
Abstract
Analysis of in-depth qualitative interviews with 20 bereaved parents and 11 service providers revealed a more holistic conceptualization of the bereavement process for parents who have lost a child. Holistic “states” included: “helplessness prior to the death,” “fog,” “turmoil,” “transition,” “new beginnings,” and “stability.” Findings showed that loss and restorative processes are characteristic of more than one state, the bereavement narrative starts prior to the death, there is often a downturn after the bereaved parent seemingly is doing better, and the process never ends but may include a continuing bond with the deceased and reoccurring moments of extreme grief. Recommendations for direct practice, program development, and future research are presented.
To this day, … people don't understand what we’re going through. … I remember many sessions we would come into the group and we’d say, “Oh somebody said, ‘It's been six months! Aren't you better yet? Are you still going to that group?'” (laughing). We were like, "Oh God. You just don't get it,” you know? … and I said, “How do we let the public know that there is no easy way around this? You don't understand until you walk in our shoes.” I said, “Isn't there a writer or somebody that could put it in words that everybody knows, and put it in the paper, and then maybe people would read it and think a little more about it?” I mean, they were just trying to be kind, I’m sure, but they weren't really, you know? We were like, “Oh my God they have not got a clue [emphasis added].” Not got a clue.
Despite a significant amount of literature and education about bereavement, experiences such as this, as described by a bereaved parent in this study, continue to show that friends, family members, and service providers lack an understanding of the bereavement process after the death of a child. Historically, theorists have attempted to describe the bereavement process for deaths in general. Over 50 years ago, Kubler-Ross (1969) published a seminal book describing five stages that people go through when facing their own death: “denial and isolation,” “anger,” “bargaining,” “depression,” and “acceptance” (p. 9). Although this model has been widely critiqued, “to this day, [Kubler-Ross's] stage theory is still widely known, taught, and used in clinical practice” (Stroebe et al., 2017, p. 460). The continued use of Kubler-Ross's model suggests practitioners and bereaved people have a need for a guide or model to understand the process.
Other theorists have rejected stage theories. Worden (1982), for example, described four tasks of mourning: “to accept the reality of the loss,” “to experience the pain of grief,” “to adjust to an environment in which the deceased is missing,” and “to withdraw emotional energy and reinvest it in another relationship” (pp. 11–15). Both Bowlby (1980) and Parkes (1970) worked on the development of four similar phases of grief: “numbness,” “yearning,” “despair and disorganization,” and “reorganization” (Parkes, 1970, p. 196).
In the context of service provision, Stroebe and Schut (1999) introduced a “dual process model” (DPM), which comprises of two types of stressors related to bereavement: processing the loss and restoration (i.e., reorienting oneself through rethinking and replanning). However, as indicated by Stroebe et al. (2010), their DPM “is a model, … of coping with loss, not a generic model aimed at explaining the broad range of phenomena and manifestations associated with bereavement” (p. 274).
More specifically, for decades, the experiences of bereaved parents have been known to differ from the experiences of people grieving other types of deaths (Rando, 1985; Sanders, 1980) and are still to this day, not well understood (Denhup, 2017, 2019; Dias et al., 2017). Some literature specific to grieving the death of a child shows unique features due to the parenting role and indicates that the process never ends (e.g., Arnold and Buschman Gemma, 2008). Rather than a final phase of a return to normalcy and/or detachment from the deceased as some past models have asserted (e.g., Bowlby and Parkes), we have increasingly seen over the past three decades a move toward understanding that bereaved parents typically maintain a continuing bond with their deceased child (Davies, 2004). What has not yet been explored is the bereavement process over time, looking holistically at the experience of bereaved parents spanning many years after the death of their child. Particularly, “few studies [have] explored the needs of bereaved parents from the parents’ perspectives” (Denhup, 2019, p. 346). To address this gap in the literature, the objective of this study was to hear the voices of bereaved parents about their bereavement process over time, including their cognitions, emotions, behavior, physiological responses, and spirituality. To better inform service providers, program developers, employers, friends, and family members attempting to be supportive, the goal was to increase our understanding of the bereavement process for parents who have lost a child.
Method
Data Collection
A total of 31 semistructured, in-depth, 2-hr individual interviews were conducted. The initial recruitment process targeted bereaved parents who were over the age of 18 years, who experienced the loss of a child at least 4 years ago (so they could retroactively speak to their experiences over time), and who indicated feeling comfortable with describing their bereavement process from the time of death until the present. Staff at the local bereavement peer-support program sent recruitment letters to previous clients who might meet the inclusionary criteria and with whom the agency still had contact. Analysis of the 13 interviews showed such remarkable consistency in the bereavement process that the researchers wondered whether the support group itself is what had shaped participants’ narratives. To answer this question, a second phase of the study was developed that included seven interviews conducted with bereaved parents who had never attended the local support group and 11 interviews with a range of service providers who were able to provide insights from the perspective of bereaved parents who had not attended this support group. For this second phase of the study, recruitment occurred through posting flyers on a local online classified platform, at local health and community centers, and through word of mouth. Service providers were recruited by sending a recruitment letter to all known bereavement specialists in the geographic area, and by mailing a letter to all churches within 10 km of the first author's office.
During the interviews, all participating bereaved parents were asked to share what was happening for them over time from their perspective (from time of death until the present). They were asked to use their terms and their labels. As participants spoke, the participant and interviewer together outlined a timeframe that included dates of when shifts in the participant's process occurred. As each time period was described, participants were asked to provide “keywords” that they would say characterized that period, and they were asked to indicate what was and was not helpful. At the end of the interview, participants were asked what had changed for them between the time of death and the present time. Bereaved parents were asked to speak about their emotions, behaviors, thoughts, physiological responses, and spirituality. Service providers were asked these same questions but were asked to try to respond from the perspective of the bereaved parents with whom they had worked. All interviews were audiorecorded and transcribed verbatim.
To increase the trustworthiness of the findings, bereaved parent participants were offered to attend one of three member-check focus group sessions where they were asked to comment on: whether they saw their responses in the findings, whether there was anything they felt should be added or deleted, and anything that might further contribute to the findings. Those unable to attend were offered the opportunity to provide feedback through email. All but one parent provided feedback. The focus groups were audiorecorded, transcribed verbatim, analyzed, and incorporated into the overall findings. All service provider participants were sent a copy of the study’s final report and invited to comment on the findings by email or by phone. All those who responded to the findings indicated that the results were an accurate reflection of their experiences; no one had any disagreement about the study findings. For phase 1, research ethics approval was obtained from the agency where the initial 13 participants were recruited. Research ethics approval was obtained from the University of Windsor for both phases of the study.
Participants
This study was conducted in a city with a population of just over 300,000, in Ontario, Canada, bordering the United States. In this geographic region, most media, literature, and service provider training regarding bereavement is American. The region had one well-known bereavement program, housed in a large community mental health agency. Programming mostly included bi-weekly 2-hr peer support open meetings, each for specific populations of bereavement, such as the death of a child. This local support program relied most heavily on Wolfelt’s (2002) touchstones and did not use any of the stage, phase, or task theories mentioned above.
Of the 20 bereaved parents, three were fathers and 17 were mothers. The average age was 58.6 years, with a range of 40–69 years (two missing). The average age of the child who had died was 17.3 years with a range of stillbirth to 34 years. The average time since the time of death was 13.9 years with a range of 2.8–39.2 years (one participant was interviewed despite not meeting the criteria of a minimum of 4 years since the child passed away). The causes of death included eight accidents (two drowning, five vehicle-related accidents, one drug overdose, and one other accident), and 12 health-related causes (two genetic disorders, one cancer, one unexpected result of an ongoing medical condition, two unexpected medical conditions, and three unknown causes—stillbirth, crib death, and unknown). At the time of the interview, 16 parents were married or common-law, two were divorced, one was single, and one was widowed. A total of 12 were employed, two unemployed, five retired, and one participant did not specify employment status. In terms of highest level of education, one parent had earned a master's degree, three an undergraduate degree, one university certificate, seven a college diploma, one some college, and seven high school. Fifteen identified as Christian (e.g., Presbyterian, Christian, United, Roman Catholic, United Mennonite, Protestant, Lutheran, Seventh Day Adventist) and five indicated other religions such as “loving kindness,” Atheist, not applicable, “Love of Spirit.” All, except one bereaved parent, were Caucasian.
When asked who provided them with support throughout their bereavement process, seven of the 13 who had been clients at the bereavement program indicated that this program had been their only support. Two identified other counseling, three indicated family and friends, and one indicated that church members were supportive. Of the seven who did not attend the local bereavement support group, four indicated receiving support from family and/or friends, and three had been to a social worker, psychologist, or therapist. One participant indicated having received most of her support from God. One participant indicated that in addition to other supports, online supports were a benefit. One participant indicated that the only support received was from her general practitioner. The 11 service providers included: one funeral director, two social workers specializing in grief, three bereavement specialists, four clergy, and one grief counselor employed in a church.
Data Analysis
Following Strauss and Corbin’s (1990) principles of open, axial, and selective coding, the first author analyzed the first phase of data with the initial 13 participants. This included: reading through each individual transcript; reading each transcript a second time, highlighting, and documenting meaningful excerpts related to the overall research question and specific interview guide questions; copying and pasting all meaningful excerpts into a Microsoft Word document; and repeatedly cutting and pasting meaningful excerpts to integrate the data across participants to form groupings that hung together in terms of the meaning of the content. As groups were being formed, themes began to emerge but were continually revised as new information was added to each group. To increase the credibility of the analysis, two research assistants (who participated in interviewing, transcribing, and analyzing some of the data) met with the first author to debrief, debate, discuss, and confirm the overall findings.
For the second phase of interviews, open, axial, and selective coding was completed by the second author using Dedoose, a qualitative data analysis program. The analysis process consisted of: coding every segment of text related to the research question for its meaning; compiling a Dedoose report that grouped like codes together; and reorganizing the codes and relevant excerpts to form patterns and themes. For the service provider data, the first author analyzed the transcripts following this same Dedoose process. The two authors had frequent contact during this analysis period to explore code labels, interpret the meaning of excerpts, and examine, compare, and contrast possible themes and patterns. Remarkable consistency was found across the two authors and across the three cohorts of participants. The results were also compared with the member-check focus group results for any additional insights provided by participants.
Findings
When asked what was happening for them cognitively, emotionally, behaviorally, physiologically, and spiritually, there was considerable consistency across participants. When asked what was helpful and not helpful for each period described, participants' responses consistently contributed insights about what was occurring socially and relationally. The only notable difference between bereaved parents who had been part of the local support group and those who had not was that those who had been part of the group used the anniversary-of-the-death dates as key markers of when transitions occurred in their process. The other participants spoke about the importance of anniversary dates but did not describe them as transition markers. Exceptions to the flow in process occurred, especially in instances where subsequent traumas occurred in the individual's life and when little support was available to the bereaved parent. Six distinctive states emerged: “helplessness prior to the death,” “fog,” “turmoil,” “transition,” “new beginnings,” and “stability.”
Helplessness Prior to the Death
When bereaved parents were asked what was going on for them at the time of the death, all of them began their narrative at a point prior to the death. Parents were setting the context and identifying relevant details that they later would refer to as part of their bereavement narrative. For some, their child had been ill for a period of time. They described how this illness came about, their experience with the medical profession, and their time by their child's side. In the incidence of an accident, they described the entire day of the accident, who was doing what, when, and where. One participant even started with the birth of the child who died as an adult because the child had been vulnerable in many ways throughout his life. As shown in Table 1, participants spoke of anxiety, feeling helpless, disbelief and not wanting to leave their child's side during the illness, at the scene of the accident, and/or after the death.
Participants’ Keywords for Helplessness Prior to the Death.
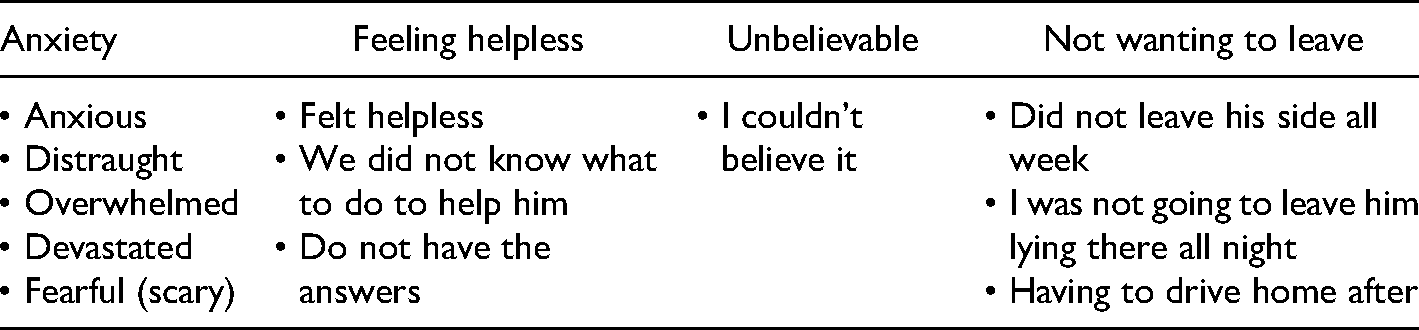
When asked what was helpful, participants spoke about the support they received from victim services, police, Chaplain, hospital staff, and family members. What was not helpful was how they were spoken to at the time of death, for example, “freaking doctor; … all he's got to say is, ‘Oh your son succumbed to his injuries.’ And boom he's out of there.”
Fog
For bereaved parents who had arranged a funeral, the time between the death and the funeral was distinct from the experience after the funeral because of the need to plan and having so many people help with the funeral. Having family and friends assist with planning the funeral and managing daily functioning helped. While they could not remember everyone who attended, bereaved parents remembered and found it helpful that, “a lot of people were there” and “[the] line-up was unbelievable.” What was not helpful was comments from others, such as “a relative saying [the child] went to hell because he was not baptized” and comments about how unchristian it is to cremate. What was also not helpful was how quickly all the supports disappeared once the funeral was over.
From the time of death until 3–6 months later (regardless of whether there was a funeral), participants described a time of “fog.” As shown in Table 2, fog included features of being dazed and confused, intense emotions, and behaviorally just managing:
Participants’ Keywords for Fog.
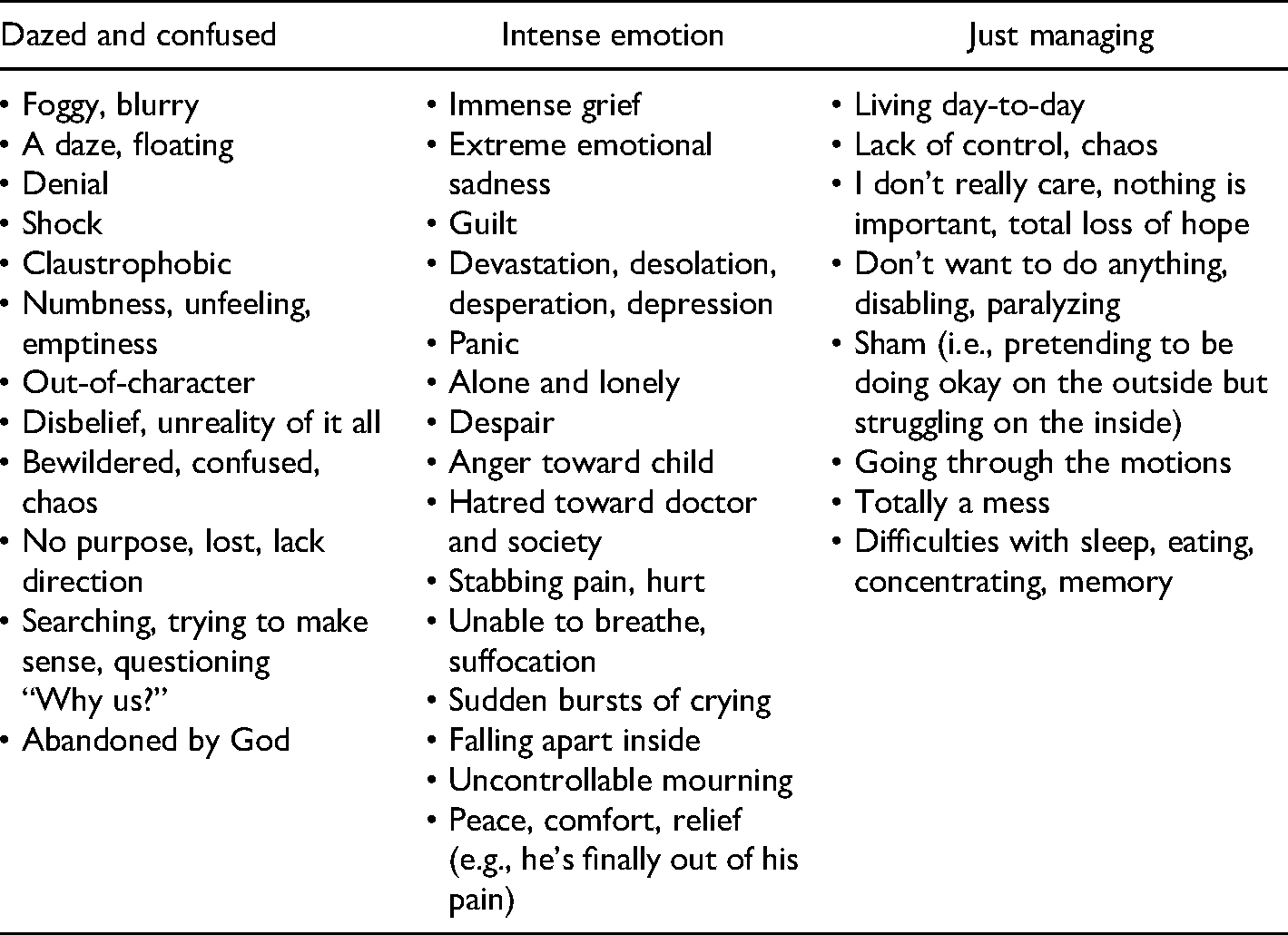
I didn't feel much like eating or anything. I don't remember wanting anything or wanting to do anything. I just, everything was just standing still. I couldn't concentrate on anything. I didn't want to do anything, didn't even know what to do or where to go. Didn't have any desire to do anything.
Examples of what was helpful included: being at work, support from family and friends, reading, and writing letters to their child. When asked what was unhelpful, every bereaved parent and service provider interviewed spoke about the “stupid things people say” or “insensitive things people say.” More specifically, it was not helpful for people to: try to make the bereaved person feel better; indicate that they understood when clearly, they did not; and expect that the bereaved person would “get over it.” Examples included: “God wanted another angel,” “God doesn't give us any more than we can handle,” “You can have another baby,” “I know what you’re going through ‘cause I lost my mother,” and a physician indicating the parent would “get over it in three months.” One participant described still being upset 38 years later about the cemetery worker saying, “Oh she’ll be good and dry. She’ll [be there] for years without getting wet. We put a cement thing around her.”
Some participants indicated what was not helpful was, “Some people who completely ignored us.” Another participant expressed, Not seeing anyone grieve, I think that was the biggest. The fact that I do not know if it was over and done for them, or if they had not grieved, or if they were holding it in, or if they were doing it in private ….
Tensions between spouses also were not helpful. For example, one participant noted, “It's like you’re separated: You’re in the same house, sleep in the same bed, but you’re separated because you’re so engulfed in trying to breathe in and out every single day and just get through the day.”
Turmoil
Participants explained that once the fog had lifted, they moved into a state of “turmoil” that lasted up to about 1 year from the time of the death. For most participants, this was the time when they expected to be better, but instead felt worse as they realized that the process was not going to end soon. Some even reported that others, such as physicians, had told them to expect to be “better” in 3 months. So, when getting “better” did not occur, they reached out to a counselor, online support, and/or the local bereavement support specialist. As shown in Table 3, this period included descriptors regarding “surreal,” “struggle,” and, for some, “relief.”
Participants’ Keywords for Turmoil.
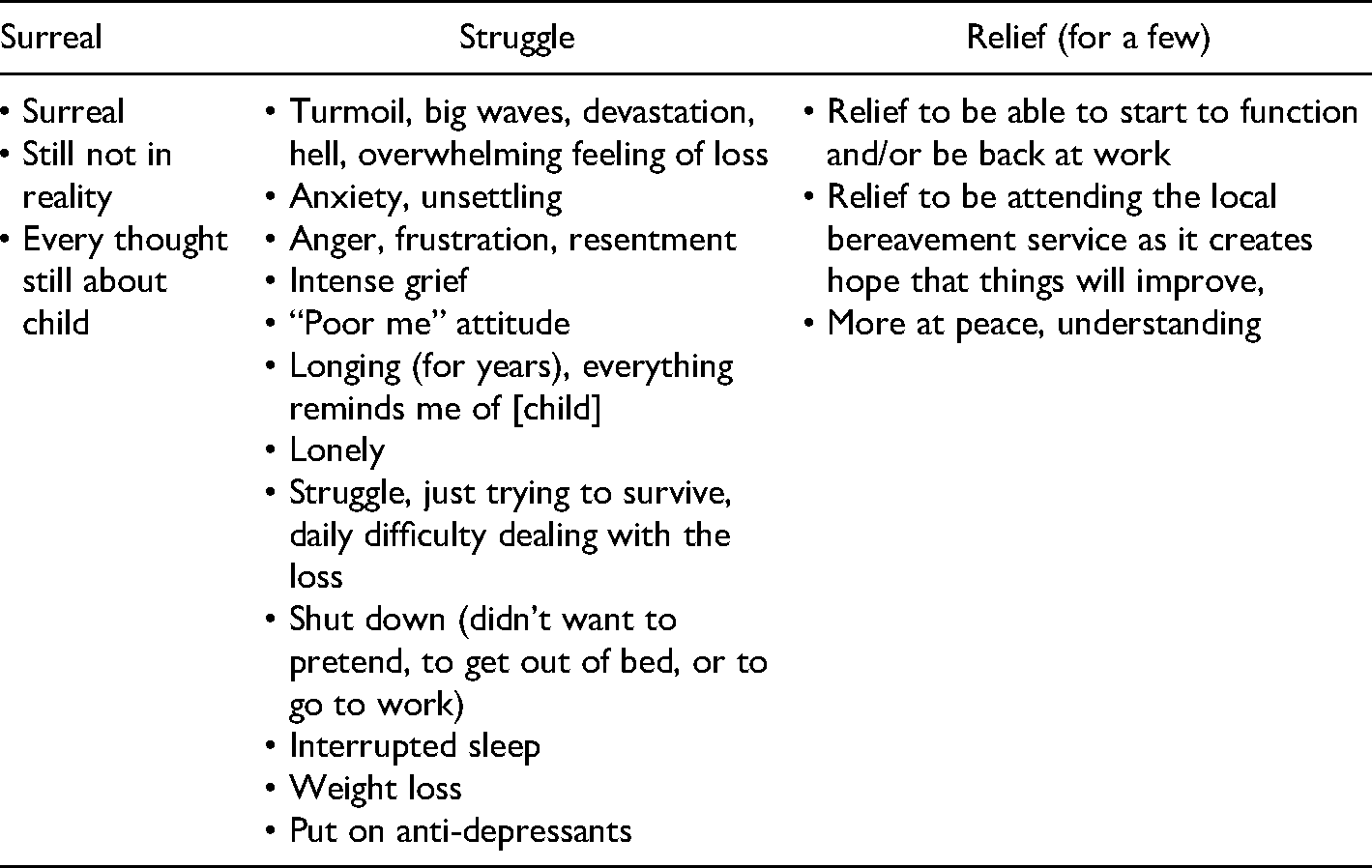
Three bereaved parents seemed to have initially skipped the turmoil state and found strength by returning to work and/or the birth of another child. These three participants seemed to move quickly to a transition phase: happy, at peace, and receiving a lot of support. However, they described later “losing ground; more thinking and pain, but not a sharp pain;” “grey;” and “depression.” Interpersonally, many described a realization about their relationships: some friends became stronger friends, others were no longer friends, and they were beginning to meet new people and form friendships with people who understood. Those friends who understood were helpful. Support groups and service providers were also helpful. People saying insensitive and stupid things continued to be unhelpful.
Transition
As shown in Table 4, bereaved parents described a time of “transition,” starting, for most, around the end of the first year. This time was characterized by now being in reality, less intense emotions, and being able to manage better. This was when participants described beginning to have periodic good days, smiling or laughing for the first time, beginning to socialize with others, and not thinking about the deceased every minute. At the same time, feelings of guilt about these moments of enjoyment led to participants feeling down:
Participants’ Keywords for Transition.
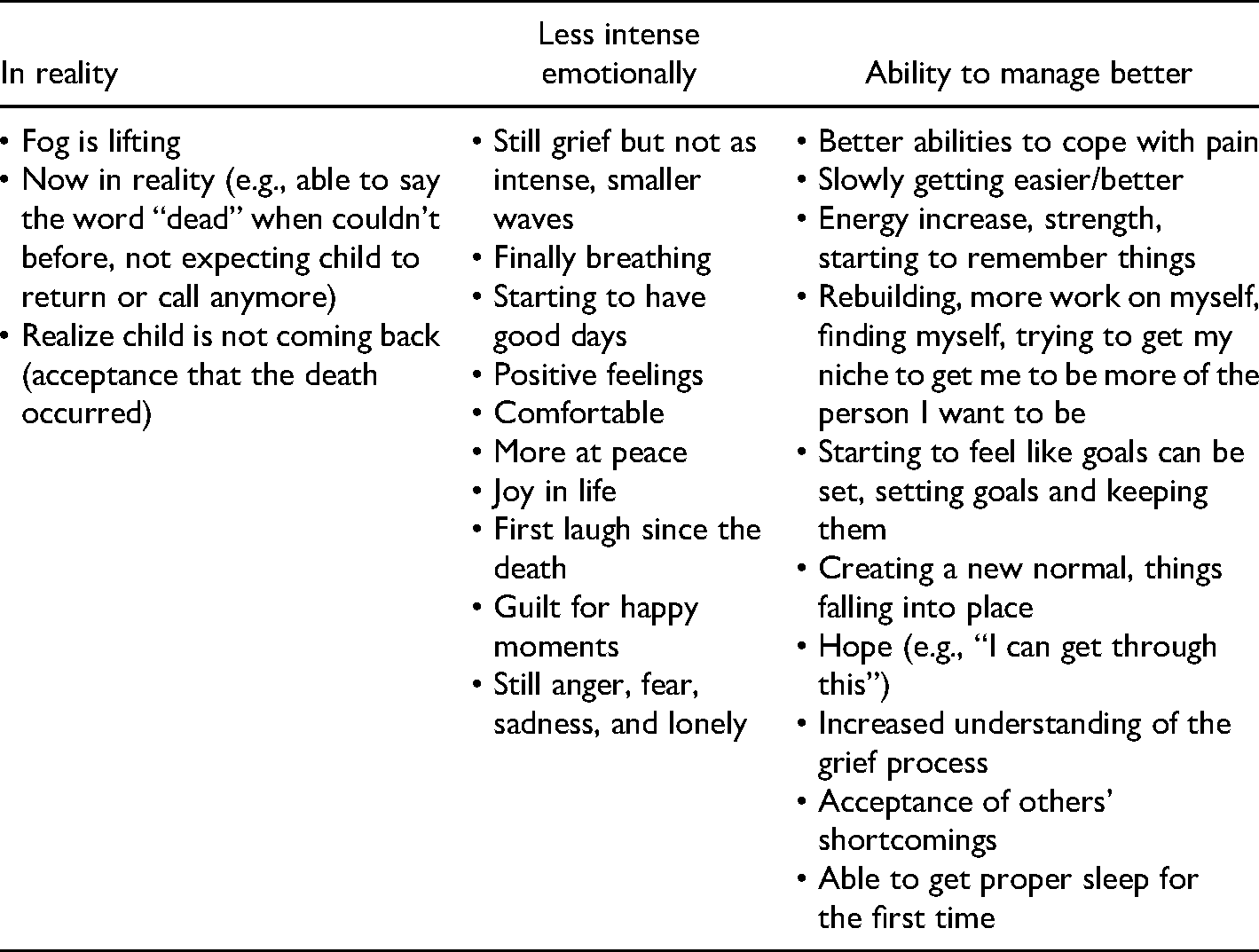
The very first time [I went out] … I thought, “Oh my God. I didn't think about [child], for a whole hour.” When you weren't thinking about her it was a big [emphasis added] deal. And then you felt guilty about that. You start to learn just to take that pain in spurts. So, you need to do that, you can't do it non-stop 24-7.
They described appearing to an outsider to have “moved on,” but continuing to have significant challenges as they transitioned to an unknown state: “it was probably a year before I could tell the whole story without getting too upset but then there were times when it was difficult again.”
For some participants, regardless of whether they had attended the local support group, the marked shift to transition coincided with a return to work or some other major life event such as a subsequent pregnancy, the birth of a grandchild, or a wedding. However, there were some exceptions. One participant whose child had died decades earlier, and who had not received any supports, seemed to still be in this phase describing her current state as “tired, comparisons, wondering.” One participant described “hell” lasting for 4 years. One participant who had not yet reached the 4-year mark was still in this phase and had not yet experienced what others described as following this phase. What was helpful was now being able to do some of the things they previously enjoyed doing, continued support from service providers, and the friends and family members who understood. During this state, holidays and the deceased child's birthday were especially difficult. People saying “stupid” and “insensitive” things continued to be unhelpful.
New Beginnings
As shown in Table 5, “new beginnings” was a time when the bereaved parent was no longer preoccupied with the death: now able to focus on redefining themselves; experiencing more good moments than difficult moments, and no longer feeling the guilt associated with good moments; and capable of having compassion for others. Participants expressed not needing as much outside support such as the local bereavement program. For those who had attended the local peer-support group, this period typically occurred after the third anniversary:
Participants’ Keywords for New Beginnings.
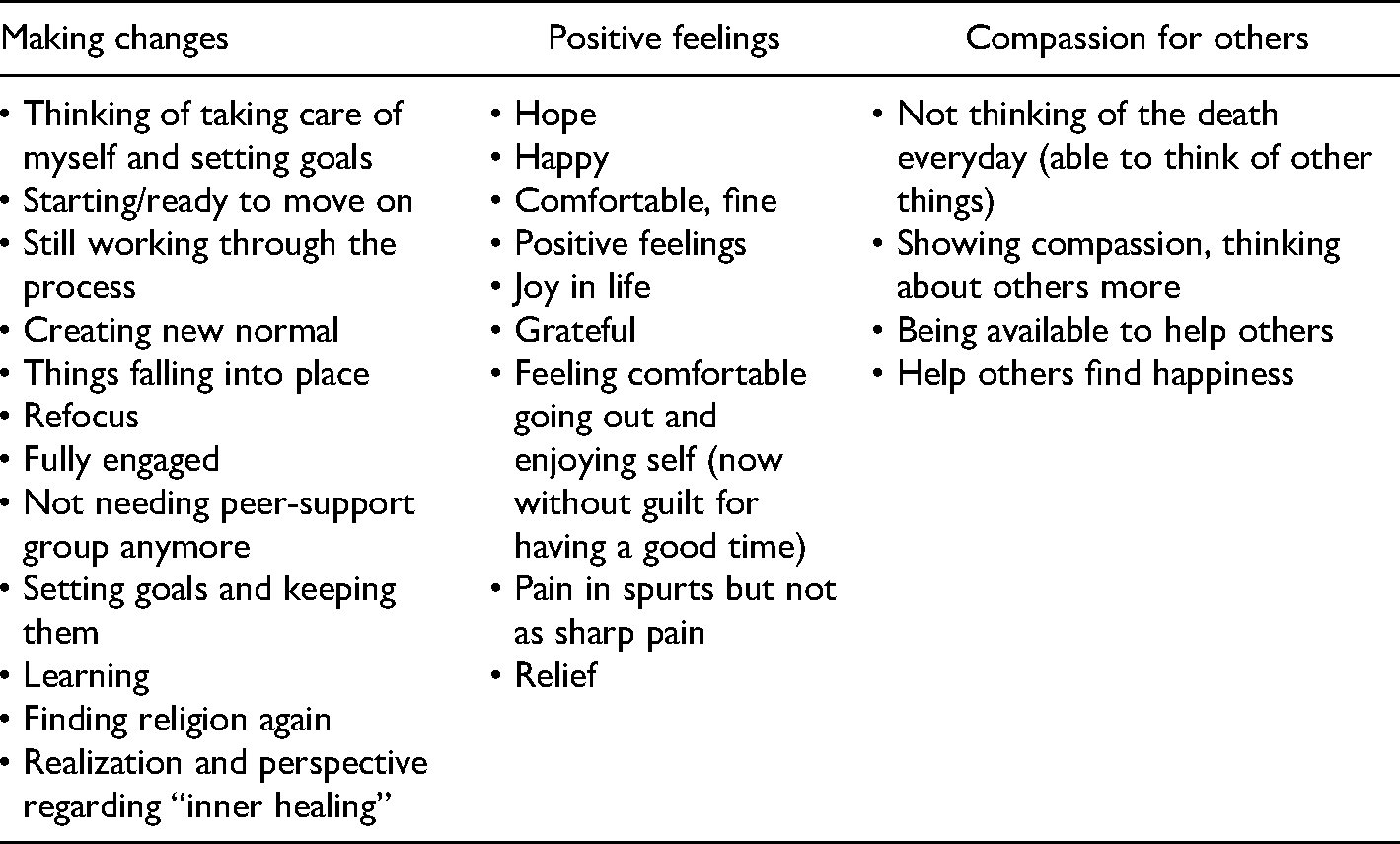
The shift in my actually feeling better about myself, wasn't until I went to the therapist [in the] third year …. I did have some days in between that were not bad. I don't want to appear that I was like that every single day. Some days I was okay. There was no joy, but I could live through the day without, you know, being really too, too, bad. But, as far as feeling joy, I can honestly say it was after that.
What was helpful was now having a better understanding of the process, not breaking down at the cemetery or when hearing their child's name or seeing reminders of their child. For some, it was helpful to now be able to help others. Now the “stupid” and “insensitive” things people said were expected and not as harmful.
Stability
Around 4 years after the death, cognition, emotion, behavior, physiological responses, spirituality, and interpersonal relations had stabilized for most bereaved parents. As shown in Table 6, participants described feeling more comfortable and content, and able to now enjoy life. Instead of a “stabbing pain” and “crying” if they saw a photograph of their child, they now smiled and thought fondly about the memories. One of the contributing factors to this comfort and ability to experience joy was the continuing bond they maintained with their child (described by all but three who had not attended the local support group). For example, one parent stated,
Participants’ Keywords for Stability.
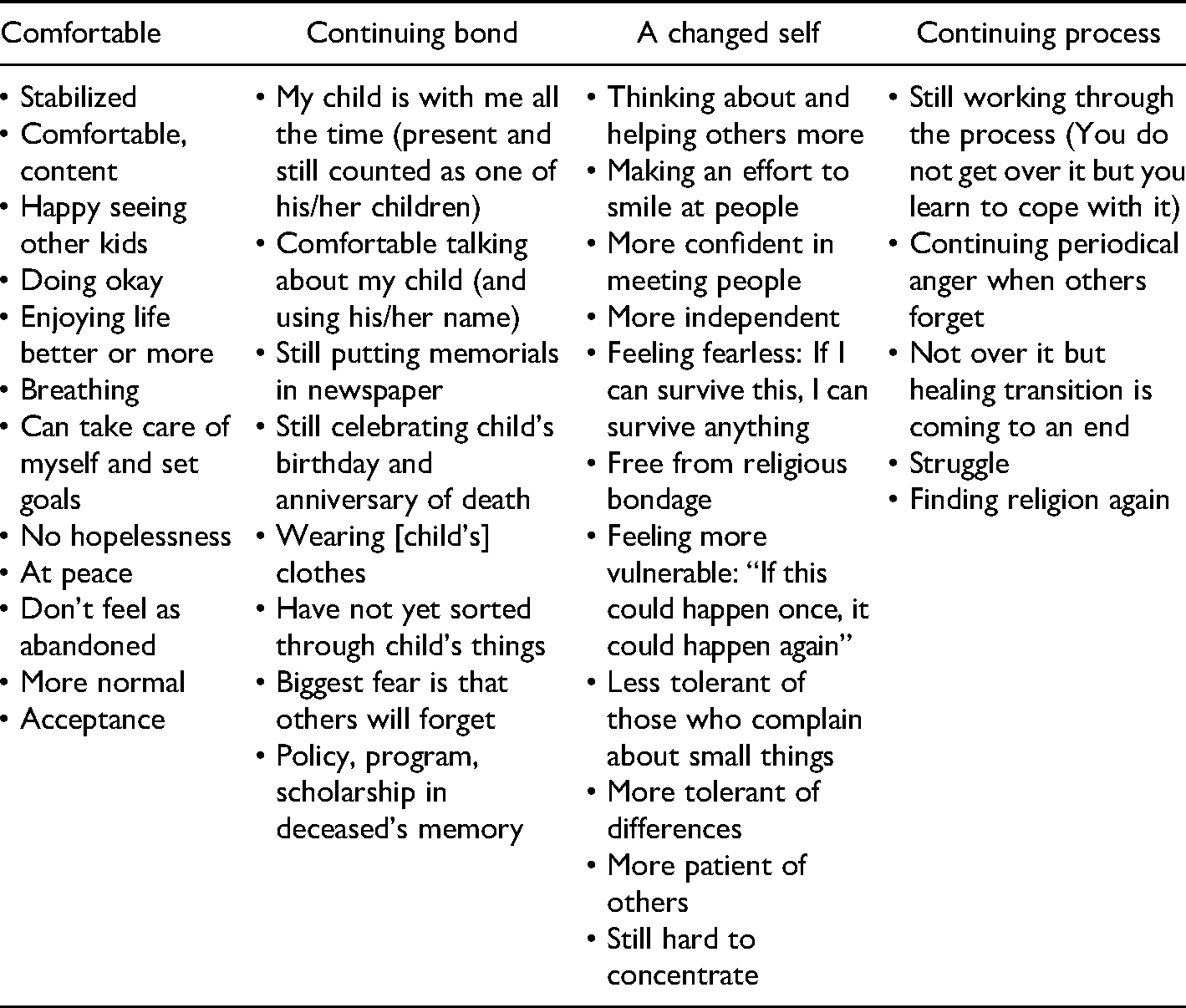
I can remember when he first died and I read all those bereavement books and the first time I read, “You will still have a relationship” I thought “How ridiculous is that? I’ll have no relationship. He's not here. How can I have a relationship?” But now I understand. I do! I talk to him all the time. I told him I was coming here and asked him to help me get through this. I talk to him all the time. It's like he's right there with me. And that's comforting.
All participants described now being a changed person in ways such as: being more considerate of, and having more compassion for, others; having more confidence and independence, yet feeling more vulnerable in some ways; and levels of tolerance, patience, and ability to concentrate. For example, one participant indicated,
My perspective has changed. Some things don't matter at all anymore. Like, I don't care if the dishes are done, or if the house … well we used to have to clean every Saturday. But it doesn't bother me now. My priorities have changed. People are my priority now because I know there is a lot of pain out there and that just helps to know that people can smile at you or do something for you.
Some described relations that had previously been strained because of the death, now stabilizing. For example, one participant who had considerable strain in her marriage indicated,
We’ll never be the same. That's the sad part. We can't. We can have fun together and we do stuff together … but it was very difficult until I found my way back. And, um, when I went to the doctor's there, a few months ago, he asked me how we were doing, I said, “We’re doing great! We’re okay.”
While almost all participants described having “moved on” or were at a point of “arriving,” they all spoke about: still (years later) trying to understand, there still being some disbelief, and continuing to change. Participants expressed surprise that the process seemed to be endless. As one participant indicated 12 years after the death,
I know some people say I am stuck [emphasis added] in my grief but I don't really think I’m stuck in it. I just think you never really do get over the death of your child. You learn ways to cope with it. And that's all I can say. You learn ways to cope with it.
Most described continuing “griefbursts”: “you would think it would be done by nine years but … there's still new stuff coming up.” The difference was that these griefbursts were now manageable. One participant indicated now looking forward to griefbursts because those were moments that helped in preserving the memory of their child.
While most bereaved parents in this study reached a point of stability around 4 years after the death, three participants were still very much struggling at this time, possibly due to other crises that had emerged that had set them back to an earlier state. In some instances, it seemed that an emotional downturn after previously feeling that things were going well was a natural part of their process:
I don't know what happened to me in the fourth year. … I thought I had made progress, and then … I thought, “Geez!” You know? “I feel like I’m starting all over again. I really don't know why. … I need more help than just the [local support group] can give me.” … I was getting a lot of headaches. I remember that. I never used to get a lot of headaches. … I was struggling with religion: I wonder if there really is a God? I wonder if there really is a Heaven? … Still questioning.
Discussion and Recommendations
In terms of the bereavement process, the findings seem to be most comparable to the four phases described by Parkes (1970): “numbness,” “yearning,” “disorganization and despair,” and “reorganization” (p. 196). The findings also fit with Stroebe and Schut’s (1999) dual process model consisting of two categories of coping: the states of helplessness prior to the death, fog, and turmoil were aligned with processing the loss; transition, new beginnings, and stability were aligned with restoration.
A few authors speak to the time before the death. However, examples such as Stroebe (1993) referring to, “going over the events before and at the time of death” (p. 19), are in the context of “grief work,” rather than the context of the time prior to the death forming part of the bereaved parent's bereavement narrative. What Parkes (1970) and most other stage or process theorists do not include in their description of the phases, is that the period prior to the death, at least for these participants, is part of the bereavement process narrative and hence part of the process. This serves as a reminder for service providers to be cautious about how they speak to and work with family members before and after the death, as their behavior can have serious lasting impacts.
Although some researchers have reported that bereaved people may seem to have improved and be high functioning, only to later experience a second downturn (e.g., Rando, 1983), only a few theorists, such as Imara (1975; one of Kubler-Ross's students) and Parkes (1970), have included similar findings in their process models. In this study, this ‘second downturn’ was described during the transition period when the bereaved parent began to make changes and experience joy but felt guilty about doing so. This finding is important for service providers, employers, friends, and family to be prepared for challenges to arise even after it seems the bereaved parent has “moved on.” For counselors, this may mean offering booster sessions or continuing counseling/treatment at a later point. For employers it may be allowing for mental health days off (especially around the birthday and anniversary of the death).
As described above, our findings are consistent with Denhup’s (2017) finding that bereaved parents “enter[ed] a new ‘state of being’ that exists the remainder of one's life” (p. 350). However, our findings add that within this new “state of being,” there are substates that occur and that shift over time, sometimes even flipping back and forth: helplessness prior to the death, fog, turmoil, transition, new beginnings, and stability. Service providers and program developers should be aware of these different substates so they can strive to respond appropriately to the bereaved parent, depending on where they are at in their process. Using anniversary dates as the determination of where clients are at in the process is unjustified and risks contributing to society's expectation that there is a specific timeline and point at which one should be “over it.”
Like other authors (e.g., Arnold and Buschman Gemma, 2008), we found that the bereavement process for bereaved parents does not end, and often includes a continuing bond with the child and occasional moments of grief, now lasting for a shorter period of time. However, we also found that there did seem to be endings to some states as bereaved parents journeyed through the process. Bereaved parents may, though, return to previous states or experience the states in different orders. Moreover, the experiences of a bereaved parent at any given time are not likely to be indicative of the experiences of other bereaved parents or even that particular bereaved parent at a different time. Hence, interventions and expectations must be flexible.
Strengths, Limitations, and Future Directions
A key strength of this study is that the voices of bereaved parents were heard and presented verbatim in the tables and quotes. Also relating to strengths, Dyregrov (2004), in Norway, found that 100% of the 64 bereaved parents who participated in research indicated that the research experience had been “positive” or “very positive.” Like the Norway participants, the bereaved parents in this study expressed an appreciation for the opportunity to tell their complete story (especially for some who previously had never had this opportunity) and they expressed hope that their contribution might be helpful to future bereaved parents. Further, targeting research participants who had lost their child at least 4 years prior to the study allowed us to hear about their bereavement process over a period of years, and sometimes decades, while most similar studies are limited to a given point in time or much earlier in the bereavement process. This allowed us to capture the full process, “arriving” at the point of stability and where continuing bonds had become strong. This study also provides a more holistic description of the experience as participants were asked to speak to cognitions, emotions, behavior, physiological responses, and spirituality. Social and relational experiences were also shared when participants were asked about what was and was not helpful. A common limitation of any retrospective research study is the accuracy of the findings due to the participants’ memory. For example, many participants found difficulty in isolating the bereavement experience as it was complicated by other occurrences in their life such as previous traumas, subsequent deaths, illnesses, and family breakups. The identification of specific timeframes was sometimes difficult because much of the experience seemed to blur together. In addition, aspects of the questions were challenging. For example, “It's hard to say about behaviours because you don't really look at yourself behaviourally.” However, this is to be expected in qualitative research. The fact that some aspects of the process may have been omitted does not minimize those aspects that were remembered and described. Moreover, remarkable consistency across participants was found despite this potential limitation.
Of note, the sample was quite homogeneous; all participants were from the same region, Caucasian, and predominantly Christian. Of the 20 bereaved parents, only three were fathers. Deaths were all due to accidents or illness. There were no deaths due to suicide or homicide. Given that this is qualitative research with the purpose of obtaining insights rather than generalizations, this limitation does not minimize the experiences of the participants but does suggest that future research is necessary to understand the process for other social and cultural locations, and geographical contexts. Further, this study did not explicitly ask about the social and policy aspects of the bereaved parent's experience, although a lot of this emerged in the data. To address the expressed concern about “stupid” and “insensitive” things people say, and misunderstandings about the process when a parent loses a child, we recommend that future research specifically examine societal influences and the dominant discourse about bereavement, such as how it is portrayed in the media and with sympathy cards.
Footnotes
Acknowledgments
The authors would like to thank the bereaved parents and service providers who participated in this study, as well as research assistants Michael Bennett and Shannel Butt.
Declaration of Conflicting Interests
The authors declare no conflict of interest in conducting this study or presenting the findings.
Funding
The author(s) disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a School of Social Work Director’s Fund and a Graduate Research Support Fund, both at the University of Windsor, Ontario, Canada.