, participants were quite receptive to learning about their local chart audit findings and, across sites, they recognized their strengths and areas for improvement related to ED use at EOL. The majority of participants stated that they felt the chart audit findings were reflective of the type of residents who are being admitted into their LTC home. In addition, they identified key factors that could have affected their ED rates, including (a) clinical expertise of LTC staff within a team approach, (b) use of external supports to build capacity within LTC, and (c) communication and engagement with family about EOL issues. Staff appeared motivated to address these areas of practice following this reflective process.
Surrounding Context of Their LTC Home
Focus group participants reflected on the chart audit data and offered some explanations for their local rates of resident deaths and use of EDs. For example, staff felt that the high death rates could be due to residents coming to LTC home frailer and with more complex needs. A participant in Site 4 stated, “a lot of individuals today are coming into the home much, much later . . . because people are living independently longer but when they do come in [to LTC] they really need to come.”
For the LTC homes with the high ED visits, some staff stated that they were surprised to see that their rates were so much higher compared with the averages. One participant from Site 3 stated, Yes I was surprised that we were a bit higher [with ED transfers] . . . I thought we would be the same or a little lower . . . I’m quite surprised with those in the last week of life . . . I guess it depends on the situation but overall it would be nice to see a decrease at least in the last month of life.
Participants explained how their home had unique challenges, such as lower socioeconomics and multiculturalism, which may have affected their high rates as well, compared with the other LTC homes. A participant at Site 4 explained, you need to see the other side . . . the socioeconomic status of the surrounding area near us really affects the type of resident that come into the LTC home . . . when they come in, they are in crisis . . . another consideration is we have a very multicultural environment so the ones teaching [staff] need to be culturally competent, aware of diversity so different people learn in different ways . . . and the families as well are from different cultures.
Clinical Expertise and Team Approach
The need for clinical expertise among staff, especially related to palliative and EOL care, was highlighted as an important area to minimize ED visits for LTC residents. A participant in Site 2 elaborated, sometimes clinical skills and judgement interfere . . . let’s say when someone falls they immediately think we should send this person to the ER . . . but why can’t we observe first and check before sending them [to the ED].
The role of registered nurses was highlighted as an enabler to help keep residents in LTC instead of being transferred to the ED: “we utilize our unit managers, which is our RN, who works with the team for that in-depth assessment . . . so that we can give recommendations to the doctor and the families to keep them here” (Site 1).
A team approach, based on collaboration and effective communication, was identified as an important strategy to limit ED visits. Site 1 also highlighted how their attending physicians aim to keep LTC residents “at home,” as opposed to an on-call physician who “usually just sends residents to the hospital.” To facilitate optimal physician–nurse communication, participants from Site 1 stated that using situation, background, assessment, recommendations (SBAR; “SBAR Technique for Communication: A Situational Briefing Model,” 2017) assists staff in gathering appropriate information for discussion with physicians about EOL issues. In this manner, the team works together to problem solve and make decisions about resident care, in light of resident and family wishes.
Optimizing External Supports to Build EOL Capacity in LTC
Participants at three of the sites stated that the outreach nurse practitioners play an important role in preventing ED transfer at EOL. A specific example was described: We had the nurse practitioners come in and help us do some training to keep one of our residents here instead of being transferred to the hospital . . . our nurses learned how to cauterize, went above and beyond learning some special skills so she could remain here until she died . . . because that was what the issue was, just to stop the bleeding, instead of sending her out and back again . . . we trained our staff and they were willing to learn—I think that was pretty amazing . . . because a lot of LTC homes would not have done that kind of thing . . . so we were able to keep her here until she died. (Site 1)
Moreover, participants in Site 4 questioned whether the staff have less expertise because they recently lost access to a nurse practitioner, which may have contributed to their higher ED visits over the past year.
Communication With Family About Palliative/EOL Issues
The important role of the family was mentioned repeatedly. Many participants spoke of the sense of guilt that family members have and “it is family guilt that makes them send residents to the hospital 10 times in two weeks” (Site 4), and that family view the hospital as “a voice of authority that provides validation that there really is nothing more that can be done” (Site 2). Others stated that family dynamics can affect treatment decisions where “some family members understand when residents are palliative, but other family members insist on heroic measures” (Site 2). Yet, “you have to respect what the family’s wishes are . . . so sometimes we might not be on board to say that’s a good decision but we still have to respect what their decisions are” (Site 1).
Participants across all the sites agreed that the chart audit findings showed that staff need to develop positive relationships with family and have more discussions with both residents and families earlier on in the disease trajectory, even before admission to LTC. A participant from Site 3 states, “I think it [chart data] emphasizes the importance of having that conversation early because we are not having that conversation in a timely manner.” A participant from Site 4 added, I think that people don’t realize that death is a part of life and we go through different stages . . . so if we accept death as a part of life, you allow the person to die in peace rather than let them be harassed and poked and probed . . . you have these discussions with these people early on then we can stop them being sent to the hospital when they can’t even say “well no, I don’t want to go.”
Participants from Site 2 stated, meeting with families at the annual care conferences helps families to be more prepared and think about place of death . . . whereas before families were just given a form and told to sign it . . . but now we explain to them this means this and this means this.
Others stated that they felt they really did not have a choice but to send residents to the hospital because it was documented to do so in the residents’ charts: You don’t really have a choice—you have to send them unless the family comes in and says, “OK that’s fine, I understand, I don’t want them to go [to the hospital] . . . but they have to come and sign the paper, otherwise you can’t change it.” (Site 3)
Participants highlighted some goals that they hope to achieve to improve their rates of ED visits. One participant stated, “I’d like to see a reduction in the amount of hospital visits in the same week and month because that would show that maybe we are having the conversations earlier” (Site 3).
Discussion
These study findings add to the body of knowledge related to resident deaths in LTC and use of the ED and hospital admissions at EOL and it helps uncover potential strategies to minimize unnecessary ED visits and allow residents to die in their LTC home if preferred to dying in the hospital. In addition, this study explores the process of audit and feedback as a quality improvement strategy in LTC homes. These findings are consistent with Canadian rates of residents deaths in LTC (27%; “Quick Stats: Continuing Care Reporting System,” 2014) and hospital use/ED visit within last year of life (62%-71%; Berta et al., 2006; “Quick Stats: Continuing Care Reporting System,” 2014). These findings are concerning given death rates in LTC are predicted to rise to 39% by the year 2020 (Jayaraman & Joseph, 2013), which could become quite costly for the health care system. Similar trends have been noted from other countries including the United States (U.S. Department of Health and Human Services, & U.S. Department of Labor, 2003), the United Kingdom (Lievesley, Crosby, & Bowman, 2011), and Australia (Australian Institute of Health and Welfare, 2007).
Focus group findings highlighted the importance of clinical expertise among LTC staff to minimize ED visits. Arendts, Reibel, Codde, and Frankel (2010) found similar qualitative findings, in that LTC staff stated that inadequate staffing intensity and staffing mix compromised the capacity of staff to make appropriate decisions regarding ED visits. In fact, McGregor et al. (2015) found that with less than 24/7 registered nurse coverage, LTC residents had a higher risk (Relative Risk = 1.11, confidence interval [CI] = [0.78, 1.58]) of having an ED visit. Given the increasing complexity of LTC residents, it is important to ensure that LTC homes employ staff with the necessary skills to care for these complex residents, such as registered nurses, across all shifts to reduce unnecessary costs of ED visits.
In addition to licensed nurses, these study findings also point to the added benefit of the nurse practitioner role in LTC. For example, Site 1 provided an example that illustrated how they were able to keep a resident in LTC by using an external nurse practitioner to help “upskill” staff when needed in a timely manner, thereby allowing the resident to die “at home.” Other research has shown that nurse practitioners care for LTC residents who are dying and their families, collaborate with other health care providers by providing consultation and support to optimize palliative care practices, work within the organization to build capacity and help others learn about their role in palliative care to better integrate it within the team, and improve system outcomes, such as improved accessibility to care and reduced ER visits (Kaasalainen et al., 2013).
In addition, study findings emphasize the important role of LTC physicians and their commitment to keeping residents in LTC during EOL, in that “it needs to be a goal”; otherwise, residents are often sent to the hospital for issues that could have been potentially managed well at the LTC home (Ouslander et al., 2010). For example, Casarett and colleagues (2005) found that a physician notification strategy and communication about resident preferences (e.g., goals of care, treatment preferences, palliative care needs) resulted in significantly more residents deemed palliative and having fewer hospitalizations. In addition, families rated the residents’ care more favorably than those in the control group. The importance of the physician role in communicating with residents and families to help them understand the nature and extent of decline for residents, how it can affect the quantity and quality of life, and empowering residents and families to engage in decision making about preferences for care, including place of death, has the potential to greatly improve quality of life and reduce hospital use at EOL (Moorehouse & Mallery, 2012; Zweig, Popejoy, Parker-Oliver, & Meadows, 2011).
Finally, this study highlights how the use of audit and feedback can be used as a strategy for quality improvement in LTC homes. All too often, research sites are not informed about study findings that they have been engaged in but report that they would like to be, given the time, interest, and efforts that they have contributed (Ivers et al., 2014). By collecting data (audit) and reporting it back to health care providers (feedback), this can prompt clinicians to modify their practice if it is inconsistent with a desirable target (Ivers et al., 2012; Kaasalainen et al., 2010). In this study, this audit and feedback process served as one of the key learnings of this study and supports the use of this strategy as a way to improve clinical practice.
There were strengths and limitations to this study. Using a case study approach to explore case-specific data as well as comparing data across sites allowed us to view the data in different ways. This was particularly meaningful for staff to allow them to reflect on their own site data and compare it with the average score across LTC homes. As such, we were able to uncover potential explanations for the differences in findings across sites or potential reasons for higher ED use (as opposed to causal claims), contextualizing the findings for more in-depth learning. A limitation of this study is its limited generalizability. Although these sites were purposely chosen to represent diversity, the findings may not be generalizable to other LTC homes in different regions.
Conclusion
Using a case study approach, findings can be both analyzed at the site level and summarized across sites for different uses. One way to use the data was to examine localized chart audit findings combined with group reflective opportunities, which served to raise awareness and engage staff in collective solutions to address preventable hospitalizations at EOL. It is hoped that these study findings can contribute to a greater awareness of possible strategies that LTC homes can use to minimize unnecessary hospitalizations at EOL, and improve both the quality of living as well as dying for residents and their family members.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Canadian Frailty Network, which is supported by the Government of Canada through the Networks of Centres of Excellence program.