
Abstract
This study focuses on the subjective well-being (SWB) of a sample of military veterans before and after their engagement with a nonclinical, alternative mental health therapies residential retreat in the United Kingdom. The study findings have relevance for trauma-exposed individuals globally. Military veterans will actively avoid seeking traditional mental health treatments due to factors such as stigma and life-long labels, as well as a reluctance to engage in talk therapies. This is despite the widespread occurrence of diagnosed and undiagnosed chronic mental health conditions such as posttraumatic stress disorder following periods of service. Moving beyond trauma-informed practice and embracing a healing-centered approach involving holistic therapies delivered during a retreat-type format has a positive impact on the SWB of service users. Positive changes in SWB were recorded using the Warwick–Edinburgh Mental Well-Being Scale and the lived experiences of the participants. A shared military identity contributes immeasurably to a veteran-centered approach to holistic therapy, healing, and recovery.
Keywords
Introduction
The well-being of serving military personnel, military veterans, and others such as emergency services first responders, who routinely face traumatic events, now occupies an elevated position within policy-making agendas and in academic research globally (Albertson et al., 2019). Within public, private, and third-sector organizations (e.g., military-related charities), there is unanimous support for interventions and well-being measures that alleviate the higher levels of common mental health issues such as anxiety, depression, chronic pain, sleep disturbance, posttraumatic stress disorder (PTSD), and suicide among military veterans, when compared to the general population. The situation is highly complex because military veterans are less willing to come forward for traditional mental health therapies. The benefits from conventional psychological therapies and interventions are also less pronounced. Identities are intersectional and there are gender differences in the occurrence of psychological difficulties among the veteran population. Women veterans are more susceptible to common mental health issues (Hendrikx et al., 2023).
These common mental health conditions among women veterans are exacerbated further by higher incidences of adverse childhood experiences, compared to male veterans (Baca et al., 2021). There is also a greater likelihood that women have experienced military sexual trauma (Barth et al., 2016; Kelly et al., 2014). Because the vast majority of military and veteran services are informed by research, much of the available support is tailored to the needs of veteran men with a one-size fits all approach. Hence carrying out research on alternative approaches to well-being support that have not garnered the research spotlight to date, opens up new and interesting possibilities for tackling common mental health problems.
The fear of being labeled with a mental illness is a key barrier to many veterans seeking help because of the real and perceived impact on their personal life and career. Mental health care has negative connotations and while serving personnel and veterans are likely to visit a primary health care setting, trauma exposure is often left undisclosed. Because underlying trauma prolongs many common comorbidities among primary care patients, many of these conditions are difficult to treat without the provision of treatments for these conditions that are trauma-informed (TI; Bergman et al., 2019). This raises important questions about the need for closer integration of primary care providers and mental health care services. TI care (TIC) practices are a step forward in that integration process and diminish some of the stigma associated with receiving mental health support (Schreiber & McEnany, 2015).
TIC is a person-centered approach to recovery and empowerment strategies (Sweeney et al., 2018). TIC offers bespoke delivery models based on the individual's circumstances, gender, and type of trauma (Kelly et al., 2014). TIC clinicians look to identify the trauma symptoms in the individual while recognizing the role that trauma has played in their lived experience. TIC systems steer away from cultures of care that might lead to retraumatization with a focus on promoting healing (Purkey et al., 2018) Previous trauma of the veterans is pivotal in avoiding conventional delivery of in-patient psychiatric treatment services as these could retraumatize and lead to violent and harmful behaviors. Despite the tailored nature of TIC interventions, there are a number of commonalities in the approach (Knight, 2019). These include an awareness of trauma and an appreciation that mental and physical symptoms are manifestations of or adaptations to trauma. Secondly, TIC recognizes the importance of the therapeutic alliance in building emotional safety to fill the vacuum where past violations and abuses have eroded trust and confidence. Thirdly, TIC facilitates personal capacity building and promotes agency in making decisions and choices to engender a sense of control over their life. Finally, veterans are supported in identifying their strengths as part of the foundation for recovery (Goodman et al., 2016).
PTSD is a common mental health issue among veterans and TIC interventions have the strongest clinical evidence for reducing PTSD and improving well-being (National Center for PTSD, n.d.). However, Possemato et al. (2021) argue that despite the ostensible efficacy of TIC approaches, these treatments remain underutilized with veteran communities for several reasons. Clinical barriers to the implementation of TIC strategies include concerns about techniques that may increase patient distress. Clinicians have also expressed concerns about the rigidity of some techniques and a lack of time and training to deliver TI psychotherapy within clinic times (Cook et al., 2017). Equally, clinicians have reservations about the time and resources needed to build rapport with patients before therapy can begin, and that TIC may not be a good fit for clients with underlying comorbid conditions such as substance addictions and depression. For trauma-exposed individuals, the barriers to take up TIC are multifarious. These include concerns that TIC may exacerbate PTSD symptoms. Treatment systems are often overburdened and follow-up appointments are sporadic (Currier et al., 2017). Finally, a lack of trust in the therapy rationale is exacerbated by providers’ overwhelming caseloads, which limit the opportunities to build trust and convey safety (Doran et al., 2019; Herzog et al., 2020). Based on this catalog of doubts and shortcomings, and combined with the stigma of being labeled with a mental health condition, it is no surprise that veteran engagement or readiness to engage in TI psychotherapy is often muted.
Mind Force Retreat
The Mind Force Retreat is the brainchild of a former paratrooper and Iraq and Afghanistan veteran. Currently serving as a reservist, the founder became a passionate advocate for holistic alternative mental health therapies having been introduced to the idea during a Mediterranean holiday. The retreat involves a 3- or 4-day residential stay in a purposely-selected hotel in a semirural or rural location. The therapies include, but are not limited to, sound baths, yoga, Tai Chi, equine-assisted interventions (EAIs), reiki, and more generally mindfulness-based stress reduction techniques. A critical feature of the efficacy of these nonclinical approaches is the support network of the veteran community. The Mind Force Retreat founder recognized the potential transferability of these holistic interventions for military veterans grappling with the stress and distress of what they have seen and done, and where more traditional trauma-focused psychological therapies (TFPT) and pharmacotherapy strategies have fallen short for this particular needs group.
Mindfulness-based stress reduction techniques, for example, can provide a viable alternative to clinical interventions where appropriate. However, they can also be used in tandem with psychotherapy and pharmacotherapy. Recent research has highlighted that at least one in six U.S. military personnel deployed to Afghanistan and Iraq have PTSD. Around one in three of these former military personnel will develop PTSD at some point in their life (National Center for PTSD, n.d.). PTSD is a mental disorder associated with significant health problems including higher rates of morbidity and physical impairment. This may or may not include other serious debilitating comorbidities, which have serious disruptive implications for the veteran and their families such as substance misuse, interpersonal violence, traumatic brain injury, and suicidal tendencies (Hall et al., 2014).
There is no specific timeline for the manifestation of these health disorders but they often coincide with phases of extreme and intense stress such as proximity to combat zones but also a detachment from active service. To indicate the numerical scale of the issue and focusing on the U.S. alone, it is estimated that there are 18 million veterans and over 2 million active reservists. Nearly 4 million U.S. military personnel who are now veterans have served in the U.S. Armed Forces since September 2001 (US Census Bureau, 2020). Shifting the focus to the United Kingdom, nearly 2 million people in England and Wales stated in 2021 that they had served in the U.K. armed forces as either a regular or a reservist (Office for National Statistics, 2023). In total, one in 25 people aged 16 years and above in England and Wales stated that they were a veteran of the U.K. armed forces. A recent research study conducted on a sizeable military cohort reports significantly worse mental health outcomes for U.K. personnel previously deployed in combat roles to Iraq and Afghanistan. Stevelink et al. (2018) highlight a rising prevalence of PTSD (6.2%), 21.9% prevalence of common mental disorders and a 10% incidence of alcohol misuse. They also caution vigilance of the data during, and post, active service. This is significant because rates of postcombat mental health problems in reserve forces are consistently high across all the U.K. studies (Hotopf et al., 2006). Data for 2019 compiled by the U.S. Department of Veteran Affairs tragically reveals that the adjusted suicide rate for veterans was 52.3% greater than for the nonveteran U.S. adult population. In 2017, the rate difference between the veterans and the nonveteran U.S. population stood at 66.3% (U.S. Department of Veteran Affairs, 2021).
Barriers to Seeking and Getting Help
Serving military personnel and veterans can face unique risks and challenges in dealing with their mental health and seeking support. Albertson (2019) emphasizes the transitional challenges faced by veterans which may include health-related problems, substance misuse, and contact with the criminal justice system (also see Albertson et al., 2017). Iversen et al. (2011) point to the enduring nature of anticipated stigma linked to declaring a mental health problem as an important barrier to help-seeking. This stigma persists despite recent efforts within the military and civilian society more generally to destigmatize mental disorders by bringing mental health issues to the forefront via public health campaigns (Adler et al., 2009; CAMHS, n.d.; Miller, 2013). Veterans also reported additional barriers associated with where to seek support. These challenges to seeking help are intensified for those with PTSD. Barriers are compounded further by personal feelings of worthiness. If an individual has not served in a combat role, veterans have reported feeling an internal sense of imposter syndrome, that their access to support and therapeutic interventions is undeserved and illegitimate. These feelings in turn can heighten existing anxieties and depression (Feenstra et al., 2020).
Depression and various mental disorders can exhibit themselves through various symptoms, which combine to the detriment of an individual's ability to function effectively. While symptoms such as fatigue, low mood, loss of appetite, weight loss and gain, decreased ability to concentrate, sleep difficulties, a sense of reduced self-worth, and suicidal behavior are well-known to medical practitioners, the manifestation and intensity of such symptoms vary markedly between individuals. Consequently, diagnosis of major depression can often be very difficult and complex and may lead to misdiagnosis and inappropriate treatments. Inoue et al. (2022) argue that the scale of misdiagnosis could be as high as one in two patients and this represents a significant practical and clinical barrier for individuals accessing care.
Taboos around the PTSD label also pose a challenge to individuals actively seeking help. Previous research with military veterans has highlighted the feeling among some participants that the condition is fabricated and made up and hence has little clinical substance or credibility (Thomson, 2021). Hence presenting oneself at clinical practice and suggesting PTSD as a possible diagnosis or given PTSD, as a clinical diagnosis may be fraught with concerns around believability, perceptions of weakness, and legitimacy of the condition (Greden et al., 2010).
There is a significant body of literature on the risk factors for developing conditions such as PTSD (Brewin et al., 2000). Pretrauma risk factors for PTSD have been identified in different population groups. Women are at a higher risk for PTSD than men. For the most traumatic events, women showed a greater risk of developing PTSD than men (Sareen, 2014). Similarly, gender differences between male and female veterans accessing care have been observed. Women generally access care and support quicker and make more use of care services. Women also experience additional risk factors for PTSD such as childhood abuse and interpersonal violence. For men, a significant barrier to accessing services is traditional masculine beliefs exacerbated by military culture. Traditional constructions of hegemonic masculinities in the military emphasize toughness, aggression, violence, and emotion suppression. These pervading narratives can then shape male attitudes toward accessing care. Militarized hypermasculine ideals can disrupt help-seeking both during active service but also postmilitary service as a veteran (Banwell, 2014; Silvestrini & Chen, 2023). For women, a lack of understanding of the role of women in modern combat situations can potentially reduce help-seeking in women veterans, as their experiences can be dismissed as less traumatic and deserving compared to their male counterparts (Bergman et al., 2019; Dodds & Kiernan, 2019).
Subjective Well-being
In this study, subjective well-being (SWB), sometimes referred to as life satisfaction or personal happiness, is an individually defined perspective on satisfaction with one's life and social relationships (McCabe et al., 2010). The long-running debate about what constitutes well-being dates back to ancient Greece. During this time, narrow definitions of well-being focused on hedonism (feelings and evaluation of one's situation). These ideas were criticized for being oversimplistic and dismissive of the eudemonic or subjective aspects of well-being linked to autonomy and making personal choices (European Social Survey, n.d.). This paper adopts both a eudemonic and hedonic perspective that highlights mental well-being along different domains of daily life. SWB is tied up with “social-psychological prosperity” (Diener et al., 2010, p. 144) and the notion that the individual is functioning well in their view and has the capability and potential to make choices for their own self-development (European Social Survey, n.d.).
Objective measures of financial well-being have an important part to play in SWB more generally but this needs to be part of a multifaceted outlook that examines physical and mental health, having a purpose in life, and social relationships. This study focuses the lens on the mental well-being aspects of SWB for military veterans and blue-lights first responders. We examine domains of everyday life that capture participants’ perceptions of self-confidence, feelings of usefulness, level of energy, and capacity to deal with problems (Vento et al., 2020). There is a need for interventions that tackle manifestations of poor mental well-being because lower perceptions of well-being generally correlate with an increased risk of depression and anxiety, PTSD, and the need for therapy (McCabe & Johnson, 2013).
From TIC Approaches to Healing-Centered Approaches
The concept of TI practices and building TI resilient communities has inundated the vocabulary of a diverse range of stakeholders including social service providers and criminal justice agencies in the last decade or so (Knight, 2019). Along with it, frameworks, guides, and policies for organizations, systems, and services have developed equally as rapidly (Champine et al., 2022). TI care refers generally to a set of principles and strategies on how we view the impact of severe harm on a social group's mental, emotional, and physical health. Consequently, a TI care strategy is a strengths-based approach, which seeks to understand and respond to the impact of trauma on people's lives (Knight, 2019). In so doing, emphasis is given to the physical, emotional, and psychological safety of the individual while also empowering the individuals to reestablish control over their lives. TI practice champions support for the whole person rather than simply the symptoms or impacts of the trauma. For example, a TI approach would offer counseling and therapy to support an individual's well-being because the harmful behaviors that they may exhibit are rooted in more deep-seated harms.
Some critics have raised concerns about the effectiveness of a TI approach to embrace well-being and move beyond the pathology of trauma. A TI care approach has certain benefits, such as avoiding retraumatization but these outcomes only recognize the impact of trauma on mental, physical, and emotional health and have shortcomings in acknowledging the collective view of trauma (Maleku et al., 2022). Treating the symptoms and reducing the trauma do not automatically constitute a return to normal or high levels of SWB. A healing-centered (HCE) approach builds upon the TI approach in a number of key ways (Ginwright, 2015). HCE approaches cast a spotlight on the root causes of trauma and what might be done to tackle the environmental factors that created the trauma in the first place. An HCE approach shifts the emphasis away from probing the trauma-exposed individual's deficits and shortcomings and asks a more positive set of questions around the agency and assets an individual has to drive and sustain their SWB (Maleku et al., 2022). In sum, an important part of healing from trauma is one's realization of the actions that created the trauma originally.
With this knowledge in mind, trauma-exposed individuals can then move forward to examine what they would like to achieve (goal setting) rather than simply treating the psychological and behavioral symptoms of their trauma (Ginwright, 2015). An HCE approach recognizes the well-being restorative influences of community and identity. Healing is best experienced collectively within a community-focused setting and pathways to healing are enhanced by a sense of shared belonging and experience. For military veterans, an overarching military identity (Kleykamp et al., 2021; Kümmel, 2018; Markowitz et al., 2023) is a key factor, though notions of a singular military identity are mediated by intersectional factors such as gender and race. Finally, an HCE approach sees healing as a dynamic process through the life course. It should also build empathy among the trauma-exposed individual's family, friends, and kinship networks to limit the pervasive nature of trauma. Underpinning this, trauma survivors, sometimes referred to as “wounded healers” (Corburn et al. 2021) and their organizations should have a key role to play in a veteran-centered holistic therapy and recovery agenda-setting. Veterans are best placed to answer the key questions, what works? For whom? And in what circumstances? (Champine et al., 2022; Sweeney & Taggart, 2018).
Ethics
Both procedural and practical ethical considerations were adopted for this study. Institutional ethics approval was obtained through the university's research ethics committee whose principles are closely aligned with those of the British Society of Criminology (BSC, n.d.). Retreaters were informed of the purposes of this study using a participant information sheet that provided more details about the project. Consent was implied and obtained when participants clicked through to the online surveys and checked a box at the start of the survey form. The option to withdraw consent to participate was available throughout via contacting the researchers with the unique answers to three questions provided within the survey (favorite color, holiday destination, and food). This would enable the researchers to identify the relevant survey forms and exclude them from the sample.
The online survey was designed so that no personal identifying information was sought, though participants could add information freely in open-ended text boxes. The stewardship of the data (raw and analyzed) were only accessible to the researchers and stored in a secure manner within the online survey database. Given the potential for emotional and psychological triggering through the survey subject matter, details of support agencies were provided within the participant information document. The researchers’ email addresses were also listed to allow participants to ask further questions about the study.
Methods
Using the JISC Online Surveys tool (JISC Online Surveys, n.d.), a series of semistructured questionnaires were designed to evaluate the impact of the Mind Force Retreat on SWB while also capturing insights into the program's potential for promoting healing and recovery. A “before” and “after” methodology was adopted whereby retreat participants were invited to take part in the study at the start of the retreat. On arrival at the retreat venue, participants were invited to complete a survey (the arrival survey) which asked about their SWB at that moment in time. A survey conducted at this point may detect what has been termed the hedonic effect, which is the anticipation, excitement, and boost to SWB from a favorable event (Gilbert & Abdullah, 2002). Another survey invite (end of retreat survey) was distributed to retreaters at the end of their stay. Finally, a third survey invite was sent to the same retreaters between 4 and 6 weeks after the retreat had finished. The objective was to assess the impact longevity of the retreat on SWB (de Bloom et al., 2009; Kühnel & Sonnentag, 2010). In total, nine participants completed the arrival survey, 11 completed the end-of-retreat survey, and six participants took part in the 4–6 weeks postretreat survey.
Data Analysis
The semistructured survey approach gathered both quantitative and qualitative data. The arrival, end of retreat, and postretreat surveys captured participants’ SWB at that moment in time and utilized the internationally validated psychometric Warwick Edinburgh Mental Well-being Scale (WEMWBS) to establish quantitative baseline measures on a series of well-being domains. These areas include scores on a scale of one to five about the extent to which the participant has been feeling relaxed, feeling good about themselves, feeling relaxed, and feeling cheerful (Stewart-Brown & Janmohamed, 2008; Warwick Medical School, 2021). These baseline surveys then allowed the participants “distance-traveled” to be assessed using the postretreat survey several weeks later. Descriptive statistics were generated to provide an overall picture of the participants’ sentiments and feelings about SWB.
WEMWBS is designed for self-completion and to create a mental well-being score when the scores for the 14-item scale are summed. The scoring range for each item ranges from one to five and the total score ranges from 14 to 70. For example, a score of one is attached to the “all of the time” responses to each question while a score of five is attached to the “none of the time” responses to each of the questions on the itemized scale. Particular score thresholds are indicative of possible depression and probable clinical depression. WEMWBS strongly recommends that studies employing the mental well-being scale include at least thirty people with data collected at two-time episodes. This Mind Force Retreat pilot study does not meet the threshold sample size for the original design use of WEMWBS. Instead, we have used the 14-item scale to develop a broader set of understandings and emerging patterns around the mental and SWB of the participants using a “before retreat” and “after retreat” data collection methodology. We have also collapsed together some of the scale responses in light of the sample size. So for example, the response “all of the time” has been combined with “often” to produce a new aggregated response of “often or all of the time.” The respective data for these two responses has been summed.
The qualitative data were analyzed using a grounded theory approach to develop common themes derived from the lived experience of the participants. The open-ended questions included perceptions of a sense of community during the retreat, and participants’ perspectives on how they felt they had benefitted from the retreat (Charmaz & Thornberg, 2021; Glaser & Strauss, 2017). The data provided uncovers layers of personal feelings, memories, and stories. Most participants shared very similar accounts related to the positive feeling they had of being among like-minded people, and been able to share stories that were relatable. This sense of camaraderie, sometimes referred to as fictive kinship, promoted a community-centered pathway to healing and improved well-being through a sense of shared identity whilst also providing a bridge to new relationships and friendships beyond the retreat experience. A second theme centered on the personally transformative nature of the retreat experience. Finally, a third theme, focused on the capacity of the retreat to instill new skills and ways of coping with life's daily challenges. The results section, which follows, summarizes the key quantitative findings from the study participants using the adapted WEMWBS. It will then proceed to highlight thematically in qualitative terms the participants’ gains from the retreat experience.
Results and Discussion
Participant Well-being Scales
The WEMWBS data presented in Figure 1 summarizes the study participants’ perceptions of their well-being prior to the retreat. The chart clearly shows a dearth of responses that indicate “often or all of the time” to the scale questions. The most positive responses are tantamount to good mental and SWB and only feature in eight out of the 14 scale questions. The “often or all of the time” response is most prevalent in “I’ve been interested in new things” where 44.4% of participants expressed this feeling. In all other instances where “often or all of the time” features, it constitutes a much smaller fraction of participants’ responses. The mean percentage response associated with the “often or all of the time” response across the 14 scale questions is just 11.9%. In sum, Figure 1 illustrates that “rarely or none of the time” and “some of the time” respectively are the predominant responses by the study participants, which by proxy is indicative of lower levels of mental well-being prior to the retreat.
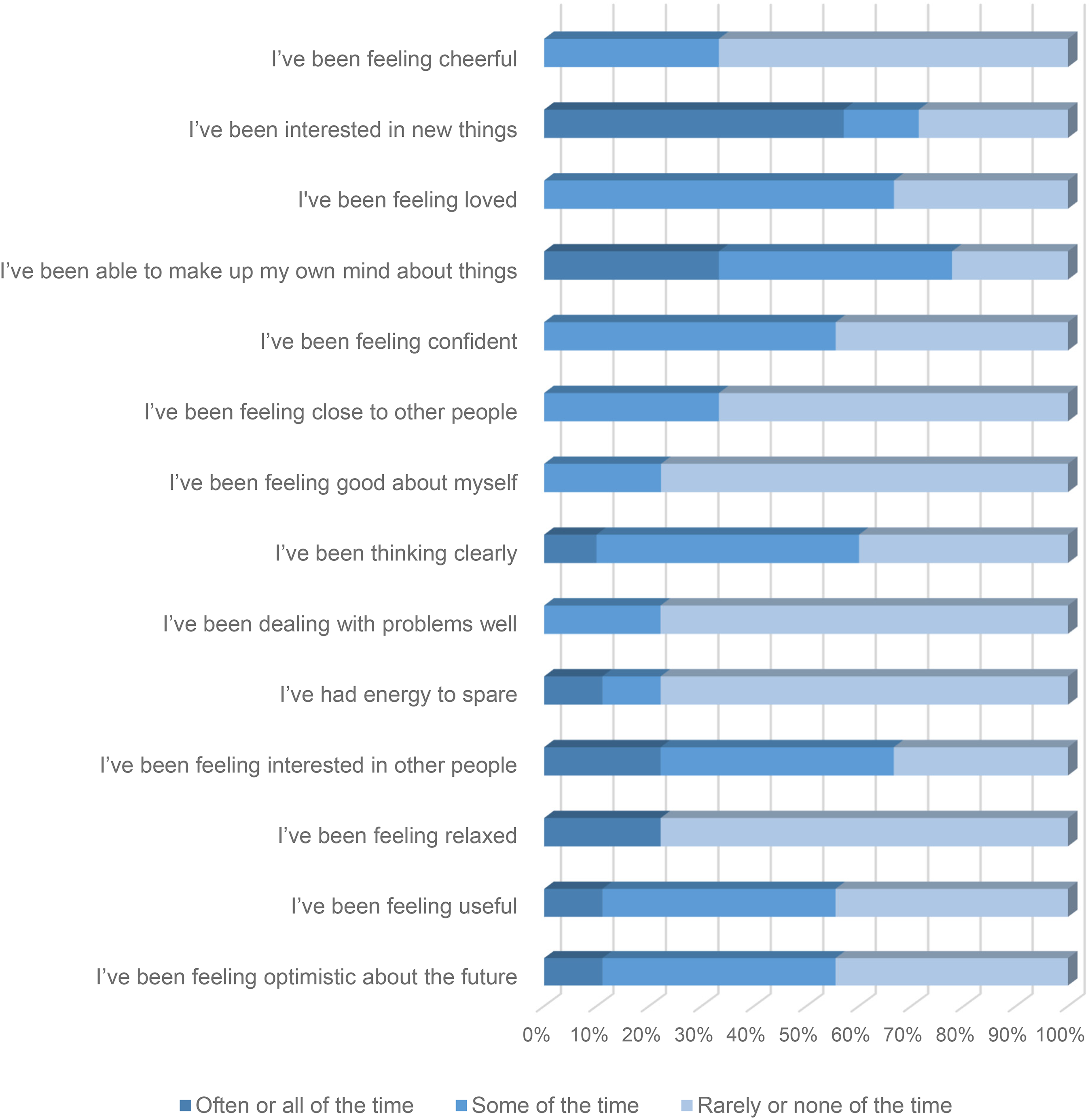
Participants’ WEMWBS before the start of the retreat.
Figure 2 summarizes responses to the 14 scale questions directly at the end of the retreat experience. This chart clearly shows the “distance-traveled” by the participants and demonstrates the impact of a “community-based” residential holistic therapies retreat. Whereas in Figure 1, the proportion of responses related to “often or all of the time” is subdued, a sharp contrast is observed in Figure 2 where the most positive of assessments dominates the scale question responses. For each question, “often or all of the time” achieves between 56.5% and 90.9% of all responses which represents a remarkable turnaround when compared with Figure 1. The mean percentage response associated with the “often or all of the time” across all fourteen scale questions is 74.8% which provides a simple but effective quantitative measure of the uptick in mental and SWB compared to before the retreat.
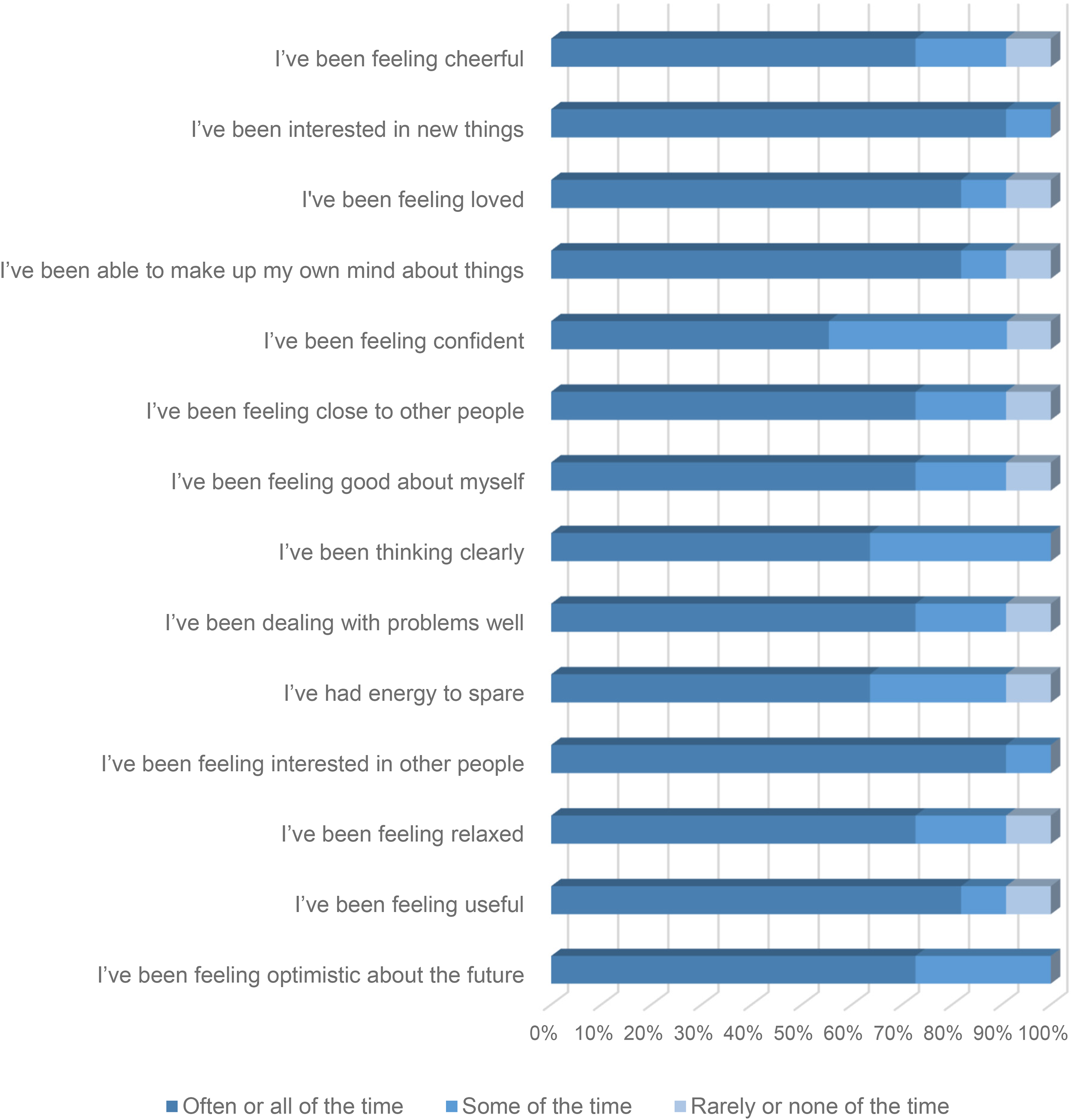
Participants’ WEMWBS before the end of the retreat.
The concept of “fade-out” assumes the existence of an effect on well-being. De Bloom et al. (2009) suggest that the waning of a vacation effect (fade-out) takes place between 2- and 4-weeks postvacation. Vacation is an important form of macro-recovery and consolidated time away from day-to-day routines and can enhance psycho-physiological health and well-being. Figure 3 summarizes participant responses for the period 4- to 6-weeks after the conclusion of the retreat to analyze the “fade-out” effect (Kühnel & Sonnentag, 2010). It is immediately apparent that the proportion of participants providing “often or all of the time” responses is still a significant feature of this chart across the 14-scale questions. The fade-out phenomenon is nowhere near as acute as discussed in some previous research studies (see e.g., de Bloom et al., 2009; Fritz & Sonnentag, 2006). Retreat participants appear to be maintaining similar good levels of mental well-being when compared to directly after the retreat ended. For each question “often or all of the time” achieves between 50% and 100% of all responses. The mean percentage of responses associated with the “often or all of the time” response across all fourteen scale questions shows only a small drop-off at 72.6%.
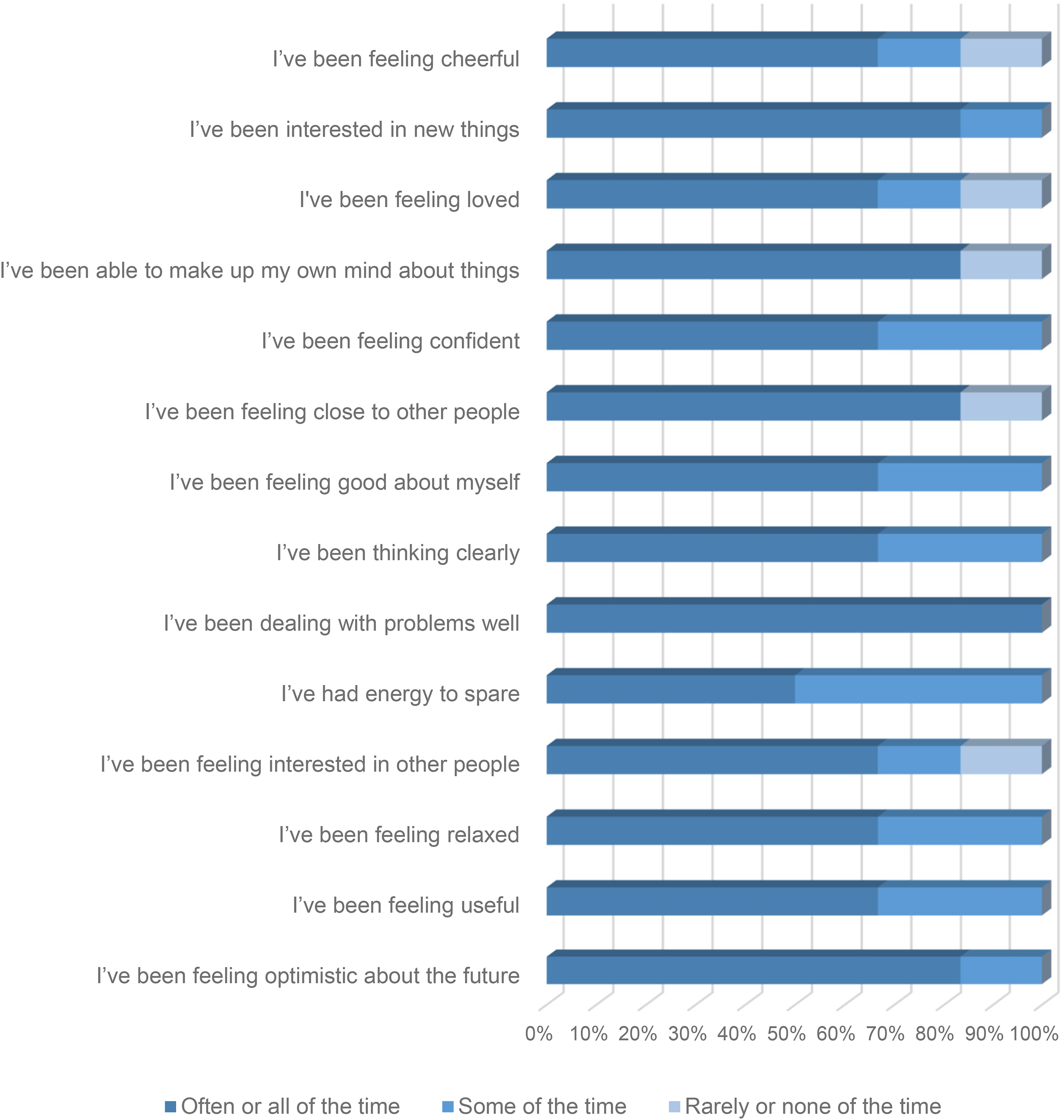
Participants' WEMWBS 4–6 weeks after the retreat.
Possible reasons for this maintenance of well-being levels over the short term might relate to the retreat activities and the potential for participants to practice and continue to enjoy the benefits of this postretreat. The activities included sound baths, yoga, Tai Chi, equine therapy, reiki, and mindfulness-based stress reduction techniques. Some of these activities have low barriers to entry. Mindfulness and yoga, for example, can easily transfer to other environments. If a participant has felt a personal benefit from engaging with these therapies during the course of the retreat, they can become part of regular home routines assisted by readily accessible YouTube videos and smartphone applications (Clarke & Draper, 2020). I really enjoyed and found benefit from all the pre-planned activities having taken positives from each one. I would recommend the yoga and sound bath activities. I found it very beneficial going through different breathing techniques and relaxation methods. (Retreat Participant)
Guided meditation and the lady who took it was exceptionally good, but all the activities were beneficial in some way be it from just allowing a moment of calm and peace to helping improve positive thinking, all were delivered in a way that made them accessible and refreshingly plain spoken. (Retreat Participant)
Moreover, the level of satisfaction with the retreat experience itself might also play a role in reducing the fade-out effect. All the participants engaged in the preplanned activities to some degree. In light of their complete experience on the retreat, participants were asked to rate their experience and whether, on a scale of 1–10 (where one is the lowest score and ten is the highest score), they would recommend it to a friend. All the participants positively affirmed the experience and gave a score of at least nine to this question. On the questionnaire conducted at the end of the retreat, all participants stated that they had personally benefited from the experience.
Healing Through a Sense of Camaraderie
In recent years, there has been increasing concern about identifying protective factors against extreme stress for those engaged in active service. The legacy of the Iraq and Afghanistan conflicts and the significant levels of poor mental health among former serving military has heightened the need to investigate predeployment vulnerabilities as well as protective factors during deployment that may affect PTSD development (Wright et al., 2013). Similar importance should be attached to the role of interpersonal support factors in postactive service scenarios. This study highlights the significance of like-minded support communities in posttraumatic contexts and the impact this can have on SWB protective factors. One of the most difficult parts of the transition from military to civilian life is losing camaraderie. Camaraderie is a cornerstone of military service and emblematic of cohesion, secure belongingness, and attachment to a military identity and culture (Albertson, 2019). The loss of camaraderie can equate to a significant emotional injury for some (Parry & Thumim, 2016). The residential retreat enabled participants to momentarily, at least, rediscover a semblance of this lost comradeship and “spend time with people who just get it” as one participant succinctly stated. Being able to share experiences that other communities would not understand and able to share stories of other colleagues gave you an almost instant bond. (Retreat Participant) The retreat not only provided respite from all the factors and stressors that cause stress and have a negative impact on my mental health but allowed me to be amongst others that have a bond and shared camaraderie that has not been a part of my life for so long like a missing piece of myself. (Retreat Participant) Was amazing to meet likeminded people who after 3 days I consider to be friends. (Retreat Participant) Before we left we all swapped numbers and plan to keep in touch. We also all had a cuddle which was lovely (and not usually like me). (Retreat Participant)
A Transformational Retreat Experience
As discussed earlier, an HCE approach to recovery does not shy away from the root causes of trauma and the environmental factors that created the trauma in the first place. Participants regaled each other with old stories from their days of active service. Talking, listening, and sharing builds trust, and reaffirmed a collective understanding and sense of community among the retreaters. I felt connected and really energized from being around beautiful, interesting people. (Retreat Participant)
I feel like it's been transformational. I feel like a different person. More open, confident and accepting. (Retreat Participant)
An HCE approach moves beyond a deficit model of the individual and instead seeks to cultivate the green shoots of human agency and resources that an individual possesses and graft these with the right support to recover SWB. Pharmacotherapy and TFPT as more traditional biomedical expert-dominated approaches might be building blocks of an SWB recovery plan for some individuals (Bajor et al., 2022). However, the Mind Force Retreat with its emphasis on a humanistic and holistic approach to improving well-being shows itself to have been a significant antigen for positive change too. Having not been away from my home suffering with ill health, the retreat broke the cycle. (Retreat Participant)
It [the retreat] has helped me to understand my emotions better and how to create a more positive mind-set for myself. (Retreat Participant)
Developing New Therapeutic Skills
The retreat involved a residential stay supported by a program of holistic therapies designed by military veterans for military veterans. These activities included sound baths, yoga, Tai Chi, equine-assisted therapy, reiki, and mindfulness. A study by Jain et al. (2023) provides convincing evidence for clinically significant reductions in anxiety levels and improvement in mental health from sound healing. Reiki is a hands-on healing therapy in which the practitioner channels universal energy to enhance and ignite vitality and promote the body's innate ability to heal. Reiki is an effective approach to decrease levels of pain, depression, and anxiety (Doğan, 2018).
EAIs within the Mind Force Retreat do not involve riding but do include grooming, feeding, and interacting with horses. EIAs can foster mutual friendships with the horse through synchronized interplay. They can also help retreaters to become active participants in their own healing and recovery process, as they engage in activities such as tending, grooming, and learning, which reinforces self-confidence, boost self-esteem, and lowers levels of anxiety and everyday stress (see, e.g., Jormfeldt & Carlsson, 2018; Punzo et al., 2022). They all created a different feeling and gave me the opportunity to explore what worked best for me. (Retreat Participant)
Holistic interventions such as sound baths, EIAs, and reiki present a series of different challenges for transference to the home environment. Conversely activities such as mindfulness which involves rhythmic breathing and meditative exercises to evoke a relaxation response, yoga which focuses on physical posture and controlled breathing, and Tai Chi reduces stress levels, improves balance, and increases leg muscle strength and general mobility and flexibility. These activities have low barriers to entry and can be easily practiced at home as part of a personal well-being plan. I know that when times are difficult I have tools to use that have worked in the past. For example meditation, yoga, and self-care and I can reach out to others. (Retreat Participant)
All the participants responding to the third survey undertaken 4–6 weeks after the retreat concluded that they had been incorporating skills taught during the retreat to improve their ability to cope with psychosocial stressors and to reduce cognitive distortions. I have certainly walked away refreshed, reenergized with a lot of new tools techniques, skills and ideas to help me on the my future path and journeys … having not attended this retreat I honestly don’t think that I would have ever looked at these types of remedies/treatments/techniques. (Retreat Participant)
I know how to wind down and stop overthinking, which used to lead me to becoming more stressed and leading to my depression. (Retreat Participant)
The tools and techniques that were shown to me I still use every day to help ground myself and find peace ….(Retreat Participant)
Study Limitations
The data consist of nine participants who completed the arrival survey, 11 who completed the end-of-retreat survey, but only six participants who took part in the 4–6 weeks postretreat survey. The attrition rate between the end of retreat survey and the final survey raises some unanswered questions about the welfare of the five participants who did not respond to Survey 3. Gathering additional data from subsequent retreat events would be a useful addition to developing knowledge and would enable analyses of patterns of persistence and change across cohorts.
An adapted interpretation of the WEMWBS was undertaken because the number of study participants did not reach the recommended WEMWBS threshold of thirty. Building the pool of data from other retreat participants would allow the desired threshold to be surpassed and a more purist interpretation of the Warwick-Edinburgh scale to be attempted. However, despite the number of participants in the current study, the retreaters provided rich answers that helped form the basis of the analysis.
Conclusions
The study has found that a program of holistic interventions delivered during a residential break can have tangible and long-lasting benefits for military veterans and their perceived mental well-being. Quantitative data from a survey conducted before the retreat, immediately after the retreat, and several weeks later, and validated by the WEMWBS 14-question scale testifies to the healing and recovery impact of the retreat. This quantitative data were bolstered further by the rich qualitative insights from the participants, which attest to their personal stories of improved SWB and positive change.
Initial skepticism of the therapy program and retreat idea dissipated when participants became aware that the program was designed by a veteran for the express purpose of other veterans. The combination of the bespoke nature of the event, shared understandings around military identities, and the assembled support network of the veteran community were cornerstones of the success of the retreat. In a participant's own words, the blend of the interventions ensured that “…people will find something that works for them if not all therapies.” However, just as importantly from a legacy perspective “…they [the therapies] each have their own benefits and gave me the confidence to try them away from the retreat setting” (Retreat Participant).
The development of TI practice to embrace an HCE approach involving holistic therapies, for example, is a positive progression on the strength of the findings from this study. This progression reflects the considerable progress made in recent years toward inculcating new treatment models and evaluating them. In turn, this is leading to significant advances in the treatment of PTSD in civilian and military populations. Holistic interventions that strive for better mental health for trauma-exposed individuals, such as military veterans, may not be suitable for all. However, where possible they should be offered universally as a credible and novel pathway to healing and improved mental well-being as an alternative, precursor, or concurrent adjunct to pharmacotherapy and TFPT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.