
Abstract
While there are opportunities for families to fulfill leadership roles in early intervention, families often report feeling disempowered and unprepared to become leaders. To this end, in this pilot study, we evaluated the effectiveness and feasibility of an 8-hour leadership program for 20 parents of children who are receiving, or recently received, early intervention services. Participants demonstrated significant increases in early intervention knowledge and empowerment after completing the leadership program. The program had high attendance, low attrition, and high fidelity to the curriculum. Participants were overwhelmingly satisfied with the program and suggested a longer program duration. Initial efficacy and participant enthusiasm suggest a need to consider program implementation more broadly with the goal of increasing parent leadership and involvement in early intervention.
Family-centeredness is a core tenet of early intervention (EI; Dunst, 2007). Although families have been shown to advocate for their child during EI (i.e., Part C of the Individuals with Disabilities Education Act [IDEA]; Schraml-Block & Ostrosky, 2022), there are few studies examining systemic advocacy (i.e., collective efforts to impact change for individuals with disabilities) and leadership among families of children in EI. The limited research is problematic because of the many leadership opportunities during EI for families. For example, IDEA requires every state to have an Interagency Coordinating Council (ICC). Each ICC should be comprised of at least 20% parents of children with disabilities aged 12 and younger. Yet, in an interview study with 15 parents who served on their statewide ICCs across the United States, parents often reported feeling disempowered, lacking knowledge about EI, and struggling to advocate at the systemic level (Burke et al., under review). Other leadership opportunities may include serving as a parent liaison for families currently receiving EI services, acting as a navigator for families in EI, and/or providing peer support for other families (Dodds & Walch, 2022).
Although not explored in EI, there is research about the mechanisms which promote family capacity to conduct systemic advocacy. For example, in a study of 185 parents of transition-aged youth with autism across three states, Li and colleagues (2024) found that when families are more knowledgeable about special education services, more empowered, and conduct more individual and peer advocacy activities, they are significantly more likely to conduct systemic advocacy (e.g., taking on leadership roles). Other research has suggested that parent motivation to impact systemic change and parent perceptions of their roles as advocates can also influence capacity for systemic advocacy and leadership among families of school-aged children with disabilities (Goldman et al., 2017). Yet, most of this research has not focused on EI and the potential for a program to impact these mechanisms of change (i.e., knowledge, empowerment, advocacy activities, public service motivation, and role identity as an advocate). Importantly, in the context of advocacy for families of school-aged youth and adults with disabilities, knowledge, empowerment, advocacy, motivation, and role identity have been shown to facilitate systemic advocacy and leadership. Specifically, participation in 24-hour advocacy programs has been demonstrated to improve knowledge, empowerment, advocacy, motivation, and/or role identity which, eventually, have impacted systemic change (e.g., contacting legislators about disability policy, testifying in public hearings, pursuing leadership positions on statewide disability councils, Burke et al., 2016; Taylor et al., 2017). Thus, for this study, we conducted a pilot study of an Early Intervention Leadership Program for parents of children with disabilities.
At the most basic level, it is important to identify whether an Early Intervention Leadership Program can improve parent knowledge, motivation to impact change, role identity as an advocate, advocacy skills, and empowerment. For example, in an experimental study of a civic engagement program with 41 parents of school-aged children with disabilities, Burke and Sandman (2017) found that, after completing the civic engagement program, participants demonstrated significantly improved knowledge of special education, empowerment, and public service motivation; 6 months after the program, participants demonstrated significant increases in legislative advocacy for the next IDEA reauthorization. In a different study of an advocacy program for parents of school-aged children with disabilities, participants demonstrated greater role identity as advocates and comfort with advocacy which then led to greater advocacy for other families (Goldman et al., 2017). Both intervention studies suggest that knowledge, role identity, motivation, advocacy skills, and empowerment can change as a result of a parent education program and that such traits can eventually improve systemic advocacy and leadership. Unfortunately, none of the previous studies targeted parents of young children who receive or received EI services.
In addition, it is important to understand the feasibility of a leadership program for parents of young children with disabilities. To assess feasibility, it is important to address the fit between the intervention and the sample via program evaluation (Goddard & Harding, 2003). Put simply, if parents cannot attend a program or do not find it valuable, then the effectiveness of the program is irrelevant. Prior research about parent education programs has found that they are feasible for families of school-aged children and adults with disabilities to attend and families report being highly satisfied with the programs (e.g., Smith et al., 2012; Taylor et al., 2017).
Family-centeredness is key to EI. Furthermore, there are opportunities for families to impact systemic change in EI (e.g., participation on the ICC). However, many parents of young children with disabilities report struggling to impact systemic change (Burke et al., under review; Schraml-Block & Ostrosky, 2022). In this pilot study, we gathered preliminary data to understand whether an EI parent leadership program could impact mechanisms that may eventually increase family capacity for systemic change as well as to discern whether the program would be feasible among families. Our research questions were:
Method
Positionality
It is important to address our positionality as a research team. Our team includes four researchers. The lead researcher is the mother of a child with a disability who received EI services. Each of us has experience working as a practitioner with young children with disabilities. Our team also includes two individuals who reflect racial minority backgrounds. Furthermore, three members of our team are bilingual. Our collective personal and professional experiences contributed to this research and our values that families should be informed participants in EI.
Participants
To be included in this study, participants needed to meet the following criteria: (a) have a child, between the ages of birth and 10 years, who currently or previously received EI services, and (b) be a parent registered to attend an Early Intervention Leadership Program in a Midwestern state that was offered in English. The age range of 0 to 10 years was intentionally broad for two reasons. First, to serve on an ICC, a parent may have a child who received EI services and is between the ages of 0 and 12. Thus, we included parents of older children as they could still serve on the ICC. Second, this was a pilot study; we included a broader age range so we could explore interest in the program and have a larger sample. Regarding the second criterion, participants needed to indicate that they wanted to attend an Early Intervention Leadership Program to learn to impact systemic change. To determine whether they met the inclusionary criteria, individuals completed screening questions electronically via Research Electronic Data Capture (RedCap). If the individual met the inclusionary criteria, then they were directed to the online consent form. After providing consent, the participant completed the pre-survey. At the end of the pre-survey, participants indicated whether they would like to attend the Early Intervention Leadership Program on four consecutive weeknights or four consecutive weekday mornings. Overall, 59 individuals indicated interest in the Early Intervention Leadership Program, registered for the program, and completed the consent form. However, only 20 participants attended the first session of the program and, thus, were included in the final sample for this study. Two of the individuals who indicated interest but did not attend the program reported that the date/time of the program was no longer compatible with their schedules; other individuals did not report why they did not attend the program. Notably, there were no significant differences between the final sample and the full sample with respect to: gender, age, marital status, race, ethnicity, educational background, household income, child gender, child age, or child type of disability or delay (ps < ns). On average, participants were 39.0 years of age (SD = 7.80, range 28–58). All participants were mothers (100.0%, n = 20) and most were married (80.0%, n = 16). The participants primarily (70.0%, n = 14) identified as White. Of the children with disabilities or delays, the majority was male (60.0%, n = 12), and their mean age was 3.8 years of age (SD = 2.35, range 1–10). The most common types of disabilities were: developmental delays (65%) and speech and language impairments (65%); notably, participants could report having children with more than one type of disability (see Table 1).
Participant Demographic.
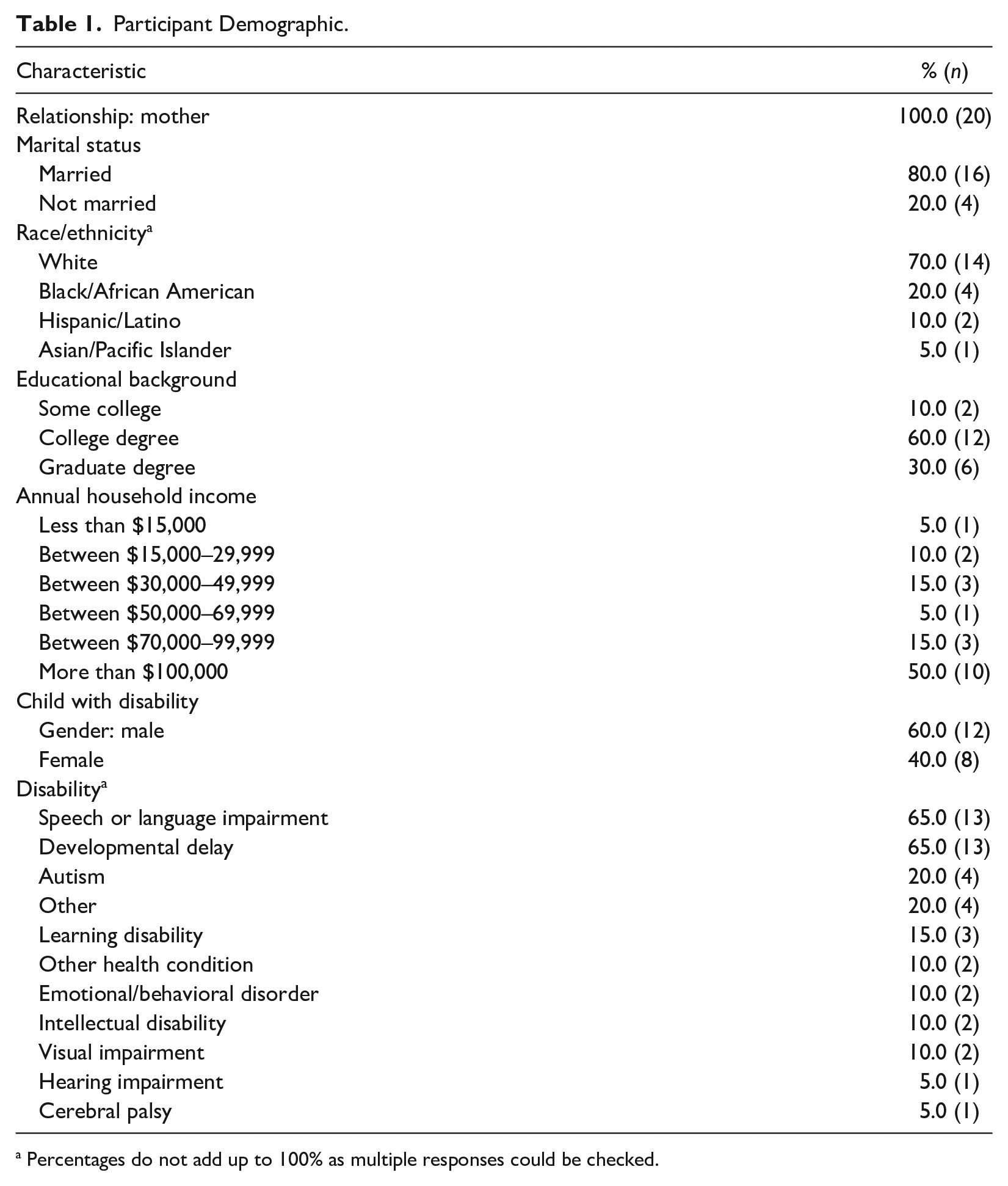
Percentages do not add up to 100% as multiple responses could be checked.
Recruitment
Participants were recruited in a variety of ways across the Midwestern state. For example, the recruitment flier was shared with EI providers, therapists, and parent and disability support groups. Sharing the recruitment flier with EI providers and therapists was intentional to reach families who were and were not connected to support groups. As this was a pilot study, no specific participant groups were targeted for recruitment; this study is based on a convenience sample. The recruitment period lasted for 6 weeks. Each participant received a total of $100 in gift cards for completing this study.
Early Intervention Leadership Program
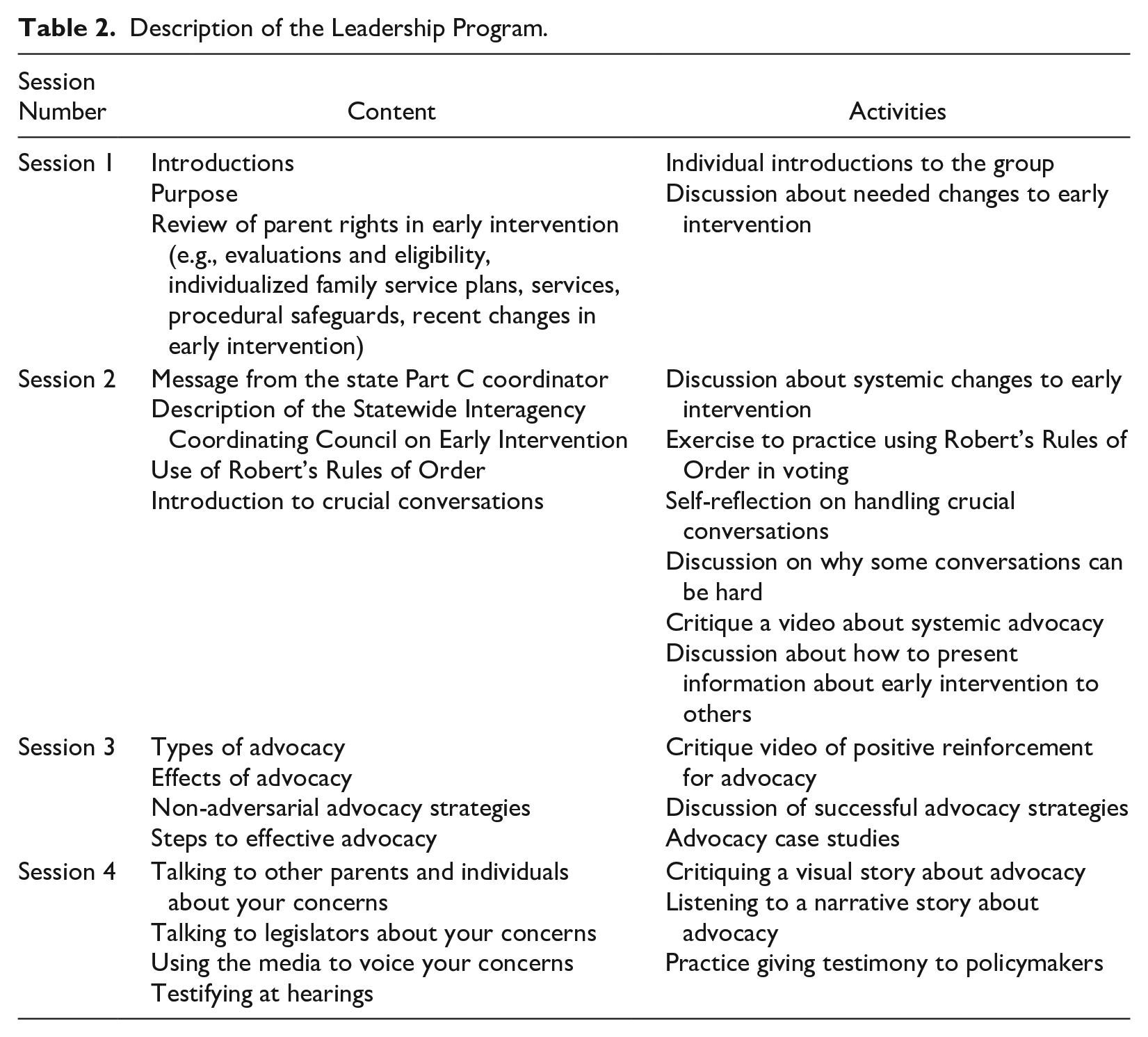
The Early Intervention Leadership Program was comprised of 8 hours of instruction (i.e., four 2-hour segments) facilitated over Zoom by the parent of a child who received EI services. Similar to most of the sample, the facilitator was a White, English-speaking mother of a child with autism who received EI services. The facilitator was also a professor of special education who conducted research about parent advocacy. We developed the Early Intervention Leadership Program by reviewing advocacy and leadership curricula from existing programs (e.g., the Volunteer Advocacy Project, Burke et al., 2016; the Civic Engagement Program, Rossetti et al., 2020; the Parent Institute for Engagement, Washington State Department of Children, Youth, and Families, 2023). Similar to existing programs, this program included content related to: creating an elevator speech; discussing concerns with other parents, legislators, and stakeholders; and advocacy. Also, this program is similar to other low-intensity programs which have demonstrated effectiveness and feasibility among families of children with disabilities (Luelmo et al., 2021). Unlike other programs, this program specifically focused on EI; thus, there was a review of parental rights in EI. Also unlike other programs, this program included a review of Robert’s Rules of Order and the role of the ICC. Prior to implementation of the program, two parents of children with disabilities (who were also emerging English language learners) and two practitioners gave feedback about the curriculum; minor changes were made (e.g., we simplified the language such as using the term “lawmaker” instead of “legislator”). The curriculum is available upon request to the first author (see Table 2).
Description of the Leadership Program.
Measures
Data were gathered using pre- and post-surveys to measure the effectiveness of the Early Intervention Leadership Program. To measure the acceptability of the Early Intervention Leadership Program, participants completed formative and summative evaluations. In addition, we (the research team) collected attendance, attrition, and fidelity data.
Pre- and Post-Survey of Effectiveness
To a large extent, the pre- and post-surveys were identical. Only the pre-survey included demographic questions about the parent and their child; this information was used to characterize the sample. The survey took 25 to 30 minutes to complete. The survey included the following measures.
Knowledge of EI Services
We created a 10-item measure about knowledge of EI services; the purpose of this measure was to gauge knowledge about EI. The research team created this measure by pooling their personal and professional experience in EI to identify basic tenets of EI knowledge. The team also created the measure by examining other measures about service delivery systems (e.g., the Special Education Knowledge measure, Burke et al., 2016; the Adult Disability Service Knowledge measure, Taylor et al., 2017). The measure was reviewed by practitioners and parents of children who received EI services to gauge the ease of wording. Each item has four multiple choice options; only one option was correct. A sample item was “How long after being declared eligible for early intervention should a child receive services?” In the state of this study, the law indicates that services should be provided within 30 days of being found eligible for EI. The total of correct responses was used as a dependent variable in this study; higher scores indicate more correct answers. The Cronbach’s alpha was .72.
Motivation
The purpose of the 14-item Public Service Motivation Scale (Perry, 1996) was to measure the willingness of the participant to provide services to others. A sample item was “I am prepared to make enormous sacrifices for the good of society.” For each item, there was a 5-point Likert-type scale ranging from (1) disagree to (5) agree. In this study, the sum of the items was used as a dependent variable with higher scores indicating more motivation. For this study, the Cronbach’s alpha was .91.
Role Identity
With five items, the purpose of this measure was to examine the extent to which participants perceived themselves as advocates (Goldman et al., 2017). Items were rated on a Likert-type scale from (1) strongly disagree to (5) strongly agree. A sample item was “I would feel at a loss if I had to give up advocacy.” The sum of the items was used as the dependent variable; higher scores indicate greater perceived identity as advocates. For this study, the Cronbach’s alpha was .83.
Advocacy
The purpose of the 16-item Advocacy Activities Scale (AAS; Li et al., 2024) was to measure the frequency of advocacy activities. Each advocacy item was rated on a five-point Likert-type scale. The AAS reflects the three levels of advocacy: individual advocacy (e.g., “I have searched the internet to find agencies and/or services to meet my child’s needs”); peer advocacy (e.g., “I have talked with other parents about agencies and/or services to meet their child’s needs”); and systemic advocacy (e.g., “I have written to lawmakers about disability issues”). The sum of each subscale was used as the dependent variables with higher scores indicating more frequent advocacy activities. In this study, the Cronbach’s alphas were .88 (individual advocacy), .87 (peer advocacy), .93 (systemic advocacy), and .92 (AAS total).
Empowerment
The purpose of the 24-item Family Empowerment Scale (FES, Koren et al., 1992) is to measure empowerment in relation to the family, services, and community. Items were rated using a five-point Likert-type scale. A sample item was: “I feel that I have a right to be informed of all services available and approve of all services my child received.” The sum of the items for each subscale was used as the dependent variables; higher scores indicate more empowerment. In this study, the Cronbach’s alphas were: .90 (family), .85 (services), .86 (community), and .94 (FES total).
Measures of the Feasibility of the Early Intervention Leadership Program
Attendance and Attrition
Attendance was calculated as the percentage of the total number of sessions attended for each participant divided by the total number of sessions (i.e., four sessions). Attrition was calculated as the number of individuals who completed the entire Early Intervention Leadership Program divided by the number of individuals who attended the first session.
Treatment Fidelity
Two research team members reviewed the fidelity to the intervention. Prior to implementing the intervention, the author of the curriculum created a checklist of objectives for each session; altogether, there were 22 objectives for the program. Two team members were trained by the first author about how to evaluate fidelity using the checklist; each team member had prior experience collecting fidelity data. A research team member watched a recording of each session and evaluated fidelity using the checklist, checking whether each objective had been met (i.e., indicating yes/no). In addition, a second research team member completed fidelity checks by watching the recordings for half of the sessions. On the treatment fidelity forms, both team members also had the option to include notes about treatment fidelity.
Acceptability: Formative and Summative Evaluations
On the formative evaluation, participants rated the sessions on a Likert-type scale with respect to: knowledge, presentation, relevance, duration, and satisfaction. On the summative evaluation, participants rated the entire program on a Likert-type scale with respect to: knowledge, relevance, sequence, and convenience. Also, for both evaluations, participants answered three open-ended questions: (a) “What did you get most out of this session/program?” (b) “What improvements would you suggest?” and (c) “Is there anything you wish this program had covered?” The formative and summative evaluations reflect evaluation measures used in previous programs (e.g., Pearson & Meadan, 2021).
Procedures
First, we received Institutional Review Board approval. Then, we recruited participants. After the end of each program session, participants were invited to complete an anonymous formative evaluation (via RedCap). After completing the entire Early Intervention Leadership Program, via RedCap, participants completed the session’s formative evaluation, the post-survey (which had identical measures to the pre-survey), and an anonymous summative evaluation.
Analysis
As a within-subjects research design, to determine effectiveness, paired t-tests were conducted between the pre- and post-survey scores. For the effect size, we used Cohen’s d wherein the magnitude of effect sizes was categorized as: small (.2), medium (.5), and large (.8). For the formative and summative evaluation data, we conducted descriptive statistics (e.g., means, percentages). For open-ended questions on the formative and summative evaluations, we conducted open coding (Creswell, 2013) and frequency counts of themes. Specifically, we had no a priori codes when examining the qualitative data. We used a word-by-word approach to provide codes to each piece of data. Each code was compared with existing codes to determine whether the new data reflected an existing code or a new idea. We reviewed the codes multiple times; then, we grouped the codes into categories and clustered the categories into themes.
Results
Preliminary Effectiveness
Table 3 shows the means, standard deviations, t-statistic, p-value, and effect size for each measure and subtest. Participants demonstrated statistically significant improvements on measures of empowerment (p < .01, d = .62) and knowledge (p < .001, d = 1.29). No additional statistically significant results were identified with respect to public service motivation, overall advocacy activities, and role identity; however, higher average post-test scores were noted on public service motivation, peer advocacy (subscale of the AAS), and systemic advocacy (subscale of the AAS; see Table 3).
Effectiveness of the Early Intervention Leadership Program (N = 18).
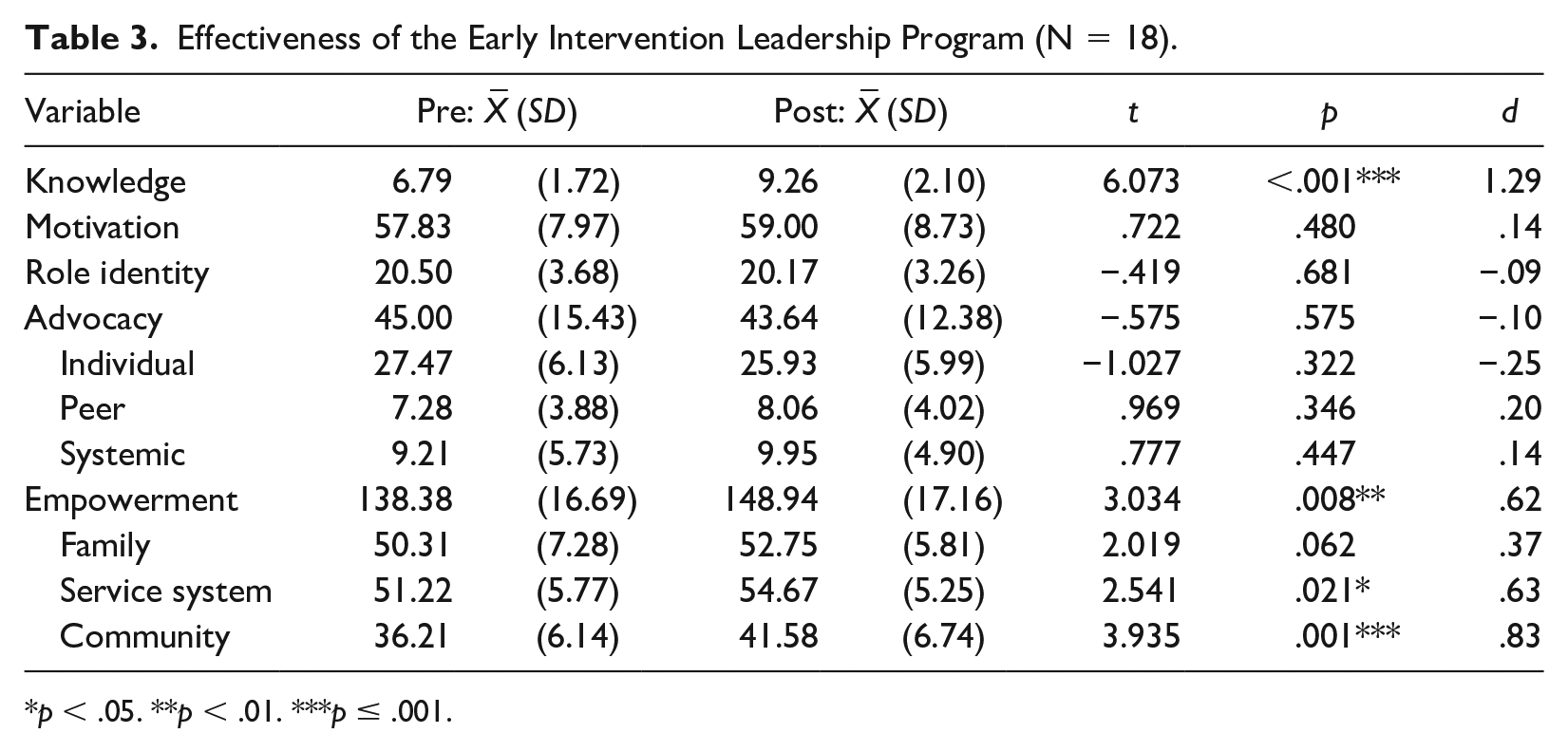
p < .05. **p < .01. ***p ≤ .001.
Preliminary Feasibility
Attendance and Attrition
Average attendance across all four sessions was 91.7%, with an attrition rate of 8.7%. Specifically, two individuals attended the first session but did not attend the remainder of the sessions. The two individuals reported to the program facilitator that their schedules changed and did not allow them to complete the program.
Treatment Fidelity
Fidelity was 100%. A second research team member reviewed half of all sessions and independently rated fidelity at 100%. Inter-rater reliability was 100%.
Acceptability
Based on the formative feedback, participants were satisfied with the individual sessions. With respect to duration, apart from the first session, more than 90% of the participants reported that the session was “just right.” For the first session, 11.8% of the participants reported the session was too long; notably, in this session, participants spent significant time introducing themselves to one another. Similar levels of satisfaction were observed with the summative findings. Nearly, 90% of the participants rated the presenter as having “excellent” knowledge. All the participants found the content relevant; almost 85% of the participants reported that the sequence of the content “always made sense.” Nearly, 95% of the participants reported being “highly satisfied” with the program. With respect to duration of the program, all participants reported that the sessions were “just right” (see Tables 4 and 5).
Formative Evaluation Results.
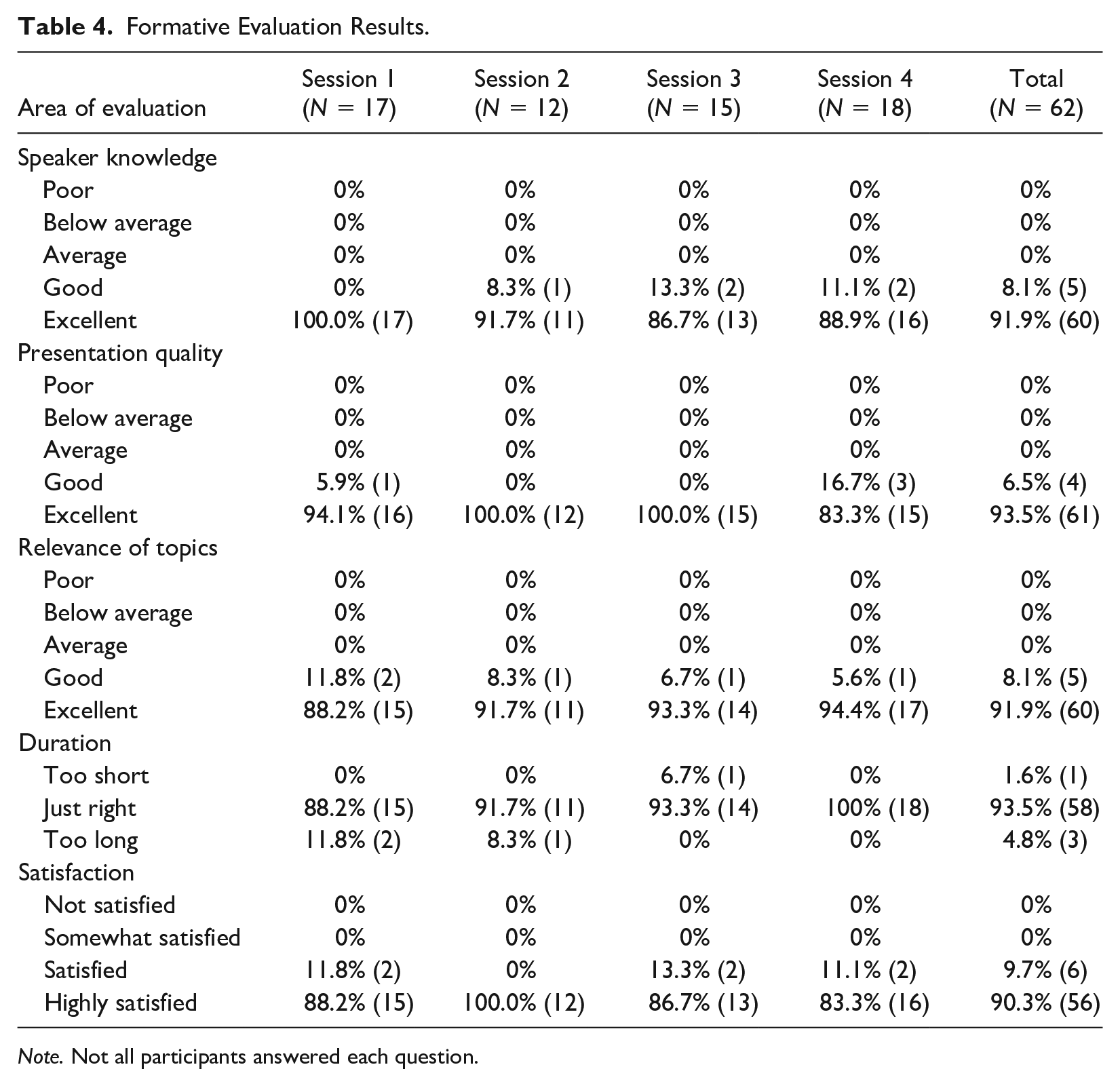
Note. Not all participants answered each question.
Summative Evaluation Results (N = 19).
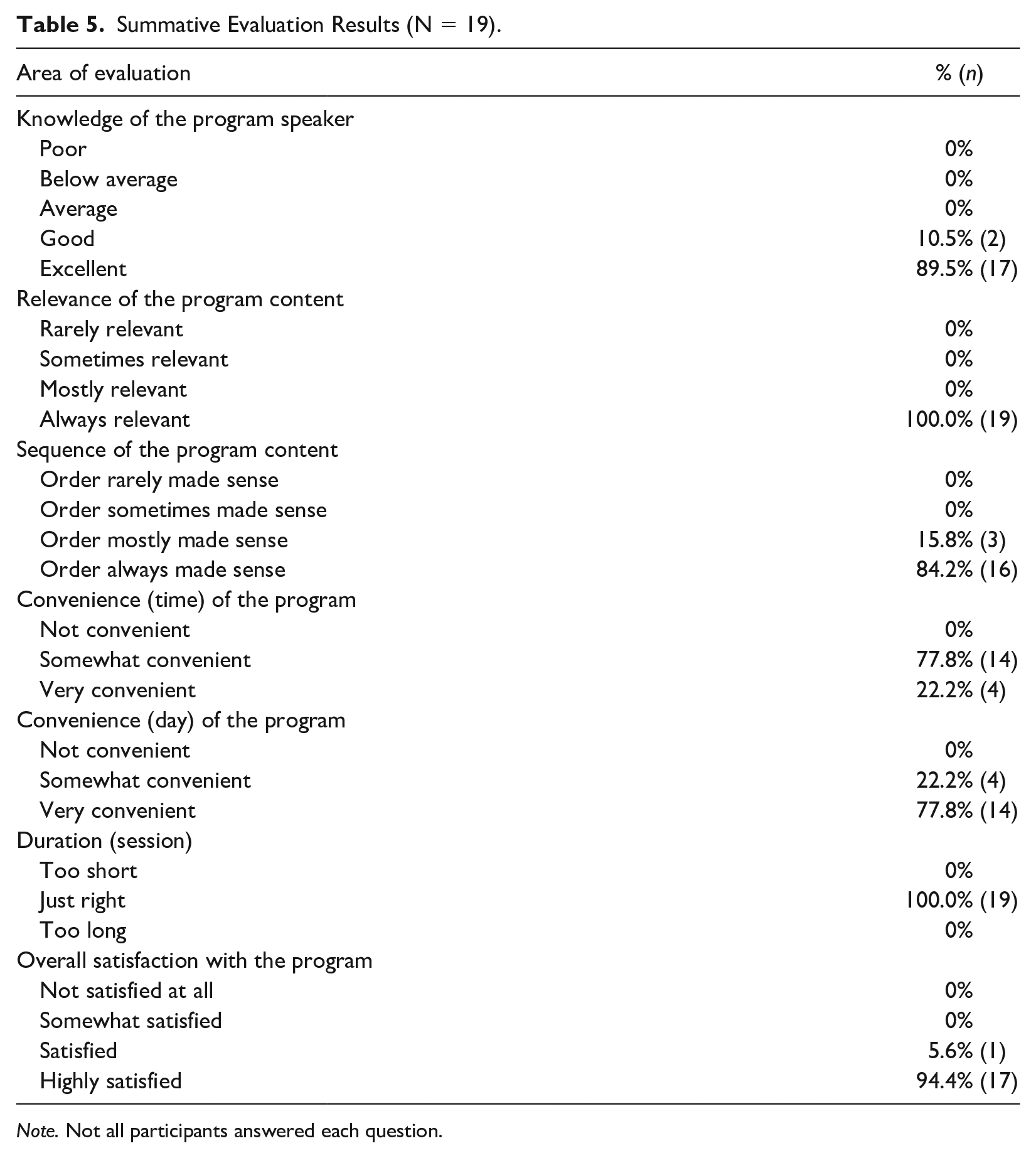
Note. Not all participants answered each question.
Acceptability: Participants Reported the Importance of Peer Support During the Program
The answers to the open-ended questions further underscore the acceptability of the Early Intervention Leadership Program. Across all of the formative evaluations, there were 21 comments about the importance of hearing other parents’ personal stories with EI. When asked about the most important aspect of the program, a participant wrote, “Everyone’s personal experiences. It’s so helpful to hear you’re not alone and the many different ways things have been handled.” Another participant reported, “The openness to listen to suggestions. Having a place to be heard but more so to share strategies for change.” Throughout the sessions, participants frequently commented on feeling disconnected and isolated from other families; the Early Intervention Leadership Program was able to offer a cohort to reduce loneliness: a participant wrote, “This [the program] was so amazing and so appreciative! I felt welcomed and accepted and not alone.” Participants appreciated meeting other families. A participant wrote, “It [the program] did teach me more on how to advocate but most importantly it helped me find a community of parents going through similar things.” Put simply, a participant wrote: “I learned a lot from both the trainer and the other participants.” Some participants wrote that the program should continue to be offered for more families: “Understandings other journeys-but how powerful would this be for all parents in EI [early intervention] . . . if they have this empowerment and training while their child was young.”
Acceptability: Increased Knowledge
There were 19 comments about the effectiveness of the Early Intervention Leadership Program in increasing their knowledge of EI. A participant wrote, “I thought I was pretty well rounded in knowing this information and I was WRONG! I learned so much on what is supposed to be done and who to go to. Thank you!” Another participant wrote, “I did not know exactly what to expect but this was just great! Every week new topics and things to learn.” Put simply by another participant, “I learned things I didn’t know before.”
Acceptability: Increased Advocacy
There were 16 comments about the program leading to greater advocacy among the participants. A participant wrote, “I had a good grasp on advocacy coming into this but now I feel so much more empowered to advocate specifically for EI services.” Another participant wrote: “Yes. I learned about many resources and how to confidently advocate.” A participant wrote that the program gave her the confidence to advocate more; she wrote “It was definitely a confidence booster and something I needed!”
Acceptability: Increase the Duration of the Program
Notably, the participants had some suggestions for improvements. The most common suggestion was wanting the program to be longer and/or sustained over time. Across the formative and summative evaluations, there were 11 comments about wanting more sessions. A participant wrote, “I do wish that this [the program] would have continued longer. I do hope there are refresher sessions or a check in that continues so we can continue to be informed.” Another participant requested, “More group meetings to come together and plan, but also to build up our community.” A participant wrote, “The only improvement I can think of is to have more than 4 sessions so we can try and build up a more tight knit community.” Another participant simply stated: “Continue to extend classes for strong advocates.”
Acceptability: Add Some Different Content of the Program
Across the formative and summative evaluations, there were some comments about the content of the program. Specifically, there were five comments requesting that the program includes information about the transition to school services. A participant wrote, “I would like to learn about the resources, training and navigating IEP [individualized education plan] for ages 3 and above.” One participant requested that the program be tailored to a child’s type of disability:
It would be nice to have more child-specific information. For example, if we had a training session specific to parents of children with ASD [Autism Spectrum Disorder] or more medically complex children, etc. I could see that level of specificity being helpful.
Furthermore, after the final session, one participant proposed, “Have a training video before it starts for parents about their rights within EI so they have fewer questions as the sessions happen.”
Discussion
While there are opportunities for family leadership in EI, parents often report feeling disempowered and unknowledgeable about EI to pursue leadership roles and impact systemic change (Burke et al., under review). To address the need to educate and empower families, we developed and tested the preliminary effectiveness and feasibility of the Early Intervention Leadership Program. We had three main findings. First, the program seemed effective in significantly increasing knowledge and empowerment. Future research should include a more rigorous research design (e.g., randomized controlled trial) with a sufficiently powered sample size to determine whether any changes can be attributed to the program (Campbell & Stanley, 1963).
Furthermore, more research is needed to determine the effectiveness of the program. For example, the non-significant findings (e.g., motivation, role identity, and advocacy) should be more carefully examined. It may be that the Early Intervention Leadership Program content should be revised to more carefully align with these constructs so there can be a significant effect. To that end, future research may examine whether interest and/or participation in leadership roles within EI (e.g., serving on the ICC) increased as a result of the program. Perhaps alternatively, future research may consider including a follow-up time point as there may be more distal effects on these constructs. For example, prior research has suggested that it may take up to 6 months to discern a significant effect on systemic advocacy (Burke et al., 2019).
Second, the program was feasible for the participants who attended the program. Many participants registered for the program indicating great interest among families. Of the participants who did attend the program, the attendance was high, and attrition was low. Notably, such attendance rates (>85%) and attrition (<10%) are consistent with extant advocacy programs (Rios & Burke, 2021). The combination of the high attendance, low attrition, and high fidelity suggests that the program is feasible.
Research is needed to understand why more than half of the individuals who registered for the program did not attend any of the sessions. For most of the participants, it is unclear why they did not attend the program. It may be that scheduling was a problem for the participants. Scheduling can be difficult for parent education programs. Scheduling the program during the day may disallow participation from working parents, whereas scheduling the program during the evening may be difficult for families of young children (i.e., the population of interest). By inquiring about why some individuals did not attend the program, we can identify and ameliorate barriers to participation.
Third, participants found the program to be acceptable as demonstrated by the high participant satisfaction ratings and open-ended comments. Notably, there was a disjunct between the quantitative and qualitative data on the formative and summative evaluations. Regarding the former, participants often reported that the duration of the program was “just right.” However, many of the open-ended questions requested additional sessions or ongoing offerings. There are two implications of this finding. First, it is important to collect quantitative and qualitative evaluation data to have a more comprehensive understanding of participant satisfaction. Second, participants were interested in attending more sessions—this could include adding more sessions to the program or offering more programs in the future.
Limitations
As a pilot study, there are several limitations that should be considered. There was no control group and a small sample for this study; thus, research is needed to attribute any changes to the program. Also, the program should be replicated in the community to determine whether it can be sustained by practitioners. Furthermore, there was a large drop-off from the individuals who registered for the program versus those who attended; research is needed to determine how to address this drop-off. Related to the sample, there was a drop-off in the sample size who completed the formative evaluation surveys; because the formative evaluations were anonymous, it is unclear whose perspectives were not reflected in these data. In addition, longitudinal data are needed to determine whether graduates of the program go on to fulfill leadership roles—the ultimate purpose of the program. Finally, the sample was primarily White, English-speaking mothers with college degrees. EI includes families of all socioeconomic, racial, and linguistic backgrounds; thus, the sample for this study is not reflective of the population of families served by EI.
Directions for Future Research
More research is needed to understand whether the Early Intervention Leadership Program could influence capacity for systemic advocacy among families. To do this, it would be helpful to include measures of intent to serve in leadership roles in the pre- and post-surveys to discern whether there is a change in intent. In addition, a follow-up survey after completing the program could ask about the systemic advocacy activities undertaken by the participants. In the same vein, it may also be helpful to examine the composition of parents serving on ICCs and whether this study’s sample is similar. To our knowledge, there is no national database showcasing the demographics of families serving on the ICCs. By having such information, we could discern whether ICCs are accurately represented by families of diverse backgrounds and target participation in the Early Intervention Leadership Program by individuals who are under-represented on the ICC. Altogether, future research should include gathering qualitative and quantitative data to understand the social validity and effectiveness of the program (Barton et al., 2018).
Another direction for future research is to identify moderators of effectiveness. For example, the duration of time a child spent receiving EI services and/or the recency of receiving EI services may impact the effectiveness of the program. Put simply, the length of a family’s experience in EI could moderate the effectiveness of the program. It could also be that the number of EI services received impacts family experiences in EI which could also moderate the effectiveness of the program. Future research should consider characterizing such traits and determining how they relate to the effectiveness of the program.
Implications for Practice
If future research confirms that the Early Intervention Leadership Program can result in improved outcomes for families of children with disabilities, practitioners may consider replicating the program. ICCs may consider offering the Early Intervention Leadership Program to families to develop a pipeline of parents who may eventually serve on the ICC. Parent Training and Information Centers (PTIs) may consider offering the Early Intervention Leadership Program to families of young children with disabilities. PTIs are federally funded agencies; there is at least one PTI in every state. While the PTIs serve more than 1.4 million families of children with disabilities annually, less than 5% are families of children in EI (National Parent Technical Assistance Center, 2016). The Early Intervention Leadership Program may be one way that PTIs can educate and empower families of younger children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.