
Abstract
This systematic review investigated the effectiveness of Acceptance and Commitment Therapy (ACT) for managing grief experienced by bereaved spouses or partners of adults who had received palliative care. Systematic searches were undertaken on seven bibliographic databases and grey literature was also searched. The review was informed by the use of the PICO framework and PRISMA-P guidelines. Initially 30 relevant papers were identified, but only two international studies met the criteria for inclusion. One was a qualitative, doctoral study using Interpretative Phenomenological Analysis; the other, a randomized controlled trial comparing ACT with usual psychosocial support. These studies showed some evidence of benefit for bereaved individuals, particularly by promoting the acceptance of troubling emotions. However, this type of therapy may be more effective in reducing psychological distress rather than grief. Further research is needed into the value of ACT in addressing grief following bereavement.
Introduction
Bereavement Following Palliative Care
Spousal/partner bereavement as a result of a death of a patient who received palliative care can impact negatively on well-being, especially where there is limited support (Ferrell et al., 2018; Holtslander et al., 2017). Considerable research has explored family carers’ experiences while their relatives were receiving palliative care, but there is a dearth of studies into their experiences following bereavement and how these might differ from the general population. Yet, grieving relatives can experience anxiety, depression, and post-traumatic stress disorder (PTSD) (Garrouste-Orgeas et al., 2019). Although many are able to adapt their emotions sufficient to engage in daily activities, for some grief can be long-lasting and result in prolonged grief disorder and even increased mortality (Maciejewski & Prigerson, 2017). Specifically, prolonged grief disorder (PGD) presents with emotional, behavioural and cognitive symptoms such as detachment, numbness, emptiness, yearning and searching, with a detrimental impact on quality of life (Ferrell et al., 2018).
Distress Requiring Clinical Intervention
There are many reasons why family carers should therefore be offered psychosocial support. Carers of adults receiving palliative care are often unprepared for the death of the person, resulting in high levels of psychological distress (Donorfio & Kellet, 2006; Thomas et al., 2014). Bonnano et al. (2008) found that such bereaved individuals often experienced acute depression from which they recovered within one to two years. However, 10-15% of them suffered chronic distress and depression for many years afterwards. This distress is likely being compounded by the spread of Covid-19, with families not knowing how they will be impacted by changing hospital or funeral practices which limit contact with their relatives before and after death (Wallace et al., 2020). Of course, a distinction must be made between people experiencing clinical and sub-clinical distress. Within the UK, anyone experiencing clinical levels of symptoms consistent with a diagnosis of depression, anxiety, panic, obsessive and compulsive behaviours and complex grief is eligible for mental health services treatment, typically provided by the National Health Service. People with sub-clinical distress can seek support from not-for-profit organisations or, alternatively, self-manage using online resources.
Palliative Care in the UK
The World Health Organization (n. d.) defines palliative care as an approach that improves the quality of life of patients and their families facing life-threatening illness, including via the early identification, assessment and treatment of psychosocial problems. Generalist palliative care is provided by health and social care professionals in all care settings, whereas specialist palliative care is delivered by specialist staff, particularly to patients with complex needs (including psychosocial) (NHS England, 2016). All palliative care services are mandated to provide psychosocial support to family carers, including bereavement support. Guidance from the
National Institute for Health and Care Excellence (2017) recommends that bereavement support should be offered after a death, but that it may also be needed before the person dies. However, there are significant barriers to delivering adequate support - including funding constraints, nursing shortages, high administrative workloads and the unprecedented challenge of COVID-19 - which, in turn, contribute to poor carer experiences (Holtslander, 2008; Morris et al., 2020; Radbruch et al., 2020). In addition, NHS England (2020) has stipulated that support, if any, following a COVID-19 related death should be provided remotely and usually only to inform families of the death. Therefore, carers - including spouses/partners - are likely to experience increased suffering (Radbruch et al., 2020). Hence, bereavement care is an under-developed aspect of palliative care services in the UK.
The Evidence Base for ACT
Acceptance and Commitment Therapy (ACT) is a form of cognitive behavioural therapy (CBT) which has been growing in popularity since its development in the 1980s (Hayes et al., 2004). ACT takes a non-pathologising view of mental health, assuming that everyone experiences challenges and distress in life. Whereas cognitive behavioural therapy focuses on the elimination of symptoms or modifying the content of thoughts, ACT supports people to develop the skills to experience unpleasant thoughts, feelings and sensations, whilst also creating a meaningful life in line with their values. As ACT is a transdiagnostic model, it is effective for a wide variety of mental health conditions and sub-clinical presentations, including subclinical anxiety and depression (Kohtala et al., 2015; Levin et al., 2014, 2017) and stress and burnout (Brinkborg et al., 2011; Flaxman & Bond, 2010).
There is a growing evidence base for ACT within palliative care where it has primarily been used with patients, with a developing literature on carers. Anticipatory grief, also known as pre-loss grief, is experienced when individuals or their loved ones are aware of their impending death and begin to grieve before the death has occurred; in carers it is linked to low post-bereavement adjustment (Nielsen et al., 2016). In a palliative care setting, patients’ acceptance was found to be the greatest predictor of anticipatory grief, over and above depression and anxiety (Davis et al., 2017a). As ACT promotes psychological flexibility, one study found that nine-weekly, individual therapy sessions alleviated distress and enhanced quality of life in a sample of 45 cancer patients, equivalent to CBT (Feros et al., 2011). In contrast, another study showed that six, individual therapy sessions for 25 people with cancer did not reduce their distress, possibly because of the brevity of the intervention and as it was delivered by phone (Mosher et al., 2019). With regards to carers, Losada et al. (2015) found that 8-weekly, individual, face-to-face sessions improved depressive symptoms among carers of people with dementia. A self-help form was an effective intervention for carers of people with MS (Potter et al., 2020), whereas web-based ACT was effective for carers of people with cancer (Köhle et al., 2015). In addition, a blended support program of face-to-face contact, telephone support and online modules based on ACT increased feelings of control in people caring for partners with Amyotropic Lateral Sclerosis and Progressive Muscular Atrophy (De Wit et al., 2020).
The ACT model of behaviour incorporates mindfulness, perspective-taking, cognitive defusion (stepping back from thoughts), acceptance, values clarification, and committed action (Hayes et al., 2006). Therefore, studies on the specific effective mechanisms of change can increase knowledge as to the potential value of this therapy. Research in the United States found that a mindfulness intervention significantly decreased symptoms of trauma, anxiety and depression following traumatic bereavement (Thieleman et al., 2014). Likewise, a study by Nam (2016) showed that experiential avoidance - a key target in ACT interventions - significantly mediated complicated grief after bereavement by suicide.
Gaps in the Evidence
To date, there has been limited research undertaken into ACT as a bereavement intervention for carers of people who have used palliative care services. In turn, there are few evidence-based strategies to guide health professionals in providing optimal support to carers after a patient’s death (Hudson et al., 2012). Therefore, we explore whether Acceptance and Commitment Therapy has been used as an intervention for bereaved adults whose spouses/partners had received palliative care.
Aim
A preliminary search for existing systematic reviews and/or scoping reviews on the topic was conducted. Within the UK, there are limited primary research papers and research syntheses available on this topic. Similarly, no other systematic review has been published or registered with Prospero or Cochrane which focuses on this particular topic. The aim is to understand the effectiveness of ACT for managing grief experienced by bereaved spouses or partners of adults who had received palliative care.
Using the PICO framework (Melnyk & Fineout-Overholt, 2005), this systematic review synthetises existing knowledge, identifies gaps in the literature and provide recommendations for future research. Note, whilst the registration of this review with Prospero stated that we would systematically compare ACT with other therapies, this was not feasible given the paucity of research on our specific topic.
Research Question
How effective is ACT in managing grief experienced by bereaved spouses/partners of adults who had received palliative care?
Secondary Research Questions
Is ACT effective in improving outcomes such as depression, anxiety, grief disorder and quality of life?
Is ACT more effective when delivered by a therapist or through online or self-help formats (or alternatively via a blended mode)?
Are there any socio-demographic differences (e.g. age, gender) evident in those who are offered ACT, or in its effectiveness?
Methods
A systematic review was deemed the most suitable method due to the research question proposed. This review follows the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) checklist (Moher et al., 2009). Therefore the Preferred Reporting Items for Systematic Reviews and Meta-analysis for Protocols (PRISMA-P) guidelines (Shamseer et al., 2015) has been used (Online Appendix 1).
Sample
The PICO criteria has been applied as follows (Melnyk & Fineout-Overholt, 2005):
Design
We included studies of any design (quantitative, qualitative, mixed-methods or professional practice articles)
Research Type
Qualitative, quantitative and mixed methods studies and systematic reviews and grey literature
Search Strategy
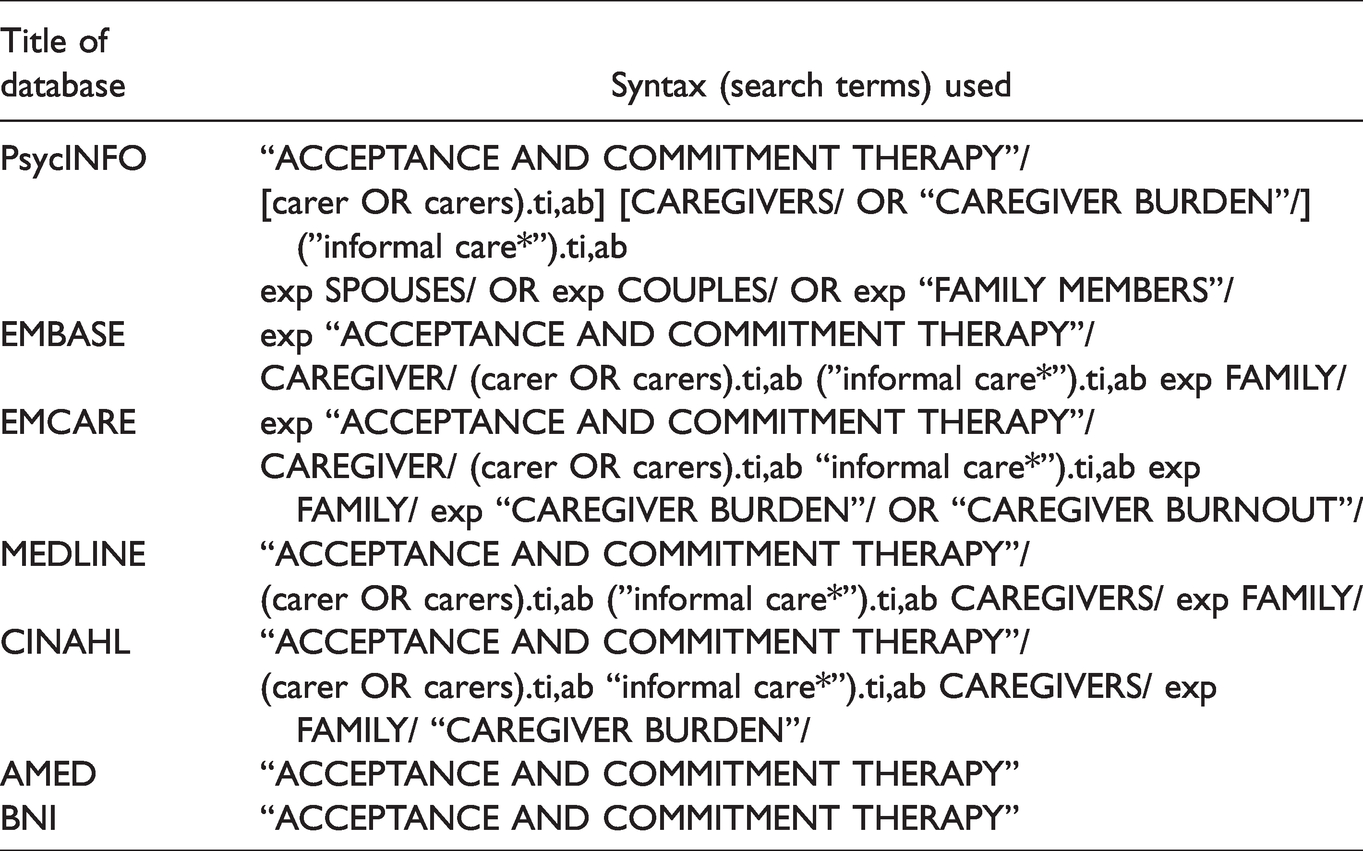
The search strategy was created by a specialist librarian, in collaboration with the authors. The search was limited to 1980 onwards to fit with the timespan when ACT has been in use. The language was limited to English only. The search, including the databases used, is shown in Table 1:
Databases and Search Terms.
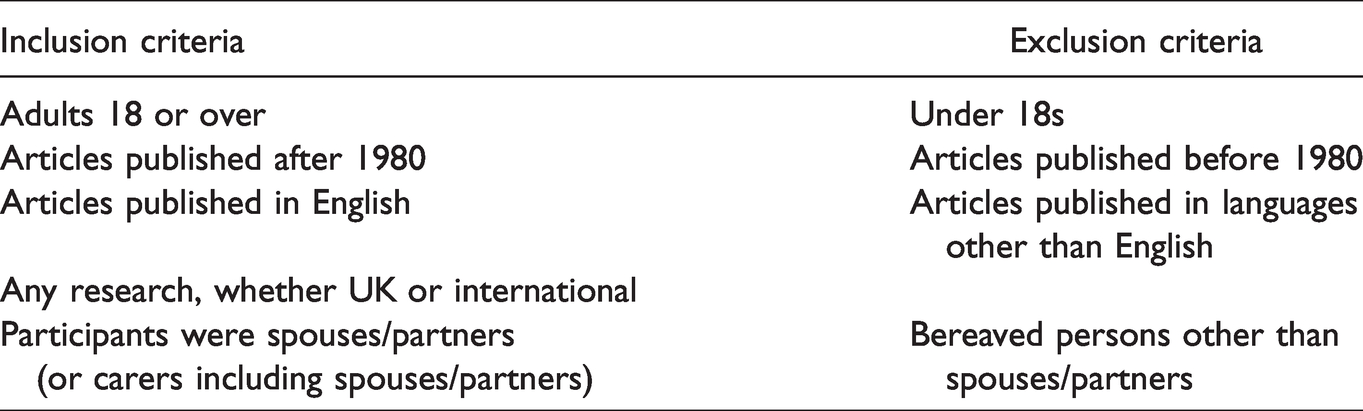
Inclusion & Exclusion Criteria.
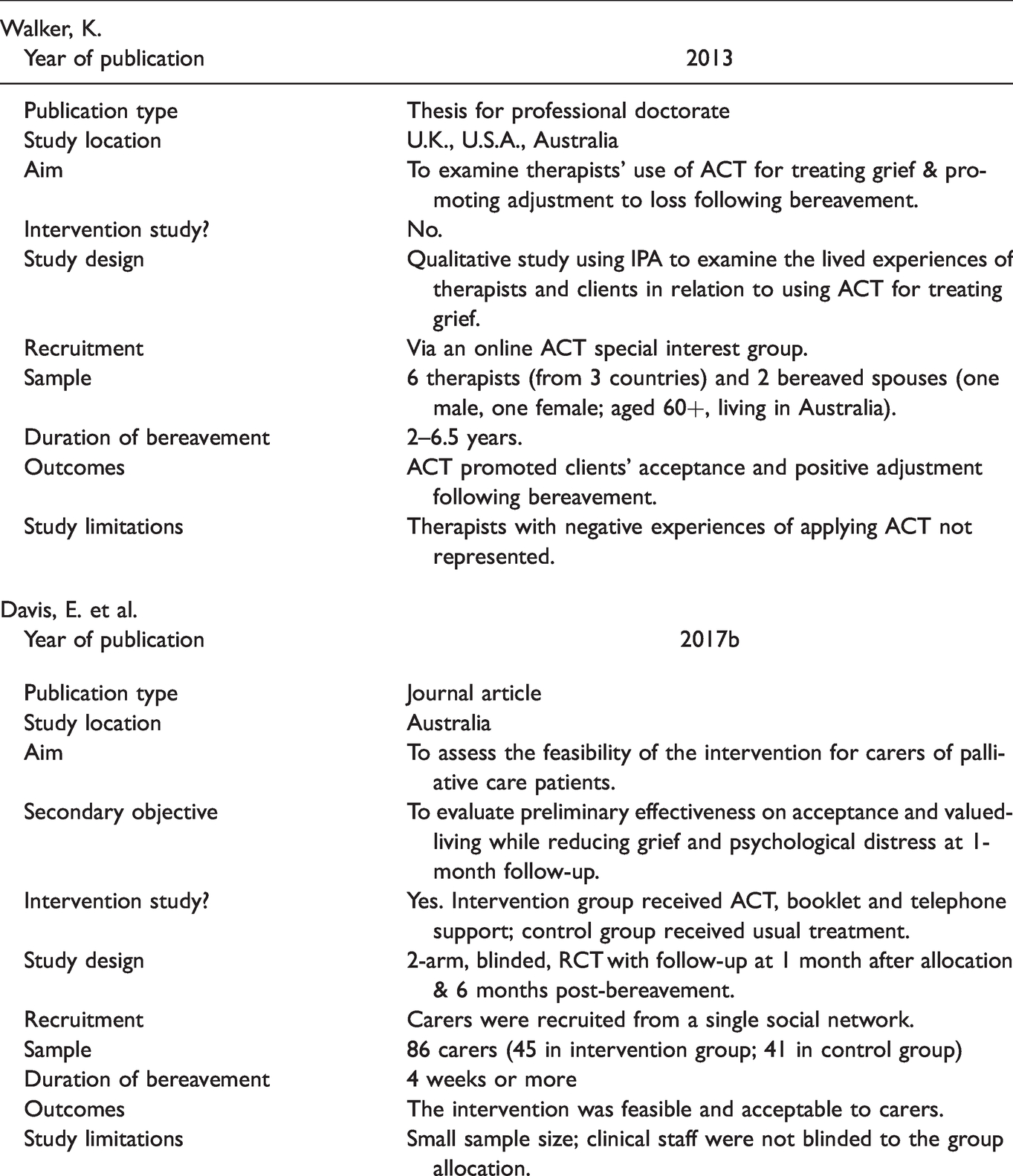
Key Characteristics of Studies.
Additionally, grey literature was searched using Open Grey, Google and Google Scholar. The search phrase “ACT and psychological therapies and managing grief by bereaved spouses/partners of adults who had received palliative care” was used to identify grey literature because these were identified as the most relevant terms in the exploratory and database searches. In addition, reference lists of all relevant studies, reviews and reports were searched.
Inclusion & Exclusion
Selection Process
Study selection (both at title/abstract screening and full text screening) was performed by three reviewers independently based on the inclusion and exclusion criteria (see Table 2). Any disagreements were resolved by the decision of another reviewer. After eliminating the duplicates (studies that were identified more than once by the search engines), an initial screening of titles, abstracts and summaries was undertaken to exclude records that clearly did not meet the inclusion criteria. Each record was classified as ‘include’ or ‘exclude’ or ‘maybe’ with comments to identify relevant texts and exclude irrelevant literature. The full texts were obtained for all records that potentially met the inclusion criteria (based on the title and abstract/summary only). In a second step, all the full-text papers were screened against the inclusion criteria, using a standardised tool. Studies that did not meet the inclusion criteria were listed with the reasons for exclusion. An adapted PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) flow-chart of study selection is shown in Figure 1 (Moher et al., 2015). Two papers met the inclusion and exclusion criteria and are outlined in Table 3.
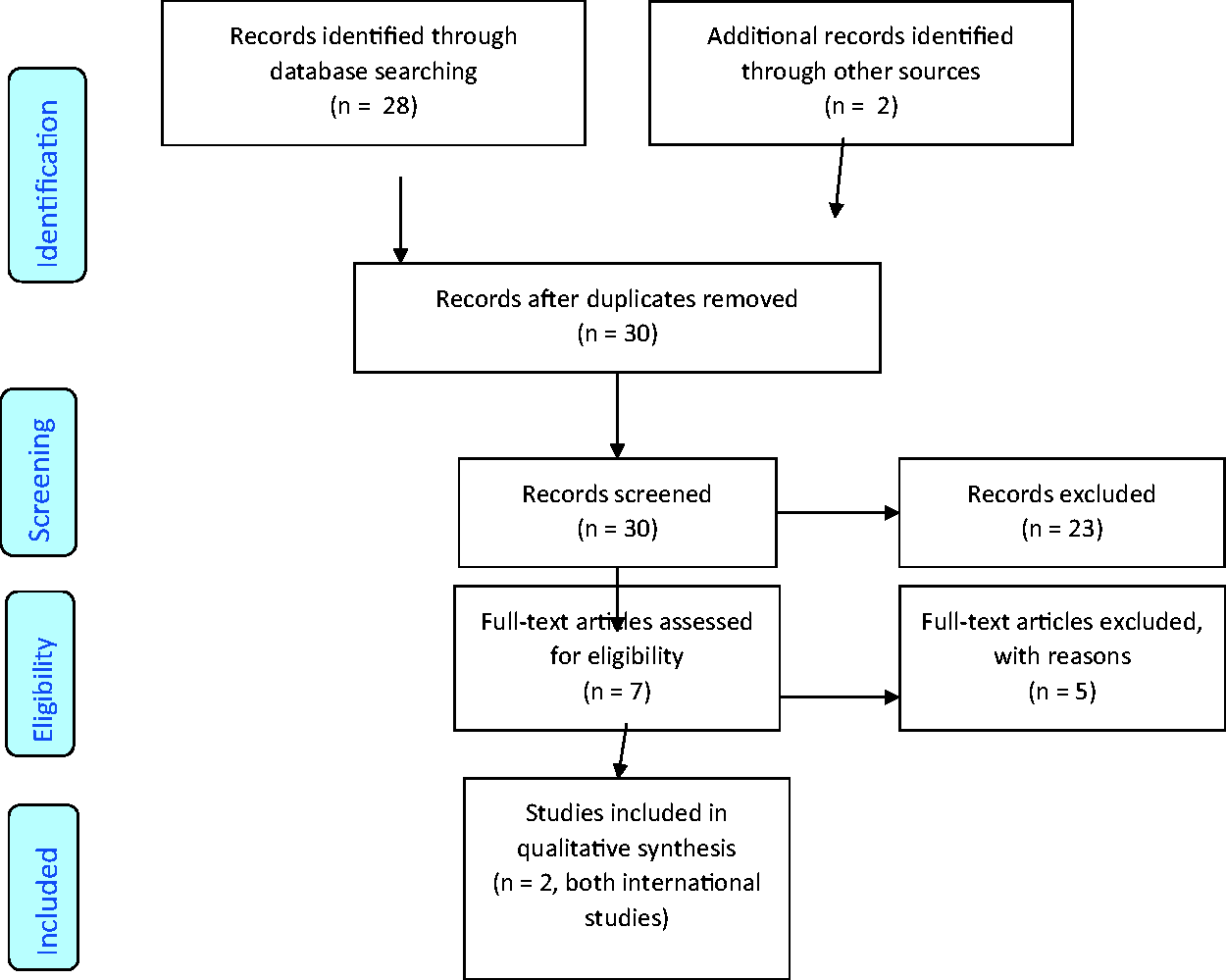
PRISMA 2009 Flow Diagram.
Data Extraction
Data for analysis were extracted from the included studies and managed in an Excel spreadsheet by two reviewers and any disagreements were resolved by a third reviewer. This included information on participants, interventions, comparators, and outcomes. The extraction sheet also contained authors, year of study/report, aim/purpose, type of paper (e.g. journal article, annual evaluation report etc), geographical location, study population (e.g. spouses’ ages and type of care provision), sample size, study design and key findings that related to the systematic review question.
Critical Appraisal
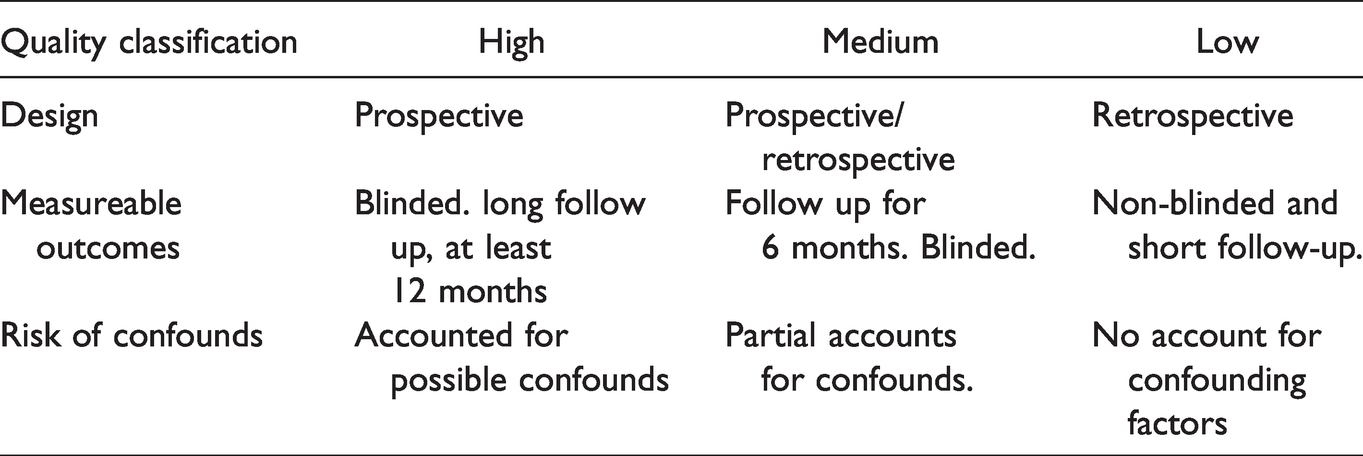
Typically in rigorous systematic reviews and meta-analyses quality assessments are implemented to ensure that only high quality studies are included. Table 4 details the quality assessment process used during the current review (Khan et al., 2003). Table 5 shows the quality ratings applied to the two studies. Due to the paucity of published research, the authors agreed to include the two identified papers, regardless of the heterogenic quality ratings. Whilst the critical appraisal found that the studies had gaps in relation to methodological quality and reported findings, they contain contextually-rich details that contribute to the overall narrative synthesis and address our research question.
Quality Assessment Applied to Included Studies.
Quality Assessment Grades for Included Studies.

Results
The initial database search returned 28 studies and a further 2 added from other sources, from which 7 publications were retrieved in full. However, upon closer inspection, studies which related to a healthy population (i.e. not experiencing clinically significant levels of distress) were removed. Studies which focused on palliative care patients only or where the types of the carer relationships - particularly whether these included spouses/partners - were not specified were also removed. Thus, 2 studies were included.
Data Synthesis
Findings from included studies have been synthesized narratively, using the ‘Guidance on the Conduct of Narrative Synthesis in Systematic Reviews’ (Popay et al., 2006). This involved describing the findings from the included studies in detail and organising them so that patterns and linkages or differences across the two studies could be identified. Given that there were only two studies, it was not possible to undertake a thematic analysis.
Descriptions of Included Studies
One study was a qualitative, doctoral study - undertaken in the UK, United States and Australia - which used Interpretative Phenomenological Analysis to examine the lived experiences of bereaved spouses and therapists who had used ACT to treat grief (Walker, 2013). The other study was a randomised controlled trial (RCT), conducted in Australia, that compared an ACT intervention for carers, including spouses, with usual treatment (Davis et al., 2017b). The aim of this review was to highlight the effectiveness of ACT in managing grief experienced by bereaved spouses/partners. The two studies (Davis, 2017b; Walker, 2013) indicate that ACT is generally feasible and considered to be an acceptable therapy for bereaved spouses/partners. Preliminary effectiveness analyses in the Davis et al.’s (2017b) study showed a small positive effect on acceptance, valued living, grief and psychological distress at 1 month and a medium effect on psychological distress at 6 months.
In the Davis et al.’s (2017b) RCT, eighty-six carers were assigned to an intervention or control group - of these 73% were female, including 38% who were spouses. Notably, the carers were recruited while the patients were receiving palliative care, but within the last six months of life. The control group (n=41) received treatment as usual (primarily psychosocial support from a social worker) while the intervention group (n=45) received ACT, a related information booklet and telephone support. The participants completed questionnaires at baseline, 1 month after group allocation and 6 months after bereavement. Key measures included the Acceptance and Action Questionnaire II (Bond et al., 2011), The Valued Living Questionnaire (Wilson et al., 2010), the PG-12 scale aimed at measuring anticipatory grief (Prigerson & Maciejewski, 2006) and the PG-13 to diagnose prolonged grief disorder (Jacobsen et al., 2010). At one month post-allocation, 14% of participants had accessed additional emotional support from a mental health worker, while 10% had accessed this type of support at 6 months follow-up.
Effect size calculations revealed that no, or a small, change occurred between baseline and 1 month after group allocation, while there was a medium effect on psychological distress at 6 months follow-up. Evidently, the initial period was very challenging for carers when they were only recently bereaved. The enhanced effect reported at 6 months also suggests that carers needed more time to engage with the content and experiential exercises contained within the booklet. At baseline, 29% of participants showed syndromal levels of anticipatory grief. However, 10% met the criteria for PGD at 6 months follow-up.
Seventeen participants provided data on the acceptability of the booklet and phone call, indicating that these were generally acceptable components of the intervention (mean 3.62; S.D. = 0.44). They reported that they would recommend the booklet to others, but the phone call was found to be more useful. Notably, the intervention was more effective in reducing psychological distress than grief (Davis et al., 2017b, p. 22). Importantly, positive outcomes were reported for acceptance and valued living, given that these are key mechanisms of therapeutic change. However, the limited extent of the changes suggested modification would be required in a main trial. The study was also limited by the relatively small sample size and the lack of blinding of clinical and research staff to group allocation.
In Walker’s (2013) qualitative study of 6 therapists and 2 older clients, ACT led to constructive experiences for the spouses. In particular, ACT facilitated them to deal positively with any undesirable thoughts and feelings, in contrast to CBT which requires clients to challenge their thoughts. The use of defusion techniques by the therapists helped clients to develop coping strategies to deal with challenging emotions such as anger and grief. The use of acceptance, mindfulness and present-moment awareness by the therapists assisted clients to manage their emotional states by embracing the truth of living without the deceased. Of particular benefit was identifying memories which facilitated a continuing bond with the deceased and assisting the clients to re-engage with life.
The therapists felt that ACT was more flexible than CBT in enabling them to situate suffering in an affirmative context, since ACT focuses less on symptom control. Indeed, the acceptance of strong or troubling emotions was considered a positive aspect of ACT as it normalises grief, as opposed to problematising it. While therapists also adopted other approaches - including Jungian therapy, dream therapy, and mindfulness - they felt that ACT enabled greater openness by their clients, such as a willingness to experience new emotions. For Walker (2013), ACT involved “less talking and more doing “which ultimately resulted in “less struggle for therapeutic change” (p. 134). A limitation of this study was that the therapists all reported positive experiences with ACT, which may not be the case for other therapists.
Discussion and Conclusions
The two studies show some evidence of benefit for bereaved spouses. Positive outcomes for acceptance were reported in both studies, including when compared to CBT. ACT promoted the acceptance of distress (rather than focusing on the control of symptoms), particularly by facilitating ways of handling difficult emotions. Additionally, ACT fostered spouses’ continuing bonds with the deceased (Walker, 2013). Yet, this type of therapy was more effective in reducing psychological distress than grief. Indeed, for a minority of participants who exhibited prolonged grief disorder at 6 months follow-up (Davis et al., 2017b), their grief was not relieved by ACT. The same authors recommended that textual guidance given to bereaved persons on applying the principles of ACT should focus more on resolving grief. However, the design and delivery of ACT itself within a bereavement context may require more fundamental adjustment in future research to address grief, rather than psychological distress. Correspondingly, emphasising the normality of grief appears to be particularly important. In addition, consideration should be given to whether ACT may be relatively more effective when initiated in advance of bereavement, by targeting anticipatory grief (Davis et al., 2017a). Since a minority of participants in the Davis et al.’s (2017b) study had accessed support from a mental health worker additional to the ACT, the therapy may not be adequate for some and/or the delivery modes may need adjustment.
Of course, caution is needed in interpreting the findings here, particularly as there were only two studies. In addition, methodological limitations - such as small sample sizes and the use of additional forms of therapy or support - may have led to any benefits of ACT being overestimated. Owing to the paucity of data it was not possible to explore whether the use or effects of ACT varied according to socio-demographic characteristics or which mode of delivery might be more effective.
Strengths and Limitations
To the authors’ knowledge, this is the first systematic review of the international evidence on the effectiveness of ACT as a bereavement therapy, notably when the deceased partner had received palliative care. Additionally, the review used broad inclusion criteria for the paper type (e.g. primary and secondary studies, guidelines, letters), resulting in an extensive literature search. As only two papers met the inclusion criteria, there is therefore a paucity of evidence relating to bereaved adults, highlighting the need for further investigation. Notwithstanding, this review has some limitations. We note that the Davis et al. (2020) paper reports on the same feasibility RCT study published initially in 2017b, which further highlights the sparse evidence base. As the review was limited to English language papers, this may have excluded other studies. Nonetheless, the review should inform palliative care commissioners and providers, carers’ and other support organisations about the potential value of ACT for enhancing the bereavement support given to spouses/partners and other family members.
Supplemental Material
sj-pdf-1-icl-10.1177_10541373211000175 - Supplemental material for A Systematic Review of the Effectiveness of Acceptance and Commitment Therapy for Managing Grief Experienced by Bereaved Spouses or Partners of Adults Who Had Received Palliative Care
Supplemental material, sj-pdf-1-icl-10.1177_10541373211000175 for A Systematic Review of the Effectiveness of Acceptance and Commitment Therapy for Managing Grief Experienced by Bereaved Spouses or Partners of Adults Who Had Received Palliative Care by K. Jones, A. Methley, G. Boyle, R. Garcia and J. Vseteckova in Illness, Crisis & Loss
Footnotes
Acknowledgements
The authors would like to acknowledge and thank xxxx Specialist Librarian, address for technical support in conducting searches.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This systematic review was funded by the main authors’ university.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.