
Abstract
There is growing international evidence of the benefits of early perinatal palliative care for babies and their families. Despite this, inconsistency remains in ways care is provided by services including fetal medicine, maternity and neonatal services, and children's hospices. The aim of this study was to answer the question “What are the benefits and barriers to family-centered perinatal advance care planning from the perspective of professionals involved in the care of neonates and infants with life-limiting conditions?” Three focus groups comprising hospice practitioners were held across the UK. A lack of awareness of the role of hospices was described as the biggest barrier to referral to hospice services. Practitioners unanimously described having a physical presence alongside teams, as being the biggest contributor to improved multiagency working, facilitated through joint working and education provision. Early referral to hospice services, in parallel with curative services led to better outcomes and experiences of families, according to participants.
Keywords
Introduction
Perinatal palliative care is increasingly available for babies diagnosed with a life-limiting or life-threatening condition (LLLTC) while in-utero or up to one year after birth (Doherty et al., 2019), and their families. Despite there being growing international evidence of the benefits of early perinatal palliative care for babies and their families (Cortezzo et al., 2013; Cortezzo et al., 2019; Hancock et al., 2018; Niehaus et al., 2020; Wool & Catlin, 2018), inconsistency remains in the care that is provided by secondary care services such as fetal medicine, maternity and neonatal services, as well as children's hospices (Boan Pion et al., 2021; Tatterton et al., 2023). This widespread variability in care means that there are inequalities and inequities being experienced by parents, babies, and their families who are journeying through the unknown territory of perinatal palliative care.
Perinatal palliative care pathways ensure parents and their babies experience a family-centered approach to care, where their individual thoughts, feelings, needs, and choices are listened to, documented, and shared across the multidisciplinary team, as to ensure consistent, compassionate, and coordinated care (Dickson, 2019; NHS England, 2023; Together for Short, 2017). Parents have strongly iterated their need to have care, support, and guidance, which is empathic, transparent, and timely after their baby has been diagnosed with a LLLTC (Branchett & Stretton, 2012; Crawford et al., 2021; Fleming et al., 2016; Tatterton & Fisher, 2023; Tatterton et al., 2023). Having a sense of control, being validated, and making memories throughout their journey has also been found to significantly impact on their experiences (Tatterton & Fisher, 2023; Thornton et al., 2021). The National Institute for Health and Care Excellence (2016) recommends the use of advance care planning with parents during the antenatal period, which has been found to enhance communication and support parents with their decision-making (Cortezzo et al., 2019; Doherty et al., 2019; Tucker et al., 2021; Wool & Catlin, 2018). The aim of perinatal palliative care planning is to ensure parents are active participants in every step of their uncertain journey, where they feel empowered and able to advocate for themselves and their baby (Vetcho et al., 2020). Not only this but it gives parents time to consider and plan for birth once their baby is born, including comfort care and symptom management (Martín-Ancel et al., 2022).
Fraser et al. (2021) estimate that 226.5 per 10,000 infants (<1 year old) are diagnosed with a LLLTC, far greater than any other group under 19 years old and recommends the need to prioritize their access to palliative care. Even though technological advancements have increased the identification of a LLLTC in-utero (Power et al., 2018), suggesting that often there is time and opportunity to make referrals for hospice care, it is purported that 98% of neonates die in the hospital setting (McNamara-Goodger, 2009), rather than in a hospice or at home.
There are 54 children's hospices in the UK (Together for Short, 2017). Hospice practitioners are skilled in integrating a family-centered, biopsychosocial approach to care, which has been found to improve outcomes for families (Danguecan et al., 2021), including bereavement (Zimmermann et al., 2022) and effective symptom management (Moore et al., 2018).
Following the completion of a national children's hospice survey, we know that there is not one single approach taken by hospices to meet the needs of families of babies diagnosed with a LLLTC perinatally (Tatterton et al., 2023). We would like to explore professional experience and perspectives of perinatal palliative care, using focus groups. This is because focus groups have been shown to stimulate the sharing of attitudes and opinions on sensitive and underinvestigated topics (Shaha et al., 2011) and therefore offered an appropriate means of exploring the perceptions of staff involved in planning and delivering family-centered, perinatal palliative care.
Aim
The aim of this study is to better understand how children's hospices contribute to care of babies and their families where a need for palliative care has been recognized. Due to the limited understanding of the contributions and working practices of children's hospices, a descriptive qualitative study using focus groups was developed. The overall aim of the study was to answer the question “What are the benefits and barriers to family-centered perinatal advance care planning from the perspective of professionals involved in the care of neonates and infants with life-limiting conditions?”
Method
This study was part of a larger project exploring the role of children's hospices in the provision of perinatal palliative care in the United Kingdom (Tatterton & Fisher, 2023; Tatterton et al., 2023). This study aimed to build upon a recently completed national survey (Tatterton et al., 2023) to understand the perspectives of practitioners on the role and impact of children's hospices in providing family-centered perinatal palliative care, by employing their experiences of being hospice-based practitioners.
Research Design
Framework analysis was used to analyze focus group data, generating themes by making comparisons within and between groups. Consolidated criteria for reporting qualitative research guidelines (Tong et al., 2007) have been used to design, analyze, and report this research.
Framework analysis was selected as an approach due to its structured yet flexible approach to analyzing qualitative data for applied health research. The method has become a popular approach in multidisciplinary health research (McKenna et al., 2022), particularly in nursing, psychology, and sociology disciplines (Ward et al., 2013). Framework analysis comprises two distinct components of creating, then applying, an analytical framework, using five steps (Goldsmith, 2021) which are:
Data familiarization: including verbatim transcription of the interview recordings and purposeful, familiarization with the data, by relistening to the recording and reading transcripts. Goldsmith (2021, p. 2063) notes that “coding can be a part of the data familiarization process, but it is not required.” In this study, we coded the transcripts. Identifying a thematic framework: by comparing codes and agreeing coding sets to be applied to subsequent transcripts, based on emergent concepts and themes (Ritchie & Spencer, 1994). Indexing all study data against the framework: by systematically applying the framework to all data from the study. Charting to summarize the indexed data: balancing the reduction of data, while preserving the original meaning and feel of the focus group and enhancing decisions around analysis. Mapping and interpretation: combining, agreeing, and expressing the key learning from the analysis across and within the framework components.
Participants
Participants were identified through participating hospices. In a preceding national survey, sent to all children's hospices (Tatterton et al., 2023), hospices were asked if they would be willing to host a focus group to explore the experiences of staff members. Invitations were sent to those hospices who indicated a willingness to take part.
To be eligible to participate, practitioners must:
work in a children's hospice in the UK have been involved in the planning or delivery of care for babies and their families in the perinatal period—this can include antenatally, before the baby is born, or shortly after birth, in the neonatal period.
Ethical Considerations
The study design and procedures were approved by the University of Bradford Research Ethics Panel (reference: E998) and the relevant clinical governance committees of Bluebell Wood and Martin House Children's Hospices. The Integrated Research Application System indicates that review by the UK Health Department's Research Ethics Service is not required, as the research is “limited to involvement of staff as participants” with no involvement of patients or service users as participants. Informed consent was obtained from all participants prior to each focus group. No financial incentives or payments were made to participants.
Participation in the focus groups will not be disclosed by the research team, and participants in the focus group were asked to respect the confidentiality of their fellow participants. Individuals have not been named in any reports or publications. Names of individuals and organizations have been redacted, described only as “hospice,” “hospital,” or “community nursing team.”
Data Collection
Data were collected in semistructured focus groups. Focus groups lasted between 60 and 90 min and were conducted using Microsoft Teams to facilitate attendance. A focus group schedule, informed by the findings of an earlier study (Tatterton et al., 2023) was used to structure discussions, the themes of which are shown in Figure 1.
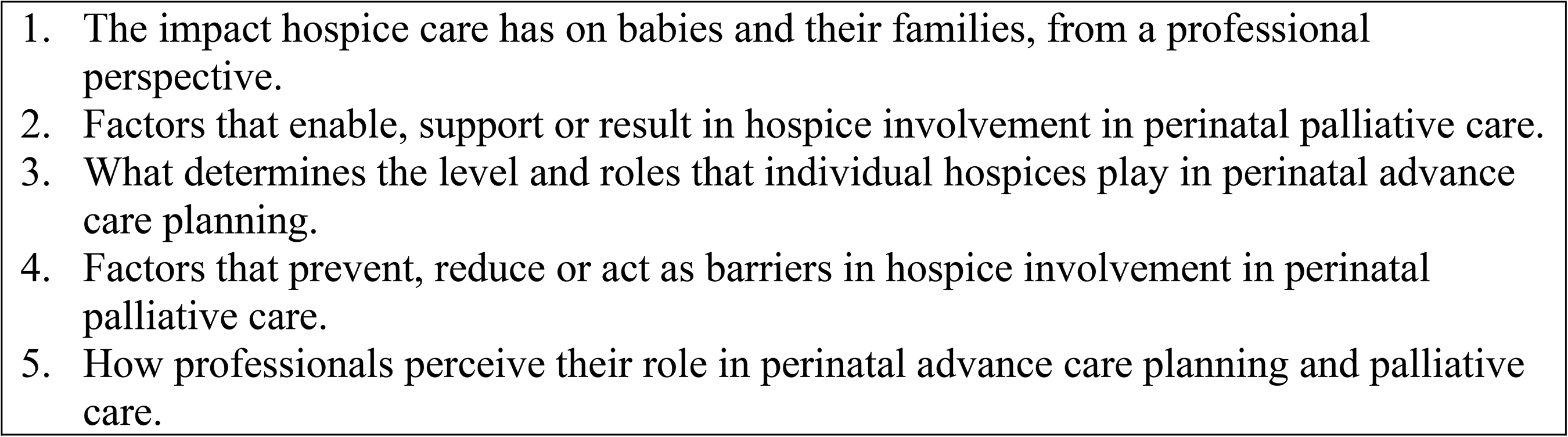
Discussion guide for the practitioner focus groups.
Focus groups consisted of five to ten practitioners and two members of the research team, as convenors. One lead the discussion in each focus group and guided participants through the discussion (see Figure 1). One convenor acted as chair. Focus groups were audio recorded and the researchers made fieldnotes during the meetings.
Data Analysis
A framework analysis approach (Gale et al., 2013) was used to analyze data from the focus groups, to explore professional experience and perspectives of perinatal advance care planning and the impact it has on babies and their families. Framework analysis is particularly suited to analyzing cross-sectional descriptive data (Smith & Firth, 2011). A priori codes were not used.
Findings
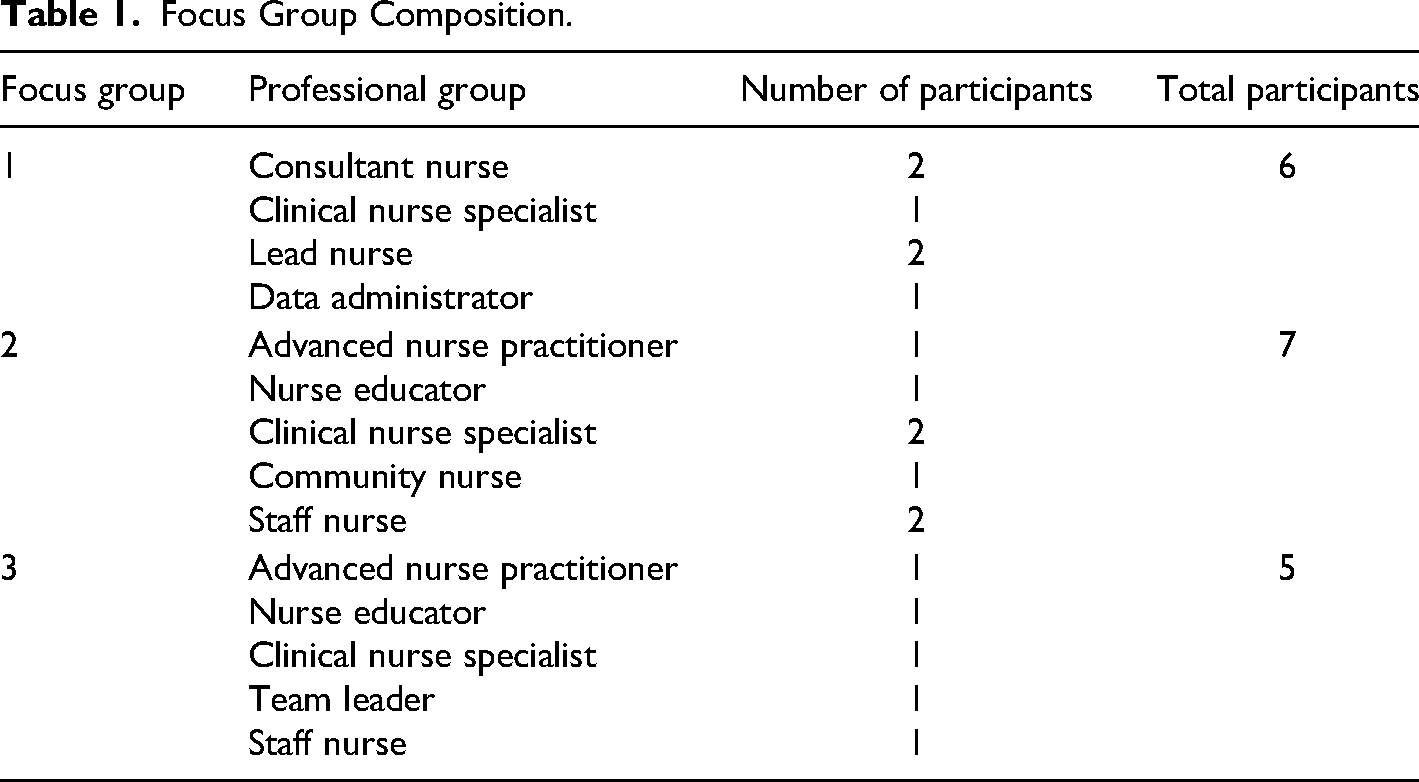
Eighteen practitioners, representing three children's hospices participated in the focus groups, as shown in Table 1. All participants were experienced in supporting families and providing perinatal palliative care. All focus groups coincidently had participants who had previously worked in neonatal units, allowing some participants to reflect on their experiences in both clinical environments.
Focus Group Composition.
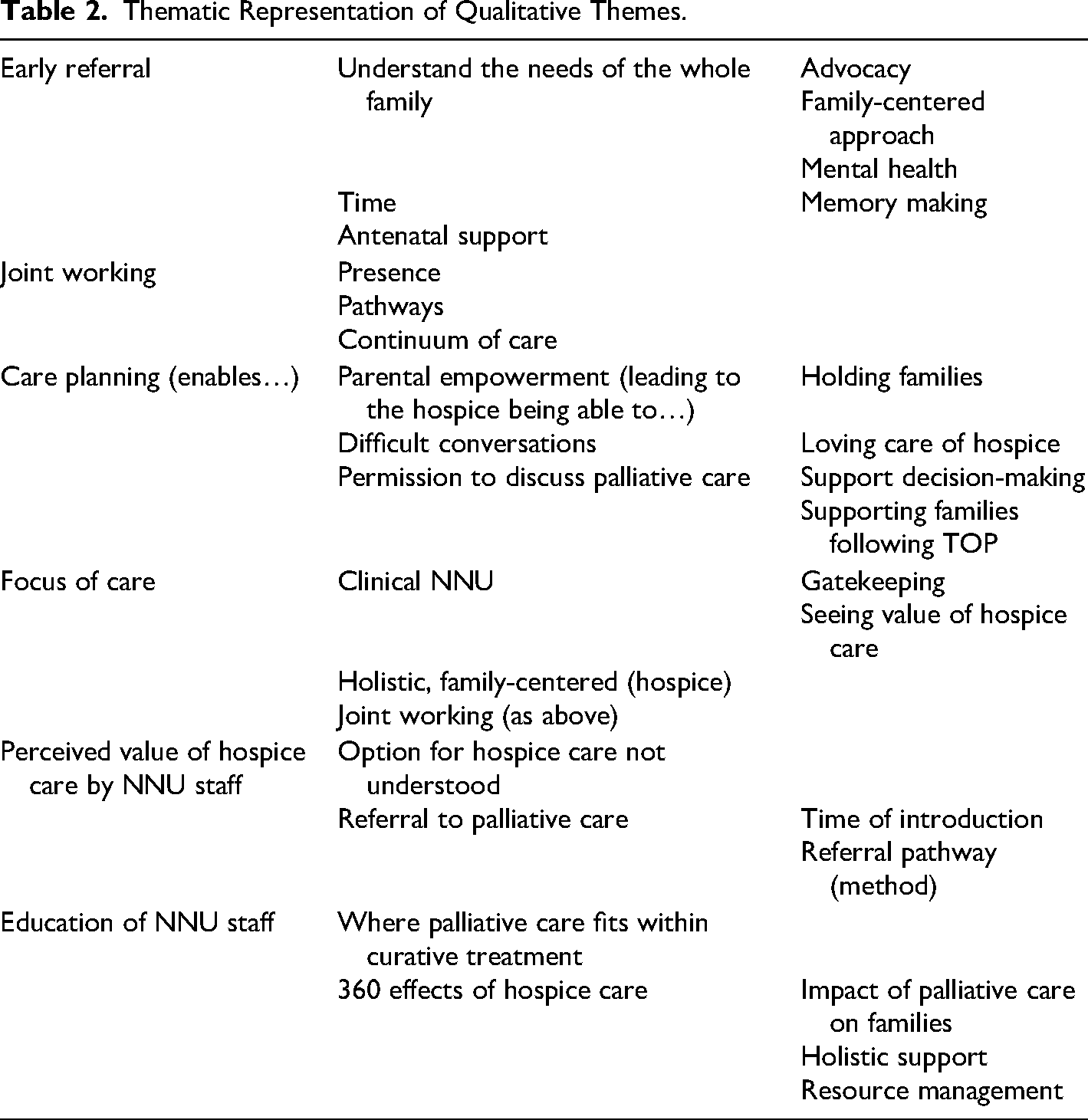
As shown in Table 2, following the initial analysis of transcripts, six themes and 31 subthemes were identified. Further refinement of the themes led to the development of a conceptual framework comprising five core themes (described as “concepts” by Smith & Firth, 2011), that demonstrates the relationships between themes, shown in Figure 2. These are: (1) hospice presence, (2) reducing barriers to perinatal palliative care, (3) strategies that enhance interprofessional working, (4) strategies that promote hospice involvement, and (5) enabling early referral to children's hospices.
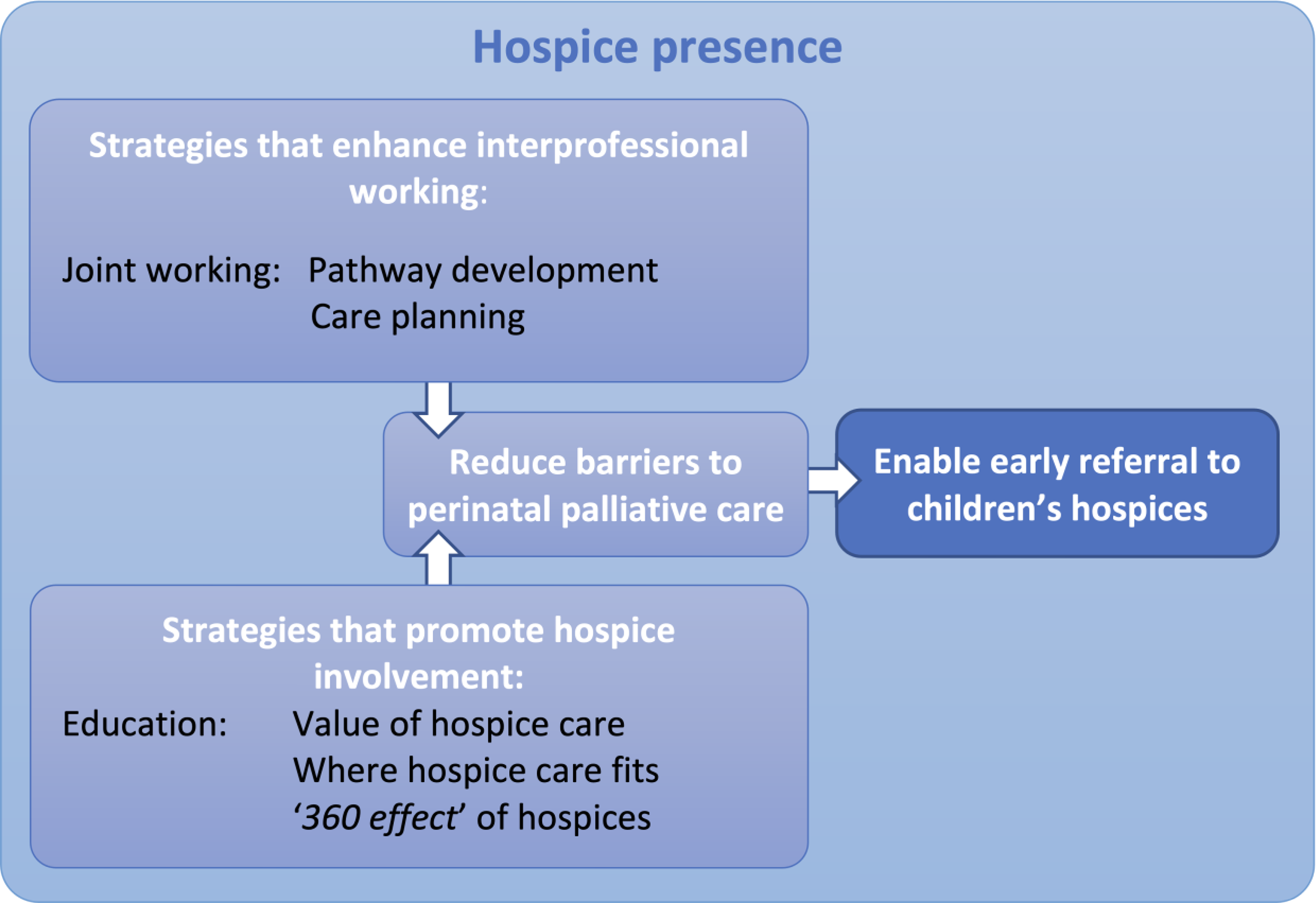
Conceptual framework of identified themes.
Thematic Representation of Qualitative Themes.
“Holding Families in Uncertainty”: Hospice Presence
The presence of hospice practitioners on neonatal units was highlighted by participants in all focus groups as being central to the establishment and maintenance of effective working relationship between organizations. It was widely regarded as integral to the development of care pathways, and an enabler to families accessing hospice-based support. “we’ve found that it's not always necessary to have a set purpose or reason to be on the [neonatal] unit, or to sit with families during consultations and appointments. There's no agenda, but it's about us holding families in their uncertainty, letting them know that there are options, and that its okay to talk about any or all of them, at any time.”
The importance of key members of the neonatal teams, particularly neonatologists, was highlighted by participants in all focus groups. Participants described how acceptance was often initiated by a consultant neonatologist, which resulted in other professionals, including nurses, accepting the support and input of hospice practitioners.
“I’d say that the neonatal and fetal medicine consultants are the most influential relations we had in the early days. We work really closely with senior nurses and the midwives, but I think it's definitely the doctors that I had to influence that then cascaded acceptance to the rest of the team.”
Reducing Barriers to Perinatal Palliative Care
Several barriers were highlighted by participants, particularly surrounding acceptance of palliative care, time, and the protective nature of neonatal staff toward babies and their families. Neonatal staff were not the only professionals that hospices work alongside to provide palliative care; midwifery, fetal medicine, and general practice services were also highlighted. Acceptance of the need (or potential need) for palliative care was discussed, and how this can prevent the referral or involvement of palliative care services, particularly when there is uncertainty around prognosis, which results in later referrals.
The time at which to introduce hospice care to families was perceived as a potential barrier too, with participants expressing concern that key opportunities were missed, resulting in later referrals. This prevented families from benefiting from some of the benefits of hospice care, particularly around enabling conversations around palliative care, the provision of holistic, family-centered emotional support, and memory-making activities. One of the focus groups discussed their frustrations around families needing to consent to palliative care involvement unlike other clinical specialties. “[Families] are not given the option whether they see a cardiologist when their baby's got a heart problem. So, if the baby has a palliative condition, why should they be offered a hospice?”
Strategies That Enhance Interprofessional Working
This theme describes what children's hospices do to ensure effective professional relationships and working practices with perinatal services. These practices result in families being offered responsive and flexible care services.
Joint Working
Joint working enabled the movement of families between care services, and for open discussions about care planning at all stages of a family's perinatal journey. It allows families to make uncompromised choices in their place of care and to understand the implications of such decisions, improving transparency, and movement between services, for both babies and mothers.
Pathway Development
The development of a care pathway was described in all focus groups as a means to ensuring a consistent and sustainable approach to care provision. These were different in each focus group, designed to reflect the NHS perinatal services offered to families locally, and the hospice-based services available to them. Effective pathways centered around choice and care planning, allowing advanced decisions to be made. Key points for referrals, as well as the expectations of all partner agencies, were reflected in the pathway that was negotiated and agreed by all involved in the perinatal support of families.
Care Planning
A variety of approaches to care planning were highlighted in the focus groups, again, centering around enabling family choice and allowing for the dynamic and sometimes unpredictable nature of antenatal and neonatal prognoses. Three types of planning were discussed: birth planning, advance care or end-of-life care planning, and parallel planning.
Birth planning was recognized as an important part of the parenting journey, acknowledged by all groups as providing families with a sense of control and normality. Participants described how they supported families to demedicalize planning, providing advocacy and supporting families to achieve birthing experiences such as water births and calmness, despite the anticipation of medical support for their baby. “[I worked with a] consultant midwife who said if that's really important to her, we will do a risk assessment and see if it's appropriate. It might not be for the full process of delivery, but it gives [parents] the feeling [of] control and some wishes. […] It was about giving them permission to explore it and it makes the birthing process of more positive experience.” “I remember having difficult discussions with one consultant who said “ this family has chosen to continue [with their pregnancy] so what value are you adding?” I reminded [the consultant] that we didn't know how the baby was going to look when they were born and so it was about and talking to them about we're preparing them for their future and the different eventualities of what might happen.”
Strategies That Promote Hospice Involvement
This theme describes the means by which hospices instilled a sense of confidence and understanding in the role and scope of hospice-based care services. These included education around the benefits of palliative care, the value of hospice care, and what was described by one participant as “the 360 effect of children's hospice care,” describing the family-centered, biopsychosocial approach to care.
Education
Participants described working with perinatal service providers, particularly neonatal services, to provide education relating to palliative care, particularly around clinical issues, bereavement and grief, and advance care planning. Participants discussed how these training sessions enabled dialogue between services and increased the awareness and credibility of hospice-based palliative care services. “Neonatal colleagues need to know about palliative care, advance care planning, parallel planning—all of those things. Because if they don't have that education, then they won't have a clue how to educate a parent or about when to refer families.”
The Value of Hospice Care
The contribution of hospice care to families during pregnancy and following the birth of a baby diagnosed with a life-limiting condition extends beyond meeting the clinical needs of a baby. Participants discussed education around the family-centered approach to care, and how hospices can support families in making uncompromised choices in relation to the pregnancy are care planning, including decisions around termination of pregnancy, and curative or palliative options.
The role of hospices in relation to parental and family advocacy was highlighted, as was the provision of emotional support and well-being, and bereavement support before and after the death of a baby. All hospices represented by the focus groups highlighted the support available to parents, siblings, grandparents, and other family members, although the way these services were arranged varied between organizations.
Where Hospice Care Fits
It appears that the role of hospices was initially misunderstood by fetal medicine, community midwifery, and neonatal services. Focus group participants who previously worked in neonatal units described how they frequently cared for dying babies, but that palliative care in a hospice felt very different: “I found it quite difficult when I first started working [at the hospice]. I thought I was good at caring for babies who were dying, but I’m not sure that really was palliative care—it's all the wrap around stuff [the hospice] do, for example one of our music therapists have just created a piece of music with a baby's heartbeat in it, and the siblings have got involved with that too.”
The “360 Effect” of Hospices
Participants highlighted that the effect of timely hospice care not only benefitted babies and their families but also impacted on the neonatal unit more widely. Such benefits include the provision of family-centered emotional support, memory making and the transfer of care to hospice inpatient units, enabling the freeing up of neonatal cots. These benefits were promoted in education sessions, enabling neonatal staff to appreciate the broader implications of hospice care, described as the “360 effect of hospice care” by one participant: “Hospice involvement doesn’t just impact on the family receiving the care, it can affect the whole unit. It frees up neonatal staff and reduces pressure on them. Knowing that the baby could be transferred to a hospice impacts on staff resilience. Hospices kind of have a 360 effect—it's not just families that they help.”
Enabling Early Referral to Children's Hospices
All participants across all focus groups advocated for early referral, discussing the wide-ranging, positive effects of palliative care provided by hospices. These centered around the establishment of effective therapeutic relationships with families, where hospices understand the individual needs and wishes of parents and other family members, enabling the tailoring of support.
It meant that care planning, in whichever form, was more meaningful and open, due to the trust built up with families. This was particularly evident in conversations around controversial decisions, such as termination of pregnancy, where families may otherwise feel judged: “Parents can be afraid that they're being judged for decisions, which makes the difficult situation they’re in even more difficult, because they can't talk about it. And that's why whenever I do go to families, I say, you can tell me anything. You can talk, you won't be judged—I won't judge you. Everybody has the right to make whatever decision is right for them.”
Discussion
This study explored the perspectives of practitioners working in British children's hospices, around their experience of planning and delivering perinatal palliative care, using framework analysis. A conceptual framework was developed, which describes the role of hospices in the provision of perinatal palliative care, and the strategies used to strengthen relationships with colleagues across agencies, improving the care pathway for families. A lack of awareness of the role of hospices was described as the biggest barrier to referral to children's hospice services. Practitioners unanimously described having a physical presence alongside teams, such as fetal medicine and neonatal units as the biggest facilitator to improved multiagency working, through joint working or the provision of education. Early referral to hospice services, provided in parallel with other, perhaps curative services led to better outcomes and experiences of families, according to participants.
A lack of awareness of the services that children's hospices offer and the association between hospices and death are frequently cited as barriers to engagement with hospice care. Limited understanding of the breadth and scope of hospice care result in practitioners failing to see the potential benefit of referral until the baby is nearing the end of life (Leong Marc-Aurele & Nelesen, 2013; Pentaris et al., 2018). The benefit of early referral to hospices is widely cited in literature (Davis et al., 2022; Falke & Rubarth, 2020; Neuburg, 2021). Earlier referrals are associated with better family–practitioner relationships (Patra et al., 2022; Schockett et al., 2005; Tatterton et al., 2021; Teno et al., 2007), leading to more comprehensive understanding of the needs of families (Boyden et al., 2021; Tatterton & Walshe, 2019; Winger et al., 2020), and stronger therapeutic relationships (Price & Mendizabal-Espinosa, 2019; Tatterton et al., 2021).
The nature of neonatal care means that care is often delivered in the neonatal unit, and provided by a specialist neonatal staff (Kain & Chin, 2020). Neonates tend to be cared for as inpatients until they are ready for discharge home (Mancini et al., 2020). Despite the relative frequency of death in neonatal units (Cambonie et al., 2023), the role of children's hospice is in supporting families, and staff around this is yet to be established in some units. Education was seen as a facilitator to this, where hospices provide learning and development opportunities to neonatal units. There is a strong association between education and service development (Park et al., 2022; Roddy & Polfuss, 2020) and the association between education and workforce culture change (Day, 2019; Williams et al., 2015).
The presence of hospice practitioners on neonatal units and during ward rounds enabled the development of relationships between practitioners across organizations, consolidated through regular opportunities for joint working. This appeared to work best where care pathways have been established. This is supported in the wider literature (Baxter et al., 2020; Gebauer et al., 2022; Selby et al., 2019), where effective joint working is associated with improved patient experiences, reduced errors, and more efficient transitions between services.
The effect of stronger, more efficient links between services and a greater understanding of the role and potential impact of hospice services can result in the provision of better palliative care for babies and their families (Price & Mendizabal-Espinosa, 2019; 2023) and better bereavement outcomes (Zimmermann et al., 2022).
Strengths and Limitations
This study is the first to explore the role and impact of children's hospices providing perinatal palliative care, from the perspective of express professionals. The coproduction of the study, developed with academic and clinical practitioners was a particular strength of this work. We believe the findings are internationally relevant to those involved in the care of families during and following pregnancy, including fetal, maternal, and neonatal services. This study is not without limitations. The nature of focus group discussions means that participants may have been hesitant to express full and honest opinions. Participants of all three focused groups included in the study were predominantly from a nursing background. Multidisciplinary focus groups may have yielded different results. Future studies should build on this work by exploring interdisciplinary perspectives, as well as those from parents and families who have experienced perinatal palliative care.
Conclusion
Hospices play an important and growing role in the provision of perinatal palliative care to babies and their families following the diagnosis or recognition of a life-shortening condition. Stronger working relationships between organizations lead to an improved experience for families, including services that are flexible and responsive to the dynamic needs of families. The development of care pathways strengthen these relationships and promote joint working, which enable efficient transitions between services and improved experiences for families before and after the death of their baby.
Footnotes
Acknowledgments
The authors are extremely grateful to the children's hospices who participated in the focus group discussions.
Authors’ Contribution
MJT, MJF, HS, ZPM, and CW were involved with conception and design of the study, as well as critical review of the literature and review of the paper from draft to completion. MJT and MJF acquired and analyzed data and also managed data curation. Clinical support was provided by HS, CW, and ZPM. MJT and MJF took the lead in drafting the manuscript. HS, ZPM, and CW provided reviews and editing as well as clarification where appropriate.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is part of the SURE Research Project funding for the project: “Multistakeholder perspectives of advance care planning in perinatal palliative care: an evaluation of current practice in the UK,” University of Bradford, reference DA5151.