
Abstract
Vaccination is without a doubt one of the most efficient ways to stop the COVID-19 pandemic from spreading. The goal of this study was to look into the acceptance and resistance to COVID-19 vaccination and its associated components using the Health Belief Model, which is a framework for changing health behaviours (HBM). The current study is quantitative; hence data was collected from attendants of patients admitted to hospitals in Pakistan's top-tier cities using a survey-based self-administered questionnaire. Nonprobability convenient sampling was utilised to approach the respondents. The model was tested in two stages using partial least squares (variance-based structural equation modelling). The measurement model's reliability and validity imply that the data is reliable and valid. Except for the impact of benefits on accepting behaviour, all of the study postulated relationships are supported by the results. The study agenda adds to our understanding of health care, immunisation, consumer behaviour, and behavioural research. It adds to the body of knowledge in the fields of immunisation and behavioural research by examining people's behaviours and changes during the worldwide mass vaccination period.
Keywords
Introduction
The need for immunization and vaccination is imperative to manage and control severe health issues such as COVID-19 (Dinleyici, Borrow, Safadi, van Damme, & Munoz, 2021; Yuen, Ye, Fung, Chan, & Jin, 2020). With the development of vaccination against the widespread of pandemic many facets of individuals behaviours prevailed. Predominantly in developing countries it was noted that individuals showed reluctance towards the immunization procedure (Roy, Biswas, Islam, & Azam, 2022; Van Oost et al., 2022). It is also matter of concern that in Pakistan people are resistant towards the booster doses of available vaccines. The resistance and acceptance behaviour towards vaccination is worthy to be studied in current times as current literature identified the need to study behaviour of individuals (Roshchina, Roshchin, & Rozhkova, 2021; Swendeman et al., 2022; Walsh, Comar, Folan, Williams, & Kola-Palmer, 2022). The stats shows that in Pakistan there is a dreadful need to conduct such studies in order to locate the cause of resistance behaviour (Chaudhry & Amis, 2022; de Figueiredo, Simas, & Larson, 2021; Shah, Faraz, Khan, & Waterfield, 2021).
The health belief model is one of the most often used models for predicting people behaviour, which can include both resistance and acceptance. The health belief model (Janz & Becker, 1984; Rosenstock, Strecher, & Becker, 1988) has been verified in research as a viable theoretical behavioural change model for assessing intentions to vaccinate against COVID-19 (Wong, Alias, Wong, Lee, & AbuBakar, 2020). However, because there is a bivariate relationship between intentions and beliefs, vaccination intentions can affect beliefs, cross-sectional studies that have been widely used in the literature do not allow a clear understanding of the effects of HBM behaviour both in terms of acceptance and resistance on vaccination intentions (Walker, Head, Owens, & Zimet, 2021). Experimental research designs therefore may provide a clearer picture to determine the factors that forces individuals either to accept or reject a certain pattern. According to the HBM, an individual chance of adopting a given health behaviour is driven by their belief in a personal risk of illness or disease, as well as their confidence in the efficacy of the suggested health behaviour (Jayanti & Burns, 1998; Prentice-Dunn & Rogers, 1986). Its components include perceived severity of COVID-19 and susceptibility to COVID-19, perceived advantages of and hurdles to receiving a COVID-19 vaccine, self-efficacy to overcome vaccination barriers, and cues to action to receive a COVID-19 vaccine (Huynh, Tran, Nguyen, & Pham, 2021a), as applied to COVID-19 and a future vaccine (Champion & Skinner, 2008; Huynh, Van Nguyen, et al., 2021b; Rosenstock, 1974).
This research aims to study an individual resistance and acceptance behaviour to get vaccinated as identified by World Health Organization (Organization, 2020). It incorporates HBM (Hochbaum, Rosenstock, & Kegels, 1952) to identify the motivators and triggers that can activate resistance and acceptance behaviour. It employs the HBM model to highlight the efforts of medical staff in promoting the intentions to accept the immunization process. It further adds up behavioural predictors of the HBM that encapsulates perceived threat appraisal, cost, and benefit appraisal, cues to action, and perceived self-efficacy. Hypotheses are based upon the association between the threat appraisal and cost and benefits appraisal with both the individuals’ resistance and acceptance behaviour of vaccination. This study would be very useful as it aims to fill the gap by identifying the positive and negative behaviours of individuals in the time of the global pandemic immunization process. The study of an individual behaviours towards the dire need to vaccinate is the need of time; therefore, the health belief model is a very effective model that sums up a lot of meaningful constructs to provide a complete picture of behaviour (Joorbonyan, Ghaffari, & Rakhshanderou, 2022; Suess, Maddock, Dogru, Mody, & Lee, 2022). The present study applied the health belief model to study the intention in favour and against getting vaccinated from COVID-19 using the health belief model predominantly in Pakistan.
Literature Review and Hypotheses Development
Health Belief Model
The Health Belief Model (HBM) is one of the extensively used model by the researcher to identify and understand the health behaviour of people (Hochbaum et al., 1952). It is aimed to predict the health related behviour of individuals in certain patterns of belief (Abraham & Sheeran, 2015). The health belief model presumes that the person is motivated to perform a certain behaviour in three forms, firstly, the individual perception, secondly the likelihood of action and thirdly, the modifying factor that leads to action (Aarts, Paulussen, & Schaalma, 1997; Yang, Wei, & Liu, 2022). Individual perceptions are elements that influence how people see sickness and how important health is to them, as well as their perceived susceptibility and severity (Commodari, La Rosa, & Coniglio, 2020). The perceived advantages minus the perceived barriers to adopting the suggested health measure equals the likelihood of action. According to the HBM, at least three factors influence the perception of a personal health behaviour threat: general health values, such as interest and concern about health; specific health beliefs about vulnerability to a pertinent health threat; and beliefs about the repercussions of the medical condition. The interaction of these elements results in a reaction that frequently emerges as an increase in the chance of that behaviour occurring (Rosenstock et al., 1988; Strecher & Rosenstock, 1997). In the current study the health belief model is adopted to investigate the response of individuals towards vaccine by testing both the resistance behaviour and the acceptance behaviour. It allow the researchers to compare and discuss the factors that leads to resistance and identify the accelerators of acceptance.
Perceived Benefits and Behaviour
The cost and benefits appraisal of the health belief model comprises of perceived benefits and perceived behaviour (Strecher & Rosenstock, 1997). The perceived benefits in the health belief model refers to the benefits that are associated with the adoption of the model behaviour (Walrave, Waeterloos, & Ponnet, 2020). In the current study the benefits are referred to the benefits attained through getting vaccinated or adopting the behaviour to get vaccinated timely. The current study investigated perceived benefits with the accelerators of individuals behaviour in both positive and negative forms, i.e., resistance behaviour and acceptance behaviour. Previously, it was noted by (Champion & Skinner, 2008) that perceived benefits are positively linked to behavioural intentions that drives behaviour. Furthermore, studies conducted to study the behaviour regarding breast cancer screening (Yarbrough & Braden, 2001), prevention and control of injuries occurring from extensive workout and various studies related immunization (Grinberg & Sela, 2021) and for waste management to avoid contagious diseases (Sandhu, 2014). The current study hypothesize that perceived benefits can be negatively related to resistance behaviour as resistance behaviour is the negative behaviour. Therefore, it is assumed that the benefits of vaccination against COVID-19 will negatively affect the resistance behaviour hence driving the acceptance behaviour.
Hypothesis 1a: Perceived Benefits has a significant negative relation with Resistance Behaviour
Hypothesis 1b: Perceived Benefits has a significant positive relation with Acceptance Behaviour
Perceived Barriers and Behaviour
Perceived barriers are defined as “a person estimation of the level of challenge of social, personal, environmental, and economic obstacles to a specified behaviour or their desired goal status on that behaviour” (Nkala, 2014). It is one of the most significant variables of the health belief model that along with perceived barriers sums in cost and benefits appraisal. Therefore, in terms of the health belief model perceived barriers are individuals’ opinion of the physical and psychological cost of the advised behaviour (Rosenstock, Strecher, & Becker, 1994). For studies conducted in the stream of vaccination and immunization it is determined that the barriers act as hurdles that forces individuals to abstain from a certain behaviour (Cover, 2016; Rosenstock et al., 1994). Priorly conducted studies regarding the vaccine intention indicate that perceived barriers play a vital role on the vaccine intention for both flu and COVID-19 vaccines (Huynh, Tran, et al., 2021a). It was also emphasized that medical professionals can help in reducing the barriers that can help in increasing the number of immunizers (Chaudhry & Amis, 2022). Medical professionals and other public health related groups could theoretically expand flu vaccine acceptance and further the COVID-19 vaccine acceptance via education and outreach centred on perceived barriers to the vaccine. Henceforth, we hypothesize that perceived barriers catalyse the resistance behaviour, but it inversely affects the acceptance behaviour.
Hypothesis 2a: Perceived Barriers has a significant positive relation with Resistance Behaviour
Hypothesis 2b: Perceived Barriers has a significant negative relation with Acceptance Behaviour
Perceived Severity and Behaviour
Perceived severity relates to an individual perception of the disease medical and social consequences, such as pain, missed workdays, and so on (Gift & Redford, 1992). Perceived obstacles refer to the unfavourable elements of becoming vaccinated that an individual perceives, such as costs, physical pain, psychological concerns, or a logistical lack of access (Eilers, Krabbe, & De Melker, 2014). Outright vaccine rejection was substantially related with a reduced perceived severity of COVID-19 if infected and the lack of a reported chronic disease in previous investigations, suggesting that vaccination complacency may drive anti-COVID-19 vaccination behaviour (Schwarzinger, Watson, Arwidson, Alla, & Luchini, 2021). Anti-COVID-19 vaccination behaviour was found to be highly linked to the following characteristics of subjects in studies: In the past, female gender, age with an inverted U-shaped connection, lower educational level, and less compliance with prescribed immunizations were all factors that contributed to poor vaccination compliance (Schwarzinger et al., 2021). In accordance with other studies on COVID-19 vaccination intentions, it is determined that perceived severity of the outcomes of coronavirus forces individuals to adopt acceptance behaviour. Therefore, we hypothesize that perceived severity has a negative association with resistance towards immunization and positive association with accepting the immunization process.
Hypothesis 3a: Perceived Severity has a significant negative relation with Resistance Behaviour
Hypothesis 3b: Perceived Severity has a significant positive relation with Acceptance Behaviour
Perceived Susceptibility and Behaviour
Perceived susceptibility is defined as the “belief about getting a disease or condition” (Emeafor, 2017). The most commonly cited concepts involved in the HBM include Perceived Susceptibility, Perceived Severity under one umbrella domain of Perceived Threat (Wilkinson, Strickling, Payne, Jensen, & West, 2016). In the context of the acceptance and resistance behaviour to vaccinate against COVID-19, perceived susceptibility refers to the individual perception regarding the chance of being infected by coronavirus (Costa, 2020; Venema & Pfattheicher, 2021). At one end the study studies the individuals that deny the vaccine and at the other end it undertakes the variables to determine the behaviour of individuals that accepts the vaccine. Likewise, a study conducted in the U.S. in 2021 found that perceived benefit of the vaccines and perceived susceptibility of infection to be significant predictors for vaccination acceptance (Al-Metwali, Al-Jumaili, Al-Alag, & Sorofman, 2021). Despite widespread recognition of the risk of coronavirus, a common theme in the literature is that of low perceived susceptibility to these risks in the context of immunization practice (de Figueiredo et al., 2021). There is evidence that some individuals are disinterested in vaccination, and they tend not to see themselves susceptible to the risks due to a lack of proximity and nonconcrete awareness about the usefulness of vaccination. Evidence from clinical experience of intolerance and resistance to the immunization process is already posing a serious risk to patients or causing problems in practice, rather than just being an abstract future threat, is particularly powerful in promoting a heightened sense of susceptibility.
Hypothesis 4a: Perceived Barriers has a significant negative relation with Resistance Behaviour
Hypothesis 4b: Perceived Barriers has a significant positive relation with Acceptance Behaviour
Cues to Action and Behaviour
Cues to action are another vitally important predictor that completes the behavioural change indicated in the original HBM, and they include the presence of internal or external incentives that aid to motivate vaccination, such as information from the media or advice from a doctor (Hochbaum et al., 1952; Huynh, Van Nguyen, et al., 2021). Cues to action are defined by researchers as “the stimulus needed to trigger the decision-making process to accept a recommended health action” (Meillier, Lund, & Kok, 1997). Findings of a study indicate that there were positive associations between behaviour and vaccination intentions including perceived benefits, cues to action, and a positive attitude (Wheldon, Daley, Buhi, Nyitray, & Giuliano, 2011). Existing literature also emphasises the impact of vaccination in response to the COVID-19 threat, which can be applied to future health education interventions that should focus on increased knowledge of COVID-19 via mass media messages and cues to action from healthcare workers’ recommendations to promote vaccine acceptance (Wong et al., 2020). Furthermore, the HBM shows that the Perceived Threat of the illness, Perceived Benefits, Barriers to Vaccination, and Cues to Action all influence people vaccination behaviour. Therefore, the current study presumes that cues to action are negatively related to the resistance behaviour and directly linked with the acceptance behaviour.
Hypothesis 5a: Cues to Action has a significant negative relation with Resistance Behaviour
Hypothesis 5b: Cues to Action has a significant positive relation with Acceptance Behaviour
Self-Efficacy and Behaviour
Self-efficacy refers to a person capacity to complete the vaccination procedure effectively (Mohr, Boudewyn, Likosky, Levine, & Goodkin, 2001). The self-efficacy questionnaire created to assess the application of the coronavirus vaccine is revised and supplemented in the HBM model to measure this variable. Self-efficacy refers to a person conviction in his or her ability to carry out the behaviours required to achieve specified goals (Bandura, 1977). Health behaviours increase when self-efficacy develops (Lee, Arthur, & Avis, 2008). Parents’ vaccination behavioural intention improved as their motivation and self-efficacy grew as a result of utilising a chatbot, according to previous research. Self-efficacy refers to a person belief in their capacity to manage their own motivation, behaviour, and social surroundings. (Fisher, Turner, & Morling, 2009) established the information–motivation–behavioral skills (IMB) model, which indicates that delivering adequate health behaviour information leads to higher motivation and enhanced self-efficacy, which can lead to improvements in health behaviours. These findings show that education, insurance, scoring high on subjective norms, having a positive attitude toward the vaccine, as well as high perceived susceptibility to COVID-19, high perceived benefits of the vaccine, high self-efficacy for getting the vaccine, and scoring low on barriers to the vaccine, are all significant predictors of COVID-19 vaccine uptake intentions. These connections are in line with the notion of health behaviour modification. According to the HBM, people who are most vulnerable to the health hazard, have rewards that outweigh the obstacles, and have the self-efficacy to overcome those barriers are the most likely to succeed (Champion & Skinner, 2008). In accordance with the priorly conducted studies the current study assumes that self-efficacy alters individuals’ behaviour positively and on the contrary.
Hypothesis 6a: Self-Efficacy has a significant negative relation with Resistance Behaviour
Hypothesis 6b: Self-Efficacy has a significant positive relation with Acceptance Behaviour
Theoretical Framework
The theoretical framework of the research is complete relies on the Health Belief Model to study the behaviour of individuals towards vaccine acceptance and resistance. Figure 1 demonstrate the model that is proposed and tested by the research, clearly highlighting the constructs, hypotheses, associations and HBM.
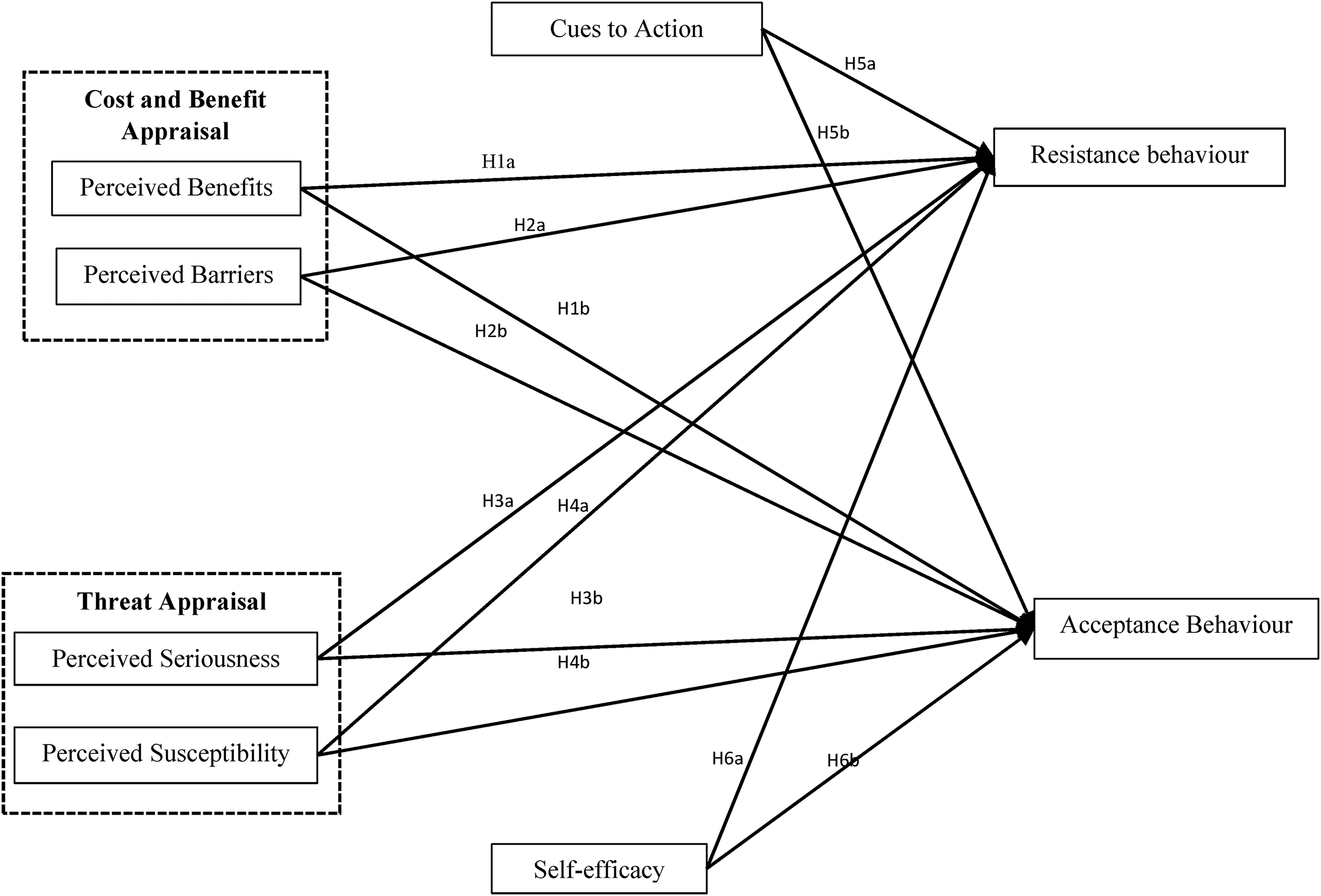
Theoretical Framework.
Research Methodology
The current study employed the descriptive research strategy to conduct the quantitative research, the deductive approach was applied based on the presumed propositions/hypotheses to deduce and interpret the results. Complying with the purpose of the study the research is cross-sectional as it relies upon the collection of data in a specified time. The data was gathered from a few hospitals located in the twin cities of Islamabad and Rawalpindi namely PIMS, Benazir Hospital, PAF hospital and Bahria international hospital. The current study focused on primary data that was collected from attendants and patients of the forementioned hospitals, as they were the direct observers of COVID-19 vaccination adoption among Pakistani patients and attendants. Survey method was adopted to collect data through convenient sampling. Moreover, the survey questionnaire consisted of two parts first section was based on demographic details and the second section comprised of variables related questions.
Measurement and Scales
The present study utilized a survey questionnaire to gather data to examine the validity and reliability of the proposed measurement model. The responses were collected on a 5-point Likert scale ranging from strongly disagree to strongly agree. The measurement items were derived from previously conducted studies, the measurement items for severity and susceptibility were adapted from (Buglar, White, & Robinson, 2010), the measurement items for cues to action, and self-efficacy were adopted from (Moriuchi & Chung, 2018). The questions for perceived barriers and perceived self-efficacy were taken from a study by (Buglar et al., 2010), while the items for resistance behaviour were taken by (Shapiro et al., 2018) and acceptance behaviour were taken from a study by (Lu, Hsu, & Lee, 2016). All of the scales have shown reliability and validity; thus, they were employed in this investigation.
Data Collection and Analysis
The data was gathered via a self-administered questionnaire that was separated into two sections: a measuring scale and a component based on the respondent demographic information. A total of 600 questionnaires were issued, however only 560 were completed, with 40 outliers being deleted. The level of agreement of responders with the statement was measured using a 5-point Likert scale ranging from strongly disagree to strongly agree. The information was gathered during a six-month period, beginning in June 2021 and ending in December 2021. As per the stats reports of Pakistan obtained from https://covidvax.live/location/pak
Missing values were considered as mean values after data collection, and data was converted accordingly by reviewing, cleaning, encoding, and modelling data to uncover important information, inform conclusions, and help the decision-making process (Henseler, Ringle, & Sarstedt, 2015; Henseler, Ringle, & Sinkovics, 2009). The behavioral outcomes were predicted using a partial least square (PLS) model (Hair et al., 2016). PLS (SEM-VB) was utilised to assess the model using variance-based structural equation modelling (Hair et al., 2014). The theoretical model and measurement model were both tested for validity.
Ethical Consideration
As genuine data was acquired from Pakistani universities, this study comprised of an examination of legitimate and credible data. The respondents were the patents and attendants of aforementioned hospitals, who were sampled in different wards and every response was recorded, so there is no issue of data tampering. The information is neither exaggerated nor exaggerated. There was no exaggeration or overestimation of values, and the findings of several research were discussed as well. The writers are given full credit for their work, and their ideas and thoughts are referred to by their names. The data was quantitatively examined in a fair manner, and the results were presented without bias.
Results and Hypotheses Testing
The following section entails the outcomes obtained from the data analysis procedure of the study.
Demographic Sample Characteristics
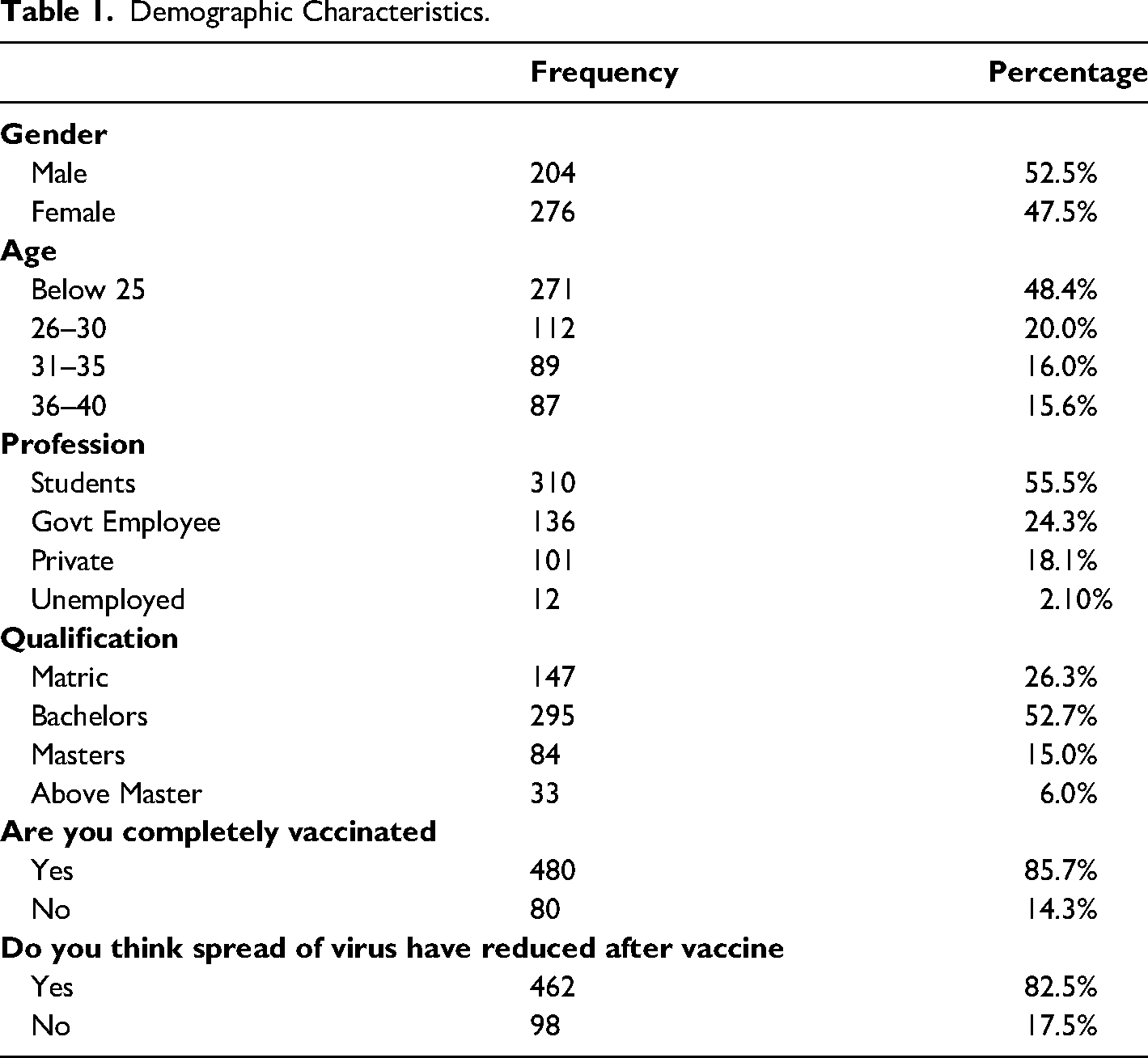
As stated above the survey questionnaire for the current study consisted of two parts, section number two was based on the demographic characteristics of the respondents. The questions asked in this part comprised of age, gender, qualification, professional status, and question relying on vaccination against corona virus pandemic. The results indicate that there were total of 304 male attendants of patients that contributed to 52.5% of the total sample of 560, while the female attendants consisted if 47.5% that i.e., 276 female participants. Similarly, the participants were split on age variations, the data composed of a greater number of individuals below the age of 25 years that included 48.4% with a frequency of 281. Secondly, the respondents included of 36.0% of participants who were between the ages of 26–30 and 31–35 years. It was also noted that the highest contribution was of the individuals below the age 25 and majority of them were students that was a total of 55.5%. The specification of vaccine related survey questions consisted of two questions i.e., we asked the respondents if they are fully vaccinated and secondly, we asked them what they think about the usage of vaccine that is does it prevents the spread of the virus. Where the data shows that majority agreed to the stance that getting vaccinated is a necessity to get rid of coronavirus. The results are illustrated in table no. 1.
Demographic Characteristics.
Measurement Model Assessment
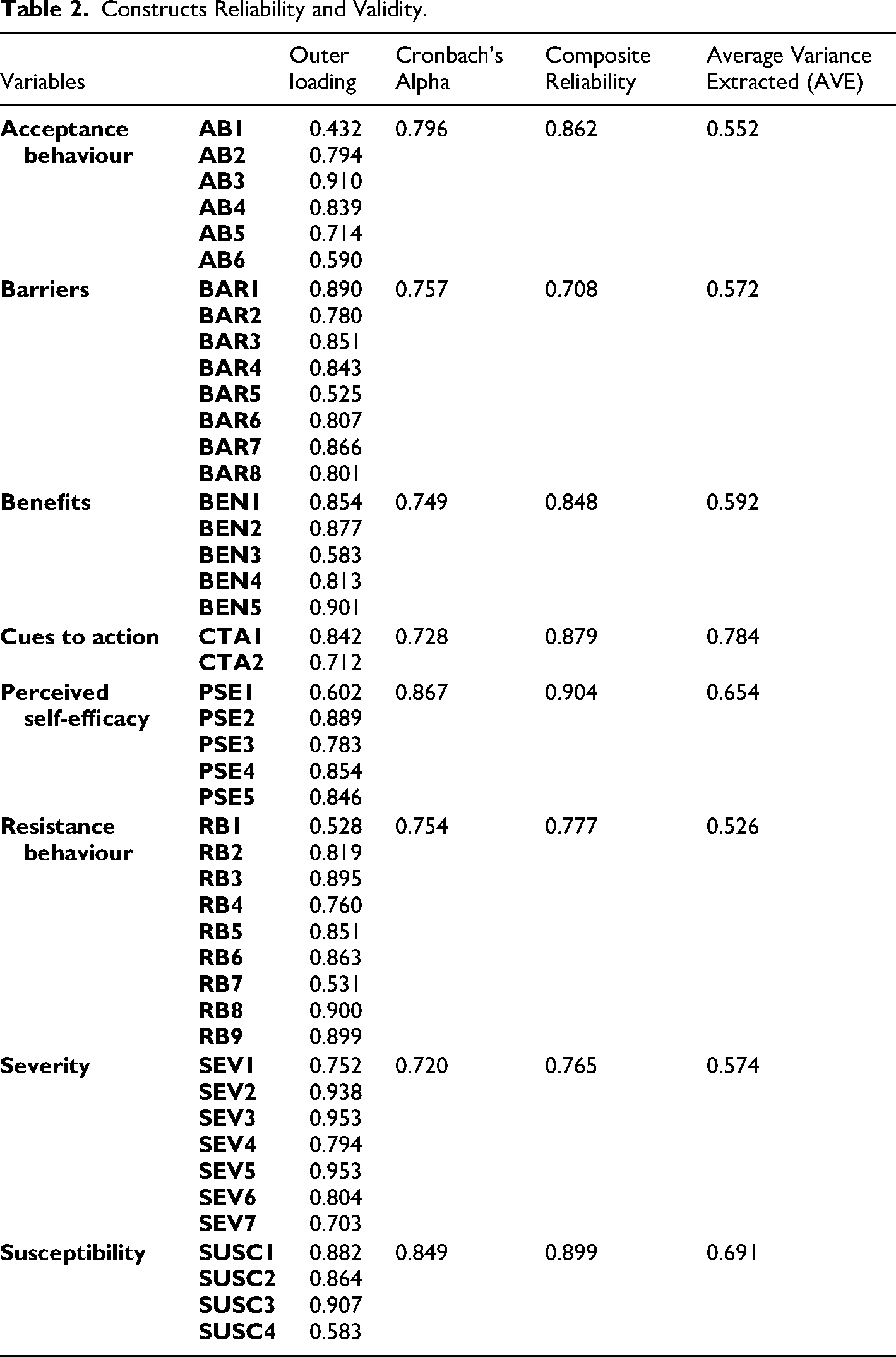
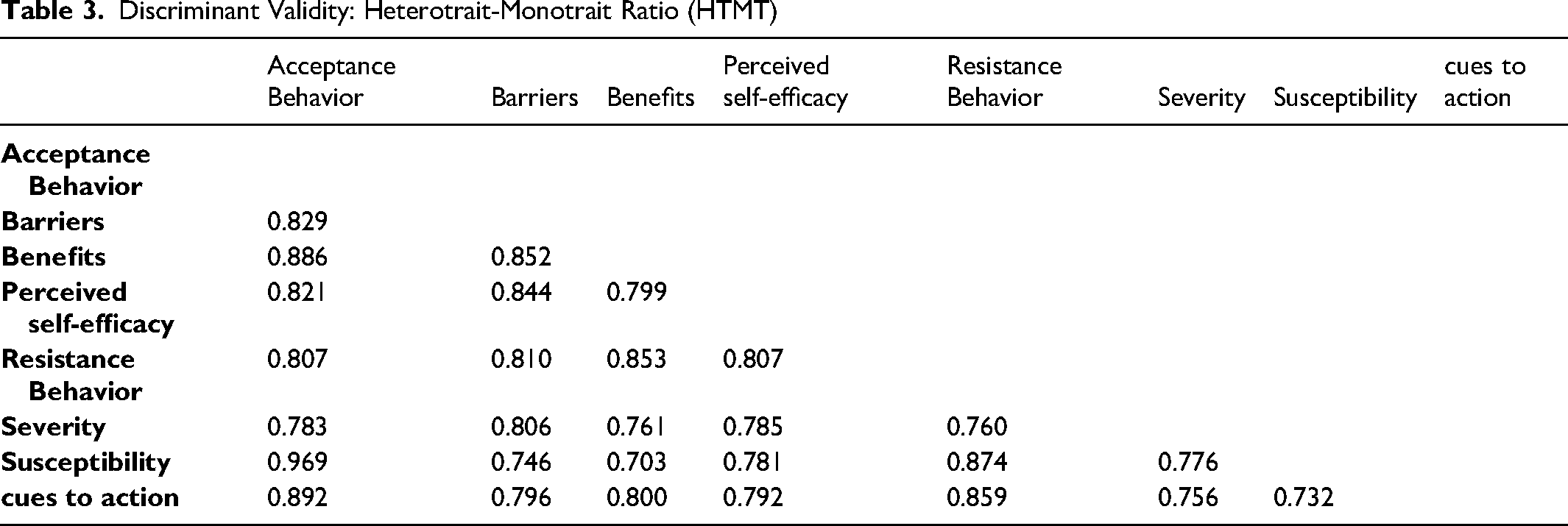
The model validity and reliability were verified using a measurement model. PLS (SEM) enables the measurement and structural model to be tested. Confirmatory factor analysis (CFA) was used to evaluate the measurement model, which examines the data’ reliability and validity using a variety of statistical methodologies such as composite reliability, Cronbach's alpha, Rho, average variance extracted, and factor loadings (Hair, Hollingsworth, Randolph, & Chong, 2017). The measuring model in Smart PLS 3.0 was used to examine the constructs’ validity and reliability, including both convergent and discriminate validity. In the measurement model that measures the type of association between predictor and outcome variable, path coefficients (beta values) were also investigated. The average variance extracted value was used to evaluate convergent validity, whereas the HTMT ratio, or hetero-trait mono-trait ratio, was used to measure discriminant validity. As shown in Tables 2 and 3, convergent and discriminant validity tests reveal that the data meets all of the relevant criteria.
Constructs Reliability and Validity.
Discriminant Validity: Heterotrait-Monotrait Ratio (HTMT)
Structural Model Assessment
The next stage in PLS-SEM is to evaluate the structural model after the measurement model has been evaluated satisfactorily. It assesses the influence and relationship between the constructs, i.e., the intensity and type of relationship that aids in hypothesis acceptance decision-making. Smart PLS 3.0 (Hair et al., 2017) was used to assess the structural model using a bootstrapping procedure with 5,000 resamples (Table 4).
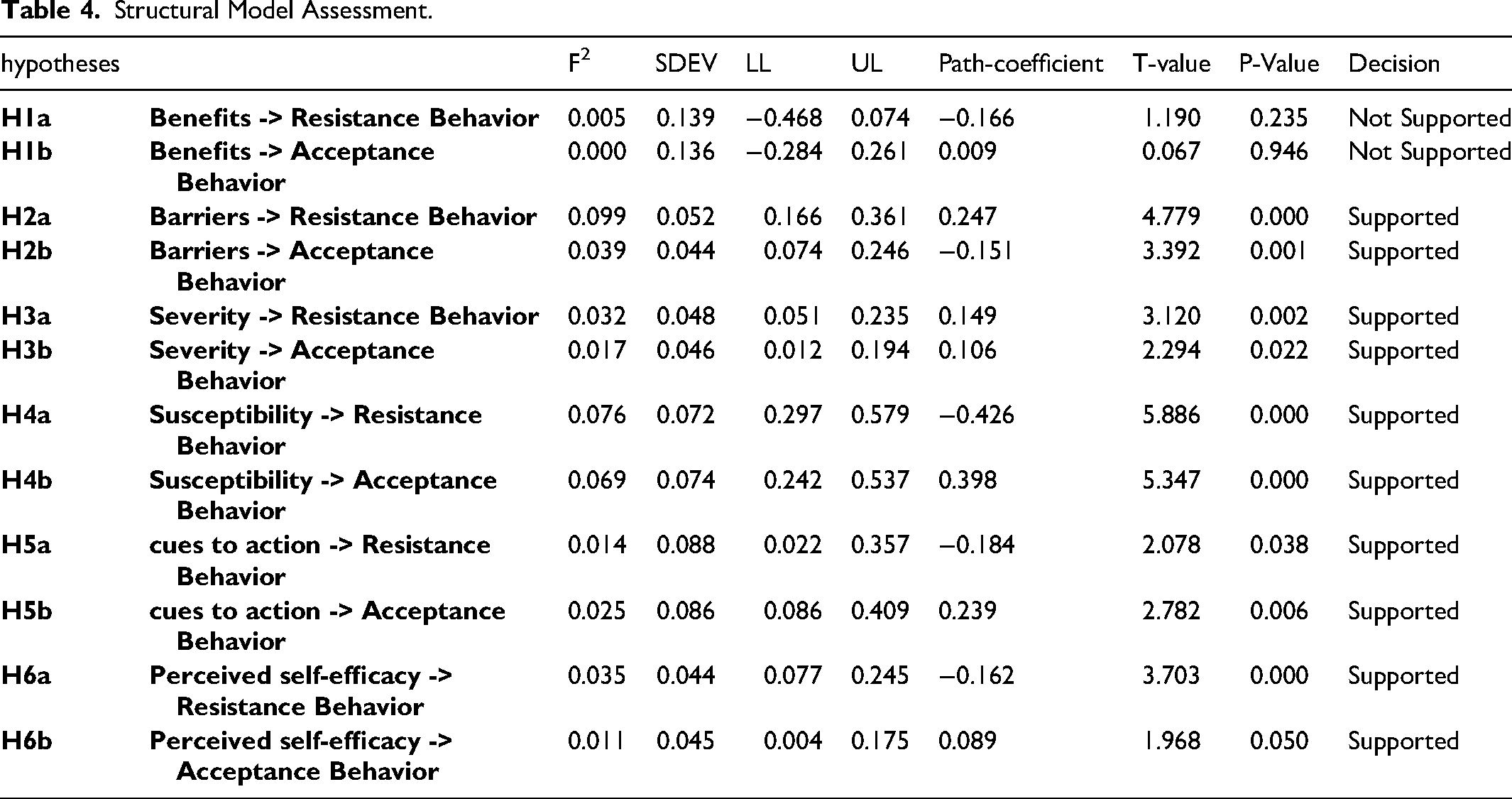
Structural Model Assessment.
Acceptance criterion for R2 values nearer to 1 imply a lesser effect size, while values near 0 indicate a weaker effect size (Henseler et al., 2009). The study findings demonstrate that the R2 value for resistance behaviour is 0.768, while the R2 value for acceptance behaviour is 0.779, indicating that the R2 acceptance criteria have been met. Table 5 displays the results.
R Square

Hypotheses Testing
The study developed six hypotheses that were divided on 2 parts a and b to study the relationship of predicting variables of Health belief model on the vaccine resistance and acceptance behaviour of individuals. There were two dependent variables and the main intend of the study was to derive a comparison based on individuals’ behaviour to identify the resistance and acceptance behaviour of people towards corona virus vaccines. Hypothesis 1a proposed that benefits are negatively and significantly related to resistance behaviour the results indicate that Hypothesis 1a is not supported as (β = -0.166, t = 1.190, p = .235), negative relation is developed but the relationship is not significant. Hypothesis 1b defined the positive relationship between benefits and acceptance behaviour, the results did not support H1b with (β = 0.009, t = 0.067, p = 0.946). Hypothesis 2a was supported as the outcomes indicated that there exists a significant positive association between perceived barriers and resistance behaviour (β = 0.247, t = 4.779, p = 0.000). The relationship of barriers with acceptance behaviour was also supported as (β = -0.151, t = 3.392, p = 0.001). Severity and resistance behaviour was proposed by 3a and the results indicated a significant negative relationship (β = -0.149, t = 3.120, p = 0.002). Parallel with the hypothesis 3b the outcomes derived a significantly positive correlation between severity and acceptance behaviour i.e., (β = 0.106, t = 2.294, p = 0.022). Consequently, hypothesis 4a was supported because the results indicate that there exists a significant indirect relationship between susceptibility and resistance behaviour (β = -0.426, t = 5.886, p = 0.000). Likewise, hypothesis H4b was also supported as, there occurred a significant positive correlation (β = 0.398, t = 5.347, p = 0.000). The results for H5a (β = -0.184, t = 2.078, p = 0.038) and H5b (β = 0.239, t = 2.782, p = 0.006) were also supported. Alongside the hypotheses for H6a (β = -0.162, t = 3.703, p = 0.000) and H6b (β = 0.089, t = 1.968, p = 0.050) were also supported as the results were parallel to the proposed hypotheses. The effect size was also calculated, and the results reveal a strong effect in almost all the relationships proposed as shown in table number 4.
Discussion
To present, authorities have mostly relied on hygienic standards and social distancing to combat the COVID-19 outbreak. People must, however, be willing to be vaccinated in order to create global immunity. According to our research, 88 percent of every 560 adults in Pakistan are fully vaccinated and they think that getting vaccinated is the only solution to contain the spread of COVID-19. The current study encapsulated the behavioural choices of attendants of patients that are admitted in different hospitals in Pakistan, in order to understand the vaccination behaviour of people that are already facing the vulnerable conditions related to health. We projected that predicting variables involved in the health belief model are related to the behaviour as per the extant theory, but we added two kinds of behaviours as dependent variables that is the vaccination acceptance behaviour and the resistance behaviour enabling us to study how each factor contributing to existing theory. We proposed that the cost and benefits appraisal (benefits and barriers) are significantly related to behavioural choices, such that barriers are directly related to resistance behaviour and benefits are directly related to acceptance behaviour. Our findings support our assumptions in terms of barriers but rejects it in terms of benefits. These results express that barrier accelerates the resistance behaviour and acts as friction towards the acceptance of vaccination. The results of this study are parallel to the priorly conducted studies that believed in negative impact of barriers on behaviour (Huynh, Tran, et al., 2021a; Streefland, Chowdhury, & Ramos-Jimenez, 1999; Suess et al., 2022). However, our propositions about benefits of vaccination that leads to acceptance behaviour were rejected due to the reason that people are not satisfied by the aftereffects of vaccination as it does not provide entirely negative COVID-19 results. This stance is also admitted by former researchers (Lockyer et al., 2021; Paul, Steptoe, & Fancourt, 2021; Qiao, Tam, & Li, 2020).
The sudden outbreak of COVID-19 pandemic, and the emergency situation created threat for the entire human race and people were bound to change their lifestyles and attitudes (Moreno et al., 2020). This condition led to the high need of vaccine that altogether help in containing the contagious virus. The threat appraisal of HBM is thus a very strong predictor of behaviour (Seyde, Taal, & Wiegman, 1990). The attendants of patients believed that severity of virus has led in accepting the vaccinating behaviour, on contrary the severity was inversely related to resistance behaviour towards the immunization. The findings are parallel to different studies highlighting the significance of severity of adverse medical condition (Dinleyici et al., 2021; Lockyer et al., 2021). According HBM susceptibility helps in believing that the virus can hit us anytime, also forced people to accept the vaccine, moreover this motivating force helped people to deny the resistance behaviour towards getting vaccinated. Multiple studies in past agrees to this relationship between susceptibility and behaviour (Smolders et al., 2010; Tarkang & Zotor, 2015).
Fitting in the HBM, we tested the cues to action and perceived self-efficacy in relation to both resistance behaviour and the acceptance behaviour. It is postulated that cues to action are a significant factor that helps people to adopt a certain behaviour (Schwarzer, 2008). Similar were our findings that indicated that cues to action are the forces that helped in accepting the Corona virus vaccine and avoid the resistance behaviour (Tarkang & Zotor, 2015; Yang et al., 2022). The outcomes of the study derived that perceived self-efficacy played a crucially significant role to create accept the COVID-19 vaccine (Chong et al., 2020; Wang et al., 2021). Yet forcing people to avoid the resistance behaviour, people confirmed that they are confident enough to get vaccinated and contain the virus. People have acknowledged their strength in making the transformation toward a sensible society, alongside the government efforts of the mass vaccination also helped in creating this level of confidence and trust on the government and immunization procedure.
Theoretical Contributions
The current research is considered an empirical extension of the current literature in the field of behavioural studies. The study purposefully used a very effective theory of Health Belief model to better understand how a society behaviour changes when an adverse medical condition such as COVID-19 strikes. The global pandemic has prompted a surge in research in a variety of sectors, including the epidemic behavioural aspects. The current study primarily assumes that the structural application of HBM will help to improve understanding of vaccination acceptance and resistance behaviour. It looked at how severity, susceptibility, efficacy, cues to action, benefits, obstacles, and behaviour affected severity, susceptibility, effectiveness, cues to action, benefits, barriers, and behaviour (both acceptance and resistance). The findings suggest that in the Pakistani setting, there are barriers to vaccination acceptability. Future studies in many circumstances may notice this feature of HBM. Furthermore, research will be performed to better understand the nature of various natural disasters and how people react to them. The work is theoretically significant since it identifies COVID-19 mass vaccination from a behavioural standpoint. This study emphasises the importance of behavioural changes, which will aid behavioural and medical research in raising knowledge about the need of vaccination and the reasons for vaccination refusal.
Practical Implications
The study has practical value in addition to its theoretical contribution. It emphasises the impact of COVID-19 immunisation on acceptance and resistance behaviour. As a result, the behaviour modifications that can be made to avoid contracting the virus are indicated. It also emphasises the necessity of vaccination, making it an important document for politicians and the government. The government, as a policymaker, can benefit from such studies to better understand the reasons behind public resistance behaviour and trends. People can battle the virus collectively by becoming vaccinated, thus policies and tactics can be developed to provide mass vaccination services. In practise, the research can be used to a variety of circumstances. If another health crisis arises, such as the coronavirus pandemic, the findings of this study can be utilised to determine how people adjust to different behaviours in other types of health emergencies. COVID-19 is a concern for the economy as well, therefore studies like this will help economists better understand people behaviour. The study included attendants of patients admitted to several hospitals in top-tier cities of Pakistan. As a result, medical practitioners can devise methods and techniques to deliver vaccination advice on a large scale in hospitals. The findings show that perceived benefits have a negative impact on accepting behaviour, implying that individuals are still unaware of the virus benefits. As a result, practitioners can figure out how to overcome these roadblocks. As a result, the study fully comprehends the reasons that cause people to modify their behaviour.
Limitations and Future Research Direction
The study carefully examines the factors that drive acceptance and resistance behaviour and derives significant outcomes that may be applied in research and practise, although it falls short in other areas. To begin with, the research report is focused on only one country, Pakistan, and hence lacks generalizability. Future research can be carried out in a variety of countries, with comparison studies being possible. Second, cross-sectional data was collected using self-administered questionnaires, with longitudinal studies being considered in the future. Finally, there was no demographic distribution in the study. According to the findings, advantages have a detrimental impact on acceptance behaviour. Future study may find ways to diminish the model advantages. Future research could include powerful moderators like awareness, sustainability, knowledge, self-regulation, and so on (Boekaerts & Corno, 2005; Howlett, Kees, & Kemp, 2008). In the future, potential mediators such as social support, culture, and values can be investigated. In the future, different ideas, such as social exchange theory, could be combined. The study is time-limited, but the research paradigm can be used in the future to investigate behaviour in the face of additional unforeseen challenges. It is suggested that the study use a variety of demographics, including medic and paramedic staff, the general public, and employees.
Conclusion
Nature and the proposed descriptive framework both point to the novelty of the study. We were able to use the HBM model to figure out how the public reacted to the COVID-19 immunisation process. Except for the impact of benefits on an individual accepting behaviour, all postulated relationships were proven in the final reports. The research primarily identifies the elements that motivate people to receive COVID-19 vaccines. Nonetheless, it may be determined that the current study is a requirement of time in times of mass vaccinations carried out all over the world.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.