
Abstract
Contemporary community-based health promotion is within a complex and transforming social landscape. Traditional place-based understandings of “community” now contend with fluid, transnational, and virtual social networks, shifting definitions of belonging, and developing political, economic, and technological conditions. Community-engaged research (CEnR)—including community-based participatory research (CBPR)—provides a critical framework for addressing these changes. CEnR's focus on partnership, co-learning, and equitable power-sharing places it as a valuable approach to uncovering emerging health priorities, devising contextually relevant interventions, and advancing health equity. This article outlines new directions in community-based health promotion that embrace social complexity, intersectionality, and narrative approaches. This discussion outlines a blueprint for scholars, practitioners, and community members to envision responsive, justice-oriented, and sustainable health promotion strategies that align with communities’ evolving social environments.
Keywords
Introduction
Over the past several decades, community-based health promotion has emerged as a powerful paradigm in public health by emphasizing local knowledge production, cultural context, and participatory decision-making in addressing complex health challenges. Influenced by ecological models of health (Green & Kreuter, 2005; McLeroy et al., 1988) and grounded in principles of empowerment and equity (Minkler & Wallerstein, 2008; Wallerstein & Duran, 2010), this approach stands in contrast to traditional top-down, individual-level interventions. However, the world in which communities operate is shifting. Globalization, technological innovations, neoliberal policy frameworks, environmental crises, and demographic transitions have made the notion of “community” far more porous, fluid, and heterogeneous than previously understood (Delormier et al., 2009; Israel et al., 2012).
In this complex era, community-engaged research (CEnR), including community-based participatory research (CBPR), offers a robust framework for navigating new directions in community-based health promotion. The guiding principle of CEnR—that local stakeholders are co-creators of knowledge and essential partners in research—ensures that health promotion efforts stay relevant, responsive, and transformative (Wallerstein et al., 2017). By foregrounding community priorities, lived experiences, and cultural nuances, CEnR challenges paternalistic traditions in research, instead supporting reciprocal learning, capacity building, and long-term investment in community health infrastructures.
This article outlines how CEnR can guide future community-based health promotion. It begins by revisiting the historical context and theoretical foundations shaping the field. It then explores how social, political, economic, and technological transformations demand more fluid conceptualizations of community and place. Subsequently, the manuscript discusses narrative and arts-based methods, digital media's expanding role, and the importance of intersectionality. Of focus is how community stories, when centered, can catalyze policy changes and inform professional practice. The article discusses limitations, ethical considerations, and methodological adaptations for improving CEnR's efficacy. Scholars, practitioners, and community members can embrace complexity, foster authentic engagement, and develop strategies to meet evolving community health needs in the 21st century.
Historical Context and Evolution of Community-Based Health Promotion
Several theoretical, social, and policy shifts over the past half-century trace the evolution of community-based health promotion. Early public health interventions adopted biomedical or behavioral models that aimed to change individual risk factors. This focus paid less attention to the broader environmental and social contexts. As individual behaviors are inseparable from the social and structural conditions in which they occur, health promotion emphasizes social determinants and community-level strategies (Kickbusch, 2003; WHO, 1986).
The Ottawa Charter for Health Promotion (WHO, 1986) marked a theoretical turning point defining health as an outcome of policies, environments, and supportive social conditions. Ecological frameworks (McLeroy et al., 1988) also highlighted the interaction of individual, interpersonal, organizational, community, and policy factors on health. Over time, approaches such as CBPR emerged to operationalize these conceptual advances, embedding research within community priorities and leveraging local expertise (Israel et al., 2012; Minkler & Wallerstein, 2008).
As the field developed, new scholarship identified limitations in traditional community-based approaches. Many early interventions, for instance, still treated community members as passive recipients or “subjects” of research. Over time, sustained critiques from feminist scholars, critical race theorists, Indigenous activists, and disability advocates pushed for more radical collaboration, recognizing that communities are best positioned to name their challenges, define goals, and design culturally grounded interventions (Minkler, 2005; Smith, 1999). This shift toward more egalitarian and collaborative relationships laid the foundation for contemporary CEnR paradigms.
Rethinking Community in a Globalized, Digital Age
“Community” has conjured images of people living in a defined geographic area, sharing cultural norms, and holding regular face-to-face interactions. While these place-based meanings stay relevant, especially for neighborhood-level interventions (e.g., improving local parks or water quality), many communities today transcend geographic borders. Diaspora networks, online interest groups, and social movements organized through digital platforms have reshaped how individuals form collective identities (Hall et al., 2016).
Communities now emerge around shared identities or experiences beyond physical location alone. For example, LGBTQ+ individuals who meet in online forums form communities with distinct health needs that differ from those of a geographically bounded neighborhood. In this way, refugee groups across multiple towns keep cohesive cultural and social ties. These transformations call for “community” to be understood as dynamic, multi-layered, and renegotiated. Such recognition fosters research approaches to fluid boundaries, trans-local interactions, and cultural hybridity.
In environmental displacement, climate migration, and pandemic-driven social distancing, communities develop new coping strategies and forms of solidarity (Cunsolo Willox et al., 2012). By recognizing the community as a developing set of relationships, researchers can better capture emergent health priorities—such as mental health struggles linked to instability, digital divides in healthcare access, or the need for specific telemedicine services. Community-engaged approaches can use participatory mapping, digital storytelling, and policy dialogues to understand and respond to these forming health ecologies.
Theoretical Foundations of Community-Engaged Research
CEnR draws from diverse intellectual traditions emphasizing equity, power-sharing, and participatory knowledge creation. Freire's (1970) pedagogy of the oppressed highlighted dialogue and co-learning, countering top-down educational models. Feminist and critical race theories further advanced the argument that marginalized communities hold valuable experiential knowledge that must shape research agendas (Bowleg, 2012; Crenshaw, 1991). Within health promotion, these theoretical traditions inform social justice frameworks. Here, interventions seeking to improve health outcomes benefit from prioritizing root factors, such as structural racism, neoliberal austerity, or environmental injustice (Wallerstein & Duran, 2010).
Social-ecological models remind us that health is influenced by factors across multiple levels of the social environment (Israel et al., 2012; McLeroy et al., 1988). When integrated with an intersectional lens (Bowleg, 2012; Crenshaw, 1991), CEnR can uncover how overlapping systems of oppression shape the distribution of health resources and risks. Geographic marginalization and discrimination based on race, immigrant status, or disability can limit a community's access to healthy foods. These layered dynamics suggest researchers and practitioners acknowledge structural inequities and work to redress them through the research process itself—by building local capacity, distributing financial resources equitably, and sharing decision-making power.
Intersectionality and the Complexity of Community Identities
Intersectionality—the idea that social categories such as race, gender, class, and ability intersect to create unique experiences of privilege or oppression—has become indispensable in community-based health promotion (Bowleg, 2012; Hankivsky & Christoffersen, 2008). As communities grow more heterogeneous and interconnected, categorizing individuals by race or gender is insufficient. Instead, intersectionality illuminates how multiple, interacting identities shape health outcomes and experiences of healthcare systems.
For instance, a community-based HIV prevention program must consider not only the sexual orientation of participants but also racial discrimination, historical trauma, language barriers, and socioeconomic constraints. Obesity prevention initiatives in low-income neighborhoods need to account for the intersection of poverty, cultural food practices, environmental pollution, and gender roles in household food procurement. By applying an intersectional perspective, community-engaged researchers can promote more culturally relevant health plans, respect locality, and be cognizant of the political and economic forces shaping health behaviors.
Methodological Innovations: Narrative, Arts-Based, and Participatory Techniques
Researchers are pivoting to narrative and arts-based methods. Traditional focus groups, surveys, and epidemiological analyses remain valuable but may not always convey how people experience health and illness in their everyday lives. Narrative methods—such as oral histories, digital storytelling, photo-voice, and community theater—offer a distinct qualitative depth to a speaker's point of view (Catalani & Minkler, 2010; Riessman, 2008; Wang & Burris, 1997).
Narrative Approaches and First-Person Accounts
Narratives are a powerful tool for understanding how community members make meaning of health, navigate barriers, and envision alternatives. First-person accounts reveal the subjective dimensions of health—fear, hope, stigma, resilience—that may be hidden in more conventional data. For example, migrant farmworkers’ stories about pesticide exposure can show the embodiedness of agricultural policies, market demands, and harm. Older adults’ stories about neighborhood walkability can highlight intersections of aging, mobility, social capital, and infrastructural neglect. Narratives can guide interventions. Community members’ stories detailing neighborhood violence can persuade policymakers to prioritize trauma-informed community policing or mental health services over statistics. As a result, narrative methods have become a form of activist scholarship, bridging the gap between research and advocacy (Cunsolo Willox et al., 2012; Minkler, 2005).
Arts-Based and Creative Expressions
Beyond storytelling, arts-based methods—such as participatory photography, mural-making, spoken word, and dance—provide alternative avenues for community expression. Participants may find communicating complex emotions, cultural traditions, or health struggles easier through visual or performative art. For example, a mural project can showcase a community's historical relationship with its environment and its struggles for clean water or green space. These representations can mobilize collective action by fostering local pride and bridging cross-sector partnerships with local artists, patrons, and cultural organizations (Leavy, 2015).
Arts-based methods similarly democratize research by inviting participation from individuals uncomfortable with formal interviews or surveys. Offering multiple modes of communication is a way these methods value different learning styles and cultural epistemologies. This approach promotes inclusivity and respects community agency, allowing individuals to shape how their experiences are represented and understood.
Participatory Mapping and Visual Tools
Participatory mapping is where community members co-create spatial representations of their environment. Maps can highlight where health-promoting resources (e.g., farmers’ markets or clinics) and health risks (e.g., pollution sources or unsafe intersections) cluster. Mapping also helps to visualize relationships between social processes and physical space, revealing patterns of inequality or access that might not surface through narrative data alone (Corburn, 2005). Researchers and communities can co-generate actionable insights for urban planning, transportation policies, and environmental regulation by integrating qualitative narratives with GIS-based participatory mapping.
Digital Media, Technology, and Virtual Communities
The prevalence of digital media and communication technologies represents another area with opportunities—and challenges—for community-based health promotion. Social media platforms, mobile health (mHealth) interventions, and telemedicine services can broaden the reach of public health messages and facilitate community engagement in real-time (Aranda-Jan et al., 2014). Communities might use Facebook or WhatsApp groups to share information about local events, programs, or resources, creating virtual support networks that transcend geographic constraints.
Digital storytelling tools, such as short videos, podcasts, and interactive websites, are a medium in which individuals can create and disseminate their health narratives. Digital formats can amplify marginalized voices, bringing community stories to policy domains that might remain inaccessible. Smartphone apps can be a valuable and accessible tool to document identified hazards, report service gaps, or evaluate broader social health interventions, contributing to data collection and analysis.
Technology also introduces new concerns. The digital divide is still a significant barrier, as not all community members have equal access to smartphones, high-speed internet, or digital literacy training (Aranda-Jan et al., 2014). Digital-only approaches may unintentionally leave out groups, including older adults, low-income families, undocumented immigrants, or those with limited English proficiency. Ensuring fair access to and literacy about digital tools is vital in CEnR.
In this context, privacy and data security become paramount when handling sensitive health information online. Ethical guidelines and community-led data stewardship practices must be in place to protect participants from surveillance, stigmatization, or exploitation. The collaborative development of data governance frameworks can ease trust and ensure that digital methods enhance rather than undermine community autonomy.
Environmental Transformations, Displacement, and Health Inequities
Environmental changes, such as climate-induced disasters and urban gentrification, pose urgent challenges to community health. As extreme weather events, droughts, and pollution reshape environments, communities face new health threats such as water insecurity, vector-borne diseases, and mental distress linked to ecological loss (Braveman & Gottlieb, 2014; Cunsolo Willox et al., 2012). Displacement because of environmental degradation or rising living costs can stress social ties, disrupting cooperative coping mechanisms and cultural practices that once supported well-being.
CEnR in this domain must consider how place attachment, cultural identity, and historical trauma intersect with environmental health. Indigenous communities, for example, may have deep spiritual connections to ancestral lands, and environmental harm can thus make up not only a health risk but also a risk to cultural heritage. Poor urban neighborhoods facing gentrification may not have access to affordable housing, forcing residents to move away from familiar social networks, culturally relevant foods, and trusted health providers, exacerbating health inequities.
Again, by working with communities, researchers can identify meaningful environmental and social well-being indicators. Collaboratively developed adaptation strategies—such as community gardens, traditional healing practices, or policy advocacy campaigns—can mitigate harm and build resilience. CEnR ensures these strategies originate from community visions rather than assumptions from external members.
Health Activism, Education, and Narrative Medicine
Community-based health promotion extends beyond research design and data collection. It can serve as a platform for health activism and community-driven education. Narratives are central here. Disseminating first-person accounts of healthcare discrimination, environmental injustice, or gender-based violence through community forums, art exhibits, or digital storytelling platforms galvanizes collective mobilization (Riessman, 2008). These narratives transform health promotion from a neutral, technical field into an arena demanding confrontation of structural inequities.
Narrative medicine, which emphasizes patient stories in clinical practice, aligns well with CEnR principles (Charon, 2006). By incorporating narrative methods into medical education, training programs, and health professional curricula, clinicians can have the tools to listen for social determinants’ impact on patient experiences and develop more culturally responsive care. When community stories inform health professional training, they help dismantle stereotypes, reduce biases, and encourage healthcare providers to see patients as whole persons embedded in rich social contexts (Kumagai & Lypson, 2009).
Communities can become health educators and advocates, using their expertise to influence policy decisions. For example, imagine a coalition of residents producing a digital documentary about local food deserts and presenting it at a city council meeting to change policies in zoning or subsidies for healthy food vendors. By centering community narratives in policy advocacy, health promotion becomes a lever for broader social transformation.
Policy Implications and Structural Change
One of the most promising aspects of CEnR is its potential to shape policy and institutional practices. Rather than translating findings months or years after a study concludes, CEnR integrates policy considerations from the outset. Community members and researchers can collaborate with municipal officials, school boards, healthcare administrators, or nonprofit leaders to co-design evidence-based and locally-led interventions.
For instance, findings from a participatory mapping project identifying unsafe walking routes to a neighborhood school might lead to immediate infrastructure investments. Stories from refugees facing language barriers in clinics could inform policies on providing in-person interpretation services. Policymakers are more likely to adopt reforms that reflect local realities by legitimizing community-generated data and ideas.
Nevertheless, not all policy environments are receptive. Structural forces—such as austerity measures, corporate lobbying, or institutional racism—may lead some locales to resist community-driven interventions. Researchers and communities must be prepared to engage in sustained advocacy, building alliances with grassroots groups, legal experts, journalists, and other stakeholders. Eventually, these combined efforts shift policy, leading to fairer resource allocation.
Ethical Considerations, Reflexivity, and Sustainability
Ethical considerations are essential in CEnR. Genuine participation comes from long-term trust, transparent communication, and a commitment to equitable benefits. Researchers must avoid exploitative “helicopter” approaches that extract data from communities without providing adequate value in return (Minkler, 2005). Capacity building, co-authorship, financial remuneration, skill development, and sustained relationships help ensure that communities do not serve as research sites but as co-architects of knowledge production.
Reflexivity—a continual process of examining one's positionality, assumptions, and power dynamics—is a core competency in CEnR (Wallerstein et al., 2017). Researchers must ask: Who defines the research questions? Who controls the data? How are findings disseminated, and who benefits? Community expertise, not just academic credentials, is essential for meaningful health promotion innovation, emphasizing reflexive practices’ critical role.
Sustainability is another vital concern. Interventions that address a community problem without building local capacity or changing underlying policies may have a limited impact. Sustainable CEnR strategies focus on institutionalizing community participation in governance structures, training community health workers, and ensuring that local organizations have the resources to continue initiatives after formal research projects end (Israel et al., 2012). This long-term vision fosters resilience and positions communities as active agents of ongoing health promotion efforts.
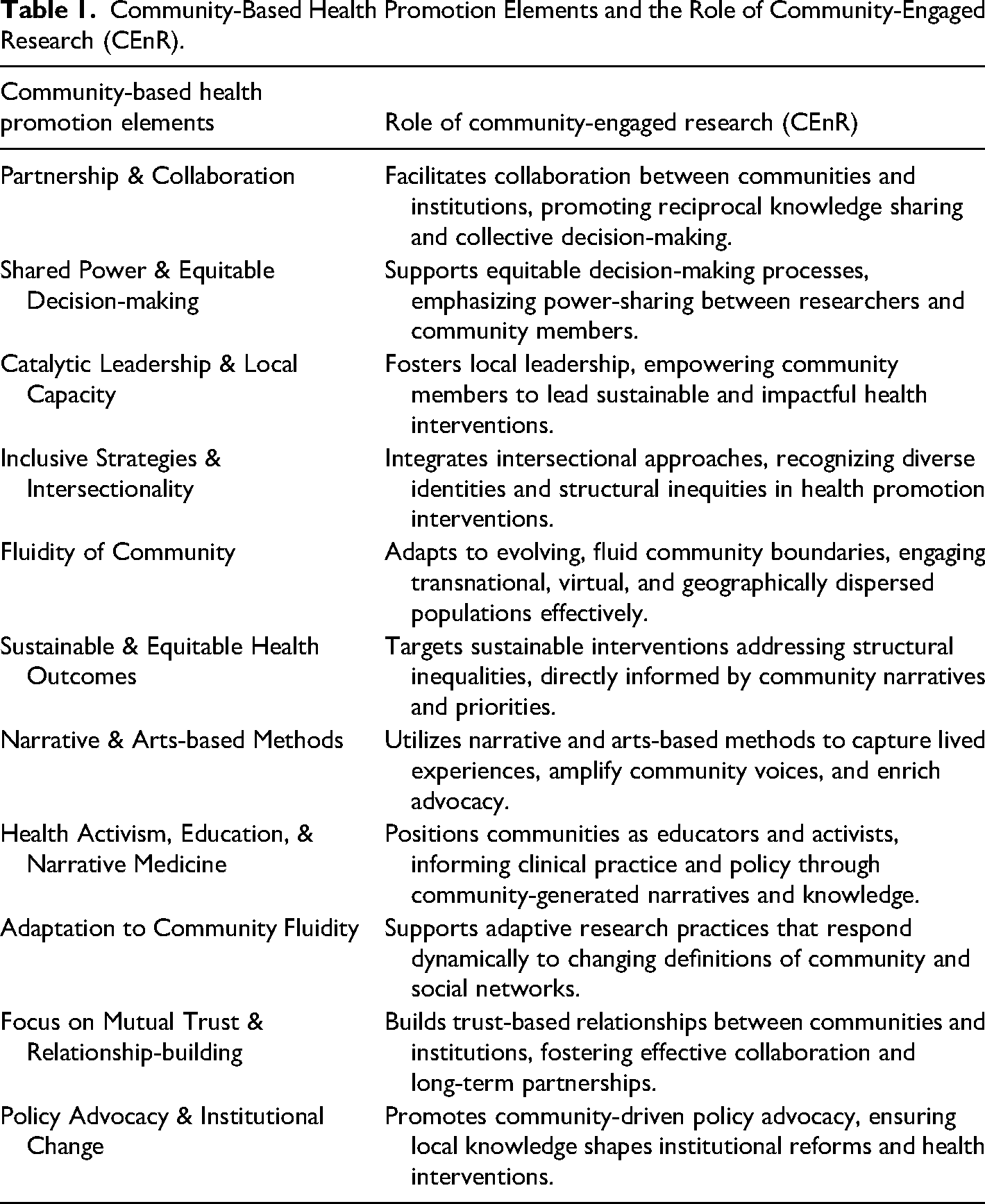
To summarize and clarify the connections among the key elements discussed throughout this manuscript, Table 1 provides an overview of the central components of community-based health promotion and the specific contributions made by CEnR. This table illustrates how CEnR methods and principles can effectively enhance each component, fostering responsive, inclusive, and sustainable interventions.
Community-Based Health Promotion Elements and the Role of Community-Engaged Research (CEnR).
Limitations and Tensions in Community-Engaged Research
Despite its transformative potential, CEnR encounters real limitations. Collaborative processes demand substantial time and trust-building; short funding cycles or academic timelines may strain these efforts. Power imbalances can persist, with academic institutions keeping control over grant funds, authorship decisions, and research framing. Community partners, especially those from marginalized groups, may feel pressured to accommodate academic priorities or methodologies that do not align with their traditions and needs (Minkler & Wallerstein, 2008).
Skepticism towards narratives and arts-based methods, despite their rich context, may arise from policymakers or funders who prefer quantitative indicators of success. Researchers and community partners must work to explain the value of these methods, linking them to measurable outcomes when possible and illustrating their unique capacity to drive community health practices.
The digital environment is also full of uncertainties. While technology can help with participation, surveillance risks, data privacy issues, and the commercialization of community data by technology companies emerge as items of concern. Navigating these issues needs transparent dialogue, established community governance structures, and institutional support for data sovereignty.
Future Directions in Community-Based Health Promotion and CEnR
As communities change, so must our research methods, theoretical frameworks, and partnerships. Future directions include integrating participatory data science tools, using community-led artificial intelligence applications to determine health risks, or employing virtual reality to simulate urban planning scenarios that promote well-being. Interdisciplinary collaborations between public health professionals, urban planners, environmental scientists, anthropologists, digital humanities scholars, and artists can yield novel insights and strategies.
Deeper engagement with decolonizing methodologies (Smith, 1999) guides future community-based health promotion. For Indigenous communities, this may include reaffirming sovereignty over research agendas, integrating traditional knowledge systems, and resisting exploitive practices. For immigrant communities, this may involve recognizing transnational ties, bilingual knowledge production, and policies that extend beyond national borders.
As environmental crises intensify, CEnR must support adaptation, mitigation, and resilience. This includes designing interventions that discuss the root causes of climate injustice, developing culturally grounded mental health support systems for communities facing ecological grief, and advocating for policies that protect natural resources central to community health and identity.
Conclusion
The landscape of community-based health promotion is undergoing profound transformations. Traditional conceptions of community and health interventions must adapt in an era defined by mobility, digital connectivity, and unprecedented social and environmental challenges. CEnR offers a flexible, justice-oriented, and responsive framework for meeting these challenges. By centering community expertise, integrating narrative and arts-based methods, recognizing intersectionality, and assuring that research leads to tangible policy changes, we can forge new directions in health promotion that are both innovative and equitable.
CEnR can move beyond academic silos and technocratic solutions to leverage the collective creativity of diverse communities. Doing so can help us reimagine the boundaries of community-based health promotion that pave the way for long-lasting improvements based on local priorities and honored culture. This vision of community-based health promotion stands ready to respond to ever-changing realities, ensuring that public health remains community-informed and community-led.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.