
Abstract
India has a significant number of people exposed to suicide. The traumatic effects of these experiences, and the healing process of suicide survivors are poorly understood. We investigated suicide survivors’ experiences and post-suicide healing. Interviews were conducted with suicide survivors who received different types of support—home visits before COVID-19 and telephonic outreach during lockdown. Two researchers used “active listening” and “human capacity for response” theory for deductive and inductive coding. Personal and socio-cultural factors affect recovery after suicide. Protective factors include religious or spiritual beliefs, as well as a sense of life purpose. Factors that hinder recovery include lack of social support, unmet need for compassionate understanding, insufficient acknowledgment of personal struggles, and social stigma. Interventions for suicide survivors should consider personal and cultural factors, including psychological and religious needs. Interventions should create safe environments that allow individuals to draw on personal and social resources for healing.
Introduction
Suicide attempters and those who lost someone to suicide are at higher risk of suicide and mental health issues. A greater understanding of their experiences, coping mechanisms, and vulnerability is needed to provide effective support. A study undertaken to examine the association between community vulnerability and social integration in residential stability, divorce, and adherence to Catholicism showed the dual nature of social integration, as a protective and risk factor of suicide and the need to examine cultural aspects in the context of suicide (Brantez & Houle, 2024)
The term suicide “survivors” refers to individuals who have experienced suicide in one form or another, for example, by losing someone as a result of suicide (death survivors); by attempting and surviving suicide themselves (attempt survivors);, or by witnessing the attempted suicide of another person or its aftermath (witness survivors). Survivors can include children, parents, spouses, neighbors, friends, close colleagues, and extended family members. A suicide event usually involves around six survivors, but may include up to 20 extended family members (Berman, 2011). In India, about 170,000 people died by suicide in 2022 and many more attempted suicide and survived, suggesting that at least one million people are directly affected by suicide and may experience its traumatic aftermath. Non-fatal suicide attempts are underreported, but show a higher impact on women than men (Vijayakumar et al., 2020).
The impact of the sudden death of a relative, as a result of suicide, can be profound for survivors, with many experiencing post-traumatic stress disorder (PTSD), depression, anxiety, or even suicidal ideation and suicide (Contessa et al., 2023). Periods of intense sadness, loneliness, disbelief, self-blame, and rage can occur at various stages of the grieving process, which can be aggravated by cultural influences such as stigma and blame (Goulah-Pabst, 2023). At the same time, some survivors are able to return to pre-loss functioning, or even to grow from the experience in ways that enhance their future well-being (Genest et al., 2021). Some survivors recover within three months, while others take longer or experience chronic grief symptoms for over a year (Mancini & Bonanno, 2009).
In the aftermath of postsuicide trauma, various individual, social, and cultural factors can play a role in the healing and coping for suicide survivors. The role of personal resources and cultural support in achieving resilience after a suicide attempt or death varies across populations due to cultural differences, perspectives on life, spirituality, gender, and purpose. (Falk et al., 2023). In India, the relevance of personal, familial, and societal anomic conditions that trigger suicides is increasingly being researched (Patel, 2023). However, less is known about how suicide survivors experience the aftermath of a loss or attempt (Lasrado & Young, 2017). Understanding of such experiences is important for the development of resources to provide effective help for survivors. It is also imperative to comprehend how individuals’ capacity to manage and recover is influenced by their interpretations of the surrounding world. This includes the social narratives concerning death, suicide, gender roles, and other related topics.
Research Objective
The current study seeks to enhance understanding of the grieving and healing processes that take place among members of urban low- to middle-class Indian communities. It focuses especially on how bereavement and resilience are mediated by individual, social, and cultural factors. Thereby, insights are sought into the ways counselors, police, nurses, mental health, and various other professionals can provide better support to suicide survivors. Our study therefore aims to identify the ways coping takes place and helps suicide survivors deal with and recover from the experience of suicide. We thus ask the following two questions: What kind of challenges and opportunities do suicide survivors encounter in the Indian setting? How do Indian culture and society provide resources to support coping and healing process of survivors after the experience of suicide?
Theoretical Lens
Social relationships, cultural norms and rituals, collectively held knowledge, and processes of meaning-making influence the ways people learn, acquire emotional self-knowledge, develop coping strategies, and process psychological trauma (Markus & Hamedani, 2007).
It is well established that grief and resilience are expressed in a wide range of experiences and are shaped by social, cultural, historical, and political factors (Bonanno et al., 2001; Silverman et al. 2020). Events such as death, mourning, celebration, and various associated emotions are both individual and collective and are often shaped by cultural interpretations that may label them as “good,” “bad,” “interesting,” or “taboo.” Such interpretations may not be stable and static, but evolve as individuals and groups renegotiate the meanings of things around them- sometimes differing significantly both in place and time. In some cultures, death itself (not suicide per se) can be embedded, and accepted, whereas in others it may be shunned or perceived as taboo (Chapple et al., 2015). Similarly, within certain social structures, various communal artifacts, including social norms, rituals, responsibilities and roles, and forms of family-making and relationships, can influence the ways individuals find their own places and spaces to understand their experiences (Silverman et al. 2020). These artifacts can function as added challenges to individuals experiencing a particularly traumatizing event, if their experiences are stigmatized (e.g., Goulah-Pabst, 2023); or can be experienced as supportive, enhancing, inspiring, and healing in cultural settings, that can support reframing of the meanings of experiences.
The presence of family or friends can function as an important lifebuoy to people who have experienced the loss of an important person by suicide (Genest et al., 2021). Additional social factors that promote resilience may include spirituality-related rituals, family member accord, flexibility, family communication, joint financial management, family time, shared recreation, routines and rituals, and broader support networks (Black & Lobo, 2008). The systems approach to family resilience shows how individuals, as members of a family unit, build on key strengths and resources in the family, including joint meaning-making, sharing of burdens, clear problem-solving, emotional sharing, and flexible connected social and emotional processes (Theiss, 2018).
Various theories—such as resilience theory (Cicchetti & Garmezy, 1993), positive psychology (Seligman & Csikszentmihalyi, 2014), hope theory (Snyder, 2002), and logotherapy (Frankl, 1985)—examine how individuals cope with adverse situations based on the personal resources.
This study is part of a larger project that employs an action-based support technique, referred to by the acronym SALT (Support, Appreciate, Learn, and Transfer) (Schleiff & Bishai, 2020). SALT comprises both an interventionist strategy and an interpretive framework about how people function, based on a conviction that people can address and respond to challenges in ways that make sense to them. SALT assumes that people have the capacity and resources to take ownership of the challenges they encounter in their lives. It can be used to provide support for individuals, who experience traumatic or adverse events, and to strengthen their responses through relationships with people, who listen to their stories and appreciate their strengths. While the SALT approach arises from positive psychology and can be used to supply novel strengths and resources, in this study we focus predominantly on resources that are already available for survivors in the cultural settings in which they are embedded.
Methodology
Research Context
Home Visit-Based Pre-COVID-19 Intervention
The team associated with “Connecting Trust,” a suicide-prevention organization based in Pune, India, offered mindfulness-based active listening (MBAL) and SALT-based (Zachariah et al., 2018) support to suicide survivors via home visits and hospital visits. The listening was offered by volunteers who received 80-hour training in MBAL skills, holding a safe space and offering nonjudgmental, nonadvisory, respectful, and empathetic listening (Zachariah et al., 2023).
First Cohort of Intervention
Community leaders in a low-income neighborhood invited the Connecting Trust team to offer survivor support to address the high number of suicide attempts and suicide deaths. Nearly 270 households in the community were systematically visited by trained volunteers, to offer SALT and MBAL-based conversations regarding high-distress behaviors and suicide incidents in the community. The visits included homes of 18 suicide attempt survivors, their families, and families of those who lost a loved one to suicide. These survivors formed the first cohort of survivors for our study.
Helpline-Based Intervention During COVID-19
Second Cohort of Intervention
In-person visits were impossible during the COVID-19 pandemic. The survivor support helpline commenced operations in September 2020 and operated for two hours on three days each week. The procedure involved two volunteers contacting survivors via conference calls, introducing themselves as helpline volunteers, explaining the listening space, assuring confidentiality, and seeking consent to continue the call. Those who consented were offered a supportive space to express their distress. A suicide risk assessment was made for all calls and follow-up calls were offered. A text message was subsequently sent to survivors, inviting them to call the helpline if in need. Follow-up calls were made to everyone who requested them. Those who refused the service were not further contacted. If the phone call was not answered or switched off three times, they were removed from the contact list. A total of 157 survivors received helpline-based survivor support and formed the second cohort of survivors for our study.
Recruitment and Consent
Survivors who received listening support were approached for consent to participate in the impact assessment study. If they expressed interest, full details of the project were read aloud and the survivor was asked to give verbal consent, in accordance with ethics committee approval. Consent included an agreement to record responses to a qualitative interview. Pre-COVID-19 interviews were conducted in the setting of home visits and those during COVID-19 were undertaken via telephone interviews. Twelve of the 18 survivors consented to participate in the research interview, among the pre-COVID cohort, and 20 out of 157 agreed to participate in the interviews in the COVID-19 cohort.
Qualitative Instrument
A standardized open-ended in-depth interview protocol was employed to focus questions on a selected number of impact variables, and to provide an opportunity for an in-depth exploration of survivor responses (Turner et al., 2010).
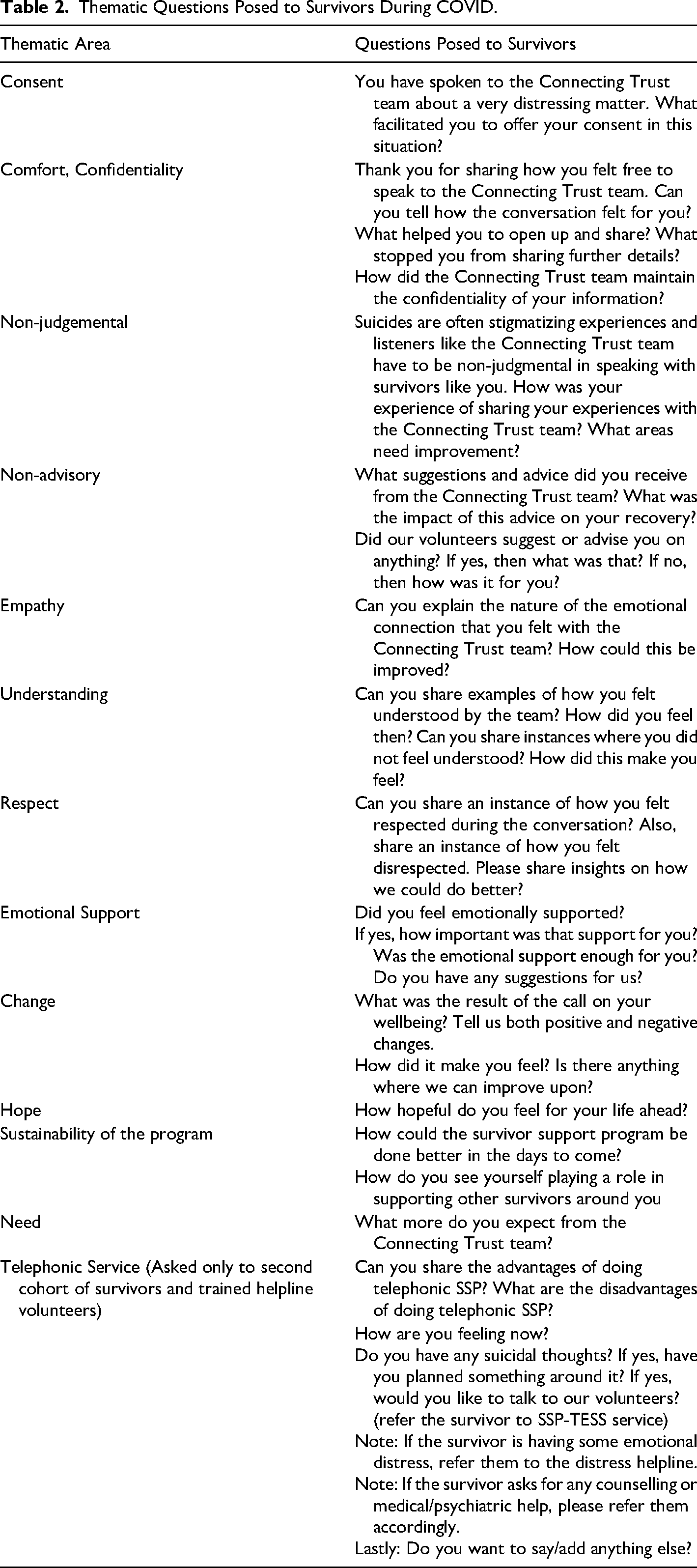
The Helpline cohort instrument incorporated the established themes of MBAL and measures of the program's impact (Gupta & Reina, 2022; Newman et al., 1987). It included the following themes: “consent,” “comfort and confidentiality,” “nonjudgmental approach,” “nonadvisory,” “empathy,” “understanding,” “respect,” “emotional support,” “change,” “hope,” “fulfillment of needs,” and “telephonic service.” Questions regarding the telephone service were posed only to the second cohort of survivors. The tool was translated into Marathi and field-tested to check accuracy and clarity, prior to being deployed. The interview tool is summarized in Table 2.
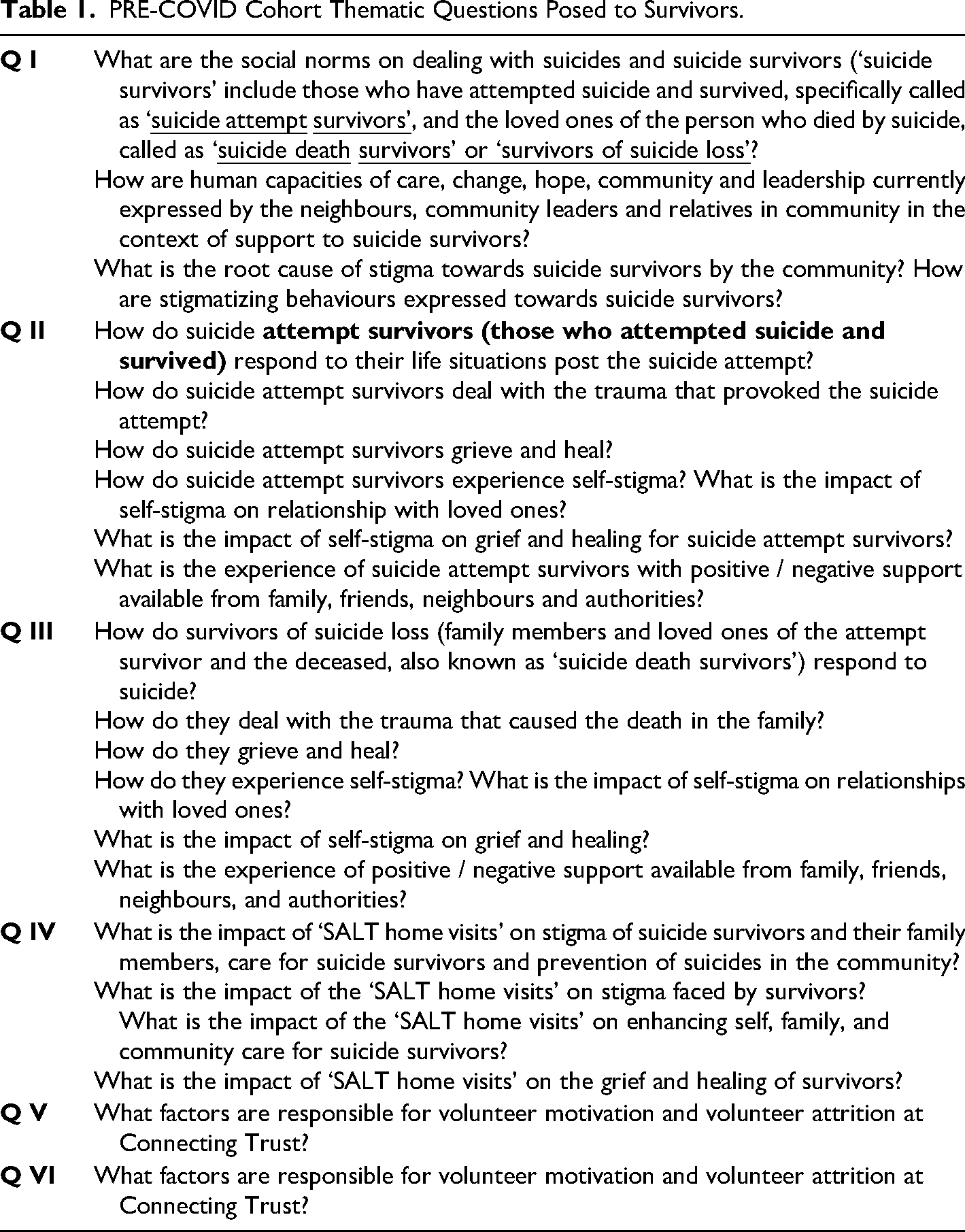
The home-based cohort instrument was based on similar principles along with SALT-based questions. See Table 1.
PRE-COVID Cohort Thematic Questions Posed to Survivors.
Data Collection
Data were collected by a team of trained volunteers for the home-visit cohort. Research interns who had received instruction in MBAL, in-depth interview skills, suicide risk factors, suicide prevention, and suicide risk assessment conducted data collection for the helpline cohort. The interviews involved the following steps:
The conversation was initiated with a team of two researchers, who introduced themselves. Consent to participate in the research was re-confirmed and either for recording of interviews or for verbatim notes to be compiled. The researchers undertook a formal risk assessment of the participant to exclude the presence of high risk or distress, in which case immediate referral to the survivor support helpline was recommended. The interview followed the protocol, with participants encouraged to provide detailed responses to open-ended questions. (See Tables 1 and 2.) The participant's well-being was checked after the interview and survivor support helpline numbers were given. Thematic Questions Posed to Survivors During COVID.
After completion, the interviews and the contemporaneous verbatim notes were transcribed in Marathi and then translated into English for analysis.
Data Analysis
Data from the survivor and the listener interviews were analyzed using the phenomenological approach described by Dowling and Cooney (2012). Briefly, the anonymized transcripts were read by two researchers, who compiled a list of potential themes in the form of a coding inventory. The coding framework was independently developed for each transcript and discussed in detail at meetings of the full research team in order to reach a consensus about recurring key themes and thematic content (Norlyk & Harder, 2010). Other members of the research team verified the outcomes again by independent reviews of transcripts. We used inductive and deductive thematic analysis methods to gain more understanding and insights from the data.
Ethics Approval
The KEM Hospital Research Centre Ethics Committee approved the study, including the recruitment and consent procedures, in June 2019.
Findings
Characteristics of Participants
Pre-COVID-19 Cohort Data Collection
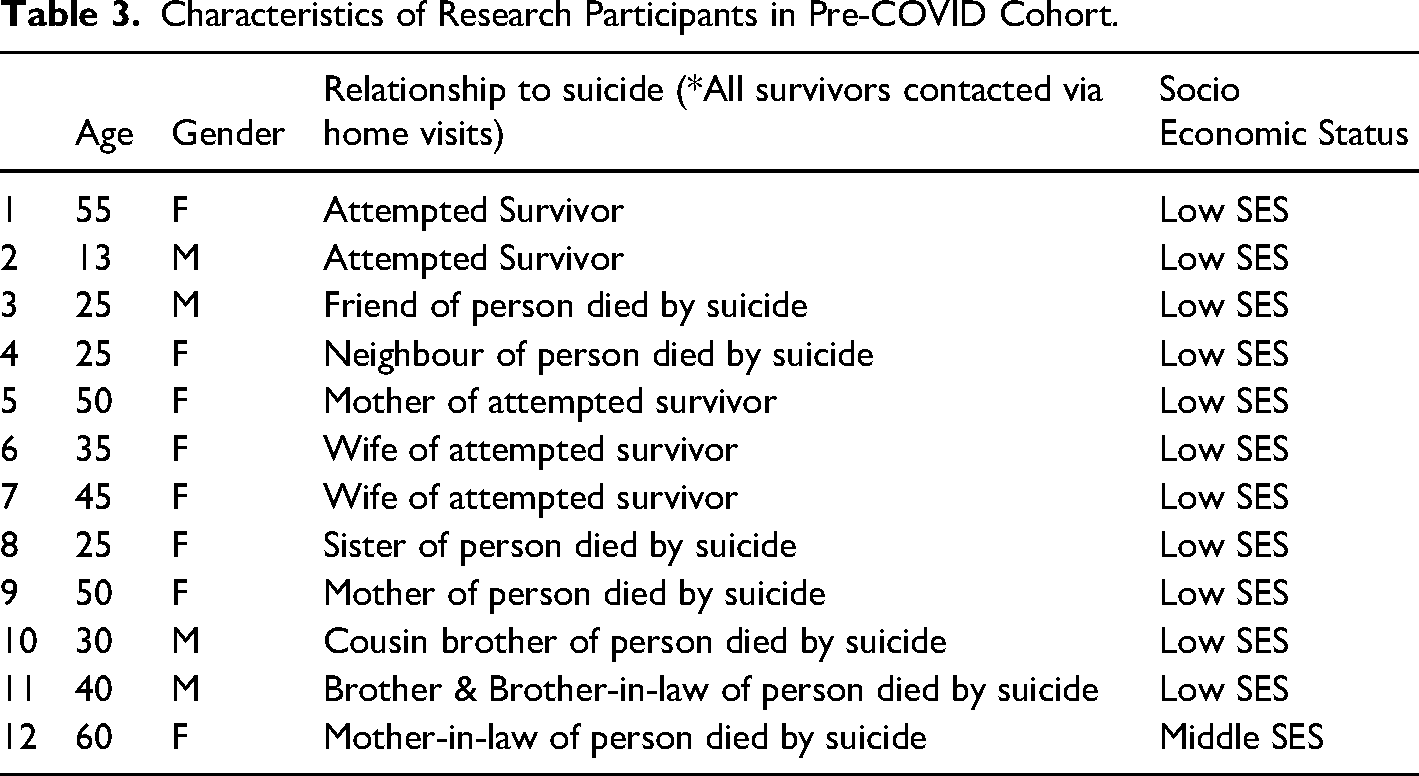
The characteristics of the 12 study participants are given in Table 3.
Characteristics of Research Participants in Pre-COVID Cohort.
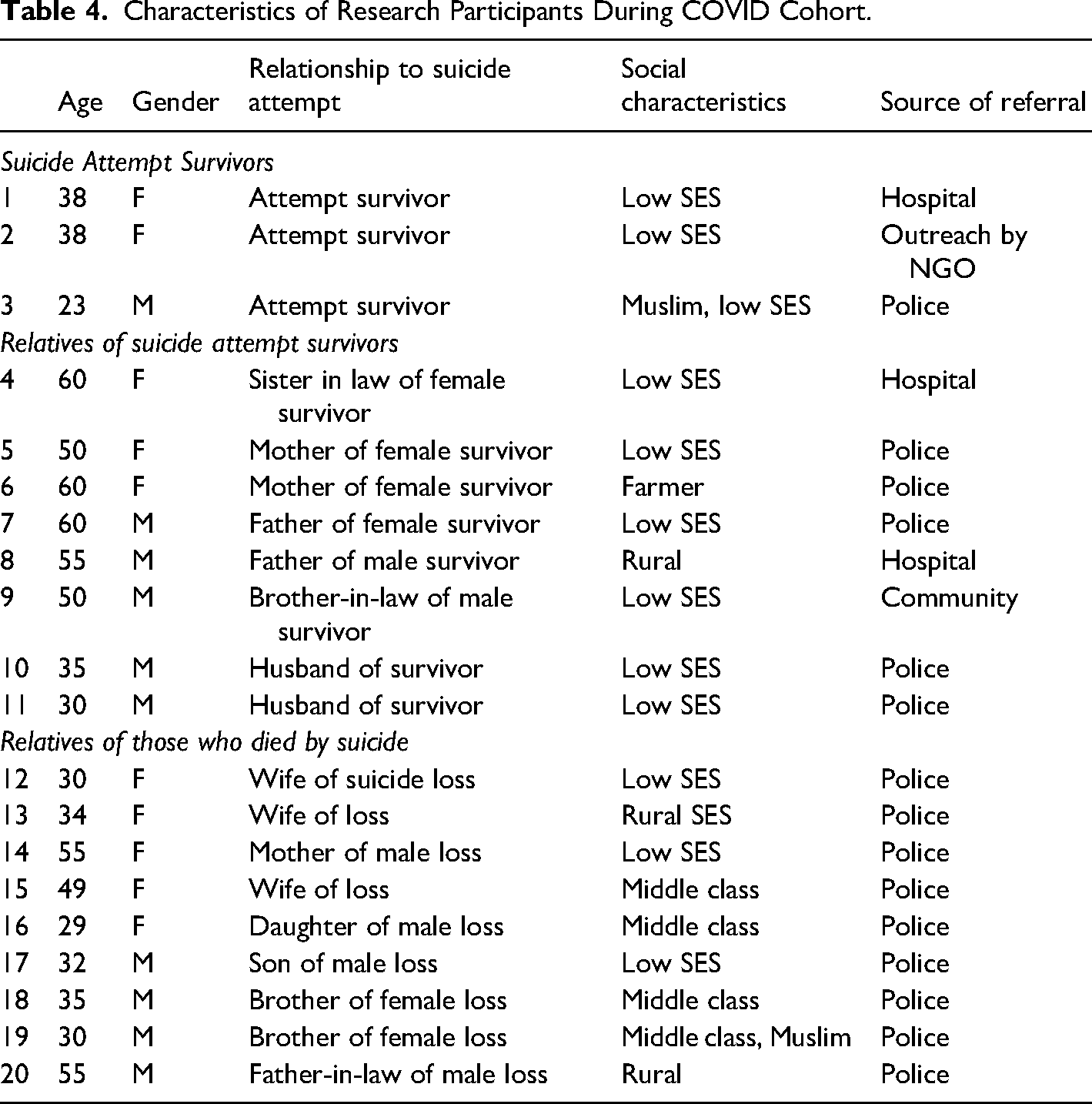
Characteristics of Research Participants During COVID Cohort.
All participants in the pre-COVID-19 cohort were identified during systematic home visits when family members revealed the incident. There were two attempt survivors, three relatives of attempt survivors, and seven people who lost a loved one to suicide. All were of low socioeconomic status.
In the COVID-19 period cohort, there were 10 women and 10 men with an average age of 42 years. Three participants were survivors of a suicide attempt, eight were family members of people who had attempted suicide, and nine were family members of individuals who had died by suicide.
Twelve were of low socioeconomic status, three were from middle-class urban areas and four came from rural areas. Fifteen were referred by the police, two by hospital staff, and two from the community.
In the next section, we highlight the most important themes found in a data set collected over five years which includes suicide survivor stories and their experiences. Analyzing these stories, we describe what they experienced as most challenging, what gave them the motivation and inspiration to keep going, how they found ways to function and take responsibility for themselves and their families, and how they experienced the support of others in this journey. We also reflect on the cultural aspects of urban India for people dealing with a suicide loss in their lives, and how these affected their healing journeys. We describe these experiences using four relevant categories/themes: (1) “responsibility and gender roles;” (2) “shades of support;” (3) “stigma and blame;” and (4) “spiritual inputs for life's purpose.”
Responsibility and Gender Roles
In the aftermath of a suicide experience, most survivors were not just confronted with the emotions related to experiencing a suicidal attempt or death (e.g., intense sadness and depression, feelings of grief and missing the loved one, fear, and anger) but also with the practical implications of losing a family member, spouse, or child (often already an adult). In the ways many low- to middle-class families in India are structured, there is a great deal of dependence in terms of roles and responsibilities among immediate and extended families, which can lead to imbalances when an important figure falls away. Naturally, the consequences of sudden gaps relating to financial stability, household chores, raising children, caring for parents and parents-in-law, and so on vary significantly between men and women because of their different roles in Indian society. Their responses to dealing with a suicide loss also differ. For both male and female survivors, the idea of having (increased) responsibilities played an important role in stories of grief. Men felt responsible for making sure the family was safe and guilty about not having been able to prevent suicide and more often took to drinking or silence to deal with the pain. Women seemed to feel more weighed down by the burden of having to take care of everyone around them. As one female suicide survivor said, for instance, during her life she regretted her husband's lack of responsibility, which was, in a way, emphasized after his death: My husband was an alcoholic and I had to take responsibility for my family when he was alive. Now he is gone… and the responsibility of family is still upon me. But I am hopeful. For 2-3 years I will have to work hard. My kids will grow up. Looking at them growing and how they will become independent is the purpose of my life. (218–31A)
Women survivors face the difficult challenge of being expected to be able to do it all. A widow in that context is left with a burden that seems, in some ways, invisible to her surroundings, but is experienced as a daily reality for her: In the current situation, emotional support is not at all helpful for women, because there are a lot of questions regarding the survival of that family. If the breadwinner is no more, what about the family, his children, and their career? Nobody cares about that. People just focus on the fact that he is no more. But nobody cares about the woman who is left behind. So I have to think about this, my children. My children's future is in the dark, and in such a situation, I have to face a lot of trouble from people in the society. After the husband's death, the woman alone has to face everything. Nobody is there to support her. Consoling words by family members or in-laws are just hollow words. Women have to face the situation alone. (218-9A)
For both male and female survivors, a sense of responsibility, and duty can also provide the strength to move on. We see this in women who take responsibility for their families, but also in some male survivors who take pride and direction from their role to take care of others. For instance, one male survivor shared: I always tried to be dutiful. When my daughter was admitted in the hospital [after her suicide attempt], I was there till her discharge from the hospital. Some people might get disturbed in such circumstances. But I calmly accompanied her. We are six brothers, and we are very strong at heart. There are many obstacles in our life, but we try to face them bravely. We are always ready to fight with adversities if the outcome is good then ok and if it is not expected then also it's ok. All of us are very practical minded. (218-30C)
Shades of Support
Indian society is commonly characterized as a close-knit and collectivist culture. In our study, we see, however, that suicide survivors experience social support in various different ways. For some, their experience in the aftermath of a suicide death has been one of relative isolation; these people felt left to their own devices and misunderstood by others. Two survivors expressed, for instance: I wanted people to be not sympathetic, I didn’t want all of that. I just wanted somebody to ask me ‘how are you?’. I told my family members, just call me up, and ask, just enough, to feel that there is a connection, there is support from far. But I think, in a way, maybe that's how the reactions I had from my family were just not sufficient. I think the family structure, as they were all intellectual, analytical, less feeling and empathy, and that sort of thing. so, I just felt very alone and bereft. (LS-2) No one, at that time, has helped me at all. I feel many emotions, but there is no use of those feelings, I have to come out of it. With all [family] members, the relations are not good, it is cross with everyone. I am going again and again into discouragement. My family always taunts me about the help they have provided. (AS-1)
Interestingly, in the cases above there was some support but it was not sufficient for what the person in distress needed at the time. They felt the outreach to be disconnected from what they were longing for, which included listening and open questions regarding their state or what they might need.
This led some survivors to put up their own walls and take ownership of their own trajectory, rather than expecting others to come help in sharing their pain: I realize that no matter whether you have supportive people around you or not, at the end you have to do the work yourself. It is up to you. Even if I had had the most loving supporting environment, at the end, it is my, on us to get up and say, ‘no’. I want to be happy; I want to live a normal life. It is entirely my call. I have to accept that responsibility as mine, nobody can do it for me. And the sooner I accept it, in my case it was sooner, because there was no option. I didn’t have any shoulder to cry on. So, I had to figure out how to keep myself afloat. That's it. As I said, it is very individual. What else can you do? I don’t know. (LS-2)
At the same time, stories also revealed pockets of assistance and support, sometimes people or institutions who were somewhat further removed from the direct family circle, including police, employers etc. People shared how they received financial support from the former employer of the person who died by suicide, or how the police offered assistance beyond their specific responsibilities. Similarly, stories were shared about teachers or neighbours stepping in during the moments of crisis, which was received as helpful and healing.
Blame and Stigma
Suicide survivors in our study face increased challenges, due to the stigma surrounding suicide attempts in India. Because of the history and spiritual context in which suicides are framed (e.g., suicides were until recently considered legal offenses), survivors experience the mental weight of having to defend themselves, or their loved ones against prejudices, feel the burden of having to hide details about the experiences in order not to be vandalized etc. Suicides were criticized as cowardly acts, and survivors were disdained by family. The relatives felt let down by the attempt survivors’ disregard for the impact on loved ones, revealing a lack of empathy. The reasons for attempting suicide were absent in the narration of the incident and recovery process. Suicide attempt survivors thus lived in an environment where blame was attributed to their actions, while having to deal with the distressing factors that led them to attempt suicide.
A 30-year-old man shared his disappointment with his wife for her poor mental health and inability to understand him. He shared: Everyone was not responsible for this. This type of incident happened because of the mental health of the particular person who attempted it, they don’t want to understand another person, or they may be not ready to do it, they may have their own psycho questions. (218-12A)
Another man whose wife attempted and survived suicide said: The one who commits suicide is a person with a very weak heart. Suicide doesn’t solve our questions. (2111-23A)
Seeing suicide as a consequence of bad choices or immoral behavior complicates finding peace and healing. As one mother explained, after her daughter's suicidal death, her son had a hard time accepting and talking about his sister's death, because he refused to interpret it through a lens of mental health, and went into denial: I am not asking you to be sympathetic or I am asking you to condone what she did or be sympathetic, I am just asking you understand what she went through. Then it is your take on how you want to respond to it. But this idea of medical condition having triggered this whole end, is still very new to a lot of people, even now. Conditions of bipolarity can push you to have suicidal tendency, you are pushed, your thoughts and everything go towards that, against your will. People say, “she should’ve been strong, she should have will power, this is not the way to deal with life.” So to inject the feeling of empathy there is very difficult, when people have this approach. ‘I didn’t like what she did, she shouldn’t have taken this step’. Agreed, it is not a comfortable step. Maybe, one time, I will show, I found a letter, she had written it long time back, there was no date, but she had written, “if you ever find this letter, that means something has happened to me.” She had already ideated it long time back. She had considered this possibility, yet she was struggling. (LS2)
Shame led some suicide attempt survivors to deny it, and blame their injuries on accidents, despite hospital records stating otherwise. In case of families who lost a loved one to suicide, the immediate relatives were blamed for causing it. This blame disproportionately affected women compared to men.
Finding Purpose in Life and Strength in Spirituality
Many religions interpret suicide as a sin and an act deserving of hell. Survivors in our study revealed that they did not want to risk their eternal life, by attempting an easy escape from their distressing situations, by ending their lives. A 35-year-old man, whose wife attempted and survived, shared his beliefs and fear of not entering heaven as the protective factor stopping him from suicidal thoughts: Even my guru [teacher] considers suicide a sin. A single thought about it is also a sin. Yes, we tell them about Gurudnyan. Suicide is like ‘पिशाच योपि (Pishach yoni). That person won’t have a human rebirth, nor will they have a place in heaven. They will have to live such a life where they won’t be able to enter any human's body or anything. It is ‘पिशाच योपि (Pishach yoni). One has to enter in that. Since my Guru has told me this, I never have any thoughts about suicide. A single thought about it is also a sin. I have got a blessing from my Guru. They gave me the knowledge of how to worship and how to live one's life. (2111-23A)
God was understood as a compassionate being, who supports and provides them with understanding, resources, wisdom to deal with adversities, manage negative emotions, and provide strength for enduring suffering. A 60-year-old, woman, whose sister-in-law attempted and survived a suicide attempt, shared her belief: In the end, suicide is a sin. God has given us strong hands and legs, if our body is good then everything is good. If we don’t have the intellect to come up with this thought, then it is of no use. At least God has given me this wisdom and whatever happens here on, and it is more for my sister-in-law. (219-30B)
Survivors mentioned multiple spiritual resources that offered them support, including the ongoing support from spiritual gurus, meditation, and spiritual lifestyle (bhaktimarg). These resources have allowed them to process their adversities in ways that calm their mind. A 35-year-old husband of an attempted survivor shared: It is still okay if somebody offends me. I do ponder upon the reason behind it or why he would have hurt me. But you can control your anger if you engage in meditation and Bhakti Marg. I feel maybe others would not have sustained in my place… Because the Lord's blessing is not always with everyone so I would like to pray that everyone receives the blessings that I have received in my life. (2111-23A)
A 60-year-old woman survivor shared her spiritual resources and its impact on her: I try to gain spiritual knowledge, read a few books related to God. I have my mobile and there are a lot of good things or videos on it, on YouTube, to calm my mind. I play a lot of such videos to calm my mind down, I listen to some good quotes, and when we keep on listening to such things, it keeps on adding to our wisdom and then we take a back step from the bad thoughts, at least God has given me this wisdom. So, you have to collect yourself and calm your mind and keep silent. If I become too tense, I just take a book and start reading it and do nothing else. (219-30B)
People also found purpose and direction in their lives from caring for others. Suicide survivors expressed immense strength in dealing with the adversity of a suicide, and the data revealed purpose in life, as a major factor that lit their paths. Multiple survivors found strength in sharing responsibility and caring for their families amidst adversities. A 30-year-old widow who struggled with suicidal feelings after her husband's death shared: At any point of time, if I feel distracted or suicidal, I save the kids’ photo as a Screensaver. The minute I open my phone, I see my kids. That's it. Ends the matter. Yes. I have to think before I take any step as I have the responsibility of my children. (218-9A)
Parents described their responsibility to support their children's recovery after a suicide attempt. An unmarried 26-year-old woman shared how care for her widowed mother and brother gave her strength to face adversity: Actually, in the beginning, genuinely telling you as my father committed suicide, I also wanted to follow him or I thought, I should be in the place of my father … but my mother and brother already lost my father, then what will happen to them? How will they feel? By keeping all these things in mind, I have decided to go with the flow. (219-30A)
People without children or direct family, still found purpose in supporting others. This include listening to those in distress, and encouraging those who were feeling suicidal. A 60-year-old widow, whose sister-in-law attempted suicide, shared: So then by strengthening our own mind, by deciding to live a good life, we can give others our support. There are many more people who are more sad than us. So then if we support them, we can gain satisfaction through that. So now I am working a little at this … company. I have products from that company; if anyone needs them, I buy those medicines for them with my own money. If that person becomes happy, if their disease goes away, if their pain stops then the relief, they are going to get from that; I am going to be more blessed because of that. So, this is the perspective through which I have been living my life. (219-30B)
A woman in her fifties, a few years after her daughter's suicidal death, and after tolerating much blame from her husband and other relatives, now feels able to live a happy and normal life. The woman, who is working as a volunteer for a suicide prevention organization, obtained insights and a purpose for living from helping others, expressing with sadness that if she had access to this knowledge earlier, she might been have able to save her daughter: I realize that no matter whether you have supportive people around you or not, at the end you have to do the work yourself. It is up to you. Even if I had had the most loving supporting environment, at the end, it is my, on us to get up and say, “no.” I want to be happy; I want to live a normal life. It is entirely my call. I have to accept that responsibility as mine, nobody can do it for me. And the sooner I accept it, in my case it was sooner, because there was no option. I didn’t have any shoulder to cry on. So, I had to figure out how to keep myself afloat. That's it. As I said, it is very individual. What else can you do? I don’t know. I came from a place where I was solution oriented. I came from an approach where the approach I had to change in Connecting Trust (NGO) is – I know now which is a big shift which I had when I took that Connecting Trust training. That was a huge, huge, huge learning. If I knew then what I know now how to deal with it, I can’t say for sure, I know for a big part, I would have been able to help her. (LS-2)
Discussion
In this study, we sought to understand the course of grief and healing for suicide survivors in an Indian urban context, in Maharashtra State of India. We will discuss the findings in relation to the extant literature to explain what we have found.
Risk Factors for Suicide Survivors in Indian Society
First, in our data women and male survivors have somewhat different trajectories in their grieving processes. This is owing to their different positions in society, the cultural expectations placed on them, and how these factors shape the ways they give meaning to their own, as well as others’, lives. For male survivors, we observed that they felt responsibility to keep their family safe, and in some ways experienced even greater responsibility, and encountered more blame, for the suicide events in their direct environments. Male survivors expressed guilt about not having been able to prevent a suicide in their family. In many Indian societies, especially in Hindu Dharma (Evans et al., 2022), it is the responsibility of a son to take care of parents. It is also expected that they be helpful and compassionate to others, without attachment to results or expecting anything in return (Chadha, 2017). Whereas, in western, individualistic cultures, survivors may feel shame instead of guilt after a suicide (Crowder & Kemmelmeier, 2018).
In many cultures, norms applying to men (such as the expectation that they suppress emotions and are professionally successful) may diminish the capacity to respond to psychological pain, and lead to a heightened risk of alcohol abuse (Bennett et al., 2023). This is particularly true for cultures that are founded on patriarchal principles (Khurana, 2018). This means male survivors find deep level of satisfaction in providing support, despite their adversity and shame they had to endure.
For the women in our study, a sense of responsibility and having to “be there” for others in the family, was an important theme in grieving. However, they seemed to be confronted with a duality of standards and expectations, which left them at risk of alienation from the broader society. This duality arose from the fact that many women, when losing a spouse, are left as the only breadwinner in the household, yet the surrounding environment does not regard (or support) them as such. Many women survivors expressed their distress at becoming the chief breadwinners of the family, a role that was supposed to be managed by their deceased husband or adult sons. A survey about gender roles in Indian families and society (Evans et al., 2022) revealed that earning is considered primarily a responsibility of men, although this is changing, with women increasingly working and contributing to the family income. When an earning male suddenly dies, this exposes the woman to a financial crisis and leaves her vulnerable, because this reality is ignored by the broader society, forcing her to enter realms of social life that were previously not expected of her.
The women also felt the negative weight of other people's opinions, perhaps more so than male survivors. In Indian society, the wife's role is often perceived as secondary, designed to support her husband, setting moral standards by sacrificing her pleasure and ambition, releasing his tensions and stress, maintaining peace at home, and standing by him in all crises (Batar et al., 2021). The Sati Pratha of times past demonstrates how women are treated as having no value after their husbands’ death. It is therefore easy to blame a woman for her or her husband's suicide or suicidal attempt (Tousignant et al., 1998). When a husband dies by suicide it becomes relatively easy for society to doubt the wife's character and lack of ability to fulfill his desires as the reason for his suicide. This blame extends further to daughters, as they are also brought up by their mothers, as shared by the daughter of a person who died by suicide, in our study.
Blame and shame are not, however, reserved for female survivors in Indian society. They extend to all because of the history and cultural stigma around suicide, in part deriving from the influence of the Hindu religion on people's perceptions of self-orchestrated deaths (Dornelles et al., 2020). Until 2018, when the Mental Healthcare Act was passed, attempting suicide, whether it was fatal or not, was considered illegal and subject to punishment (Helal Mehtab et al., 2022), further increasing the sense of shame.
The media's failure to adhere to reporting guidelines on suicide in India exacerbates stigma and victim-blaming (Armstrong et al., 2020). Suicides are generally reported with superficial remarks about isolated facts on mental health, economic or family-related problems, and focusing on disconnected “sensational” personal details without taking into consideration the broader social contexts in which suicide victims became suicidal. This leads to skewed stereotypes such as “suicides can only occur in people who are mentally disturbed, and who are impulsive” (Banerjee et al., 2021). Thus, culturally, politically, and spiritually, suicide is regarded as a grave error and a sign of mental and emotional weakness in Indian society. This view was frequently encountered in this study.
Resilience and Protective Factors
In the course of our study, we found that people are endowed with a variety of strengths that they derive from their inner, family, community, and institutional resources. These strengths enable people to deal with adversity. A few survivors spoke about the healing role played by spiritual beliefs, practices, and resources. Centuries-old spiritual practices, like Satsang or following some saint or “guru,” are common in India, and contribute to well-being (Singh et al., 2020). During Satsang, the orator guides people based on their respective religious books, and the group works as a peer support group whose members share their pain while others listen, appreciate, and support each other. These sessions can help survivors deal with the pain and distress of suicide experiences. These sessions resonate with the approach of SALT, which allows concerns to be shared and human strengths to emerge (Zachariah et al., 2018). Spiritual beliefs can be perceived as a double-edged sword, with families wondering whether their relatives reside in heaven or in hell. Also, the guilt that prevents people from committing suicide may exacerbate the survivors’ distress unless they find a way specifically to address it. As a result, survivors may live with immense pain without attempting suicide to avoid going to hell.
Survivors also talked about a “sense of purpose” related to the future of their children, the needs of their extended families, and a commitment to supporting others in distress as helping them “move forward.” Thus, gaining an understanding of the purpose of life allowed them to suffer the pain and work for the future (Bradley et al., 2024; Frankl, 1985). The socio-cultural theory of Lev Vygotsky (Van der Veer, 2014), emphasizes the importance of the social and cultural processes, norms, and semiotic systems of whatever society we happen to be born into. Indians, especially Hindus, follow the spiritual aspects of being or becoming a “Satvic” person, which can be seen in the context of the experience of suicide and coping. Research has shown that as a consequence of their sorrow, many suicide survivors exhibit a heightened sense of compassion toward others struggling with mental health issues, often stimulating them to connect with and support others (Lynch, 2000).
These findings align with the theory of Logo-therapy proposed by Victor Frankl, according to which a sense of meaning in life is an essential shield against suffering (Bradley et al., 2024; Frankl, 1985). Suicide survivors’ love for their families, children, mothers, and siblings, and their compassion toward others, helped them to cope with grief and loss and gave them the courage to move on and to live meaningful lives (Praetorius & Rivedal, 2017). The new realization of love and courage to meet responsibilities added value to their existence, helping them to fulfill their Dharma, develop a sense of self-efficacy and empowerment (Hawgood et al., 2022; Matel-Anderson & Bekhet, 2016), leading to enhancing their well-being and sense of fulfillment as they are able to follow the norms of their society.
The experiences of survivors illuminate the positive healing factors available in society. These include individual resilience and support received from the family and spiritual practices. These positive experiences demonstrate the potential of individual traits, resources, and support available and align with the theory of (first wave of) “Positive Psychology” (Seligman & Csikszentmihalyi, 2014; Wissing et al., 2022). Similarly, the “human capacity for response” theory speaks of the human strengths of care, community, change, hope, and leadership that is present in individuals in their relational context (Lamboray, 2016). These capacities enable people to respond to their concerns, learn from them, and adapt (Campbell et al., 2019). We saw the caring spirit of survivors providing meaning in their lives to live for the rest of the family. This motivation thus became a protective factor for them from attempting suicide and became a “capacity for life,” promoting care for the family and self-care. It is in these inner strengths of human beings that the potential and the healing journey can begin, even when the external support mechanisms are severely truncated.
Limitations, Implications, and Final Remarks
A small component of our data included a section of interviews derived from our intervention study with survivors, during the COVID-19 pandemic. This created a situation where individuals were locked in their homes with little access to their families or to social and institutional networks. It was interesting to note that the data elicited in this period were not distinctly different from our larger data set. This might be explained by the fact that a suicide event weighs even more in people's lives than the factors in relation to social distancing. Thus interviewees when asked how they were managing in their grieving journeys, mostly commented on aspects that were generally true for suicide survivors, who were born and raised in the context of urban Maharashtra. It might have been, therefore, that our inductive way of eliciting the stories of survivors, both before and during COVID-19 elicited a similar set of themes and categories, regardless of this change in backdrop. If anything, we could see that survivors of COVID-19 dug even deeper into their inner resources, to endure the challenges and heal, and in some cases show early evidence of thriving. As this study was conducted in Maharashtra, and most of the survivors were from lower socioeconomic backgrounds and one particular religion, its findings cannot be generalized.
Footnotes
Acknowledgments
The authors thank all survivors for participating in this study, giving their time and sharing their experiences. We would like to thank to Mrs. Arnavaz Damania, Founder and Managing Trustee, Connecting Trust, Mrs. Sandy Andrade, Co-Managing Trustee, Connecting Trust, for their support. We are grateful to the volunteers of Survivor Support Helpline for providing support and safe listening space to the suicide survivors. We extend our gratitude to our program partners who helped us to reach the suicide survivors; Pune Police, Sassoon General Hospital and the research interns Ms. Sanjana Nair, Mrs. Rashmi Joshi, Ms. Peeyusha Diwan, Ms. Jigisha Zope. We express our gratitude to Ms. Deborah Eade for her language editing support.
Data Availability
The data for this research was collected under confidentiality agreement with suicide survivors. Anonymized data can be released based on direct correspondence with the first author of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was partially funded by Mukul Madhav Foundation, Pune, India.
Author Biographies
As a physician, Paul’s field of specialty is endocrinology. He is the Director of the International Ethics Center, the Centre for Ethics in Medicine and Society. He believes that one of the objectives of medical research is to contribute to the improvement of clinical practice and the development of new, more effective social policies.