
Abstract
During the Covid-19 health emergency, the self-assessment of psychological relapses in 24 health workers through a Covid-19 Emergency Triage Card sought to examine how doctors, health technicians, nurses and auxiliaries perceived their mental state immediately after the communication coronavirus positivity. A Covid-19 Emergency Triage Card consisting of two sections was submitted to the study sample. First section personal data: age, sex, educational qualification, seniority, marital status, offspring, job, workload in hours, presence of night shifts, lifestyle habits (use of alcohol, tobacco, coffee). Second section: self-assessment of the psychological repercussions of the pandemic event with five sub-dimensions: anxiety; psychosomatic disorder; depression; thought disorder. behavioral changes, rated on a three-level scale: mild - medium - severe. The analysis of our results shows that anxiety-depressive symptoms take on significant values in Covid-19 positive healthcare personnel, with greater predominance among nurses. This results in identifying workers most at risk of adverse mental health outcomes during times of health emergency is a public health task. Ensuring the physical and mental health of health care workers is crucial to maintaining a high level of health care in the population.
Introduction
Health emergencies, pandemics or other catastrophic events can pose a threat to mental health. Coronavirus disease (COVID-19) is an infectious disease caused by severe acute respiratory syndrome (SARS-CoV-2). During the first months of 2020, the virus spread rapidly, forcing many countries to impose a state of quarantine and confinement.
The interruption of a normal life following the blockade imposed by European laws and the days of quarantine have had a significant impact on the mental health of those affected by the virus. Several studies have highlighted anxiety, changes in mood, sleep quality and hours of sleep during this period. A cross-sectional study (Shah et al., 2021) states that the uncertainty and isolation of the COVID-19 pandemic triggers mental health problems, with anxiety, stress and depression and the analysis of 678 questionnaires completed during the COVID-lockdown. 19, with a non-probabilistic sampling technique, showed that 50.9% of the participants showed traits of anxiety, 57.4% showed signs of stress and 58.6% showed depression; factor analysis showed notable associations and manifestations of stress, anxiety and depressive symptoms, with prolonged days in quarantine and ultimately lack of exercise was associated with increased stress, anxiety and depression.
In India too, in addition to the obvious symptoms of infectious pathology, there has been serious damage to public mental health. India, like other countries, has implemented a national blockade to contain and curb the transmission of the virus and a research (Rehman et al., 2021) wanted to explore the psychological distress among people residing in India; 403 participants were asked to complete a questionnaire with questions about symptoms of depression, anxiety, stress, and family economic well-being. The results indicated that people who did not have sufficient financial resources to support the blockade were the most affected and family economic well-being was negatively correlated with stress, anxiety and depression. Although not directly experienced as a traumatic event, the pandemic has indirectly caused changes in habits and life perspectives.
A study with an online survey of the adult population of the Netherlands concluded that the coronavirus crisis has led to a healthier lifestyle in one part and to a lesser extent an unhealthy lifestyle in another part of the Dutch population, stating that more studies are needed to see if this behavioral change is maintained over time and how different lifestyle factors can affect the susceptibility and course of COVID-19 (Van Der Werf et al., 2021).
In Sweden a study (Molarius & Persson, 2022) with a population survey states that there were, apart from economic difficulties, very few differences in lifestyle and health factors. Some evidence indicates that those most at risk of developing mental health problems are women, young people, those with sleep disorders, those with already poor health and those with relatives with COVID-19 (Brooks et al., 2020). Furthermore, patients with pre-existing psychiatric disorders are a population at vulnerable risk for worsening of their condition and relapse of symptoms (Belz et al., 2022). All changes can have negative repercussions with dysfunctional emotional reactions and implications for physical health. The psychological impacts of the pandemic are increasingly reported in the scientific literature highlighting that people with COVID-19 can experience depression, anxiety, stress, panic attacks, irrational anger, impulsivity, somatization, sleep disturbances, and even suicidal behaviors (Kawohl & Nordt, 2020; Sher, 2020a, 2020b, 2021; Thomas, 2020). It is stated (Holmes et al., 2020) that the total duration of imprisonment, fear of contagion, frustration, boredom and excess of media information, could be predictors of stress highlighting the negative impact of COVID-19 on mental health with anxiety-depressive symptoms. In addition, there are several factors associated with mental health problems for COVID-19, which include age, gender, marital status, education, occupation, income, place of residence, close contacts with people with COVID-19, comorbidities, coping styles, psychosocial support, health communication and protective measures for the risk of contagion (Bhattacharjee & Acharya, 2020; Budimir et al., 2021).
A review suggested that stressors such as prolonged quarantine, fear of infections with frustration, boredom, inadequate supplies, inadequate information, financial losses, and stigma resulted in symptoms of long-lasting post-traumatic stress, confusion and anger (Nicola et al., 2020). Among the different professions, students and healthcare professionals have been found to experience stress, anxiety and depression more than others. The epidemiological distribution of coronavirus-associated mental health problems is heterogeneous among healthcare professionals and current evidence suggests that the ongoing psychiatric epidemic with the COVID-19 pandemic requires the attention of the healthcare community (Labrague, 2021). The coronavirus pandemic (COVID-19) affects both health and psychosocial well-being and studies suggest that suicidal tendencies and PTSD commonly follow severe economic crises or natural disasters (Beaglehole et al., 2018; Chaves et al., 2018).
Similar considerations hold true for the COVID-19 pandemic. The psychological effects of persistent emergency health stress among the population and the exacerbation of mental health disorders among vulnerable individuals will strain the international health system, preventing the resumption of normal life for many people even when the threat of viral infection will tend to decrease. Future epidemiological studies should analyze the psychopathological variations and temporality of mental health problems during Covid-19 in different categories of subjects and especially in health professionals, considering that the quarantine studies and the prevention strategies adopted have found that depression, anxiety, mood disorders, post-traumatic stress, sleep disturbances, panic, stigmatization, low self-esteem and lack of self-control are most prevalent among individuals with physical isolation (Hossain et al., 2020). The purpose of our study is to investigate, with a Covid-19 Emergency Triage Card, how the health personnel of a Sicilian hospital perceive their mental state in the period following the communication of the SARS-CoV 2 positive report, when in home isolation.
Ethical Considerations
Participants were informed about the purpose of the study and signed an informed consent form. The ethical principles enshrined in the Declaration of Helsinki have always been observed. The confidentiality of the data and the anonymity of the subjects have been preserved in compliance with the GDPR 679/2016 on the Protection of Personal Data. Participation was voluntary and without compensation when the subjects were already in isolation.
Materials and Methods
In the staff of a Sicilian hospital, from April 2020 to November 2020, in a maximum time of 15 min, with a COVID-19 Emergency TRIAGE CARD, an attempt was made to evaluate how doctors, technicians, nurses and auxiliaries perceived their mental state in the period immediately following the communication of the COVID-19 positive report. All the staff in the sample examined had been engaged not only with Covid-19 positive patients, but also with negative patients and with patients whose positivity, at the time of the provision of health services, was under investigation. The sample of 50 subjects was chosen after telephone contact and voluntary participation. After explanation and informed consent, the COVID-19 Emergency TRIAGE CARD was administered to all subjects via Skype, approximately 24 h after the coronavirus positive communication, when the subjects were already in home isolation. However, of the sample only 24 subjects, contacted after the notification of the report, expressed their availability, the other 26 subjects were not available for various reasons, including exhaustion resulting from the disease or other symptoms that reduced the interaction. All the interviews were conducted maintaining a neutral attitude so as not to influence the responses and moods of the subjects. In all cases, before starting the purpose of the research was explained in a complete, reassuring all participants on anonymity and full respect for the right to privacy. The card in self-assessment, after a brief explanation of the dimensions investigated; it consists of a registry section and a self-assessment section. Each subject interviewed a progressive number was awarded as a unique identifier, avoiding name and surname.
The personal data section revealed: age, sex, education, work seniority, marital status, offspring, job, workload in hours, presence of night shifts, lifestyle habits (use of alcohol, tobacco, coffee) The self-assessment of the psychological repercussions of the pandemic event has five sub-dimensions: anxiety - psychosomatic disorder - depression - thought disorder - behavioral alterations; dimensions evaluated with a Likert scale from 1 to 5 referring to the last two weeks taking into account that 1 indicates the minimum (mild) and 5 the maximum (severe), weighted on a three-level scale: mild - medium – severe.
Results
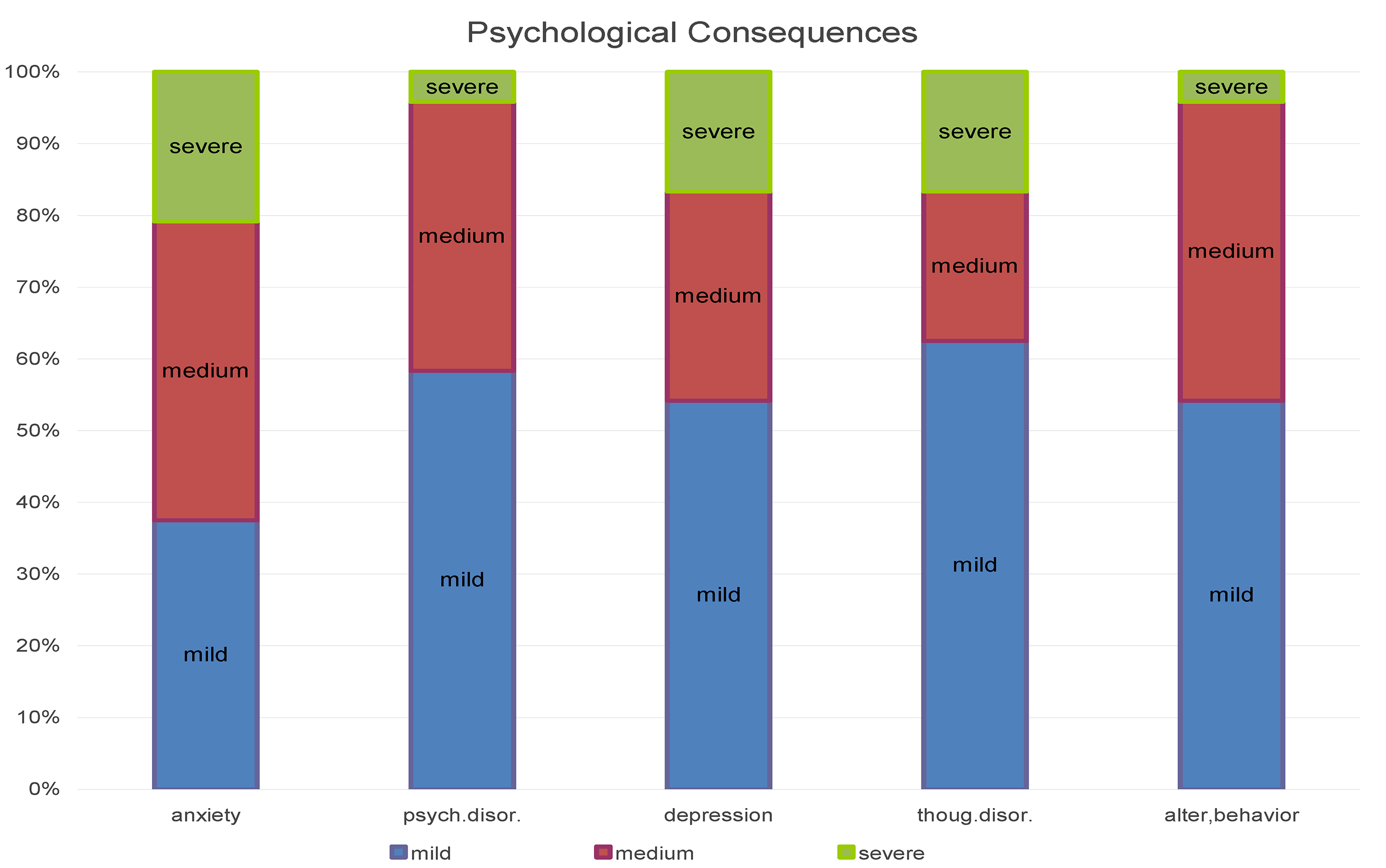
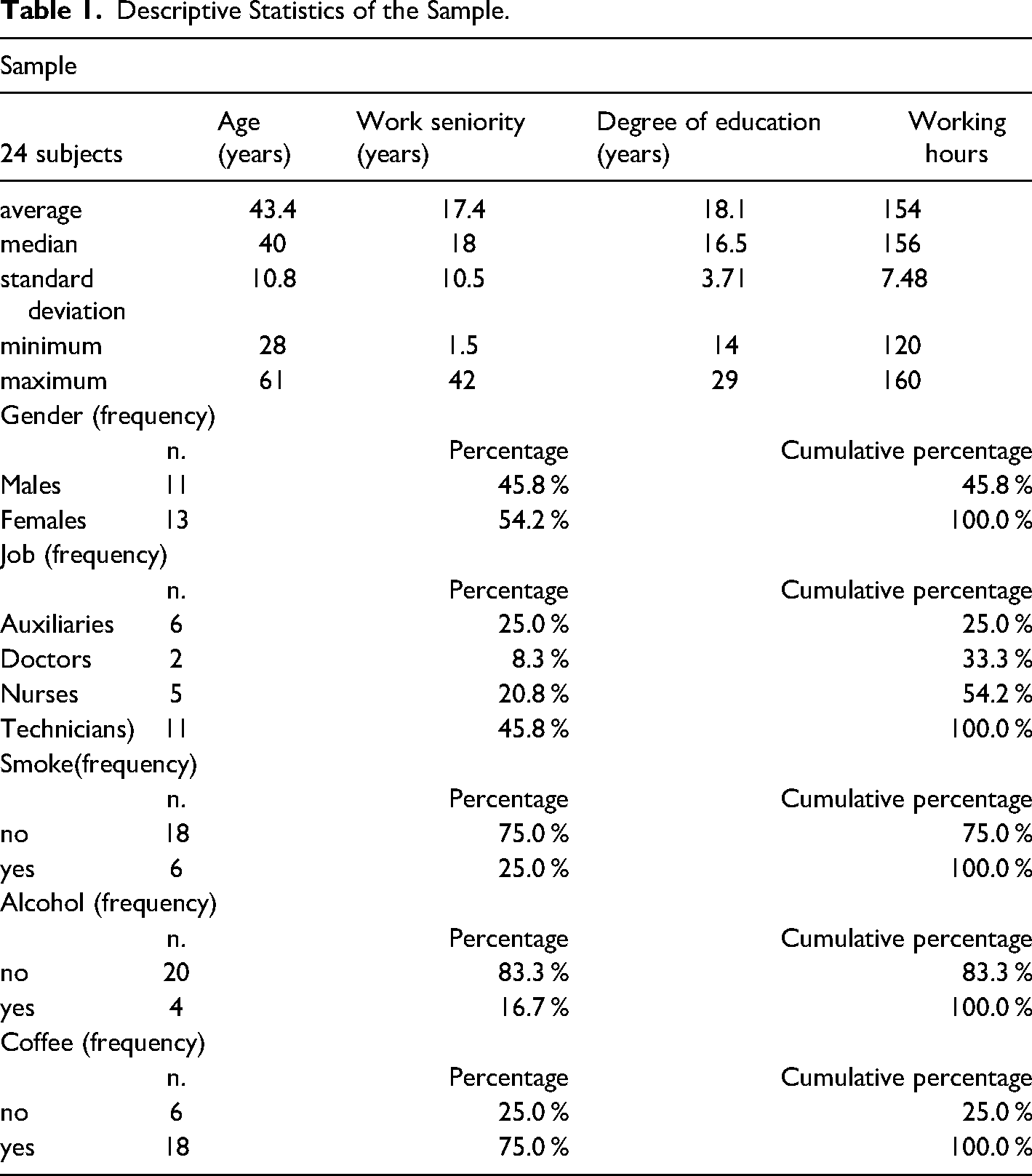
Given the small size of the sample, it was decided to proceed with a descriptive analysis of the data obtained by analyzing the registry section. Collected the data, we calculated the descriptive statistics of the sample referring to: sex, age, education, job, seniority in employment, working hours, lifestyle habits (alcohol - coffee - smoking) (Table 1). The self-assessment of the psychological consequences of the pandemic event, divided into five sub-dimensions, results in the distribution illustrated in Figure 1. The mean of all five distributions lies between the “mild” and “medium” levels, with a major shift towards higher severity for the “Anxiety” and “Depression” dimensions. The strong correlations between the mental states investigated could be an artifact introduced by the limited amplitude of the three-point scale used in this section of the questionnaire, or it could indicate a holistic approach to the evaluation of one's own undesirable mental states, or it could reflect a poor capacity of discrimination between these five dimensions. Consistent with Sullivan (Sullivan & Artino, 2013) on the possibility of parameterization of discrete factors, we have created a severity scale of the reported symptoms, derived from the application of a min-max normalization function to the average of the scores (from mild = 1 to severe = 3) indicated on the self-assessment scales: anxiety; psychosomatic disorder; depression; thought disorder;. alterations of behavior, according to the formul
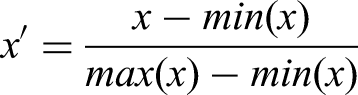
Psychological consequences.
Descriptive Statistics of the Sample.
In this way we have derived an amplitude interval of 10 points with the following correspondences: mild = 0.00
medium = 0.50
severe = 1.00
Overall, the subjects report symptoms as a whole between mild and medium, with a median of 0.20. However, the range of data is considerable, which assumes a value of 0.9, going from a minimum value of 0.00 to a maximum value of 0.90, on a theoretical maximum of 1.00 (Figure 2). This transformation will allow us to more easily visualize any differences between data clusters. Based on the premises and acquired data, the following clusters have been identified and developed:
✓ By sex ✓ By age ✓ By length of service in ten-year bands; ✓ By professional profile (doctors, nurses,. auxiliaries, technicians)
Symptoms severity scale.
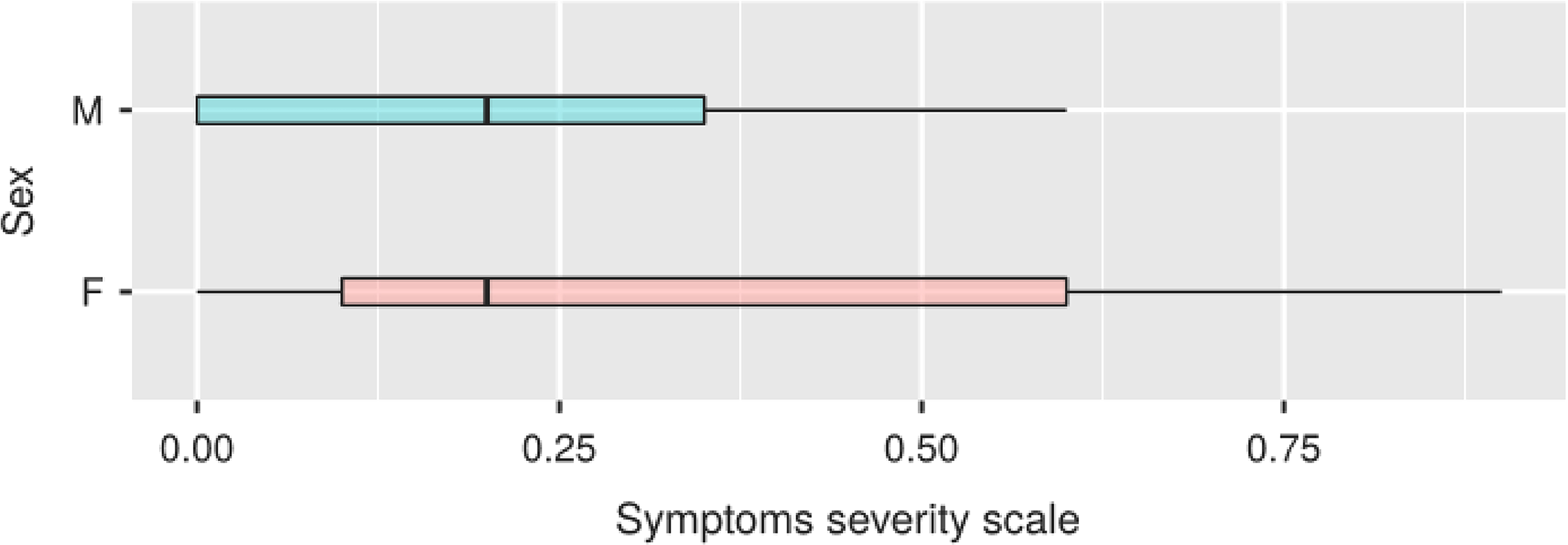
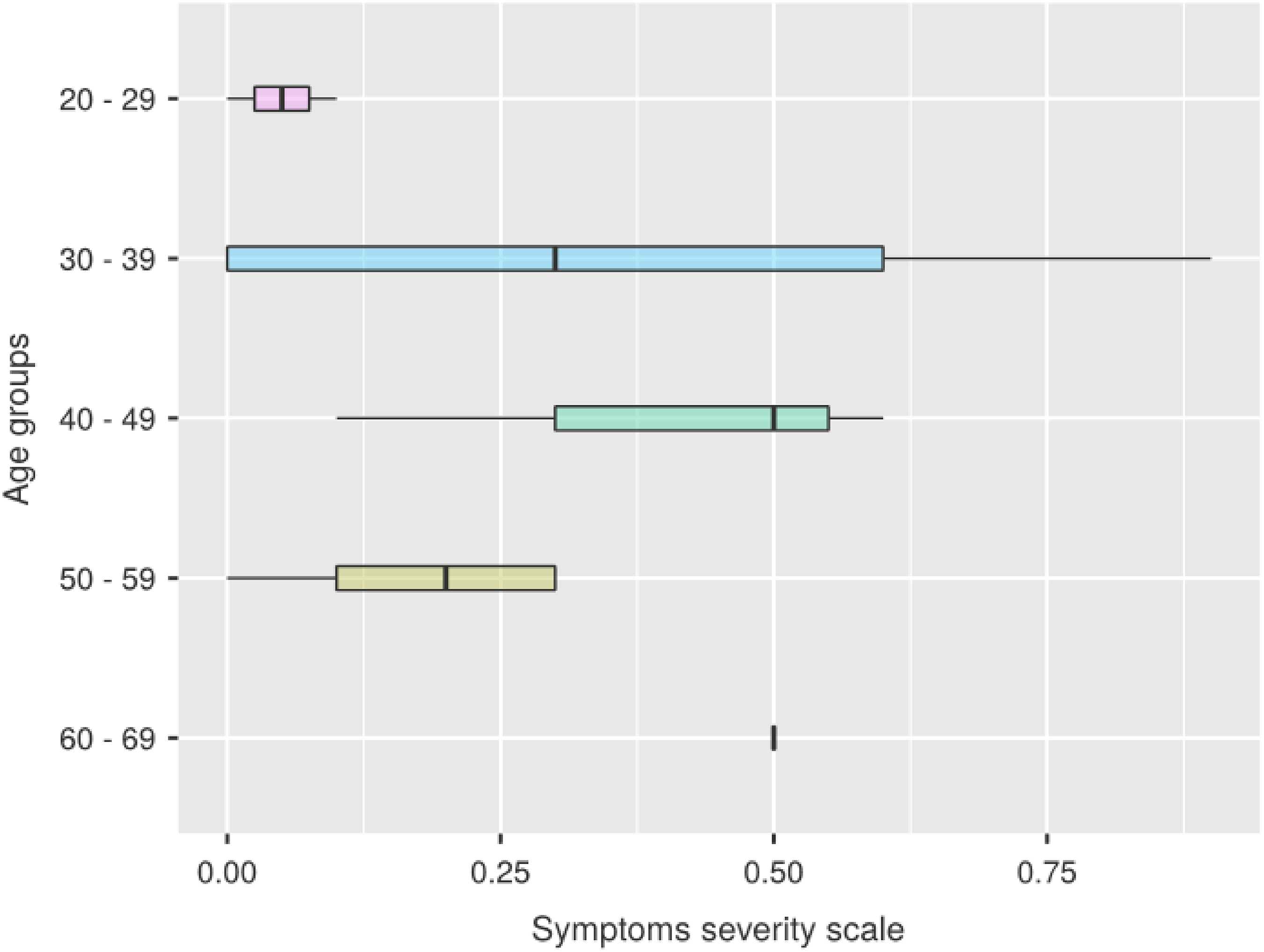
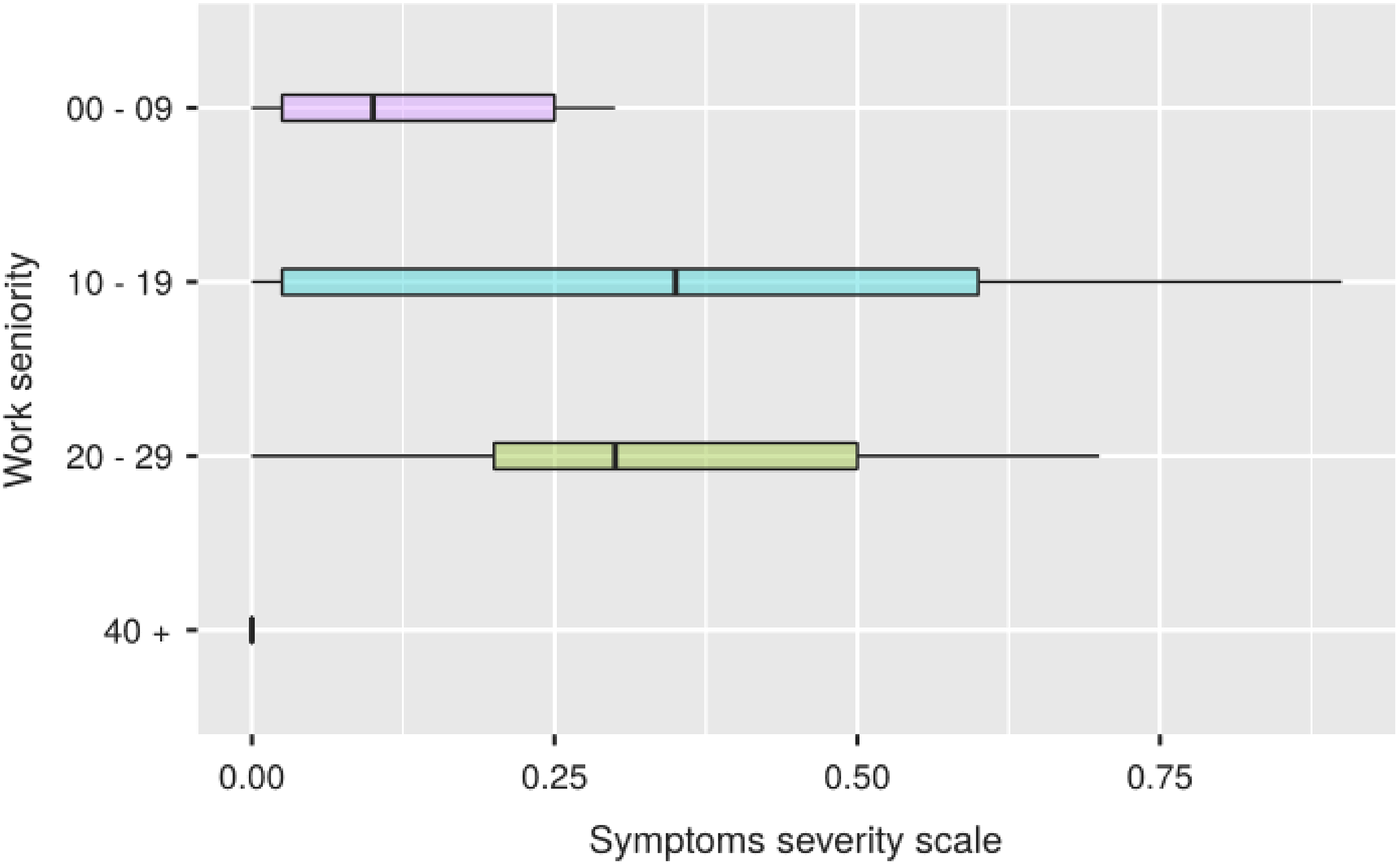
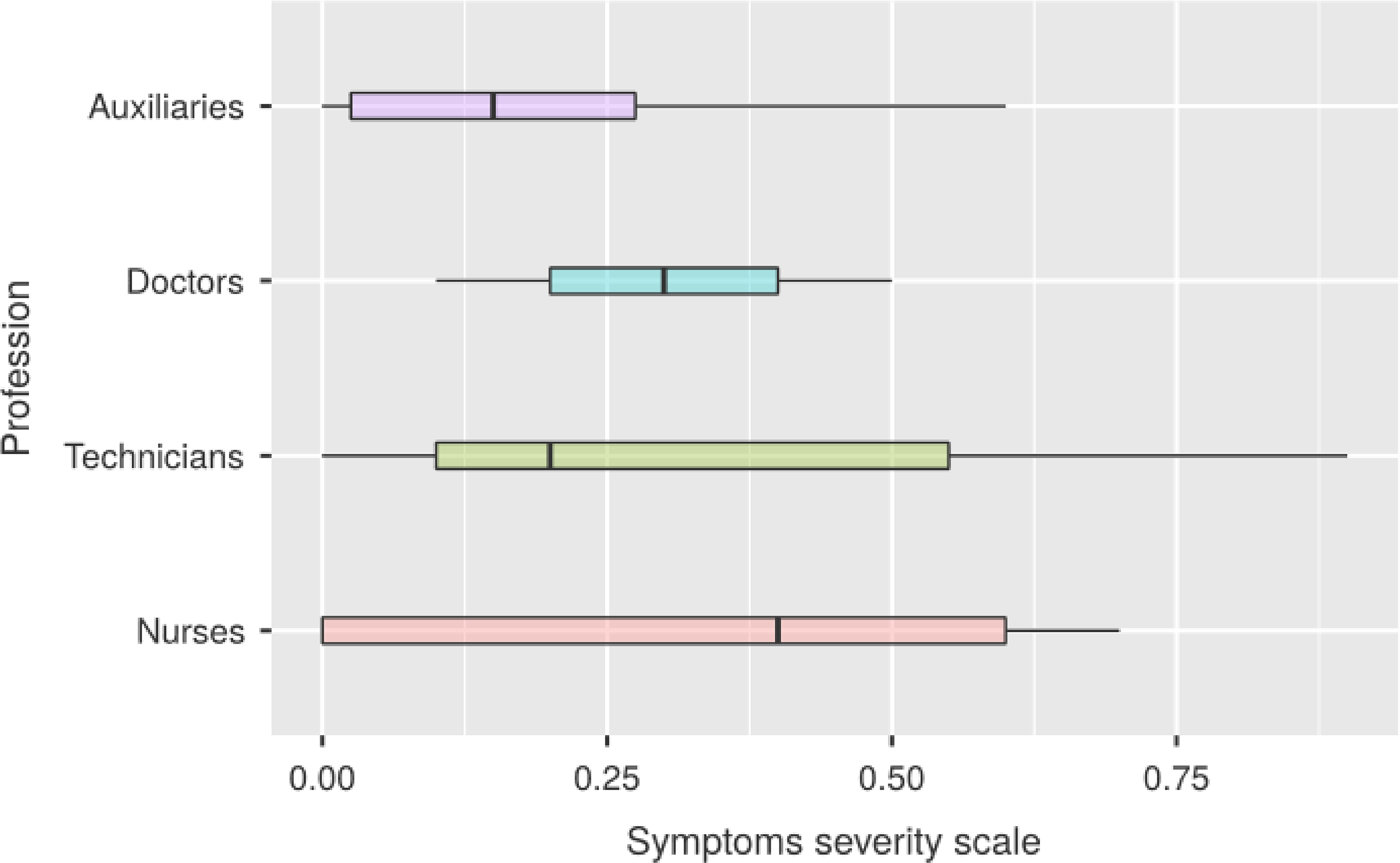
In the Figure 3, we note that in women the right tail of the distribution is wider, compared to a median identical to that of men, due to a greater number of female subjects reporting a combination of symptoms ranging in severity from medium to severe With respect to the age groups and seniority of service (Figures 4 and 5) the data we obtained seem to follow a normal distribution, with a peak of symptoms in the decade 40–49 for the chronological age and in that 10–19 for length of service. Compared to the professional category, the one that reports more severe symptoms overall is that of nurses, followed in order by doctors, technicians and auxiliares (Figure 6).
Symptoms severity scale.
Symptoms severity scale.
Symptoms severity scale.
Symptoms severity scale.
Discussion
Recent literature has indicated that anxiety diagnoses have increased following the COVID-19 pandemic. The diagnosis of anxiety often presents with sleep problems and comorbidities with depression. A Hong Kong population study, just 3 months after the first coronavirus case, assessed depression and anxiety during the pandemic, respondents were randomly recruited and asked to complete a structured health questionnaire (PHQ-9), and on generalized anxiety disorder- (GAD-7); of the 500 respondents included in the study, 19% had depression (PHQ-9 score ≥ 10) and 14% had anxiety (GAD score ≥ 10), and 25.4% reported that their mental health had deteriorated in following the pandemic (Choi et al., 2020). According to a study by Lai et al. (2020) “a sizeable portion of health care workers reported experiencing symptoms of depression, anxiety, insomnia and distress. Depression is a state of overwhelming sadness that hinders the ability to carry out daily activities, including work. According to a survey, health professionals at Chinese hospitals who have treated patients with COVID-19 reported experiencing anxiety, depression and sleep disturbances (Huang & Zhao, 2020). The element of unfamiliarity in dealing with COVID-19 increases the levels of fear experienced by healthcare professionals, as partial knowledge of the disease instinctively generates an additional level of suspicion. The individual response to fear depends on the personality and therefore cannot be predicted. Fear is not always a negative emotion, as it can ward off impulsive decisions that could lead to unwanted outcomes. However, the resulting levels of fear can have a severe impact on individual performance resulting in occupational stress and a greater likelihood of work-related errors. In particular, work-related stress has been observed to affect performance in numerous professions afflicted with excessive workload and lack of social support, as described by the American Psychological Association. This is confirmed by our data, which showed an increase in anxiety and depression, even if of medium degree.
Conclusion
With reference to the health emergency caused by the coronavirus, the analysis of our results shows that the anxious-depressive symptomatology takes on significant values in healthcare personnel with greater predominance among nurses. Identifying the individuals and populations most at risk of negative mental health outcomes is a very important public health task during and after the pandemic (Nicolini, 2020). Consequently, it becomes essential that staff are constantly trained and stay up to date on coping strategies. The psycho-emotional impact of the COVID-19 pandemic on the staff is indeed multifaceted; it affects both their ability to work and their ability to cope with mental health problems. In addition, the situation can be made worse by the shortage of protective equipment and excessive working hours and the huge number of patients. Ensuring the physical and mental health of staff is critical to maintaining a high level of health care.
In the past, a review (Folkman & Greer, 2000) encouraged researchers and clinicians to pay the same attention to the development and maintenance of psychological well-being in the face of serious illnesses as to the etiology and treatment of psychiatric symptoms.
All governments must invest in human capital, protective equipment and adequate mental health improvement strategies to ensure the best possible conditions. The anxiety-depressive symptoms of COVID-19 can be addressed through organizational interventions, including increasing social support, providing psychological support services, and providing interventions that promote resilience and stress management (Labrague & De Los Santos, 2020).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.