
Abstract
It has been well documented that experiencing trauma impacts all aspects of child development. Young children experience trauma at high rates, and children with disabilities are at an increased risk of experiencing trauma. One way to mitigate the effects of trauma is through the implementation of trauma-informed care, which requires a well-trained workforce. Yet, to date, minimal research has been conducted about the professional development needs of early childhood special education (ECSE) teachers related to trauma. The purpose of this qualitative study was to understand ECSE teachers’ professional development needs related to trauma and trauma-informed care. Eighteen ECSE teachers participated in interviews. Results indicate that while ECSE teachers are familiar with the basics of trauma-informed care, more training is needed, specifically in the areas of working with families, implementing trauma-informed classroom strategies, and supporting children with disabilities who have experienced trauma.
Trauma is an “event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life-threatening and has lasting adverse effects on the individual’s functioning and mental, physical, social, emotional, or spiritual well-being,” (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014, p. 7). These experiences can include, but are not limited to, child abuse and neglect, natural disasters, loss of a loved one, and living in community violence (National Child Traumatic Stress Institute [NCTSN], 2013). It is estimated that one in two preschool-aged children have experienced a potentially traumatic event (Jimenez et al., 2016). Moreover, children who have experienced trauma are more likely to receive special education services (Sullivan & Knutson, 2000; Zetlin, 2006) and children with disabilities are more likely to experience trauma (Jones et al., 2012). The prevalence of trauma in preschool-aged children, combined with the relationship between disability and trauma, highlights the need for ECSE teachers to be prepared to implement trauma-informed care.
Trauma-Informed Care
Trauma-informed care is a term used to describe service delivery that integrates an understanding of the pervasive biological, psychological, and social outcomes of trauma with the aim of ameliorating, rather than exacerbating, their effects (Harris & Fallot, 2001; SAMHSA, 2014). Trauma-informed care is an approach to structuring the organizational culture, practices, and policies that are sensitive to and center the experiences and needs of individuals who have experienced trauma (McInerney & McKlindon, 2014). The recognition of the benefits of trauma-informed care in schools is expanding, along with an interest in using trauma-informed care in school settings (Cole et al., 2013; Mendelson et al., 2015; Overstreet & Chafouleas, 2016).
SAMHSA (2014) has identified the need for a well-trained workforce as an “essential” feature of providing trauma-informed care, believing that a well-informed staff reduces negative outcomes for children (p. 13). Therefore, it is imperative that ECSE teachers are prepared to support children with disabilities who have experienced trauma through the implementation of trauma-informed care (Corr et al., 2018; SAMHSA, 2014).
Special Education’s Commitment to Children Who Have Experienced Trauma
The field of special education has made a commitment to children with disabilities who have experienced trauma through the release of position statements (Council for Exceptional Children [CEC], 2018; Division for Early Childhood [DEC], 2016). These statements provide the message that special education teachers are responsible for supporting children who have experienced trauma. In addition, DEC’s (2016) position statement drew attention to the lack of support available to young children with disabilities or developmental delays that have experienced trauma. By doing so, it emphasized the critical role ECSE practitioners, researchers, and policymakers can play in protecting, supporting, and advocating for young children that have experienced maltreatment (DEC, 2016). Notably, the position statement advocates specifically for additional research to focus on the current knowledge base of ECSE professionals to further inform training and professional development opportunities.
Personnel Preparation Related to Trauma-Informed Care
There is a growing body of literature that focuses on the importance of trauma-informed care in schools (Chafouleas et al., 2016; Chu & Lieberman, 2010; Loomis, 2018). The field of early childhood education has begun to explore trauma-informed care and the importance of implementing it in classrooms (Dorado et al., 2016; Douglass et al., 2021; Holmes et al., 2015; Lipscomb et al., 2019; Loomis, 2018; Loomis & Felt, 2021; Whitaker et al., 2019). However, minimal research has focused specifically on ECSE teachers and their experiences with trauma-informed care. The studies that have examined ECSE professionals found they do not feel prepared to implement trauma-informed care (Chudzik et al., 2022; Miller, 2018). Moreover, Miller and Santos (2020) found that professional development opportunities regarding trauma-informed care for special education teachers are lacking. Before additional training and interventions can be designed to support ECSE teachers in implementing trauma-informed care, we need to understand their current knowledge and areas of need. This research study aims to meet this gap. Specifically, our research questions were:
What do ECSE teachers currently know about trauma and trauma-informed care?
What do ECSE teachers want to learn about trauma and trauma-informed care?
Methods
This research study is a smaller portion of a larger mixed methods research study that explored ECSE teachers’ attitudes toward and experiences with trauma-informed care (Chudzik et al., 2022). In this study, we examine only the qualitative data to examine what ECSE teachers know about trauma-informed care, and their professional development needs related to trauma-informed care. The primary researcher’s Institutional Review Board approved this study.
Conceptual Framework
We used SAMHSA’s (2014) concept of trauma-informed care to frame our study. This framework highlights four main components of trauma-informed care: (a) realizing the widespread impact of trauma, (b) recognize the signs of trauma, (c) respond by integrating trauma-informed care, and (d) resist retraumatization. In addition, it highlights the importance of a well-trained workforce being key to successfully implement trauma-informed care. In this study, the SAMHSA framework supported our overall aim of exploring ECSE teachers’ knowledge of trauma-informed care to understand their training needs to further improve the ability to implement trauma-informed care. In addition, we used the framework to inform the design of the interview protocol.
Positionality
The research team for this research study included the first author who identifies as a white graduate student in special education and two special education professors who also identify as white women. As first author, I leveraged my experience as an early childhood special education (ECSE) teacher and advocate of trauma-informed care when designing, conducting, and analyzing this research study. As researchers who work in an early childhood teacher preparation program, we used our natural connections and relationships to recruit participants for this study. In addition, as researchers and practitioners, we are keenly aware of and troubled by the ways in which race, trauma, and challenging behavior are interconnected in ECSE, and attempt to address this in our work.
Participants and Setting
We used a convenience and snowball sampling strategy to invite ECSE teachers from the United States to participate in this research study. A flyer was shared via email to school administrators and on social media that included a brief description of the project and a link to an online screening form. After participants gave their consent to participate, they were directed to an online survey. Participants could indicate interest in completing an interview by providing their email address at the end of the survey. Sixteen participants were recruited this way. In addition, two participants were recruited with snowball sampling, as previous participants recommended reaching out to them about participating in the study and provided their email addresses, making for a total of 18 interview participants. These participants were from four states, with most of them from one Midwestern state (n = 16).
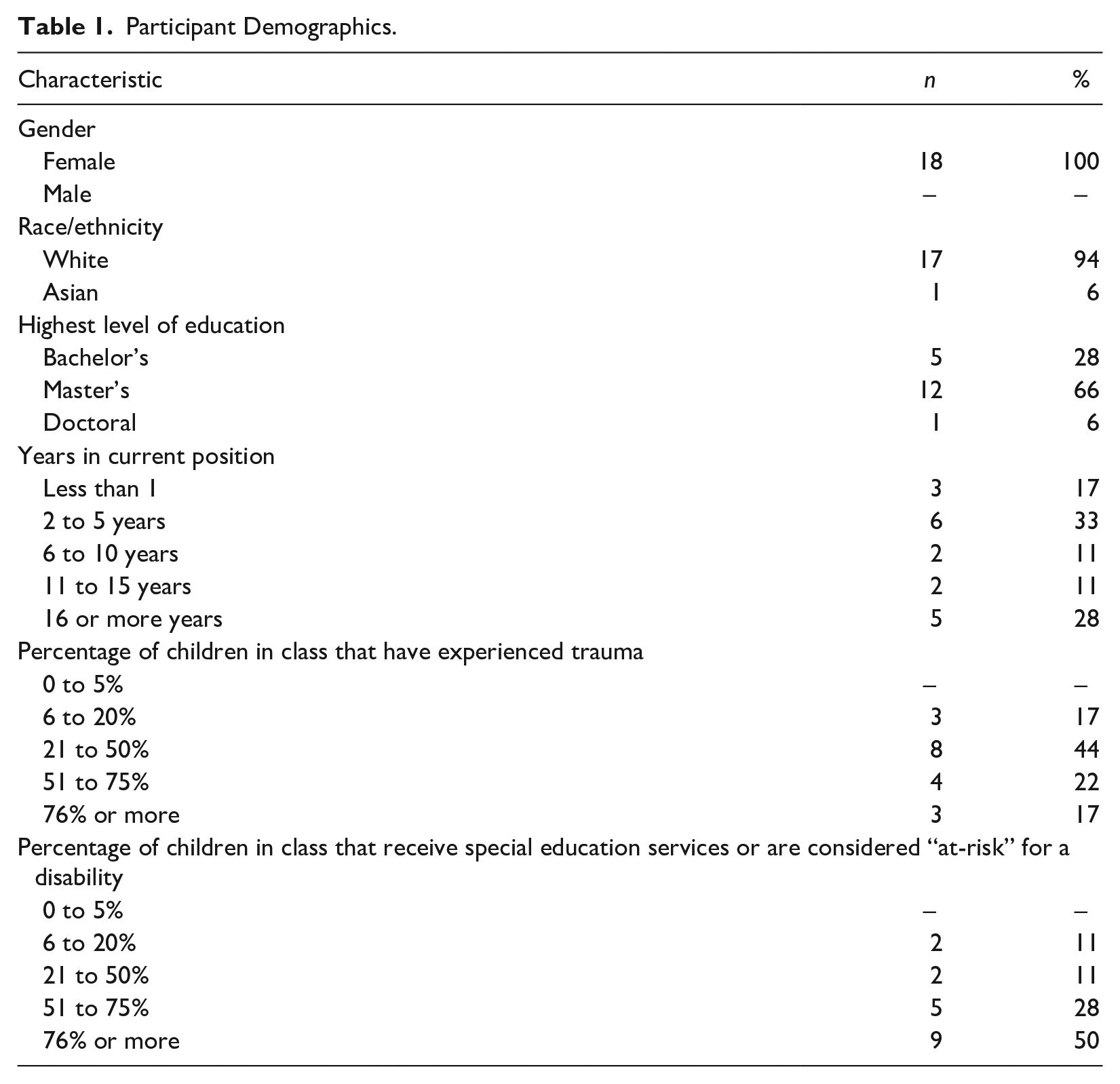
Eighteen ECSE teachers working in public ECSE programs participated in this study. All participants had at least a bachelor’s degree, with the majority having a master’s degree (n = 12). All participants reported having at least one student in their class that had experienced trauma, and seven estimated that at least half the students in their class had experienced trauma. See Table 1 for additional participant demographic information. Participants were automatically entered in a raffle to win one of three U.S.$25 Amazon gift cards.
Participant Demographics.
Interview Protocol
Based on professional experiences, SAMHSA’s trauma-informed care framework, and gaps in the literature, our research team developed a semi-structured interview protocol. The interview was composed of six main interview questions and probes to elicit more information (see Supplemental Appendix A). The purpose of the interview was to understand participants’ experiences with trauma-informed care in the classroom, current knowledge of trauma-informed care, and their training needs related to trauma-informed care. We used a semi-structured interview protocol to ensure participants are asked the same questions which increased the comparability of responses, while also allowing the flexibility to ask follow-up and clarifying questions (Patton, 2014). The interview protocol was piloted with two preschool teachers who were not eligible to participate in the research study. After completing the pilot interviews, the interview protocol was edited for clarity and flow by changing the wording and order of some questions. After the edits, the protocol was piloted again by the same participants to determine if the edits had improved the flow of the interview.
Procedures
The primary researcher contacted participants who indicated interest in an interview via email. Eighteen participants agreed to participate in the interview via phone or Zoom, based on their preference. Interviews were conducted by the first author, audio recorded, and transcribed professionally by REVTM. The interviews on average took 35 minutes (range: 13-57 minutes) to complete. All identifying information was removed from the transcripts and replaced with a data collection ID. First-level member checks were completed by emailing each participant a summary of their interview and asking for any changes, clarifications, or comments (Brantlinger et al., 2005). All participants responded to the membercheck via email and five of the 18 provided clarifying comments, such as changing the name of a curriculum or intervention they used that they did not remember during the interview. The remaining participants requested no changes.
Data Analysis
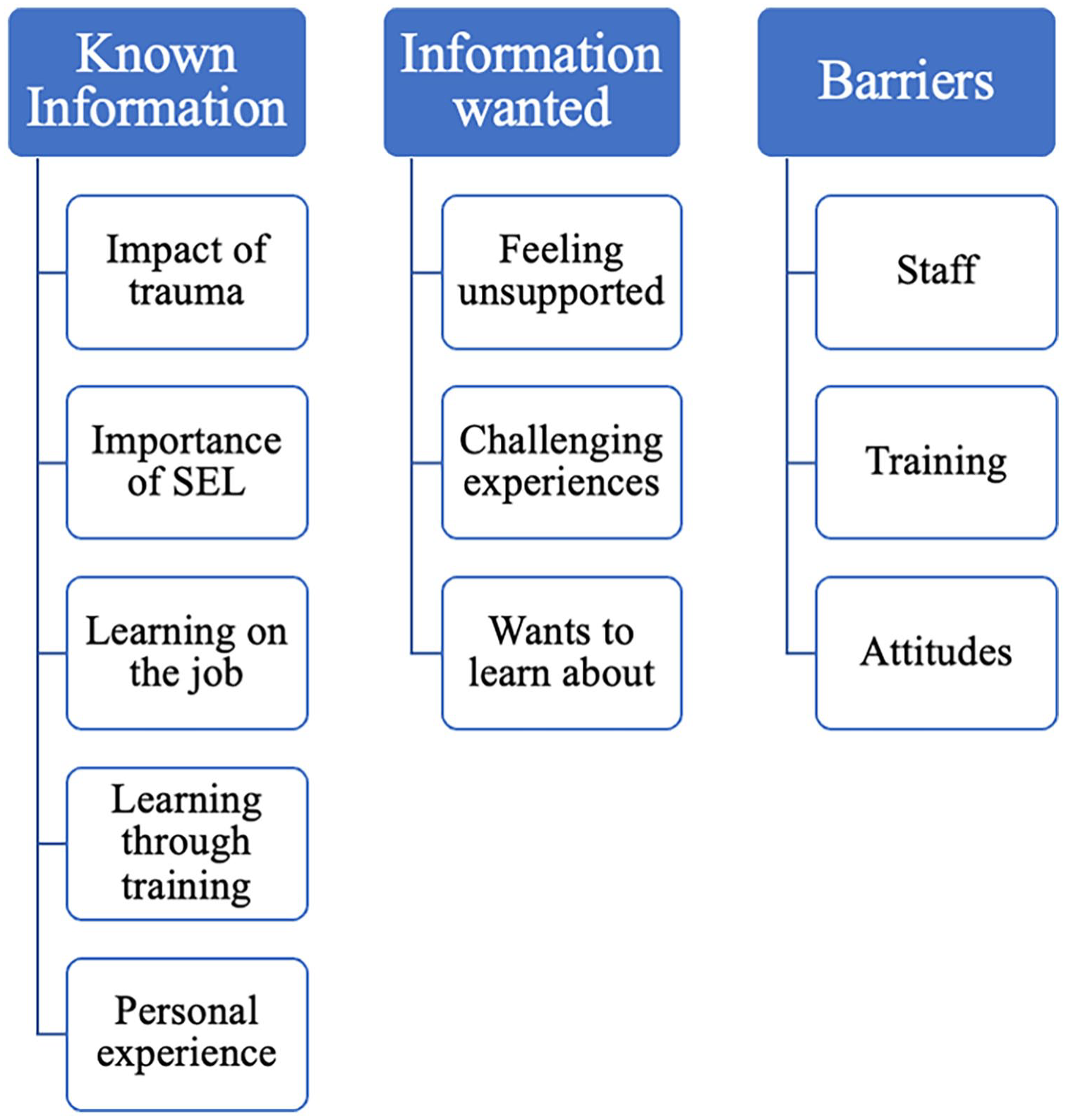
The research team used a thematic analysis approach for the qualitative coding process (Braun & Clarke, 2021). First, two research team members read three interviews and coded the data using an inductive and descriptive process (Saldaña, 2021). The two coders met to discuss the data and collaboratively formed an initial codebook. We then read the remaining transcripts and coded using the same process. We read the transcripts and coded independently, then the coders met to review the transcripts, discuss coding discrepancies, and come to consensus. Then, we used pattern coding (Saldaña, 2021) to group our codes into three main patterns from the data: known information about trauma-informed care, information wanted about trauma-informed care, and barriers to implementing trauma-informed care. These are represented in Figure 1. The codebook evolved throughout the analysis process to reflect new codes or clarifications in code definitions and notes were taken that described the decision-making process. This process supported the consistent application of codes and revisions to codes (Miles et al., 2020).
Codebook.
During the second level of analysis, both members of the coding team reread the excerpts organized by code to ensure appropriate categorization and consistency (Saldaña, 2021). This was done by sorting all excerpts by codes, reading each excerpt, and determining if the code(s) applied to it were the best fit. If an excerpt did not fit, we discussed and re-coded the excerpt. During the third level of analysis, we explored codes for similar areas of meaning to develop themes (Braun & Clarke, 2021). First, we independently reviewed the coded data and developed initial themes. Then, we came together to discuss and come to consensus on the themes. Our final themes and subthemes are displayed in Figure 2. Throughout the analysis process, notes were taken as a form of an audit trail during the meetings to document which transcripts were coded, pertinent discussions that occurred, and any codebook adjustments. The collaborative nature of this process and the use of multiple researchers to identify meaningful data excerpts and to categorize, define, and apply codes enhanced the trustworthiness of the analysis (Brantlinger et al., 2005; Tracy, 2010).
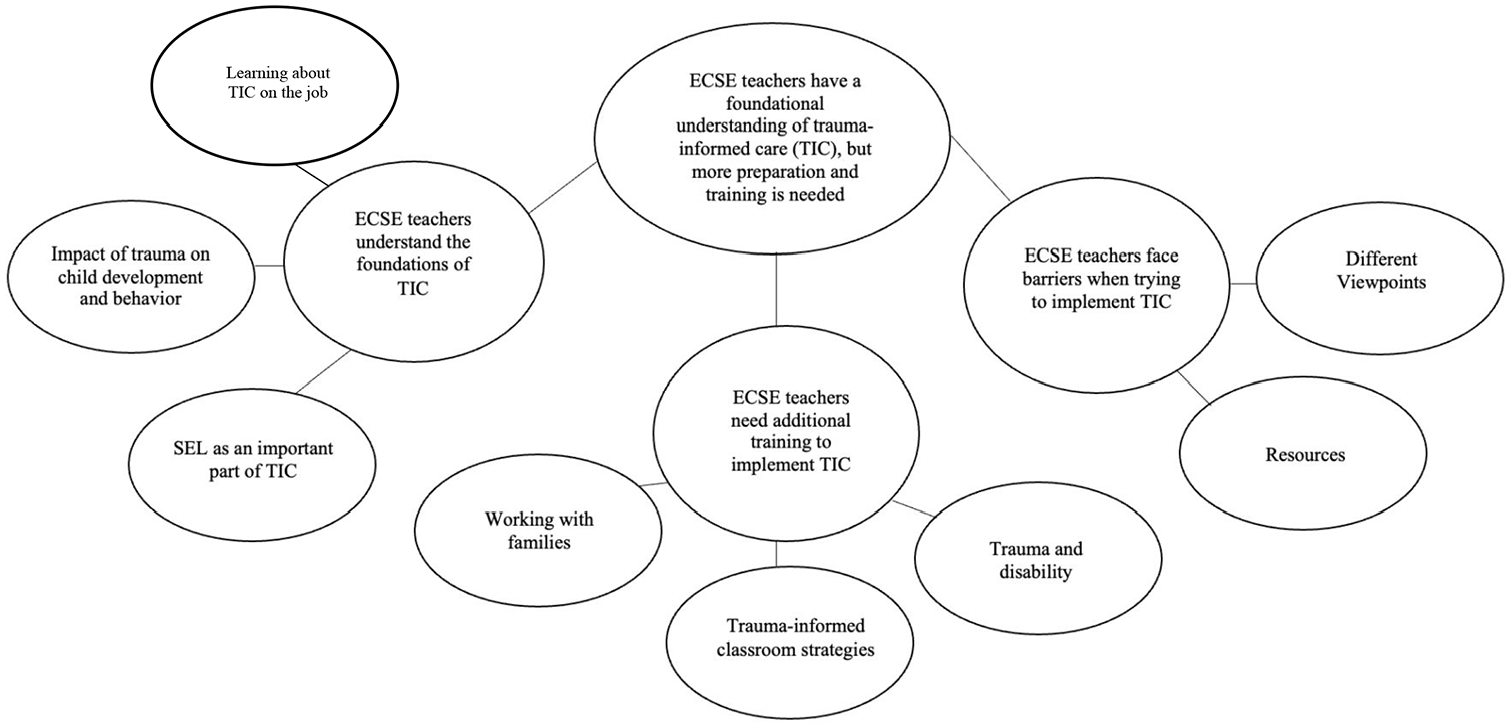
Thematic Map Representing Themes and Subthemes.
Findings
Overall, our findings demonstrate that participants have a foundational understanding of trauma-informed care, but additional preparation and support is needed to successfully implement trauma-informed care. We present the findings under three themes and subsequent subthemes. Figure 2 displays our thematic map and how themes connect with subthemes.
Theme 1: ECSE Teachers Understand the Foundations of Trauma-Informed Care
Impact of Trauma on Child Development and Behavior
Participants recognized that the first 5 years of a child’s life are important for development and that trauma can negatively impact child development. When participants knew a child had experienced a potentially traumatic event, they described changing their classroom approach or detailed taking additional steps to better support the child. As one participant said, “It affects every piece of development, social and emotional, physical, cognitive. It just reaches all of those avenues.” Participants discussed seeing specific areas of development being affected, most frequently, such as executive functioning and social–emotional development. They noticed children having a hard time regulating emotions, calming down, and engaging in classroom activities. The impact on social–emotional development then impacted that child’s abilities to grow and develop in other domains. Claire described this connection by saying “If you’re not feeling safe, you can’t really focus on anything. Can’t focus on interacting with this toy, learning, can’t engage in this activity fully. There’s a lot of impact in all areas of learning.” When participants were aware of the impact of trauma on children’s development, it helped them contextualize the behaviors they were seeing in the classroom.
Participants also described the impact of trauma on child behavior in the classroom. When participants noticed a change in a child’s behavior, they felt the need to discuss it with their school team or the child’s family to learn more about what could be causing the behavior. Participants described this as helpful to better understand the behavior. Serena said: He seemed like he couldn’t control his body, certain times when a friend asked for a turn, he would really refuse to give it or if he wanted something and a friend wanted it, he would cry. And then I found out . . . that there’s domestic violence at home. Now I know he doesn’t have the model of how to label your emotions and deal with your emotions appropriately. And so it’s coming out through the way he is interacting with everyone in the classroom and he needed a lot of extra help and support.
This participant shared that knowing the context of what was happening in the child’s life helped her further support the child. Similarly, others shared they would reach out to families or school staff members to learn more about what could be causing problematic behavior, which would help them tailor the support they gave in school. This helped participants understand what the children and families went through and how it potentially can impact the child’s classroom behaviors.
Social–Emotional Learning as an Important Component of Trauma-Informed Care
Participants discussed the importance of supporting social–emotional learning in the classroom, especially for children that have experienced trauma. They discussed specific strategies, such as having a calm down corner in the classroom, using specific and positive reinforcement, and labeling emotions. They also described using frameworks and curriculum to support social–emotional learning, such as the Second Step curriculum (Committee for Children, 2022) and the Conscious Discipline (Bailey, 2011) framework. It was beneficial when their school or program placed an emphasis on social–emotional development because of the additional supports that were made available to them, such as a provided curriculum or support from other staff members. Maggie shared: We actually have a school social–emotional program. And we have our social worker that comes in once a week and does a small group with whoever wants to come to her . . . they can pull kids and be talked to individually, and they can play and it’s all play based, but they get pulled to have that individualized counseling time. So they can play and talk and discuss things.
Many participants shared that building relationships with their students was foundational in supporting social–emotional learning in the classroom, saying that relationships should come before anything else. Other frequently discussed strategies included maintaining a schedule, creating a safe and welcoming environment, and direct teaching social–emotional content. Grace described this by sharing: I think the number one step is just creating a comforting, warm, and welcoming environment for them. You never know what home life is like for them obviously, or what traumas they have that I don’t know about. It’s cliche, but fostering that love of the environment . . . it’s so huge. That’s the first step is making it a place they want to come to every day, a place they’re excited to come to, and a place they feel safe and they feel loved.
Overall, participants were aware of the importance of social–emotional support. They shared classroom strategies and daily practices they use to encourage social–emotional development and support children who have experienced trauma.
Learning About Trauma-Informed Care on the Job
In addition to what they know about trauma and trauma-informed care, participants discussed throughout the interviews the ways in which they learned about them. Many reported that they did not receive targeted pre-service preparation in the area of supporting children who have experienced trauma and that most of their knowledge in this area was gained through their personal and professional experiences working with individuals who have experienced trauma. The most commonly shared way of learning was on the job learning. Participants talked about their different experiences in the classroom and how it shaped their views on trauma. While discussing how experiences in the classroom impacted them, Erica said: I think they’ve definitely had a huge impact. Things that maybe I wouldn’t have thought of, especially when I was younger or new to teaching. Things that I just, “Oh, yeah. That happens to people.” I don’t think I realized what a lasting effect it can have on children. I guess I should say things like foster care, adoption, homelessness, all that.
Participants described the process of supporting children who experienced trauma as “trial and error” and that it’s been “day-to-day.” Many described talking to co-workers or other teachers about what they were going through. The participants shared that they frequently collaborated with other teachers, related service providers, or mentors to determine the best next steps. Classroom demographics also influenced how participants viewed trauma and implemented trauma-informed practices. They described seeing the impact on children in their class from experiencing poverty or living in foster care and how that shifted their views on trauma. Courtney shared Working with students where about 90% of them are in poverty, and I actually have one student in my class right now who, his personal experiences with it and seeing how it specifically impacts his everyday life, it’s changed my view on trauma.
Another common method of learning about trauma and trauma-informed care was through attending a training or professional development event. Most often, these were a one-time event or workshop that they attended as part of a larger professional development program, such as a school institute day. Frequently discussed topics in these trainings included Adverse Childhood Experiences (ACEs) (Felitti et al., 1998), specific frameworks, such as Conscious Discipline (Bailey, 2011) and Responsive Classroom (2022), and the impact that trauma has on child development. While participants were able to recall information from the training, they shared that they often covered basic information and were looking for more specific strategies to help them in the classroom.
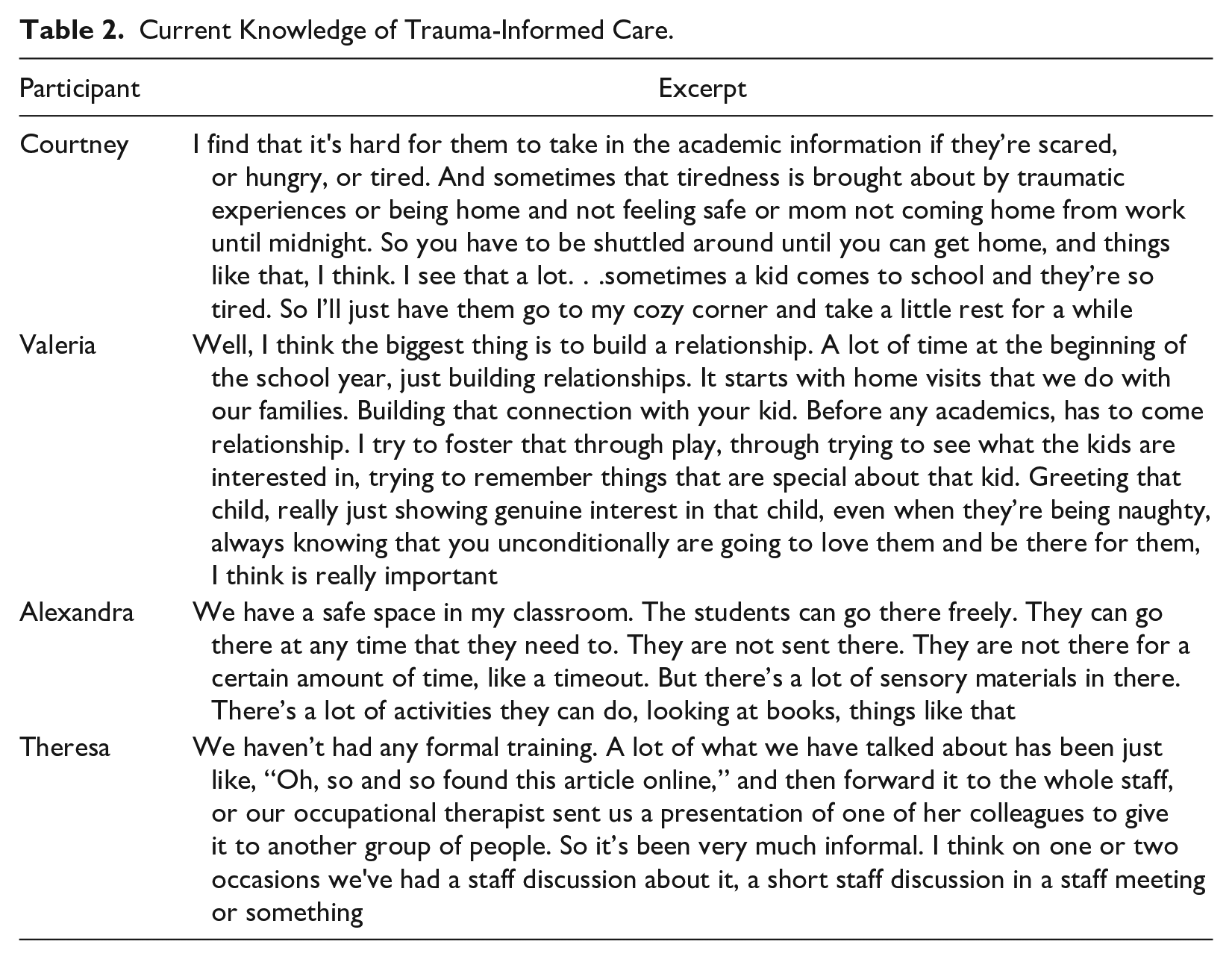
Participants’ personal experiences with trauma also influenced their approach to teaching. Participants reflected on experiences that were traumatic for them or their family and when they knew children in their class were going through the same experience, they recognized it as potentially traumatic, which they reported impacted their interactions. For example, Angela described her 18-month old daughter being diagnosed with cancer, undergoing chemotherapy treatments, and seeing the impact it had on her development. She said, “I mean, that’s not trauma like physical trauma, but it’s traumatic to the developing brain . . . the trauma from it is very easily connected.” Finally, only one participant discussed learning about trauma as part of their teacher preparation program. They recalled reading a research article about the impacts of trauma, but not how to actually implement trauma-informed care in their classroom. See Table 2 for additional excerpts related to participants’ current knowledge of trauma-informed care.
Current Knowledge of Trauma-Informed Care.
Theme 2: ECSE Teachers Need Additional Training to Implement Trauma-Informed Care
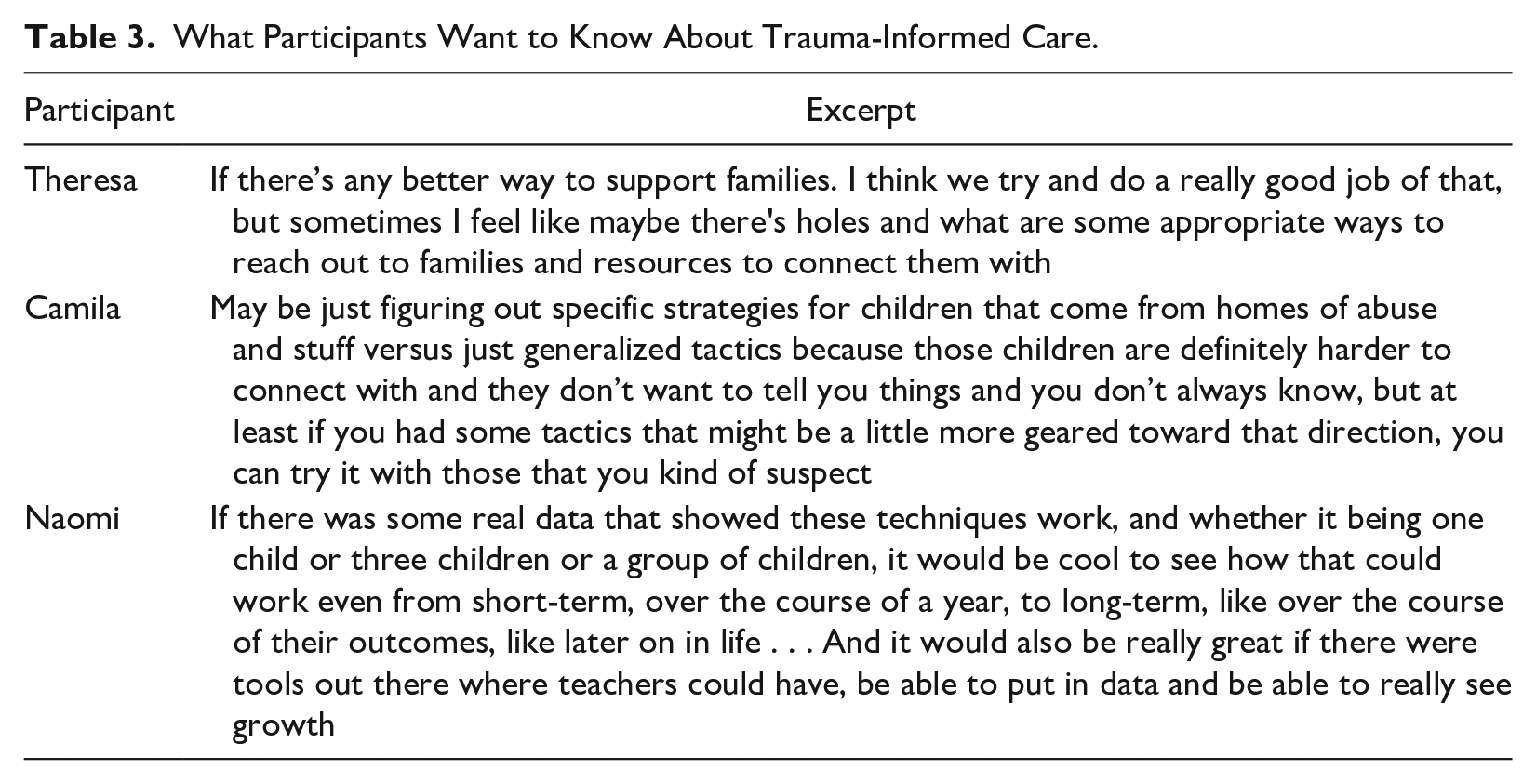
Uncertainty Around Working With Families
Many participants shared uncertainty around working with and supporting the families of children in their class who were experiencing potentially traumatic events. Specifically, participants were not sure if it was appropriate to reach out to the families with resources or materials to help. They reported feeling as if they were walking a fine line between wanting to ensure the families knew they were not alone or isolated, but did not want them to feel bad about what was happening by bringing it up. Theresa described this feeling by saying, “I don’t always know what’s appropriate to do for a family. If they’re in crisis, I don’t necessarily feel qualified . . . I don’t even know who to connect them with, or if it’s appropriate.”
Another common feeling participants shared was that it was difficult to remove their own feelings of judgment when working with families. They discussed recognizing that they should not be critical of a child’s home life, yet still finding themselves questioning the choices that caregivers were making and struggling to reconcile feelings that arose from that. They addressed a disconnect between home life and school life that impacted their ability to support children in their class. Kelley said, “As a teacher, I can’t change what has happened to them or what they go home to, and so there’s only so much we can do when I have a school day of two and a half hours.”
However, when discussing these feelings of uncertainty around supporting children and families, participants also shared that they wanted to improve their ability to support them. Many of them talked about the importance of home visits and how they wish there was more time to connect with families and learn more about them. In turn, they felt they would feel more comfortable reaching out to provide support and would have an easier time interacting with families. In light of the COVID-19 pandemic, some participants were aware of the effects the pandemic may have on children and families and desired more information on assisting families. Jess shared, “In light of this illness (COVID-19) I fear how many kids are going to maybe be experiencing the loss of a loved one, a grandparent passing away or something that way.” Participants recognized the importance of working with families, yet felt uncertain or did not have the tools to properly support them.
Needing Additional Trauma-Informed Classroom Strategies
Participants discussed wanting more strategies to use when working with children who have experienced trauma. They recognized that these children might have different needs and experiences and that traditional strategies may not work for them. Specifically, participants were looking for strategies to address challenging behavior because the typical strategies they used were not working, or they were unsure if they were doing more harm than good. Courtney reflected back on an experience with a student in her class that stood out to her, saying: I feel like just knowing why it’s happening doesn’t help in the moment. Because you can say, “Oh, this is they’re not able to regulate themselves,” and I’m like I can see that, but right now when they’re breaking down and screaming in the middle of circle time, I need some solutions of what to do right now.
Other participants echoed the need for more strategies to address challenging behavior in the moment when it came from children who have experienced trauma. They shared that they recognized the basic things they need to do in the classroom, such as creating a safe and welcoming classroom environment and understanding the “why” of the behavior, but were frustrated that the only resources they had access to were recommending those same basic steps and they had nowhere to go to learn about the next steps. In addition, participants worried that they were lowering their expectations or being “too soft” on students who had experienced trauma. Serena described this dilemma by sharing: You want to have that relationship, that softer side with them. But at the same time I still want to have those really high expectations because sometimes I’ve seen the flip side of it is they’re like, “Oh well you just don’t know what’s going on at home.” But that doesn’t mean we shouldn’t have high expectations for these kids in our classroom. You still want them to reach that level. So I think it can be really hard to know how to walk that line.
Other participants felt like the strategies they learned about in trainings or on their own were not enough and that they needed more individualized support. They recalled doing things like creating a safe classroom environment and focusing on social–emotional learning, but still feeling frustrated. Anna said, “I want more strategies that are beyond the basics. What do we do next? We don’t know what’s right and what’s wrong and that’s hard because I want to do what’s right.”
Some participants expressed wanting access to current research related to trauma-informed care in early childhood. Participants shared that if they had access to current research, they might learn about more strategies to use in the classroom. Erica said, “It would be nice just to know the latest research on it and any new strategies or suggestions for working with children who have been impacted by trauma.” Participants were looking for more research about the manifestations of trauma and outcomes for children that received trauma-informed care versus those who didn’t. Participants hoped that access to research would help them implement trauma-informed care in the classroom.
Overall, participants were looking for more information about how to build meaningful connections and collaborations with families. They sought information about classroom practices to best support children who have experienced trauma, and specifically for children with disabilities. They felt that having more access to current research related to trauma-informed care would help them be better prepared to implement it.
Understanding the Connection Between Trauma and Disability
Another frequently discussed topic was understanding the connection between trauma, disability, and special education. While participants saw similarities in behaviors that stem from disability and trauma, they shared confusion particularly around the relationship between trauma and disability and how each manifests in children. They expressed confusion on how to best support a child who has experienced trauma and shows delays in the classroom, but does not qualify for special education services. One participant described the challenges around getting a support plan in place for one of her students transitioning to kindergarten because they did not struggle academically, but required significant support throughout the school day, such as sensory breaks and additional assistance to regulate themselves. Others noted that having a disability can lead to experiencing potentially traumatic events, such as frequent medical interventions or negative interactions with peers.
Participants also described thinking that being in and out of the hospital for medical reasons or undergoing frequent surgeries could be potentially traumatic for children. In addition, some worried that children with disabilities were isolated from peers in their classrooms due to behavior. One participant described this, saying But then the fact that we’re constantly dealing with her social and emotional needs, and we’re dealing with her outbursts, she’s lacking other things that her peers are getting at that time, and she’s not building those relationships with peers.
See Table 3 for additional quotes related to what participants want to know about trauma-informed care.
What Participants Want to Know About Trauma-Informed Care.
Theme 3: ECSE Teachers Face Barriers When Trying to Implement Trauma-Informed Care
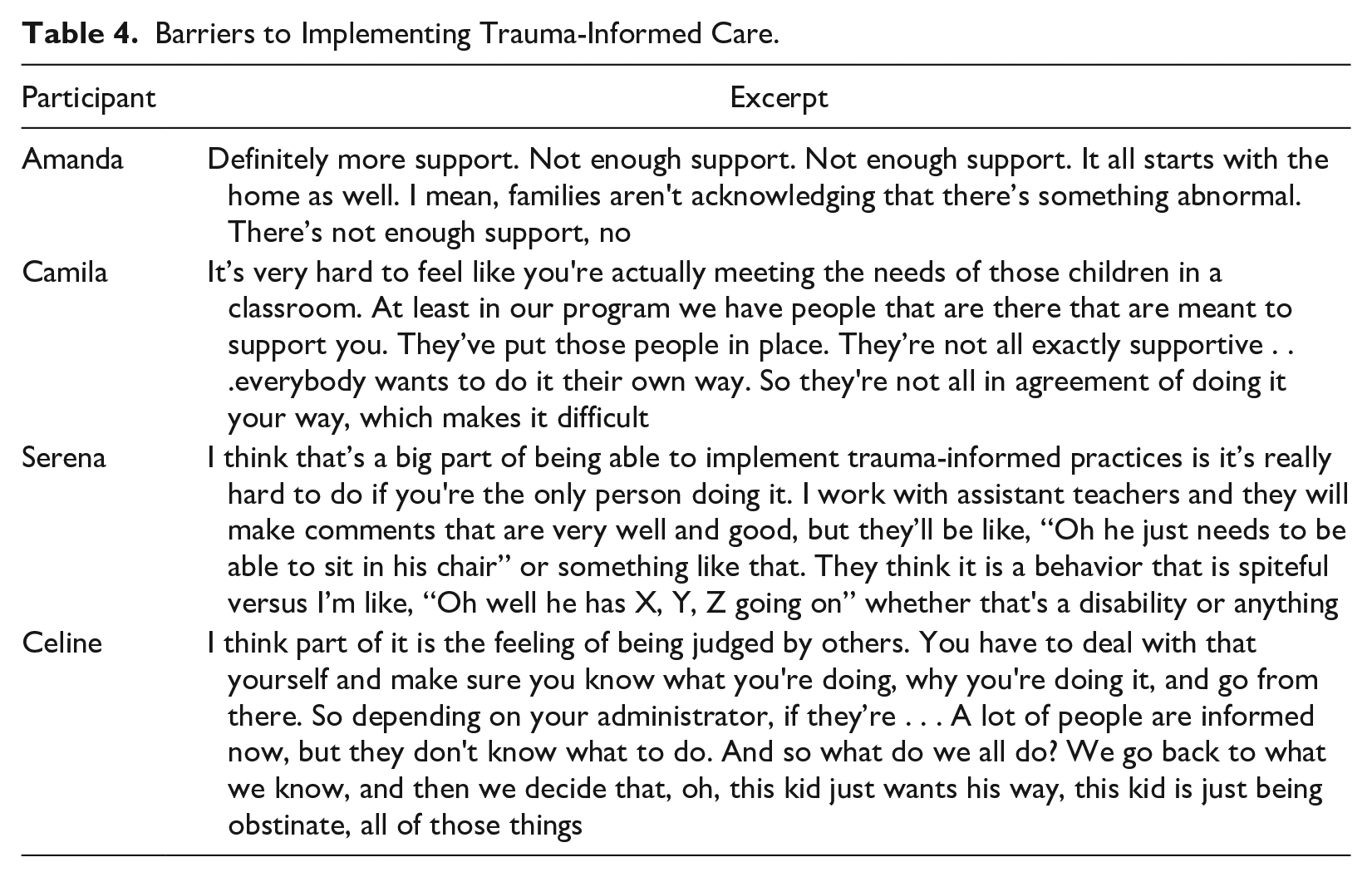
A Lack of Resources Impacts the Ability to Implement Trauma-Informed Care
Throughout the interviews, participants shared barriers to implementing trauma-informed care. While this was not originally addressed in the research questions, it is important to discuss the barriers ECSE teachers report facing when trying to implement trauma-informed care. One frequent barrier to implementing trauma-informed care was the lack of additional staff members, such as paraprofessionals or classroom aides, in the room to assist throughout the day. For example, Valeria shared: I think it would be really helpful if we had more adults available . . . Because when you have 20 kids sitting around the circle and one is hiding under a table shaking and crying, I don’t have the power to just be like, ‘Hold on, 19 kids. I’m going to go and talk to this one.’
Another participant described the repercussions of being short staffed, saying that she often sends students with the school security guard when they are experiencing challenging behavior. The lack of consistent and adequate staff members in a classroom hindered the participants from implementing trauma-informed care.
Participants also discussed shortages of all school personnel including substitute teachers, paraprofessionals/classroom assistants, and related service providers. This impacted not only their classroom, but the climate of the whole school. Some effects included children not receiving their weekly speech therapy minutes and teachers feeling like they had to do the bare minimum in their classroom just to get through the school day. When participants struggled to complete routine classroom tasks, such as toileting or addressing Individualized Education Program (IEP) goals, it made it harder to even think about trying new strategies related to trauma-informed care in the classroom.
Turnover among staff members was another common barrier to implementing trauma-informed care. Participants explained that with high turnover rates among school staff, new members of the school were missing pieces of training that help to address trauma in the classroom. Oftentimes, the school did not have the funds or the time to implement the training again. These school-wide issues made it difficult for participants to use trauma-informed care strategies in their classrooms.
Differing Viewpoints Impact the Ability to Implement Trauma-Informed Care
Participants shared the difficulties of not having consistent staff-wide views on trauma-informed care and the strategies that come with it. These challenges arose when a participant tried to implement something in their classroom but others disagreed or belittled their attempts. Kelley described her coworkers reaction when implementing a “calm down corner” in her classroom, saying “I feel completely unsupported. I come in and they look at me sideways like, ‘Who is this girl?’ or say ‘That’ll never work,’ right away shut it down. Which is hard.”
Participants shared that when members of their own classroom team, such as paraprofessionals or related service providers did not understand or agree with their strategies in the classroom, it made it difficult to implement trauma-informed care because the team members interacted with the children just as much as they did. For example, they recognized that a child crying after the teacher announces a change in the schedule may be because they do not like the uncertainty of the change, but a paraprofessional may view it as the child not listening to the teacher. Serena summarized this sentiment by saying, “I think that’s a big part of being able to implement trauma-informed practices. It’s really hard to do if you’re the only person doing it, you know?”
Overall, when staff members in a school did not hold similar beliefs about trauma and trauma-informed care it created barriers for the participants trying to implement it in their classroom. This highlights the need for school-wide training and professional development related to trauma-informed care in ECSE. See Table 4 for additional excerpts related to barriers to implementing trauma-informed care.
Barriers to Implementing Trauma-Informed Care.
Discussion
A well-trained workforce is a key part of implementing trauma-informed care (DEC, 2016; SAMHSA, 2014). Therefore, it is important that ECSE teachers have the knowledge and tools they need to implement trauma-informed care in their classroom. The findings from this research study have important implications for how we provide professional development on trauma-informed care to ECSE teachers.
First, findings indicate that while participants have some knowledge of trauma and trauma-informed care, participants are not fully prepared to support young children with disabilities who have experienced trauma. This article confirms the work of Miller (2018) and Miller and Santos (2020), which suggested that special education school staff members are unprepared to support children who have experienced trauma. This article extends on current work by providing explicit information as to what the professional development needs are of ECSE teachers in regard to implementing trauma-informed care. In addition, the DEC (2016) Position Statement on Child Maltreatment (2016) calls to “identify the research gaps pertaining to supporting young children with disabilities who have been maltreated and their families” (p. 5). By highlighting areas ECSE teachers discussed needing more support in, this article helps to address the gap.
Second, participants in this study shared that they had attended training and professional development events about trauma and trauma-informed care, but that they covered introductory information. While this information is important, it was not enough for participants to change their day-to-day classroom practices. Specifically, ECSE teachers need professional development opportunities that not only impact their beliefs and attitudes around trauma and trauma-informed care, but that actually help them change their behavior in the classroom and give them strategies they can use. Successfully implementing trauma-informed care is achieved through ongoing and embedded training (SAMHSA, 2014). Therefore, future research can explore the effects of embedding trauma-informed care training into ongoing and common professional development topics, such as curriculum, challenging behavior, and assessment. In addition, the feasibility of using other professional development opportunities, such as coaching or reflective supervision to impact teachers’ trauma-informed classroom practices should be explored, as these practices have been shown to successfully change behavior (Artman-Meeker et al., 2015; Varghese et al., 2018). State policies can be implemented that require information on trauma and trauma-informed care to be embedded within current training, teacher preparation programs, and professional development programs. Furthermore, specific language about trauma-informed care can be embedded into the DEC Early Intervention (EI)/ECSE standards (Division for Early Childhood, 2014) to promote trauma-informed care content in teacher preparation programs.
Finally, participants noted that it was difficult to implement trauma-informed care when they did not have adequate support and buy-in from other staff, including paraprofessionals and administrators. Others have noted the importance of school-wide buy-in and implementation of trauma-informed care (Chafouleas et al., 2016; Jones et al., 2012; SAMHSA, 2014). This points to a need for further research to understand the trauma-informed attitudes and practices of school personnel at a variety of levels, such as paraprofessionals and administrators, to better understand how school personnel work together to implement trauma-informed care. This type of research may also highlight barriers and facilitators that different professionals face when trying to implement trauma-informed care. In addition, professional development opportunities related to trauma-informed care can be expanded to support all school personnel, including administrators, teachers, paraprofessionals, and other school personnel. An important first step is for teachers to become trauma-informed. However, the work does not end there, as it is essential for schools to also take steps to become trauma-informed to sustain this work long term.
Limitations
This study has its limitations. First, the majority of participants were white and female. While this does not represent the entire ECSE workforce, it does closely match the demographics of ECSE teachers in the geographic locations where the study took place. Future research can recruit a more diverse pool of ECSE teachers. Second, participants voluntarily participated in this research study. Therefore, it is likely that teachers who had an interest in trauma would be willing to participate and may already have knowledge about this topic. Finally, participants were from different schools in different areas of the United States. Training opportunities related to trauma-informed care may have differed depending on their location and workplace. Despite these limitations, findings from this study contribute to our field’s understanding of the knowledge gap for ECSE teachers about trauma-informed care.
Conclusion
Young children experience potentially traumatic experiences at high rates (Jimenez et al., 2016), and children with disabilities are more likely to experience trauma (Jones et al., 2012; Zetlin, 2006). In addition, children and their families have faced a myriad of issues throughout the COVID-19 pandemic, including child care and school closures, remote learning, disruption of daily routines, family economic insecurity, mental and physical health problems, and potential loss of a loved one due to the disease (Adegboye et al., 2021; Egan et al., 2021; Neece et al., 2020). Therefore, it is critical that trauma-informed care and practices are being delivered to children in ECSE settings. Findings from this study give insight into ECSE teachers’ current knowledge about trauma and trauma-informed care, the professional development needs related to this area, and barriers faced when trying to implement trauma-informed care. The field of ECSE has highlighted the need to better support children that have experienced trauma (DEC, 2016), and we now have more understanding as to what the knowledge gap is for early childhood special educators.
Supplemental Material
sj-docx-1-jei-10.1177_10538151231164898 – Supplemental material for Trauma-Informed Care: The Professional Development Needs of Early Childhood Special Education Teachers
Supplemental material, sj-docx-1-jei-10.1177_10538151231164898 for Trauma-Informed Care: The Professional Development Needs of Early Childhood Special Education Teachers by Mia Chudzik, Catherine Corr and Kim Wolowiec Fisher in Journal of Early Intervention
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.