
Abstract
In this paper, we explore how existential aspects of being diagnosed and living with cancer are shared in stories that are publicly communicated online. Through a narrative analysis of online texts and blogs, we explore how people deal with their cancer experiences, how cultural norms about illness are expressed in their stories and why they write and publish their stories online. We found that the writers described cancer diagnosis as a defining moment in their lives. They portrayed it as a crisis that was followed by unpredictability, doubt, grief and loss, fitting with the term ‘existential uncertainty’. Writing and sharing their stories online, connecting with others and staying positive were ways of dealing with this uncertainty. These naturally occurring data offer insights into phenomena that are not easily accessed in a clinical setting; moreover, they provide unique insights into the cultural norms in which online illness narratives are embedded.
Introduction
Since the 1990s, particularly in the Western world, new communication technologies have enabled people to share their illness experiences publicly online. The internet creates a virtual space for social interaction among people to share, exchange ideas and debate experiences via verbal, textual and visual means. These spaces have now become widely used to share illness experiences such as cancer, as recovery work and as a place for enacting agency (Lian & Nettleton, 2015; Conrad et al., 2016; Stage, 2019). Over time, there has also been a shift in the social acceptance of cancer narratives; whereas people were discouraged from speaking about their cancer experiences at all in the 1970s (Jain, 2013; Sontag, 1978), many are now comfortable communicating their narratives, and first-person accounts of this serious illness are more commonly seen in research, literary texts and social media. Our interest lies in what stories they tell.
In the Western world, an increasing number of people survive after cancer treatment and the term ‘cancer survivorship’ is often used to describe the phenomenon. The term is internationally debated, as its definitions vary from the time of the onset of the disease until those defining a cancer survivor from 5 years after ending treatment (Marzorati et al., 2017). At the same time, the connotations and attitudes towards the term vary among those with cancer experiences, as some have never felt like dying (thus survival is misplaced) and others see the term as indicating that you are cured in every sense of the word (which is not the case). Also, with strong influences from the breast cancer campaign, called Pink Ribbon, in the United States, many western countries have developed cultural expectations of staying strong and optimistic both during cancer treatment and after. The images of millions of women happily running together in pink t-shirts have spread all over the world. Also, the imperatives to ‘make the best of the time you have’ and ‘never give up’ are highly influential and work well with the good intentions and in need of hope by family members and health care workers (Ehrenreich, 2001; Willig, 2011). Over the years, the debate has further explored whether the strong presence of breast cancer in the media has created such an influence that it can be called a ‘breast-cancer-isation’, narrowing the possibility of voices from other cancer types and creating an expectation that all cancer experience should be dealt with the same way: with positivity and heroism (Bell, 2014). Other voices suggest that there is increasing openness to more diverging narratives (Stordahl, 2015).
Previous research on people's personal experiences in their post-cancer years has shown that most people struggle to go on with their lives as they had lived them before the diagnosis (Fauske et al., 2020; Deimling et al., 2017). The transformative effects a cancer diagnosis has on an individual's identity, sense of being and meaning of life have been acknowledged; as Carel (2019) described it, ‘one's being in the world is altered’ (p. 91). Contributions to the existential aspects of living with cancer have shown us the impact cancer has on psycho-social health and rehabilitation (Hvidt, 2015; Vehling & Kissane, 2018). Existential uncertainty we consider in line with Adamson (1997) as ‘those uncertainties associated with biographical disruption, changes in self-concept, and adjustment to the cultural meanings attached to different diseases’ (p. 134). The cancer experience is here considered a trauma; where the impact on the self is not only a physical injury but also an existential one ‘insofar as it can damage, distort or even destroy our sense of self and how we fit into the wider world’ (Thompson & Walsh 2010, p. 379). A few pioneer studies on online cancer communication have been performed that inform us about the nature of blogs and their usage during cancer experiences (McCosker & Darcy, 2013; Orgad, 2005; Stage, 2017). Still, many aspects of online communication are under-researched, and the current study contributes by analyzing people's personal online cancer stories when living with and beyond serious illness. Based on a narrative analysis of online texts from women and men with pelvic and colorectal cancer experiences, we explore how these writers describe existential aspects of living with illness, why they write and share their stories and how they are influenced by western cultural norms within cancer and illness.
Materials and Methods
Data Material
Data collection was performed between November 2019 and February 2020 and consisted of 31 online texts and blog posts from 23 women and 8 men (Table 1) with pelvic or colorectal cancer in Norway. The empirical material comprises personal blogs, guest blog posts and one-time personal stories published by cancer organizations. Our inclusion criteria were as follows: a) publicly available Norwegian blogs and texts, b) texts with a first-person perspective, c) writing by individuals with all types of pelvic or colorectal cancers and d) writers above age 18. All text was written in Norwegian and has been translated by the research team and proofread.
Writers’ Main Characteristics.
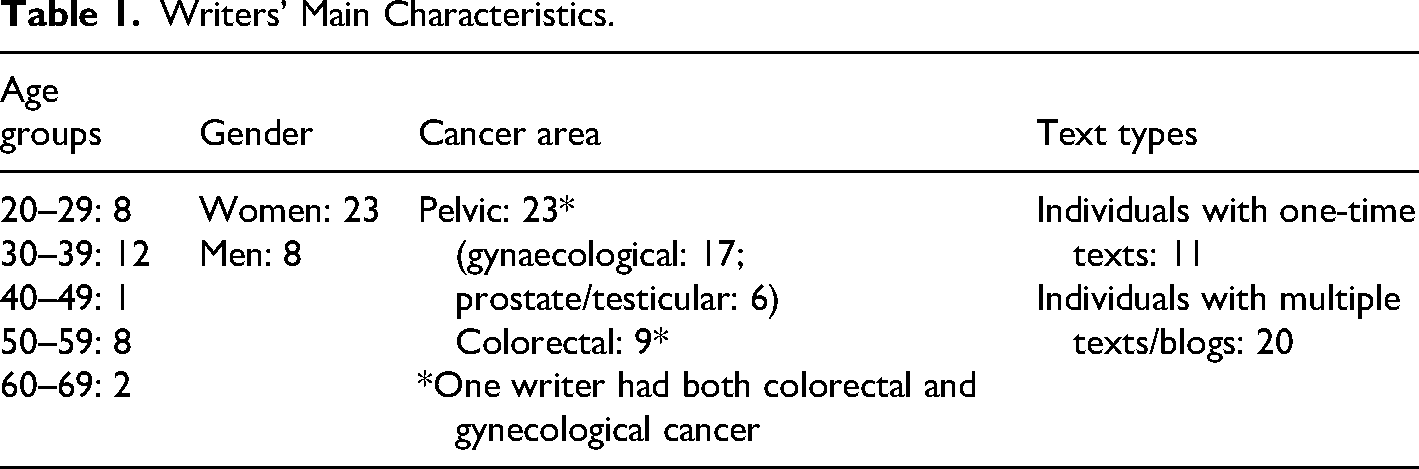
The cancer types were chosen because they included areas of the body that relate to taboos and receive less public attention, as people are often uncomfortable talking about the organs affected by these cancers (McCallum et al., 2012; Søreide & Bretthauer, 2007). Since there are no existing registries of such online texts in Norway, the material was obtained through strategic sampling, in which the first author searched for texts via cancer associations, newspaper articles, social media posts and specified terms on the web.
Blogs, or ‘weblogs’, appeared in the late 90s and are webpages that are frequently updated and have archived postings, usually in reverse chronological order. The posts are often discontinuous and episodic; they primarily contain text, but they may also include photos, links to other websites and comment functions. Researchers in digital media have discussed the nature of blogs and whether they can be considered diaries or as Lovink (2008) coined ‘public diaries’ due to the focus on communication (Lovink 2008, McCosker & Darcy, 2013). The writing style is often informal, autobiographical and written then and there, but there are style variations. The immediate and often unedited character of blogs influences the topics in the texts to a high degree, depending on the writer's daily mood, experience and state.
The material is considered naturalistic data; this implies that the researchers cannot shape what is found in the material, which does not always provide us with direct information. This means that characteristics (e.g. those in Table 1) are aggregated and often based on the information given throughout the texts. In this vein, since we lack information about the writers’ current phase in the illness trajectory, it is important to point out that they are understood as both ‘patients with cancer’ and ‘survivors of cancer’, including the points on the spectrum between these two concepts.
Analysis
The material was analyzed via immersion in the data, where each text was re-read several times within the context of the specific webpage or blog. The next step was to study the text line by line and code it as closely as possible to the subject of the line or paragraph. The codes consisted of descriptive words or sentences derived directly from the data. Since both what and how questions were important in this study, all data-driven codes were classified thematically concerning the content and form (the same paragraph could be coded under both). Although all text was coded, not every post was relevant to our study (e.g. political blog posts or descriptions of knitting recipes). These posts on other topics were coded as ‘Unrelated’—a code that was critically reviewed at the end of the analysis. We used NVivo software to accomplish the following: a) establish a systematic overview of relevant illness narrative texts included in the selection and b) look for patterns, variations and underlying assumptions, focusing on dominating themes and language. The themes were constructed by looking at what expressions and representations of living with illness the writers communicated and what the story was about, both directly and indirectly. All codes and interpretations were discussed within the interdisciplinary team to attain higher levels of trustworthiness.
Considering that the texts were created in a specific time and place, a narrative approach guided the analysis, intending to situate the writings in a wider context (Riessman, 2008). We emphasized ‘the recognition of illness narratives as speech acts, as performative, and as cultural phenomena that express socially shared resources’ (Atkinson, 2009, section. 3.1). In looking for influences on composition and choices of words in the texts, we sought the possible social and cultural norms and influences within this specific context. The context indirectly shapes how people should think and react; the texts are one representation of these cultural influences.
At the same time, we considered the stories to be actively created by the writers as a story written as they wanted them to be read by the assumed readers. The latter point is particularly relevant since the texts we looked at were consciously and openly shared online and sometimes explicitly responded to by their readers. The awareness of the ‘intended reader’ affects how the story is told, revealing the use of common scripts and compositions.
Ethics
The project was approved by the Norwegian Centre for Research Data (project no. 977764), and because the topic is considered sensitive by the European General Data Protection Regulation, a Data Protection Impact Assessment was conducted and approved (project no. 977764, date 22.10.2019). All writers quoted in this paper provided written informed consent to participate. Some writers published with neither contact information nor full name; to protect their privacy rights, we did not pursue a search for their identities, and their texts are not quoted.
Findings
In their texts, the online writers shared reflections on how the defining moment of the diagnosis had altered their being in the world. The most frequently recurring themes in our material related to the existential and uncertain aspects of living with and beyond the disease. The writers vividly described the immediate chaos and trauma of receiving the diagnosis and how uncertainty from that moment connected to all aspects of their lives—specifically, everyday tasks, interpretations of their body, social relations, their identity and the ‘new’ meaning of life. They expressed their uncertainties mainly with words like ‘hope’ and ‘fear’ (Table 2), which are related ways of expressing uncertainty (i.e. hope might go hand in hand with fearing that something will not happen).
Recurring Words (Direct and Indirect) Reflecting Uncertainty*.
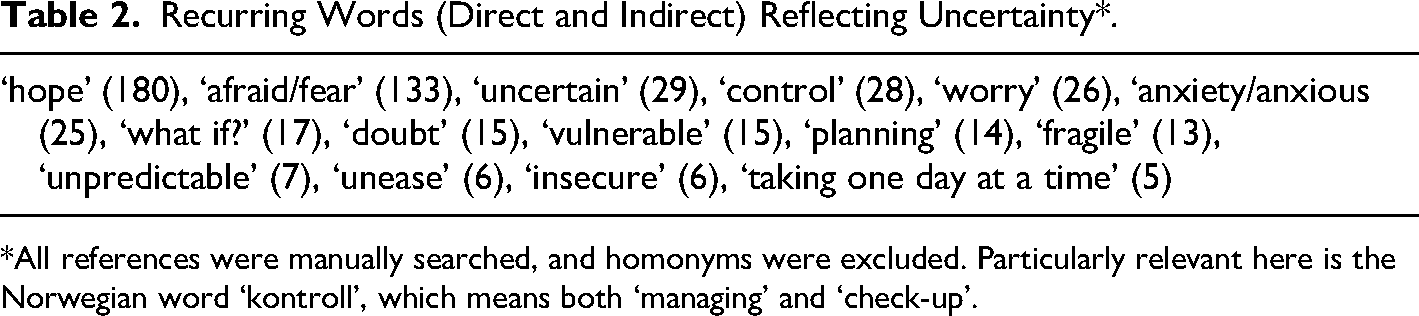
*All references were manually searched, and homonyms were excluded. Particularly relevant here is the Norwegian word ‘kontroll’, which means both ‘managing’ and ‘check-up’.
The writers’ expressions were defined as illustrating existential uncertainty; they involved themes connected to the meaning of life, the writer's identity and the writer's awareness of living as undetermined. In what follows, we present how they expressed their experiences of existential uncertainty, followed by ways of dealing with it and why they wrote about and shared their experiences online.
Experiencing Existential Uncertainty
The writers contemplated how life used to be, how it might become and what had been lost during the process, including control, the previous self, fertility and an ideal future self. In their writing, the writers expressed a general sense of insecurity, vulnerability, fragility, a lack of control and a lack of predictability, which all connected to a fundamental experience of existential uncertainty.
Fragility of life
A recurring theme across the texts was the defining moment of the diagnosis when the writers realized that life is fragile, a fundamental crisis when everything was categorized into a ‘before’ and an ‘after’. The writers described their illness as something that had made them aware of how rapidly and unexpectedly life can change, and they were conscious of this transformation. As one woman wrote: A few weeks after my 40th birthday, I had an appointment at [hospital name] for my 4-year check-up. Those two extremes really define my life. The future and hope that lies in celebrating another year and the uncertainty and helplessness that lies in a cancer check-up. Actually, it's a better description to say I’m 36 + 4 years old. The years after the disease feel like bonus years. There was something before, and it's something completely different after. (T13)
Thus, the writers depicted their life after as fragile, as opposed to the life before, when they took too much for granted. If they had known this earlier, they would have lived every moment to the fullest.
Other corresponding expressions included how life is ‘on hold’; writers expressed ‘standing on the sidelines’ or being ‘outside their previous life looking in’. Another recurring issue was how, after the onset of the disease, they were no longer in charge of their lives: I have gradually realized that this is out of my control right now anyway. The doctors can just drug me up and do what they have to, and then I’ll just have to take whatever comes after that… Taking one day at a time. One hour at a time. And allowing myself to be present in the moment—no matter how damn painful it must be. (T5)
This loss of predictability and control was particularly pertinent in the early stages of the disease. From the time of the diagnosis, the writers suddenly needed to let the medical personnel take over their schedule and their autonomy, leaving all routines and normalcy behind. Taking one day at a time, or not making plans, was sometimes written about as relief from thinking about the worst-case scenario—possible mortality or the recurrence of new rounds of treatment with unpredictable outcomes. This uncertainty made planning seem ‘uncomfortable’ or even ‘meaningless’ because everything the writers created could suddenly be lost. Some writers described how they attempted to regain control or rebuild their lives. When one woman's doctor approved of her planned move to another part of the country, she reacted as follows: Suddenly life did not feel like something we had completely lost control of but something we could influence again. Just like then, I get tears in my eyes now, when I think back. Not because it was as important to do as we had planned, but because we could. It felt like an enormous privilege to be able to choose again and make some plans for the fragile life we had been given. (T13)
Soon after, the enthusiasm evaporated, and she continued: I’m still not entirely comfortable making plans again. Plans feel like a privilege for healthy people, whereas we have to take life as it comes. It feels scary to make plans, knowing how incredibly quickly life can change, making all the plans completely worthless. (T13)
The motivation to re-create one's life was often described as being interrupted by fear or reluctance to let one's guard down and look towards the future.
Fear of recurrence
Commonly, writers expressed disbelief in their inner thoughts, their bodies and the information from doctors after treatment ended. During periods of check-ups and scans, they experienced worries, fears and amplified unpredictability of the future because they were reminded of previous bad news and treatments. They struggled to believe they were truly cured. One woman asked: Do I have a lump in my chest, does that mole have a weird shape, am I so tired because a tumour is growing in my brain? (T19).
In this passage, the writer expressed being filled with doubt after experiencing how even small symptoms can lead to a devastating diagnosis. The body as such, or her brain's interpretation of the body's communication, can no longer be trusted; therefore, it will always be second-guessed.
Many writers wrote actively in the period before and after check-ups, which seemed like a strained waiting game. One woman described anticipating an appointment for a positron emission tomography (PET) scan as follows: The fierce anxiety is washing over me. The pain that I must have displaced, but that is now so recognizable. Oh damn, that's what it felt like when I first got the diagnosis. I can't believe it was so hellish. (T13)
Although the results of check-ups could reduce uncertainty, the days of waiting for the results seemed to be a particularly stressful period: First, it's all about the waiting, twenty-eight days of mental self-distress—what if… (T20)
The commonly used words in this period were ‘angry’ or ‘irritated’, and the writers described how they often experienced symptoms while waiting for the results. Their writings during these periods also give the impression of a need to communicate their nervousness, anxiety, fear and worry. Even after positive follow-ups or scan results, they expressed that although they made it this time, they might not be so lucky in the future. In these periods, the fear of recurrence was amplified in their writing: The wait after the test is taken—I’ve become pretty good at persevering, but it's like living on borrowed time. I think about all the nice things that happen every day, like picking up my youngest daughter from kindergarten, like taking a hike in the mountains with a friend, like hearing how my eldest daughter is thriving in her theatre course and wondering if I will still be allowed to live this life next week. Or whether the test results will force us to undo everything. Again. (T13)
Despite being most affected during the check-ups, they worried that the periodic fear they experienced could endure: Mostly I have it under control; I push the experience away. Thinking it was so long ago that I have to move on. Thinking that many people are tired, tired of me talking about the disease, I’m healthy now (…) sometimes I’m taken by surprise. Then it all comes back. It feels physical, like a blow to the stomach. The crying comes, it wants out. The legs give way, the heart beating in my chest. It could be a song on the radio, which reminds me of the lady next to me in the hospital. (T19)
This woman depicted how, four years after treatment, she felt completely fine, but suddenly, everything would shift when, as she described it, her ‘body remembers’. Descriptions of smells, pictures and even colours were described by several writers as being triggers for previous memories, even those that had seemingly been forgotten.
The future self
After ending treatment, the writers expressed concerns about what life would be like for them as persons in the post-cancer stage. They questioned what they had lost, who they would become and what they would be capable of; for them, the illness required changes in all aspects of life. One woman dwelt on the unknown that she experienced every day immediately after treatment: And when you finally start to feel a little nimble, and can even eat, read and go to the bathroom on your own, and then get discharged from the hospital and sent home—then what? (T5)
A bit later, the enthusiasm for getting well and experiencing pleasant activities was still clouded by the fear of who she might become: I can't wait to get my everyday life back. But I’m scared, too. What if my body and my brain don't work? What if I can't work as much as I expect? Or manage to train as heavily and as much as I want? Or… Or… Or… (T5)
In addition to questioning their capabilities, the writers also considered external expectations when returning to everyday life. One woman stated: I felt like everything had changed now. When I was unsure how well I could work in full employment again, I had to assume that a potential employer would be too. (T13)
Writing about the present, they often described their energy levels and pain, along with preoccupations around their ability to perform duties and leisure activities. Work, family and social relationships were among the areas where they felt they constantly had to prioritize. They analyzed their capacities and worst-case scenarios, such as lying down in the middle of the road from exhaustion or knocking on a stranger's door to ask to use the bathroom.
When writing about the past, they depicted a longing to go back to life as it was and the simple things they looked forward to returning to: Seven months and I’m home. Enjoying the sound of the alarm clock every morning. Enjoying the feeling of wooden floors underfoot. Enjoying waking grumpy teens and preparing packed lunches they might throw away. (T19)
Those with children often mentioned daily routines as something they missed, but many wrote about experiencing nature or everyday activities, such as taking the tram and people-watching. One might say that they idealized the past and were continuously comparing their current life to the one they had before their illness.
Dealing with Uncertainty by Writing and Sharing
We consider how the writers expressed and responded to their life-altering experiences as ways of dealing with the uncertainty of their illness. By looking at their writing, we gain insight into what is culturally expected of them and the further function of writing and sharing that writing publicly.
Staying positive and using humour
From one day to another or sometimes within the same text, the writers alternated between expressing negative and positive thoughts. One frequent example is how, even in the darkest hours, they considered that their situations could have been much worse and looked for rays of light. In this context, ‘lucky’ was one of the most frequently used words in the material. The word ‘luck’ often appeared in the same paragraph as ‘gratitude’. Such phrases as ‘it could have been worse’, ‘there's always a way’ or ‘others are not so lucky’ recurred as important mantras. One woman expressed such a sentiment several times on her blog: I’ve learned to completely change focus, and words can't describe how grateful I am because I was one of the lucky ones who got my life back, as a gift. (T10)
Writers related being grateful and lucky to the fact that they had been diagnosed with a potentially curable type of cancer, that it was caught early or that they had received help from a specific doctor, hospital or the Norwegian health and welfare system. They also expressed gratitude for having a support system, most often family: My health is not quite what I’d wish, and every day is not amazing, but I am cancer-free, I am in good shape, I have the world's best family, wonderful friends and an exciting job. I wish everyone was just as lucky. (T13)
They often expressed optimism as an external obligation, starting the sentence with ‘I just have to’, followed by ‘think positive’, ‘look ahead’, ‘be strong’, ‘not give up’, ‘make the best of the situation’ or ‘accept the situation’. The intention is felt as an imperative; that they were obligated to think more positively: Time is the most valuable thing you have, so use it with your heart and live it with your happy glasses on. (T20)
The intention to stay positive was also evident when the writers sought to avoid being perceived as depressing or self-pitying. Some apologized for a sad text they had written earlier because they did not want to come across as whining too much. Even more commonly, when writers allowed a tirade of negative emotions to break out, they would end by turning the focus completely around—interrupting themselves, using the word ‘but’ and concluding with something positive. For example, one woman concluded her description of a terrible morning as follows: … And headaches. And chaos in my head because I’m wondering how to handle all this. Shit day! But there are some bright spots, of course: I sat a little in the sun this morning. Had a coffee visit from a good friend. Chatted with nice people. And soon a friend will bring me food. So… Life really isn't too bad!!! (T5)
Another strategy evident across the texts was the use of humour, particularly gallows humour. Writers described the function of humour as a way of having a break from the darker thoughts that loomed in their uncertain situation and as a way of neutralizing the insecure, sad state in which they—and those around them—often found themselves: I tell [husband's name] that I look forward to him finally really getting to know me. Like on the inside… of the intestines… We have a good laugh, which is much better than crying. (T20)
Humour and self-irony are underestimated medicine (…), and I disarm the scary stuff through humour. (T5)
Some used humour by writing lists with such titles as ‘The Benefits of Having (Had) Cancer’, in which they ironically described advantages granted by the illness, such as you always have an excuse for not attending a meeting or that people always say you look good (T20). A form of humorous ‘rating’ of the hospital facilities was used by several writers, assigning points for the food, décor, and service, as one would do in a review of a bed and breakfast. As examples of points that would increase the facilities’ ratings, writers noted: ‘I get dessert every day’ or ‘I have free access to drugs’. One woman prepared a list of funny stunts she could perform if the doctor delivered bad news, such as popping balloons in his face. Although this writer consciously used humour as stress and anxiety relief, she also chose to create laughter rather than be present and feel the dreadfulness of the potential life-changing moment.
Why write and share with the public?
Besides being part of dealing with their uncertainty, their motivations to write are particularly relevant to us, as their personal content is deliberately and openly shared online. The writers often explained directly or indirectly at some point in their texts why they were writing and sharing their experiences. While some argued that they did it for logging or archiving reasons, the writers’ motivations more often included some form of processing, connecting and being useful to others.
Several writers expressed how the act of writing helped them process their experiences and function as alleviating fear and anxiety: As I type, I look at the keyboard and screen as my therapist, and as my diary. (T3)
In fact, for me, being so open through the blog has helped me. I’ve been able to put things into words (…) I use blogging and humour as a kind of ‘survival strategy’ in what I am going through.” (T5)
They described the function of writing as something they would do to ‘sort things out’, ‘get stuff out of my system’ and process the shock of what they were going through. Thus, writing can be seen as a resource to help them make sense of their new, unfamiliar situation by taking the time to put their thoughts into writing: Nevertheless, there were some days when it was heavy. Once I’ve blogged, I’ve processed what's happened right then and there and kind of finished it. (T13)
Another dominant function of their writing was the aspect of sharing the writing—to connect with others and alleviate loneliness: I used to probably not be as good at putting into words everything I thought, and I kept most things inside me. But after I loosened up a little bit and started the blog, I see that I am not alone at all. A lot of people feel and think the way I do, a lot of people. It's unbelievable that I’ve walked around feeling so alone. (T10)
Many writers responded to feedback from their readers, expressing that they were thankful for ‘not being alone on the journey’: And yes, I also choose to be open about this because I need all the support and encouragement I can get. No one should go through this alone. At least I know I need you! So, thank you for being here <3. (T5)
This connection with others in similar situations relieved the feeling of being an outsider, unsafe or lonely with their illness at a time when even close family and friends seldom sufficed. This loss of belonging served as a strong motivator to reach out because the writers’ illness had placed them in unknown surroundings requiring new insights.
Most of the rationales for why the writers chose to be open about their experiences concerned a feeling of being useful to others. These findings show us how helping others could be felt as an imperative, as well as a way to ‘do something’ even when the writers were experiencing a lack of control and uncertainty in their own lives: I sat thinking that if I’m going to write about something as woeful as my cancer and something as taboo as sexuality, it's to make a difference for people in the same situation. (T6)
Knowing that their texts could ‘make a difference’, serving to help just one person follow the screening programme or become aware of their symptoms, gave them a sense of purpose in the face of their personal tragedy. Therefore, the idea of ‘being useful to others’ indicates that something valuable can come out of their dreadful experiences.
Discussion
The writers in our study all raised the kinds of fundamental and existential questions that emerge following the experience of a potentially fatal disease. From the defining moment—the instant they received the diagnosis that breached the course of their life—they are reminded of their finite lifespan and urged to raise existentially charged questions (Carel, 2019). The diagnosis entails both a crisis and a form of ‘disruption’ (Bury, 1982): since the new regime is out of their control, they put their life on hold and contemplate the fragility of life and the essence of their being. Thus, the onset of the disease requires new perspectives, as well as the need to take it ‘one day at a time’. Therefore, we might understand perceptions of uncertainty as ‘experiences of wondering, being insecure or worrying about something hypothetical that might or might not be or become’ (Lian et al., 2021). The writers describe the past as ‘normal’ or ‘safe’ indicating a secure state that they now crave. In the present, they experience periods of chaos and further doubt their abilities and who they have become. Their fear of recurrence—which causes them to constantly question physical symptoms and information from doctors—feeds their deep-seated existential uncertainty. They can never let their guards down. Uncertainty is most clearly represented when they write about the future because it is difficult to see how all they have lost of themselves might come back. As Thompson and Walsh (2010) describe the experience of trauma, individuals ‘find it difficult to maintain a coherent sense of identity in the present because so much of what they have taken for granted in the past has been made problematic and there is so much uncertainty and insecurity about the future’ (Thompson & Walsh 2010, p. 385).
The writers prompt us to reflect on the general meaning of such concepts as health, illness and disease, and particularly the notion of a ‘cancer survivor’. Their texts show that even when they are deemed cancer-free, the experience of loss of self, uncertainty and doubt continues. From the writers’ perspective, then, the border between cancer ‘patient’ and cancer ‘survivor’ is blurry if at all relevant. In addition, despite research indicating that the cancer culture in Western society is now more open to less glorified stories (Segal, 2012), this idea seems only partially accurate in our study because openness about personal challenges following bodily changes in the affected areas was notably absent from the texts. For instance, research has shown that sexual function after gynecological cancer is highly impaired, and affects individuals’ quality of life and way of being (Donovan et al., 2006). Still, the subject was hardly mentioned in our material, which can be interpreted as indicating that the physical and the sexual are still taboo or that the existential dimensions are experienced as more challenging than these aspects.
Cultural influences can be discerned in how the writers respond to uncertainty through forms of expression in the text. Highly relevant is the articulated importance of ‘staying positive’, being grateful and feeling lucky. We thus see similarities with cancer culture in English-speaking countries, where the norm of staying strong and optimistic—known as ‘positive thinking’—and influenced by the Pink Ribbon campaign in the United States (Ehrenreich, 2010; Wilkinson & Kitzinger, 2000). Positive thinking and the use of humour as a strategy both act as ways of coping for themselves and those around them. At the same time, they attempt to consider their readers by writing entertainingly and avoiding being too pessimistic or causing discomfort (Jurecic, 2012).
Our findings also suggest that the writers deal with uncertainty through the act of writing and sharing. Writing is ‘therapeutic’, and the writing function is seen as a way of reflecting on and making sense of the individuals’ illness experiences. In narrative theory, the construction of stories is considered a culturally acknowledged part of the healing process (Frank, 1995; Pennebaker & Seagal, 1999). In our material, writing could be a way of enacting agency, countering the helplessness of the writers’ everyday life and taking control over something—namely, their story. By publishing their stories online, they could also connect with an audience and share thoughts that might be useful for other people in similar situations. Communication with readers and statements of support seemed highly important for the writers. Online spaces may be a fruitful place to vent feelings and thoughts while feeling ‘connected’ to others in a time of crisis when a sense of belonging might be crucial (Thompson & Walsh 2010).
The primary strength of the study is its use of naturally occurring data with no researcher influence. One potential weakness lies in the unknown impact of the intended reader on the writers’ choice of wordings and content; we did not ask writers for clarification or discuss our interpretations of their words. Online writing may on the other hand provide an in-between distance from which to write personally and freely because it is less dependent on the immediate impressions and regulations of others (Markham, 2005). The gender disparity in the material and the fact that there may be people with certain characteristics who share their thoughts online might have affected the types of reflections that were gathered. Finally, because of the small sample size, we were not able to draw conclusions about patterns between individual characteristics; nevertheless, the sample's breadth in terms of age and types of cancers can be considered a strength.
Conclusion
In the online texts included in this study, the ephemerality, fragility, unpredictability and uncontrollability of life were recurring themes. The immediate crisis of the diagnosis and the writings after ending treatment both included descriptions of loss; of their previous and potential future selves. The writers were highly concerned with the existential aspects of how to live and what is considered meaningful in their new situation.
The analyzed texts appeared to have multiple functions. Most importantly, they seemed to function as a means through which the writers could make sense of their immediate crisis and later experiences and as a way of connecting with others and receiving support during a difficult time. Writing and sharing stories about cancer experiences emerged as ways of dealing with illness-related uncertainties. The texts also communicate ambiguous messages: on the one hand, they describe the low-spirited existential repercussions of the disease, and on the other, the intention to stay positive despite the illness. Thus, the texts are drawn between the existential dimensions of the writers’ lives and cultural expectations regarding how they should respond to these thoughts and experiences.
Our findings contribute to an improved understanding of how individuals experience the existential sides of cancer as a crisis and the life beyond, in this place and time. By analyzing online texts, we gained insight into how this experience is expressed—or not expressed—in our culture. Both should be considered further by people with cancer, those working in health care settings and research fields within social science and humanities.
Footnotes
Acknowledgments
The authors are grateful to all the writers for allowing their texts to be used in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Norges Forskningsråd, (grant number 283517).