
Abstract
Background
Worldwide over 21 million children and young people are living with life-limiting conditions (Coombes et al., 2022). These include conditions where treatment may be faesible but can fail (e.g., cancer); conditions where a shortened life is inevitable (e.g., cystic fibrosis); progressive conditions that do not have curative treatment options (e.g., mucopolysaccharidoses) and irreversible conditions that cause severe disability (e.g., multiple disabilities following brain injury) (Together for Short Lives, 2023). Historically, children diagnosed at birth/childhood with a life-limiting condition had little hope for survival into adulthood. However, increasing numbers of children and young people are now living longer than expected and transitioning to adult healthcare. Studies suggest young people (18–24 years) with life-limiting conditions (young people) experience an increased complexity of needs, including unmet psycho-spiritual needs, and a higher healthcare burden as they move into adult services (Booth et al., 2018; Jarvis et al., 2022).
In adult palliative care settings, Dignity Therapy (Chochinov et al., 2005), an evidence-based psychotherapeutic intervention, is offered to support psycho-spiritual wellbeing. This is achieved through a process of life-review, meaning-making and legacy leaving. Dignity Therapists undertake one-to-one semi structured interviews with individuals, usually lasting no more than an hour, drawing on the The Dignity Therapy Question Protocol (Figure 1). These questions encourage a reflective discussion about valued memories, accomplishments, life roles and lessons, and future hopes for significant others. The interview is digitally recorded, transcribed, edited into a storied narrative and returned to the individual, who can suggest changes before the document is finalised. This may involve several meetings. The document is considered a generativity document or written legacy (Chochinov et al., 2005). Many people share their documents with others prior to death, providing opportunities for meaningful conversations that can assist bereavement processes (McClement et al., 2007).
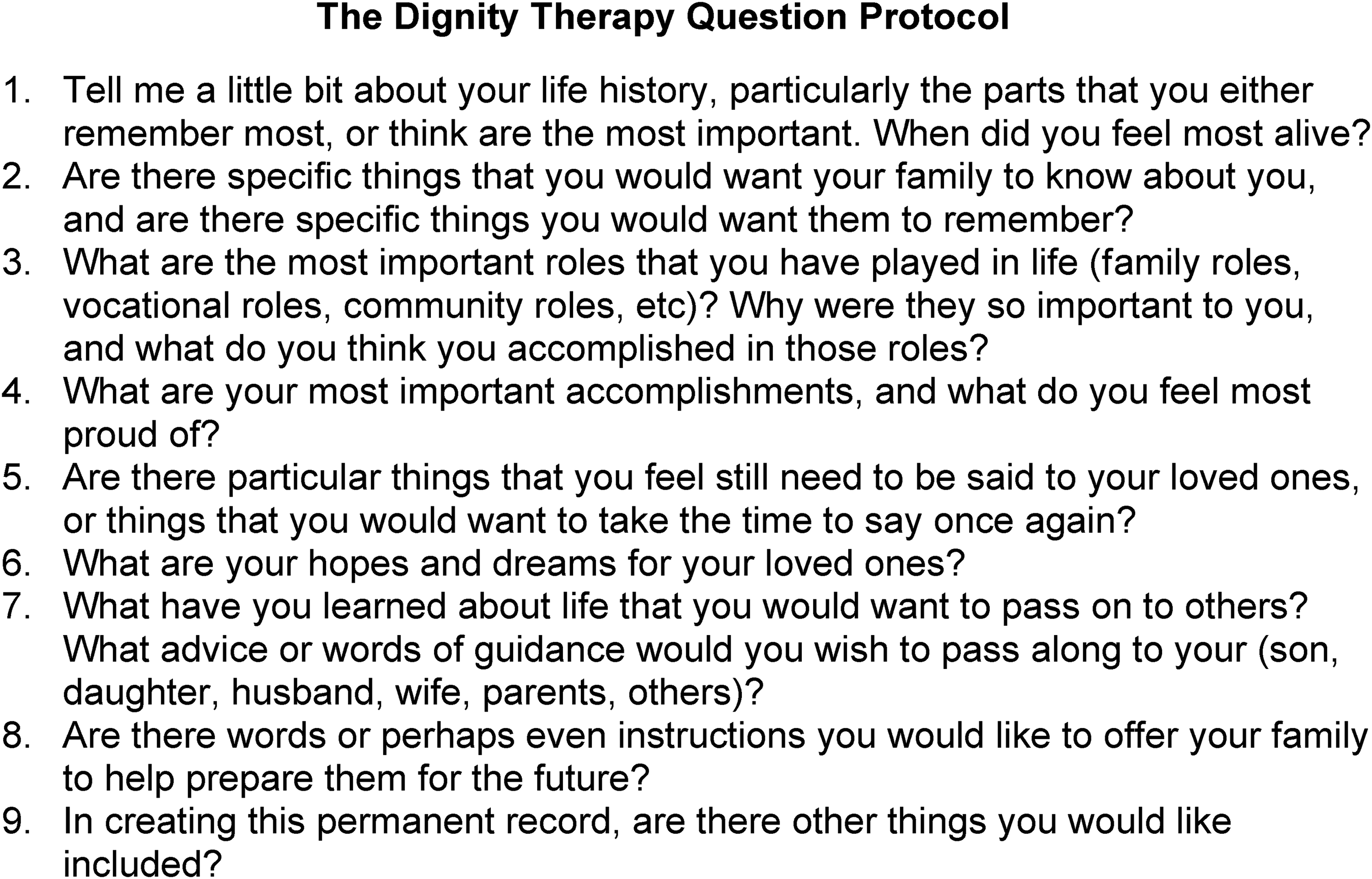
The dignity therapy question protocol (Chochinov et al., 2005).
A literature review exploring Dignity Therapy with young people (Rodriguez et al., 2018) found few studies had included young people. Most studies included people middle aged upwards with cancer conditions. More recently, studies have explored the utility of Dignity Therapy for children and young people. The Dignity Therapy question protocol has been adapted for adolescents with cancer in Portugal (Julião et al., 2020), and a digital story board technique for children with cancer (Akard et al., 2020) has been created in the USA. In addition, Dignity Therapy has been used effectively in hospital settings in the USA, involving children, young people, and families (Schuelke & Rubenstein, 2020). Consultation activities undertaken in the UK, however, suggest that although Dignity Therapy could be a supportive intervention for young people, the approach would benefit from adaptations to better reflect their needs (Watts et al., 2020a & 2020b). As life-limiting conditions advance there are especially high burdens placed on families to support care (Ammann-Schnell et al., 2021; Veronese et al., 2015). The option of family engagement in Dignity Therapy for young people would acknowledge their diversity.
In exploring how and in what ways a Dignity Therapy-based intervention could meet young people's needs, the theoretical bases of Dignity Therapy need to be considered. Dignity Therapy is based upon the Dignity Conserving Model of Care (Chochinov et al., 2002). This model constitutes what dignity means to adults, drawn from the end-of-life experiences of middle aged and older adults with advanced cancer conditions. Dignity Therapy relates especially to several tenets of this model including generativity, the continuity of self, the maintenance of pride, hopefulness, role preservation, aftermath concerns, care tenor and social support.
Cai et al. (2023) explored the dignity model of conserving care for terminally ill children, from the perspectives of parents (n = 11) of children with cancer conditions and healthcare professionals (n = 14). Although the tenets of the adult dignity model (Chochinov et al., 2002) were deemed relevant for children, additional tenets were recognised. It was suggested that Dignity Therapy for children should further consider how stigma can cause psychological distress, and how acknowledging regrets and supporting the child's sense of security can assist coping. In addition, dignity in children can be supported by them having the company of loved ones, showing them ‘fairness’, exploring any unfinished wishes, resolving any family disputes, and having a decent and dignified death. It is plausible that the tenets of dignity found in both adult (Chochinov et al., 2002) and child (Cai et al., 2023) models of dignity may be relevant to young people.
The current study aims to co-design a life review, meaning-making and legacy leaving intervention for young people. DIGNISPACE will be a Dignity Therapy-based digital intervention; a way of delivering supported psycho-spiritual care acceptable to young people with a range of life-limiting conditions and their families. Through the co-design process dignity in young people will be explored. The sections that follow outline the study's methodology, a thematic discussion of findings, detail of a proposed model of dignity in young people and detail of the content of the Dignity Therapy-based digital app for young people ‘DIGNISPACE’, with a discussion and concluding section that draws together key points.
Methods
Design
A descriptive qualitative design, drawing on naturalistic inquiry (Erlandson et al., 1993) facilitated the co-design of DIGNISPACE.
The study includes two phases:
A qualitative exploration of dignity and Dignity Therapy for young people. A small-scale qualitative user evaluation of the DIGNISPACE digital app prototype and the related question protocol.
An advisory group of eight young people and eight family carers supported the study. Reporting follows the COREQ Checklist (Tong et al., 2007).
Participants and Setting
The study was undertaken in the North of England, in a mixed urban-rural region. Participants were recruited from child and adult hospice settings due to the palliative and psycho-spiritual focus of the proposed intervention.
Participant inclusion criteria was as follows:
Young people: 18–24 years; living with a life-limiting condition, can provide informed consent; access to internet/smartphone technology; no evidence of confusion/delirium based on clinical consensus. Family carers: family member of a young person with a life-limiting condition; directly involved in care; access to internet/smart phone technology. Healthcare professionals: Employed by a hospice; directly involved in care; access to internet/smartphone technology.
Sampling
Sampling was purposive as appropriate to the aims and qualitative design of the study.
Recruitment
Recruitment was facilitated by six hospices with young people caseloads. Hospice healthcare professionals were research gatekeepers, and shared study information documents with eligible participants. Recruitment was undertaken between April 2021 and December 2022.
Data Collection
In phase 1, participants were involved in semi-structured virtual interviews (young people) or virtual focus group discussions (healthcare professionals) via the ZOOM video conferencing digital platform. Participants were invited to share their views on dignity in young people and the acceptability of Dignity Therapy for young people. The Dignity Therapy question protocol (Chochinov et al., 2005) with some suggested amendments for young people (Watts et al., 2020a & 2020b) along with a basic mock-up of DIGNISPACE were shown to participants. Participants shared recommendations for question amendments and digital development.
In phase two, participants were invited to participate in semi-structured virtual interviews (young people and family carers) or face-to-face focus group discussions (healthcare professionals) at a regional hospice setting. Participants were invited to evaluate the co-designed DIGNISPACE question protocol and DIGNISPACE digital app prototype and suggest any necessary amendments.
Data Analysis
All data were digitally recorded, transcribed, and anonymised. Framework analysis (Smith & Firth, 2011) was undertaken on all data and included:
Developing an initial coding frame from study aims, refined following review of the first focus group and two young person interview transcripts. The coding frame was applied to the whole data set, with categories reviewed following team and advisory group discussions. Categories were condensed to form overarching themes and sub-themes.
Following analysis, the model of dignity in young people was developed and the DIGNISPACE question protocol and digital app prototype were finalised.
Ethical Considerations
The study received ethical review and approval from the School of Healthcare Research Ethics Committee, University of Leeds, UK. The study was approved 28/01/2021 (reference: HREC 20–005). Before any participant was recruited, governance approvals from participating organisations (hospice settings) were achieved. All team members are experienced in research with young people. AR (psychologist, Dignity Therapy trained) undertook interviews and chaired focus group discussions, supported by MT and JS. Processes were in place to support participant withdrawal and distress/safeguarding need.
Results
Participant Details
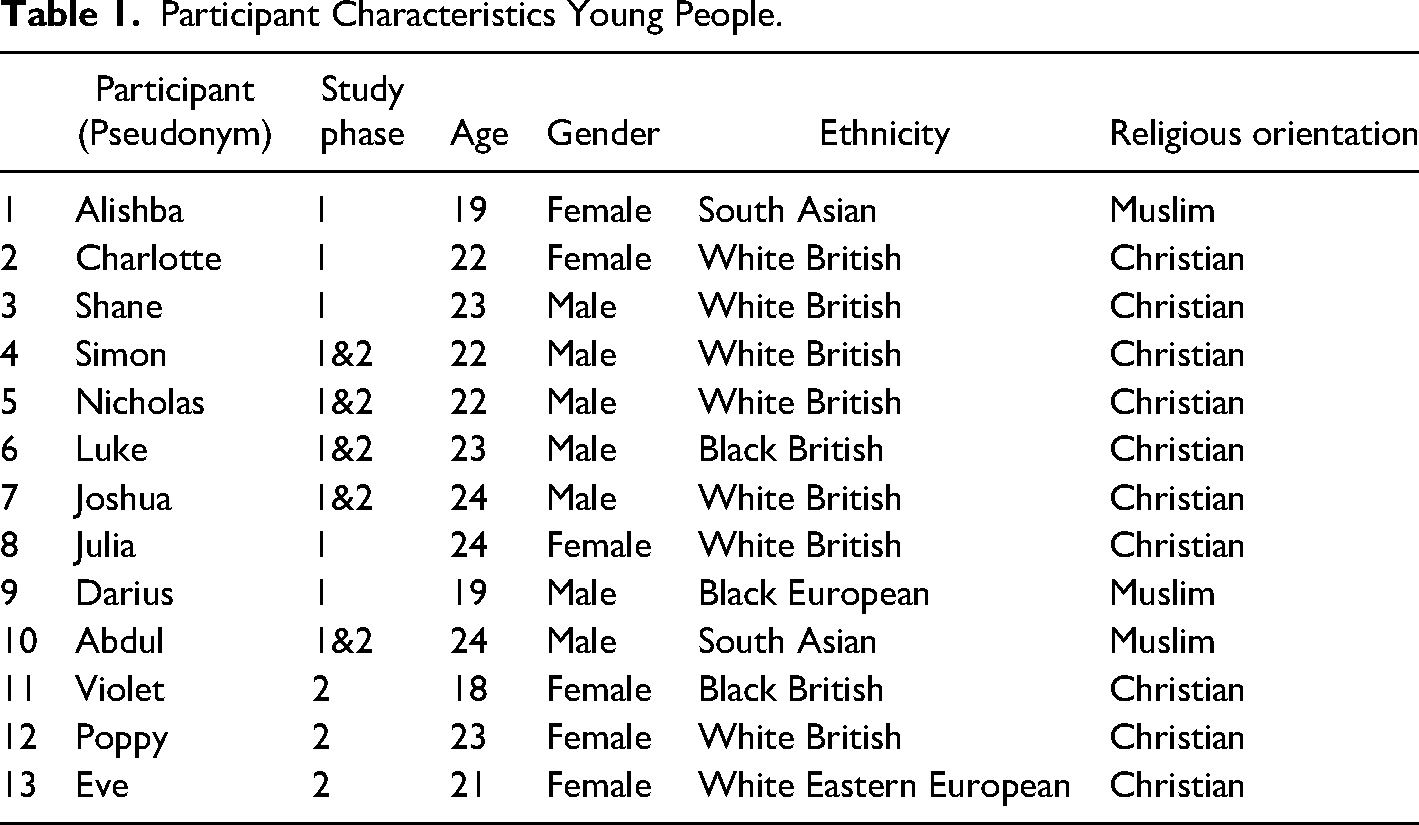
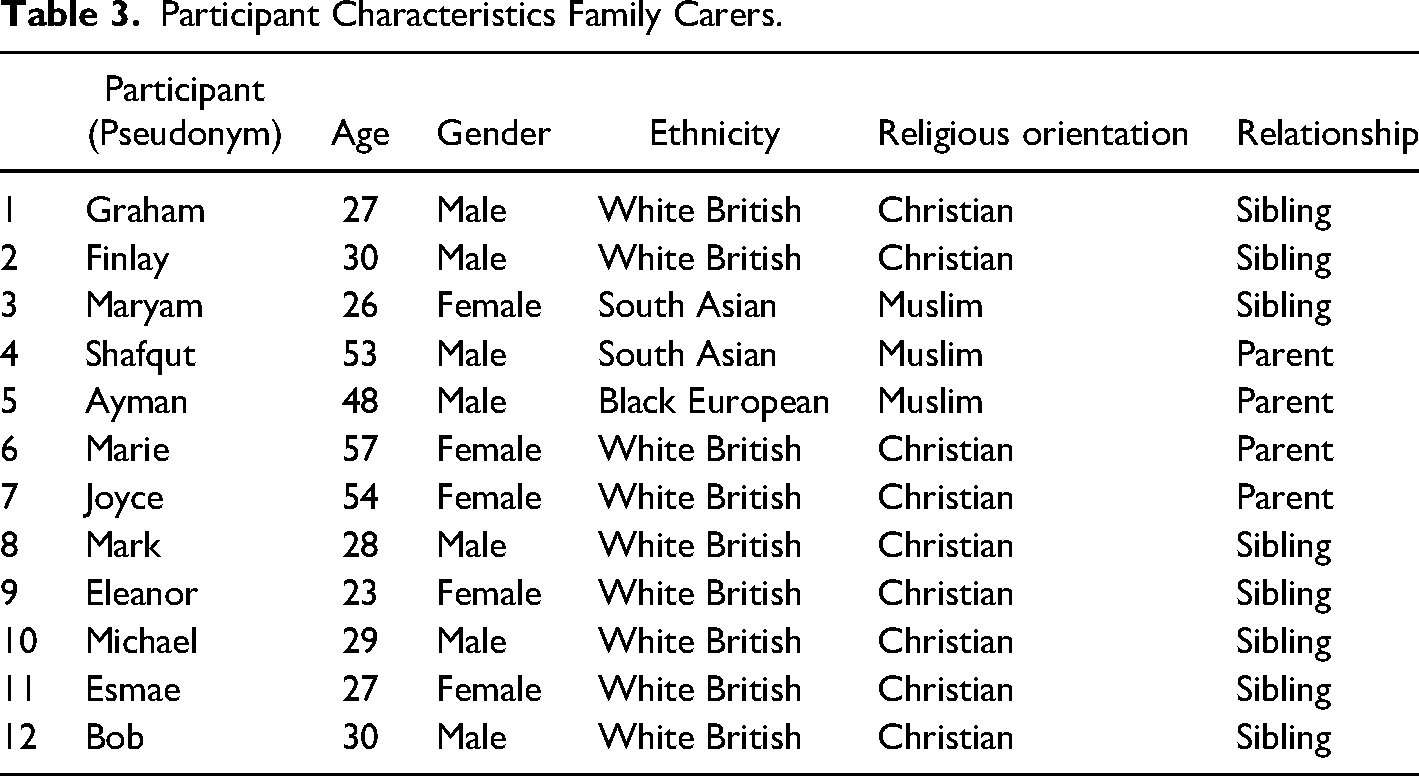
The study included 48 participants: 18 semi-structured interviews with young people (mean age 21 yrs.), 12 semi-structured interviews with family carers (8 siblings, 4 parents) and five focus groups with 23 healthcare professionals (13 nurses, 8 therapists, 2 physicians). Data collection was from April 2021 to January 2023 with interviews 40–90 min and focus groups 50–70 min in duration. Tables 1–3 detail participant characteristics.
Participant Characteristics Young People.
Participant Characteristics Healthcare Professionals.
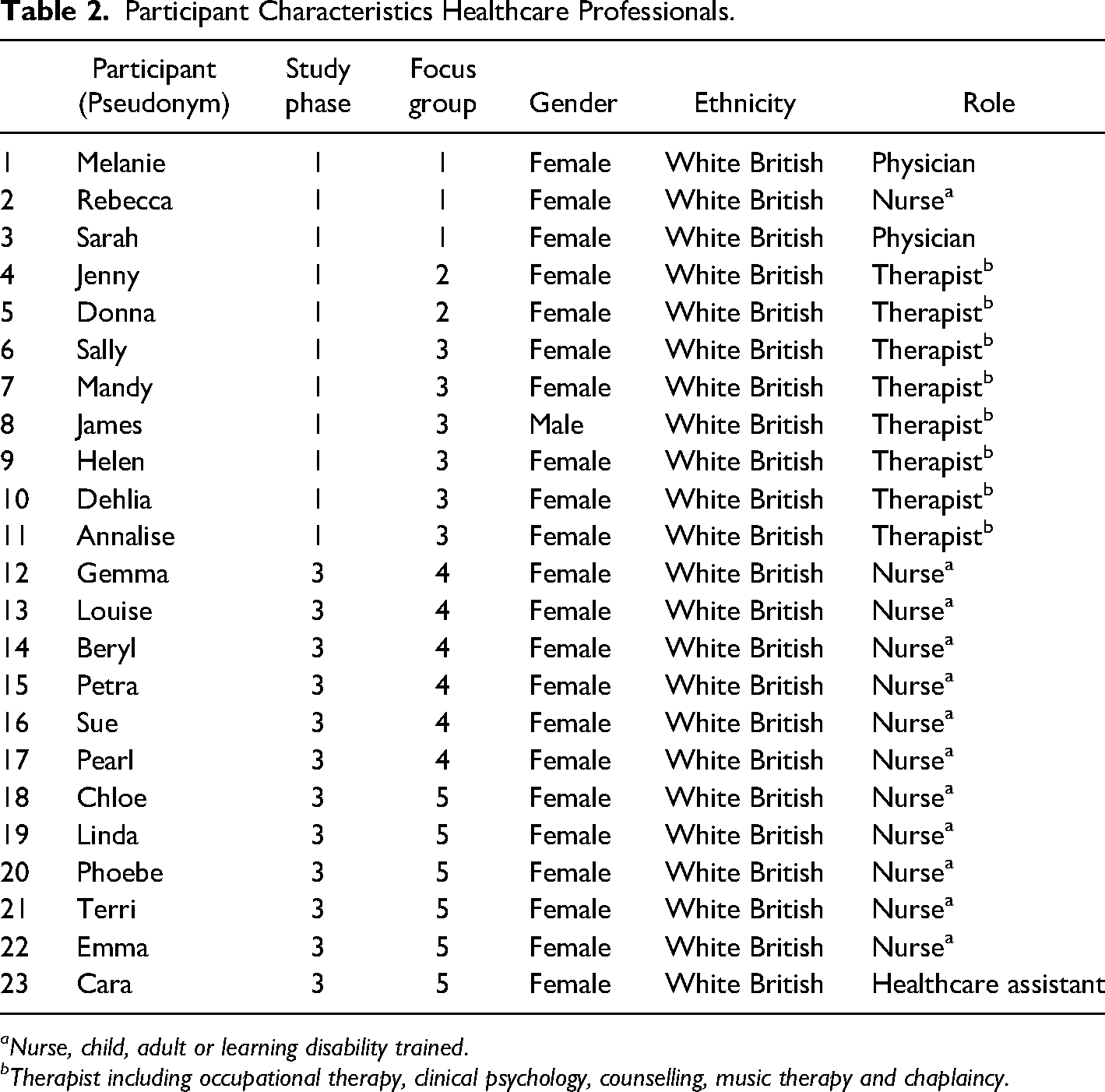
aNurse, child, adult or learning disability trained.
bTherapist including occupational therapy, clinical psychology, counselling, music therapy and chaplaincy.
Participant Characteristics Family Carers.
Framework Analysis
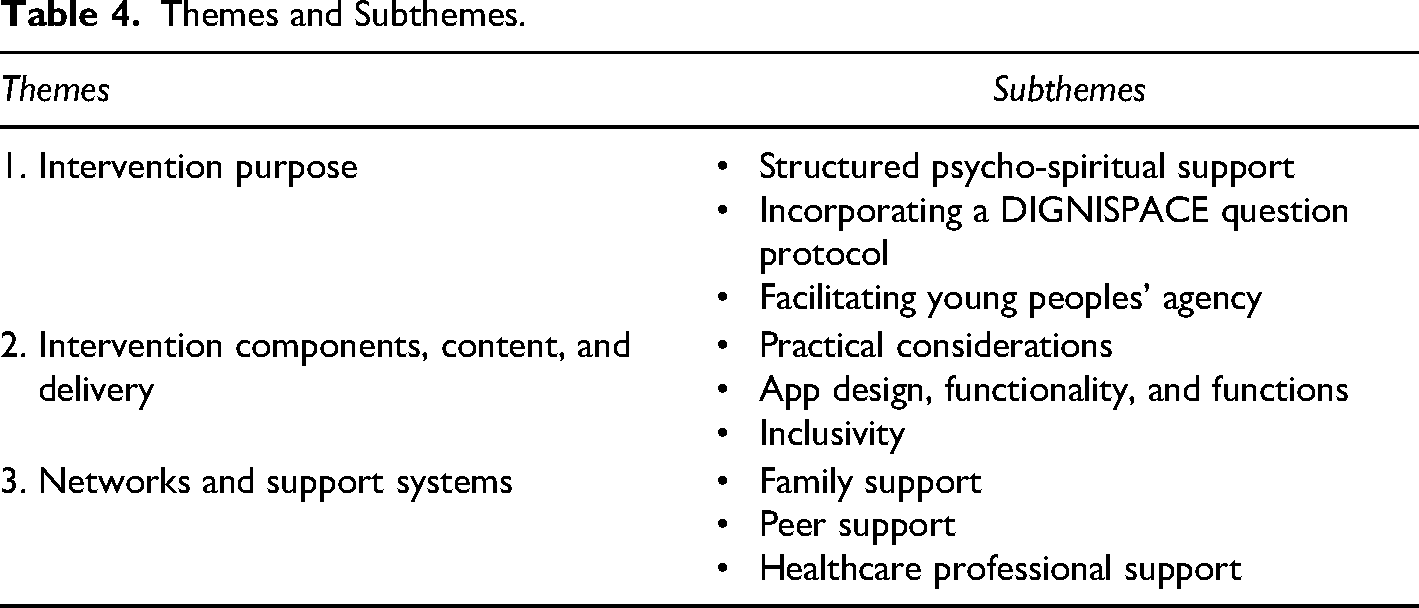
Findings from phases 1 and 2 were analysed, deriving three overarching themes influencing the development of DIGNISPACE: ‘intervention purpose’, ‘intervention components, content and delivery’ and ‘networks and support systems’ (Table 4).
Themes and Subthemes.
THEME 1: Intervention Purpose
Young people emphasised the potential of DIGNISPACE to help them make sense of their lives. Whereas healthcare professionals highlighted the value of an evidence-based tool in their practice to support young people's psycho-spiritual wellbeing: ‘I think this would be a lovely tool for them… and I think in the adult hospice world there's a lot of holistic and spiritual support need as well and which I think they will see the value in this as well… brilliant’ (Sarah, doctor).
Several young people talked about how they did not have an outlet for their troublesome thoughts and feelings. They had struggled to speak about their death anxiety and related wishes. Some had desires to talk about challenging topics in depth but did not feel they had anyone they could easily access to discuss these topics with. They did not want to place any more upset on their families and to uphold their dignity they wanted to be able to have control over what they spoke about, when and to whom, for example: ‘Talking about my life is something I’ve found difficult as I don't want to upset people around me. Having a space where I could share moments from my life good or bad would be a real weight off my shoulders mentally.’ (Simon, young person). ‘Just thinking about working with a young person… when do you feel most happy and what inspires you… that feels very current and that feels comfortable to ask somebody that. ‘ (Dehlia, therapist) ‘As soon as they start touching on them topics… the flood gates are going to open so… I think the phrasing needs to be sensitive and the support ready’ (Shafqut, parent). ‘I think it is important the activity is theirs… for some with neuro problems ownership might be difficult but the family can share that ownership… what is produced even if minimal, or if drawing on shared experiences would be extremely valuable’ (Mark, sibling).
THEME 2: Components, Content, and Delivery
Central to the DIGNISPACE app development were participant views about content, and practice delivery. There was some initial confusion amongst healthcare professionals with respect to how DIGNISPACE would be different to advance care planning. In sharing the Dignity Therapy question protocol and DIGNISPACE mockup, healthcare professionals could see how DIGNISPACE would be a supportive intervention separate to, but also complementing, advance care planning. Several of the healthcare professionals identified how DIGNISPACE would support young people and healthcare professionals to constructively discuss topics that may have therapeutic benefit. In practice there can be a struggle for young people to initiate talk and for healthcare professionals an absence of tools to assist timing and engagement, for example: ‘It's not to replace the children and young people's advance care plan; it's the idea of those therapeutic conversations, that's what this is meeting, and other tools don’t meet currently’ (Petra, nurse) ‘This is different to advance care planning, and I think more motivating… it's about wishes but it's about how life has gone…who am I… and what do I want to say… and pass on about myself, my experiences’ (Violet, young person). ‘Having someone who's trained to help young people talk though their worries and concerns is something I feel has been missing from mine and my son's life… we have a lot of medical support but no real support for his mental health’ (Joyce, parent). ‘To be honest… this is going to sound rude… but it is better than what I thought… Yes, I mean, it's really… it's got a really appealing interface’ (Poppy, young person). ‘Obviously you’d need a good navigation menu so you’d have the time capsule here (the time capsule incorporates all the DIGNISPACE questions and topic pages) with the key questions, you’d have your socials listed separate that you could lift content from’ (Julia, young person). ‘These you know some of my top memories, and these are the things I want you all to remember, and these are all the things I want you to learn, and you know my words of wisdom kind of thing would be so wonderful because I do think it's a beautiful thing to do… I'm a little nervous about the idea of the bucket list, calling it that’ (Melanie, doctor). ‘Maybe you could put when did you feel at your worst and how did you bounce back or something like that… It sort of normalises real life emotions. It's not always incredible, you have your rubbish times… and everyone has a bucket list’ (Nicholas, young person). ‘It would be good for all families living this, when they lose some capacity, it can get harder and harder but working on this together can keep us thinking about who that person is, they are still there inside what is happening to them and it could become a focus for us all and help us through’ (Michael, sibling). ‘We would need alt text to be able to help my daughter with the digital app, but I think the digital app allows you and them the space to get on with it or think about it at least’ (Marie, parent).
Participants identified how some questions would be more emotionally difficult than others, suggesting that there could be ‘locked’ sections/pages, and facilities to alert supporters to help young people to manage the more thought-provoking content from the outset (while still ensuring agency). Young people assumed support would be available for the more ‘difficult’ questions and suggested ways that support could be triggered. Shane suggested an informal approach: ‘(On alerting a supporter) Could it be a text? Yeah, like hello, are you okay, but very colloquial: are you okay, do you want to talk about …? Yeah, is all good, are you happy with what you’ve written, if not call us or give us a shout’ (Shane, 23 yrs., young person).
THEME 3: Networks and support systems
Participants’ suggested support networks be embedded into DIGNISPACE. Across participants the role of family was highlighted as fundamental in supporting young people and therefore, in the broadest sense, families could be involved in aspects of DIGNISPACE and legacy leaving activities. Donna further highlighted the diversity of young people and families in her care and the implications of such for engagement with DIGNISPACE: ‘I think some might need more help and support from families than others, some just no communication, but they haven't got the cognitive ability to understand any of this process whatsoever, and that it might be useful for the parents to do it on their behalf, and then be useful for the parents’, (Donna, therapist). ‘Lot of his (young person) questions were all about who was going to look after his family, they weren't about him at all, or they were about how his family was going to be, who was going to look after the family. What were they going to remember’, (Rebecca, Nurse). ‘They are now reflecting on the fact that one of their friends has died… they weren't able to say goodbye… they approached me to say, could we set something up’ (Jenny, therapist). ‘We are a small but tight knit community, when someone's child passes, we all feel and need to talk about it’ (Ayeman, parent). ‘I think that comes down to the therapists, well trained, well supervised in, knowing when's a good time and how to manage that conversation’ (Helen, therapist)
The Model of Dignity for Young People with Life-Limiting Conditions
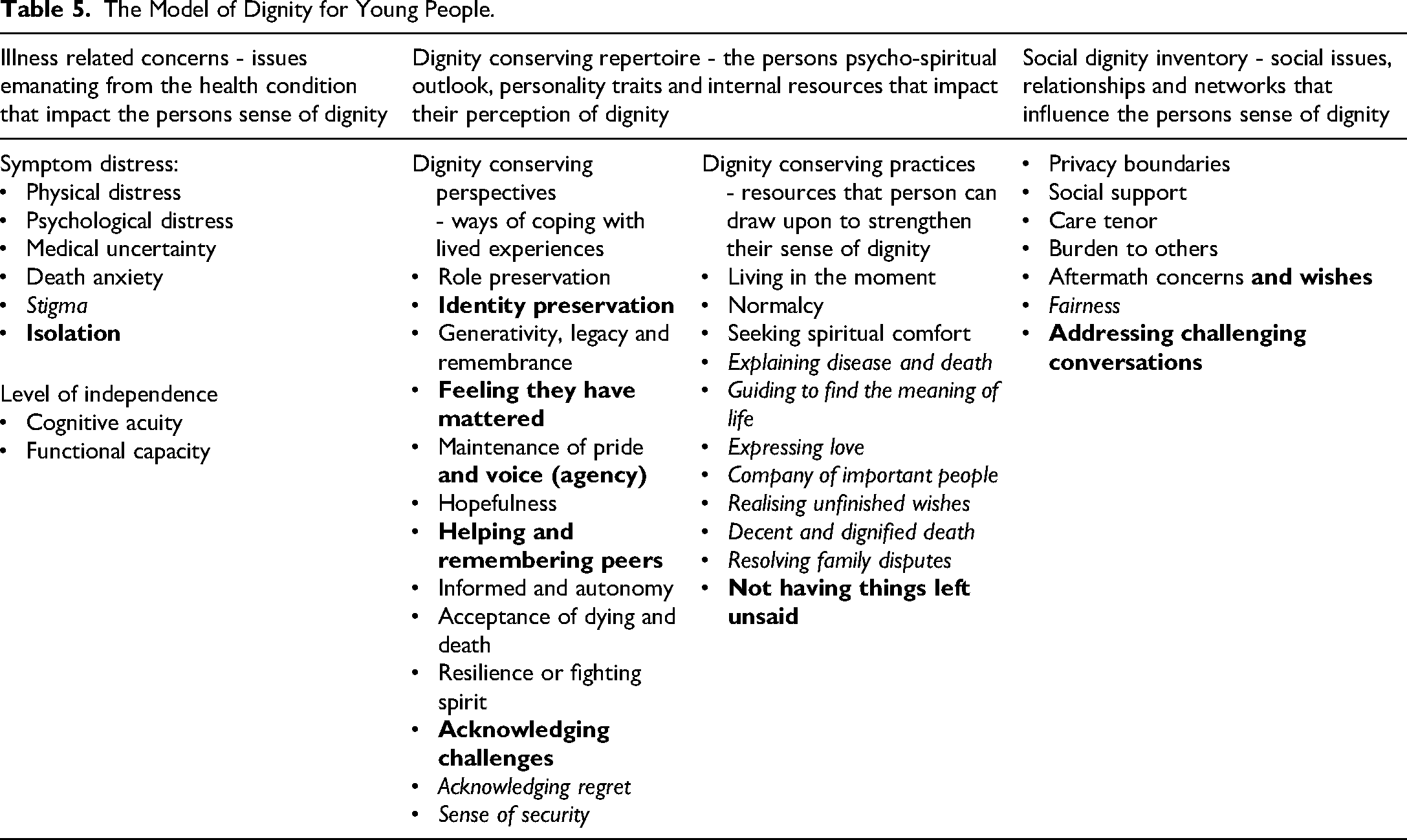
The model of dignity for young people with life-limiting conditions has been developed from the findings of this study, as highlighted in Table 5. Within this model, tenets of dignity relevant to young people with life-limiting conditions are highlighted in bold alongside the already identified tenets of dignity provided within the adult (Chochinov et al., 2002) and child (Cai et al., 2023) (provided in italics) models of dignity. The model of dignity in young people is considered within the DIGNISPACE question protocol and digital app prototype.
The Model of Dignity for Young People.
DIGNISPACE
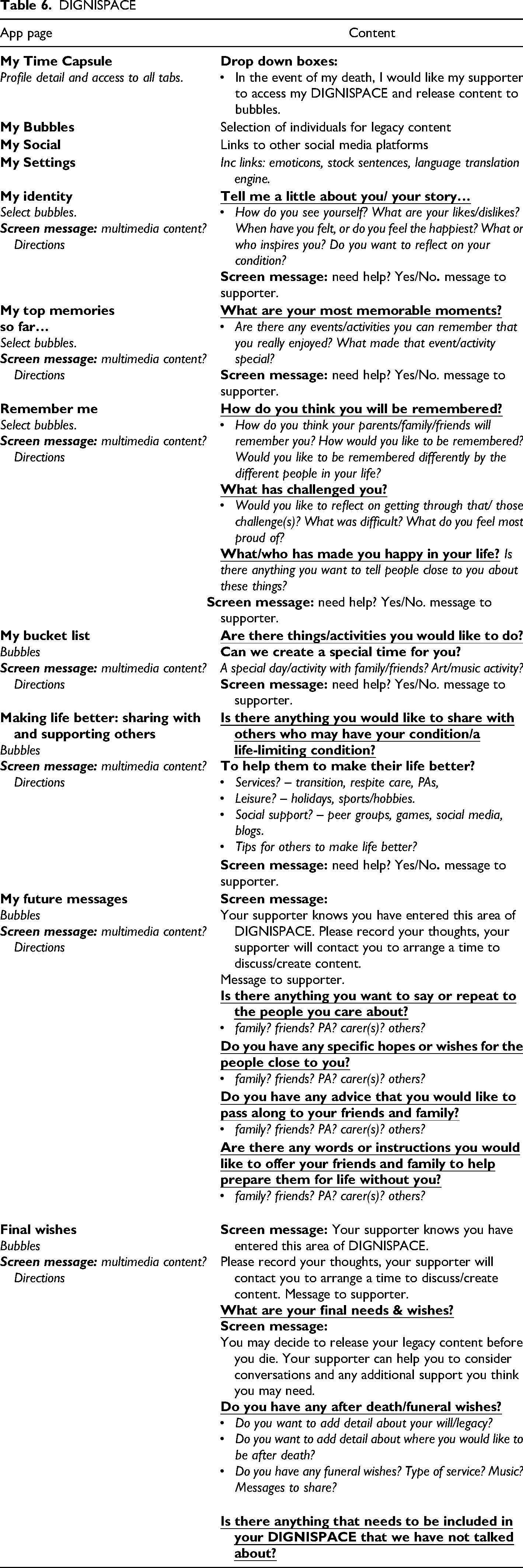
The DIGNISPACE app prototype is developed as a React Native app accessible via Android and Apple devices, and web browsers. The DIGNISPACE question protocol is mapped to defined sections, broken down into questions and prompts to assist user reflection and meaning-making. To ensure flexibility, users can insert multi-media content when completing questions. The app is built around the idea of bubbles: bubbles are groups of people the user wants to share information with. The user can define different bubbles with any number of people and share sections of the app with them. Users can request support from a healthcare professional (supporter) from within the app, generating a support request alert. The same mechanism applies for sensitive questions; they can be unlocked; a message is then sent to the supporter and content then completed with the supporter.
The app has been developed using:
Database: Secure and encrypted data repository in the cloud; implemented using mongo DB installed on a university server. API: Core element in the software that allows interaction between the database, the web app, and the mobile app – implemented in the form of a RESTFUL API, directly linked with the back-end (server and database) and the front-end (mobile and web visualisation). Web app: Application for users, accessible via web browser, to complete and review the questions. Mobile app: Smartphone application for users to complete questions with text, voice messages, photos and/or videos.
The DIGNISPACE app prototype content incorporating the DIGNISPACE question protocol is summarised in Table 6.
DIGNISPACE
Discussion
The study has co-designed a Dignity Therapy-based psychotherapeutic intervention for young people. DIGNISPACE (name suggested by advisory group and agreed by participants), considers what dignity means to young people and offers a solution to meeting some of the psycho-spiritual needs young people face in living with medical uncertainty and a shortened life prognosis.
DIGNISPACE is: An activity to promote dignity, psychological and spiritual well-being. Young people with therapeutic support are encouraged to reflect upon life experiences, poignant memories and related meaning making. They are supported to share identity forming elements of ‘their story’, to voice ‘their views’, detail ‘their wishes’ and create content of sentimental value and guidance for significant others including family members, friends, and peers. The activity content and processes enable young people to engage in challenging conversations and explore the many ways in which they have had purpose and impact across their lifetimes.
DIGNISPACE and Psycho-Spiritual Needs
A systematic review of Dignity Therapy highlights its international appeal with studies undertaken in North America, China, Japan, Taiwan, New Zealand, Australia and Western Europe (Martínez et al., 2017). Several randomised controlled trials have explored its effectiveness compared to standard palliative care, with improved outcomes in anxiety, depression, quality of life, sadness, dignity and a sense of purpose (Chochinov et al., 2011; Hall et al., 2011; Juliao et al., 2014; Rudilla et al., 2016; Silva et al., 2019). It is possible that DIGNISPACE could reduce psycho-spiritual burden in young people to a greater effect than standard palliative care.
With increasing medical advancements young people are living longer sicker or with increased frailty (Cook et al., 2016). This impacts the complexity of their psycho-spiritual needs, particularly as they move to adult services with differing support available (Barker et al., 2019). A recent review of adult palliative care for young people discussed themes linked to psycho-spiritual burden and adjustment difficulties, suggesting many young people (irrespective of location) receive no or very little specialist support (Abdelaal et al., 2023). We found emotional distress was mostly linked to feeling isolated, a loss of privacy and the fear of dying. Many participants coped by comparing their own condition to others or by drawing on the deeper meanings of their ‘suffering’ (Silva et al., 2019). To some degree humour and engagement with peers is helpful but there remains a need for tailored support (Jamalimoghadam et al., 2019; Mohammadi et al., 2023).
In addition to the considerations of Chochinov and colleagues (2002) and Cai and colleagues (2023) in their models of dignity conserving care and dignity in children respectively, the dignity of young people is impacted by several additional tenets. In considering illness related concerns leading to psychological distress, being or feeling isolated is relevant to this group. Dignity conserving practices including the need to preserve identity, feeling they have mattered, maintaining their voice and agency, helping, and remembering others and acknowledging the challenges they both have faced and overcome are important. In addition, dignity conserving repertoire practices for young people include the desire to not have things left unsaid. In terms of the social dignity inventory, it was important for several participants that not only would aftermath concerns be addressed but also their post death wishes be acknowledged alongside other challenging conversational needs.
It was important to participants that DIGNISPACE would be inclusive and flexible to the needs and abilities of all its potential users. The use of storytelling, narrative, and multimedia can enable creative DIGNISPACE content and help people even with profound and multiple disabilities to have their preferences acknowledged about their lives and wishes (Watson et al., 2019). It is in this way that DIGNISPACE offers a mechanism to give voice to young people who are seldom “heard” especially those with difficulties communicating their needs with words or whom may not have a shared first language with their formal carers (Liddiard et al., 2019; Spencer et al., 2020).
Young people enjoy arts-based activities for memory-making (Foster et al., 2012), but there are no structured tools for healthcare professionals to use to support allied meaning-making and legacy leaving. The Children and Young People's Advance Care Plan Collaborative (2023) supports healthcare professionals, providing resources, to plan and record end of life directives. However, the focus is on care choices. DIGNISPACE could enhance advance care planning, offering young people, families, and healthcare professionals a structured approach to preserving dignity, offering broader psycho-spiritual support, and incorporating much creativity.
Implications for Practice
Studies suggest end-of-life conversations are best introduced by palliative care teams (Sansom-Daly et al., 2020). Healthcare professionals with experience of working with young people could be trained to become DIGNISPACE supporters. DIGNISPACE supporters would need to introduce and guide young people to use DIGNISPACE, help them to develop content, work with them through emotions and address adjunct challenging conversations. The digital app is designed to have inbuilt flexibility with functions to support physical needs and to work with family units if preferred. DIGNISPACE could strengthen partnerships between child and adult palliative care services and offer a new approach to community palliative care through transition.
Implications for Research
Through this study some of the challenges that healthcare professionals and families can face in supporting young people to address their psycho-spiritual needs have been identified and these warrant further investigation. The tenets of previously derived models of adult and child dignity are relevant to the participants of this study. However, further important tenets of dignity for this group have been identified and considered within a model of dignity in young people. This model of dignity could be used for the development of other dignity focused interventions for young people.
Further research is needed to explore the role of Dignity Therapy-based interventions in supporting young people at home and especially through transition to adult services. DIGNISPACE will be feasibility tested and the fidelity of training across child and adult hospice settings explored, examining the effectiveness of different models of healthcare professional support. This work will consider young people's behaviour change and engagement and how and in what ways communities of DIGNISPACE practice are formed.
Study Strengths and Limitations
To our knowledge this is the first study that has co-designed a Dignity Therapy-based intervention to be delivered digitally. As a research team we were guided by an expert by experience team member and an advisory group of young people and family carers. However, because hospices offer fewer short breaks compared to pre-pandemic service levels, our ability to promote the study to families, and to support recruitment was impacted. Sadly, several young people were unable to participate due to their health deterioration or death. However, a depth of data was still achieved.
Conclusion
Evidence based interventions to support young people's psycho-spiritual needs are limited. Dignity Therapy is a validated approach that young people view as acceptable, however, the question protocol and delivery of DIGNISPACE is more reflective of their lives lived and accessibility needs. DIGNISPACE is the first co-designed Dignity-Therapy-based intervention for young people that can be delivered digitally. It is proposed that DIGNISPACE will complement the excellent work already undertaken in hospices and palliative care teams by providing a supported, structured intervention for young people (and where appropriate families) to engage in life reflection, meaning making and legacy leaving.
Footnotes
Acknowledgements
We would like to acknowledge Dr Mari-Cruz Villa-Uriol and Mr Jiaqi Fu, University of Sheffield, for their work assisting VL with digital design and coding. We would also like to thank all participants for sharing their experiences and perceptions and to members of the advisory group ‘Striding Forward’ for their consistent support and guidance. We would also like to thank Prof Harvey Max Chochinov for his support at the time of study design and set up, to use the Dignity Therapy materials. Finally, we would like to remember Miss Lucy Watts MBE, research team member and youth ambassador, whose ideas and strength of commitment to this work was invaluable.
Author's Note
Joanna Smith is currently affiliated with College of Health, Wellbeing and Life Sciences, Sheffield Hallam University, Sheffield and Sheffield Children's Hospital, Sheffield.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this publication was supported by the National Institute for Health Research (NIHR) Devices for Dignity MedTech Co-operative. The project was funded by the National Institute for Health and Care Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant reference number NIHR201597). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.