
Abstract
Parent-implemented interventions (PIIs) hold promise for young children with autism spectrum disorder (ASD) and their families. Yet, reports of parent and family perceptions regarding PIIs are limited. The present study’s purpose was to gain parent perceptions regarding the helpful and challenging intervention components and contextual factors in the implementation of one PII in their daily lives. Six interviews were conducted and analyzed using an exploratory qualitative approach. Findings included considerable parent satisfaction with intervention experiences, particularly related to the use of videos taken of themselves and their children during intervention sessions. Some parents voiced discouragement after watching video examples, and parents reported challenges finding time to implement the intervention. Parents valued the supportive relationship formed with their interventionist. Additional findings and implications for research and practice are discussed.
Autism spectrum disorder (ASD) is recognized and diagnosed earlier than in previous years due to recent advancements in behavioral and neurological research (Guthrie et al., 2013). With this earlier identification comes an increased need for effective early interventions for young children with ASD and their caregivers. Research indicates that the earlier interventions begin, the greater the outcomes are for children with ASD (Fenske et al., 1985; Wallace & Rogers, 2010). Therefore, studies are beginning to focus on developing and identifying efficacious early intervention models for very young children (birth through 3 years old) with ASD (e.g., Brown & Woods, 2015; Siller et al., 2013). Parent-implemented interventions (PIIs) are becoming increasingly common for children ages birth to 3 years old with ASD and their families (Boyd et al., 2010; Siller et al., 2013). However, there is limited information regarding parents’ lived experiences as implementers of these interventions. The purpose of the present study was to obtain information related to parents’ perceived challenges and successes in implementing one PII.
Researchers have linked optimal child and family outcomes with family-centered practices (e.g., Trivette et al., 2010). Family-centered practices are defined as respecting individual families’ priorities and concerns and including family members as collaborative partners in early intervention service delivery (e.g., Division for Early Childhood [DEC], 2014; Dunst, 2002). They are accomplished by providing families with important information concerning services and supports and allowing families to make informed decisions for their children. In fact, federal policy as designated in Part C services of the Individuals with Disabilities Education Improvement Act (IDEIA, 2004) mandates family-centered services. The Division for Early Childhood of the Council for Exceptional Children (DEC, 2014) Recommended Practices in early intervention also emphasize family capacity building and collaboration with families. Moreover, a recent policy statement on family engagement released by the U.S. Department of Health & Human Services and Education (2016) recommends that practitioners form partnerships with families promoting active family engagement in early intervention.
In some situations, interventionists provide services in homes or centers directly to children with minimal parent involvement. This approach often allows for service delivery in highly structured settings, which may be beneficial to young children with ASD (e.g., Dawson et al., 2010). However, with an increased focus on natural and inclusive learning environments with the parent and interventionists creating nurturing and responsive learning opportunities for the child, the inclusion of parents in the intervention process has become a more general practice (DEC, 2014). Thus, early intervention services have evolved from a therapist-centered to a child-centered ecological model (Sameroff & Fiese, 1999). The interventionist collaborates with the parent to plan and deliver interventions leading to PIIs within a family capacity building framework (DEC, 2014). Taken together, the above policies and recommendations indicate that PIIs are a viable option aligning with family-centered practices.
Feasibility and Acceptability
Family-centered practices are guided by family priorities and concerns, implying that we should determine the acceptability and feasibility of interventions with families. As a result, many researchers measure this construct as a necessary component of PIIs, often in the form of surveys following the intervention (e.g., Brian et al., 2016; Brown & Woods, 2015; Schertz et al., 2018; Stahmer et al., 2017). In a recent review of PIIs for infants and toddlers with ASD and their families, Bradshaw et al. (2015) concluded that parents perceive most PIIs as feasible and helpful, suggesting their general acceptance. Yet, many of the measures of feasibility and acceptability were reported through parent completed Likert-type scales, which often do not include in-depth explanations regarding why parents perceived the interventions to be useful for their families.
Implementation of PIIs in Natural Environments
In addition to designing PIIs to meet families’ concerns and priorities, PIIs also should be applicable to families’ everyday routines and activities. Thus, there is a need to understand parent experiences implementing PIIs throughout their everyday routines and activities. PIIs, by nature, are designed to be implemented by parents and involve multiple layers of interactive implementation components (Wainer & Ingersoll, 2013). Gaining a complete understanding of those times when parents implement the interventions during their everyday routines and activities can be challenging. Conducting observations in family homes throughout their daily lives would be intrusive and not feasible. Yet, it is necessary to explore parent implementation during daily routines and activities to remain true to family-centered service delivery and determine PIIs’ feasibility in home environments. PIIs are especially important to explore as parents’ learning often occurs during scheduled intervention sessions in a clinic or in the home to be applied and used in their daily lives (Dawson & Bernier, 2013; Elsabbagh et al., 2014).
Gaining an in-depth understanding of parents’ implementation experiences in PIIs could be beneficial by providing valuable information regarding PIIs’ applicability to children’s and families’ daily lives. Given the multidimensional components of PIIs and that parents and families implement PIIs in their daily activities and routines, an examination of implementation experiences seems important to determine why or why not PIIs are aligning with family priorities, needs, and schedules.
Parent Perceptions of PIIs
Qualitative inquiry is a potential method for gaining an in-depth understanding about parents’ perceptions of early intervention experiences. The approach allows for open-ended exploration about lived experiences perceived by parents. Although qualitative studies examining parent perspectives of PIIs designed for infants and toddlers with ASD are limited, a few researchers have attempted to gain a greater understanding of parents’ and families’ experiences in such interventions. For example, Stahmer et al. (2011) examined parent and provider perspectives regarding the feasibility of PIIs. The researchers provided informational sessions on selected intervention models and then conducted focus groups to determine how parents and providers felt about the models. Parents and providers reported the models would be feasible and suggested some noteworthy components to be included, such as including siblings in the interventions and parent support groups. However, these were focus groups designed to inform stakeholders about the interventions and obtain feedback about the feasibility of the models without their having actually implemented them. Thus, the participants may have had a limited understanding of the implementation experience.
Researchers have also assessed parent experiences following participation in PIIs. In a pilot study of a PII, Freuler et al. (2014) found parent participants described the important role the relationship with their interventionist played. The parents also reported challenges with finding time to implement the intervention, traveling to assessment sites, and anxiety and disappointment associated with the child developmental assessment results. Yet, little information was shared about the parents’ experiences actually implementing the intervention (Freuler et al., 2014). Employing a slightly different approach, Stahmer et al. (2017) conducted phone interviews with parents as they exited a PII. The parents were highly satisfied with the ways in which they were trained and coached and noted improvement in the quality of the parent–child relationship. However, some parents expressed challenges regarding implementing the intervention in their daily routines, and a few were particularly frustrated with the intervention being designed for children with high verbal skills while their own child was not yet verbal. As a result, the authors suggested a need to individualize support to help parents apply intervention strategies at home and in the community (Stahmer et al., 2017).
The above research provides important preliminary information for the EI field of possible ways to increase the feasibility, acceptability, and family-centeredness of PIIs. However, to achieve the goal of family-centered service delivery, additional research is needed to determine parents’ perceptions of PIIs and how they can be enhanced to match families’ priorities and concerns within their daily lives. Thus, there is a critical need to continue to study parent perceptions and experiences to truly understand what is working for parents and what is not.
In sum, previous findings suggest parents view PIIs as beneficial, and they may hold promise for positive child and family outcomes. However, a better understanding of parents’ perceptions of the feasibility and acceptability of PIIs is needed. Gaining an understanding of parents’ perceptions of intervention components and contextual factors leading to successes and challenges in parent implementation throughout daily routines and activities may contribute to the design of these models. In the present study, we used an analysis of social validity data collected from families who had participated in a PII to purposefully select parents for qualitative interviews that could provide deeper insight into the following research questions:
Method
Research Design
A qualitative research design was used to explore parents’ perceptions of their experiences implementing a PII with their toddlers with ASD. The open exploratory nature of the study included key characteristics of qualitative research such as (a) the researcher serving as the data collection instrument through a focused interview protocol; (b) deductive and inductive logic in data analysis; and (c) multiple interviews to obtain a variety of participant perspectives (Creswell & Poth, 2018). Specifically, the approach included a targeted purposive sample of participants (Miles et al., 2013), who were interviewed to develop themes and subthemes related to their experiences implementing the intervention. The first author conducted individual interviews with a subset of parents from one site, a Southeastern state, of a multisite randomized, controlled trial (RCT). Parents were recruited from this site only to allow for face-to-face conversations. The first author also was familiar with the interventionist and intervention delivery at this site and thus had knowledge of family experiences regarding the general protocol followed during intervention sessions. The first author’s role in the RCT included conducting poststudy assessments in family homes as a blind assessor. She also attended a few home visits with the interventionist to observe the intervention process.
The interviews occurred at a single time point following parents’ participation in the PII. The range of time between parents’ completion of the intervention and participation in the interviews ranged from 11 to 25 months with an average of 19.5 months. Interviews were conducted once the entire data collection process was completed in the final year of a 4-year research study. Although the time lapse between the intervention and interviews was more than 18 months in some instances, all parents regardless of the time lapse were able to recall the specifics of the intervention and details regarding their relationship with the interventionist. Data from these interviews were combined to discover parents’ perceptions regarding the intervention components and contextual factors impacting their overall implementation experiences.
PII in Present Study
Parents participated in a PII intervention targeting early social communication skills (focusing on faces, taking turns, and responding to and initiating joint attention) through a series of stages (Schertz et al., 2013). The intervention was developmentally focused by including such strategies as following the child’s lead, integrating intervention strategies into play, and building on the child’s interests. During weekly home visits, parents were educated on how to incorporate mediated learning principles, which included (a) focusing, (b) organizing and planning, (c) giving meaning, (d) encouraging, and (e) expanding to facilitate child acquisition of the above social communication outcomes. Sessions began with a check in and the interventionist video recording the child and parent interacting while the parent used mediated learning principles toward achievement of the targeted outcome from the previous week. The parent and interventionist viewed these video-recordings together during each intervention session and parents were guided to reflect on the recorded play session. The interventionist then introduced the goals for the next week using video examples, providing verbal explanations, and demonstrating how the target outcome could be mediated. Specific video and print examples represented ideas generated by other parents rather than modeled by the interventionist. A curriculum including a parent manual with information regarding the target skills, strategies, and sequence was used to educate parents on successively more challenging social communication outcomes and mediated learning principles. Parents were encouraged to take the lead on how they would be translated into specific activities in home and community settings. Parents were recommended to set aside 30 min per day for planned activities and to integrate them throughout their daily activities. Parents recorded activities, challenges, and successes in a parent log which was reviewed with the interventionist at each visit. Parents also were able to contact the interventionist between the weekly sessions if questions or issues arose during their daily implementation. However, the majority of feedback, reflection, and planning occurred with the interventionist during the home visits.
Participants
Participants were parents living in the Southeastern site who had been enrolled in the PII. They received the intervention from a single interventionist. Sixty participants completed the intervention across sites in the RCT. The children in the study were all under 30 months at the beginning of the intervention period and scored above the designated cut-off levels on the Toddler Module of the Autism Diagnostic Observation Schedule–II (ADOS-T; Lord et al., 2012). Following participation in the intervention, parents completed a Likert-type scale measuring the intervention’s social validity. Social validity includes the perceived value an intervention relating to the participants’ perceptions of (a) goals (whether the goals matched what participants want), (b) procedures (whether the procedures were acceptable and feasible) and (c) outcomes (whether the outcomes/effects were satisfactory) of an intervention (Callahan et al., 2008; Wolf, 1978). The present study explored the feasibility and acceptability, which is only one component of social validity, but the forms served as a useful tool in selecting a sample that included a variety of parent perspectives. The forms contained 16 items ranked from strongly agree (5) to strongly disagree (1) and two open-ended questions asking parents what they liked most about the intervention and their suggestions for improvement. A total of 17 parents in the Southeastern site had completed the forms.
Preliminary analysis of the social validity forms indicated that parents found the intervention to be highly socially valid, with the majority of parents agreeing with most items on the form. For example, all parents strongly agreed or agreed that the target behaviors were important to them. Visual analysis indicated a few parents rated the social validity slightly lower on a few items, such as items assessing child progress toward goals and parent preference in making decisions in the intervention planning. From these data, a purposive sample of nine parents who either ranked every item as a 5 (strongly agree; n = 5) or parents who ranked a few items with a neutral or disagree rating (n = 4) was selected for recruitment (Miles et al., 2013). For example, on the item, “I liked making my own decisions about which activities, materials, or toys we used in our planned activity sessions,” two parents were neutral. Of the nine participants contacted, six parents (three who rated the social validity very high and three who rated inconsistently high) consented to participate. The sampling strategy intended to create a multifaceted sample with diverse perspectives regarding the intervention’s social validity, implying that their perspectives may also differ regarding feasibility and acceptability of the PII. However, the diversity of perspectives across participant interviews was minimal. Specifically, those parents who rated the social validity as high or even neutral offered very similar perceptions of the intervention. Further details regarding the minimal differences are described below. See Table 1 for items on the social validity scale along with the six parent participants’ responses. All interview participants were married mothers aged 31 to 40 years while participating in the intervention. See Table 2 for additional demographic characteristics, including education level and additional children in the household.
Social Validity Items and Participant Responses.
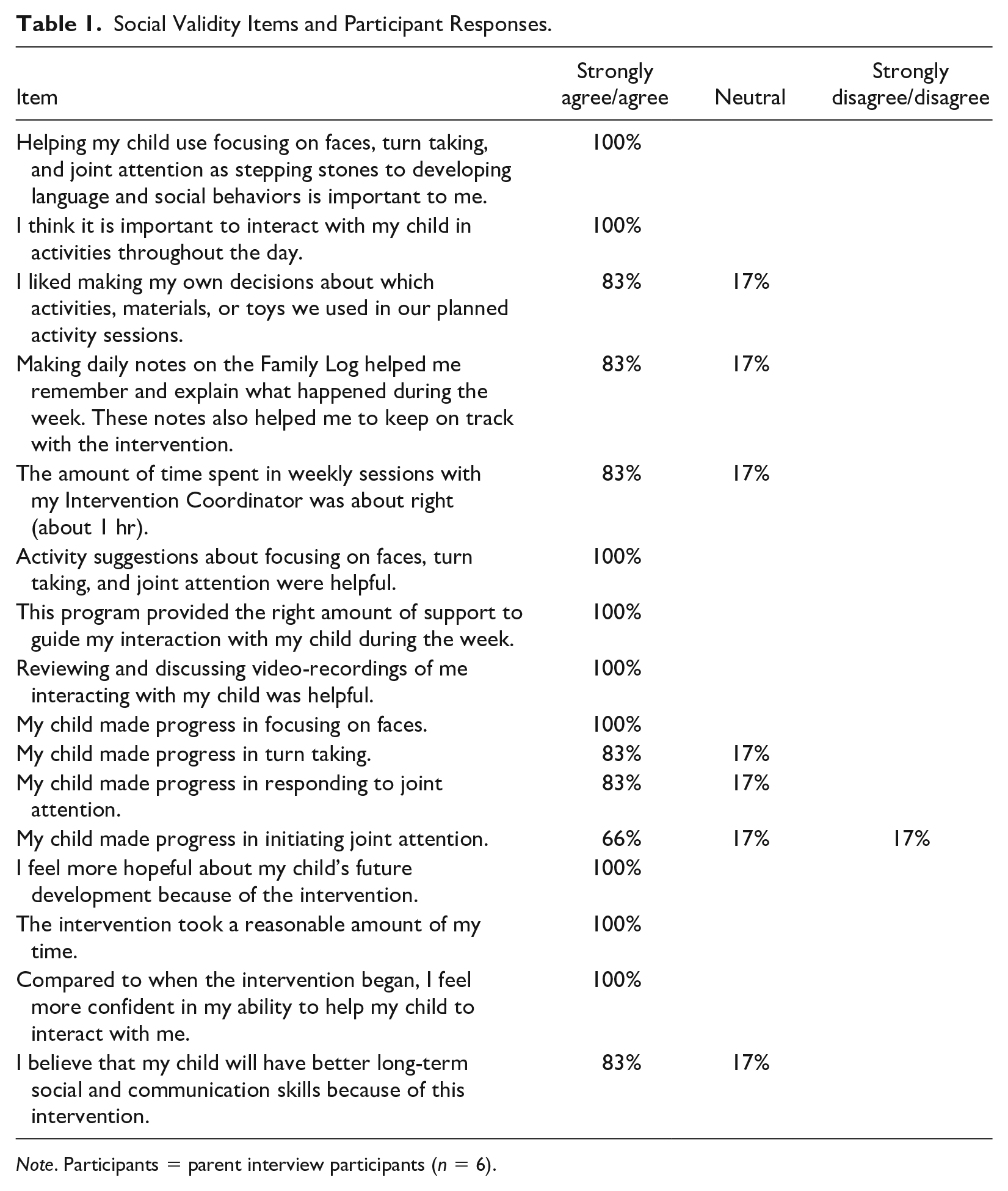
Note. Participants = parent interview participants (n = 6).
Interview Sample Characteristics.
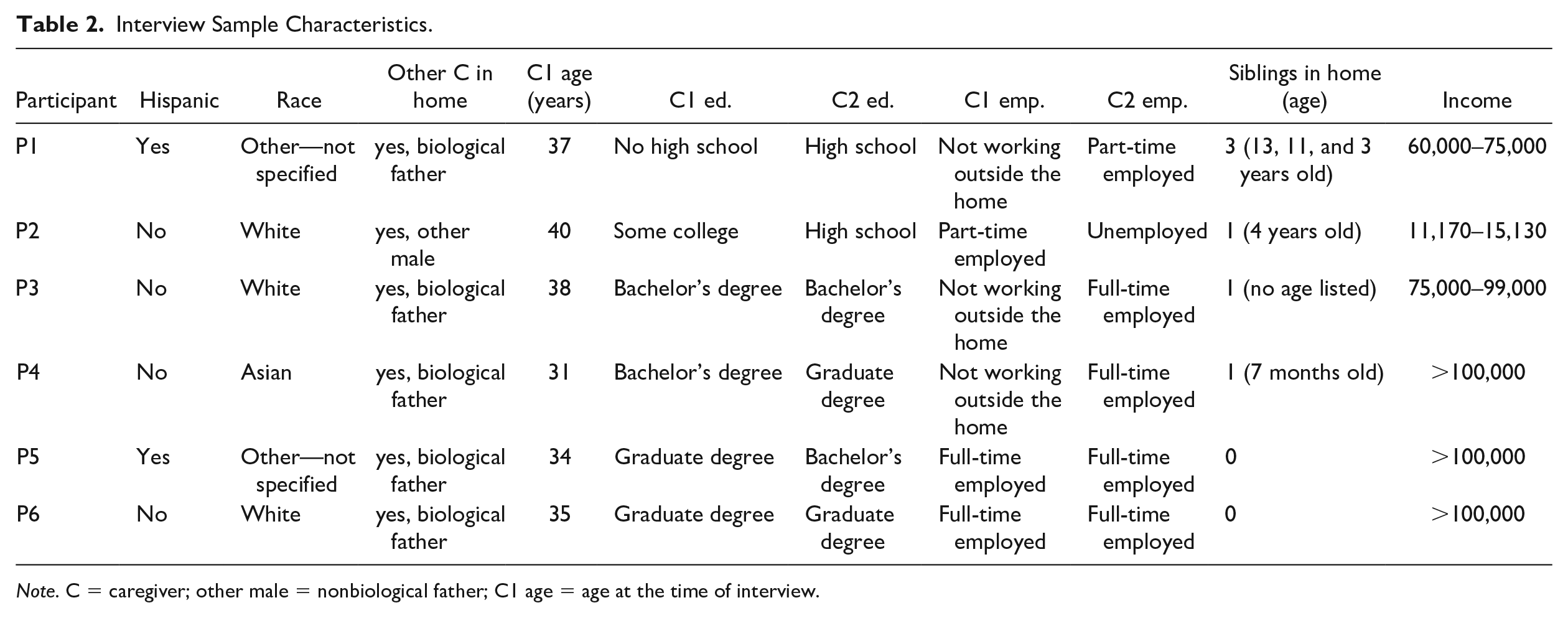
Note. C = caregiver; other male = nonbiological father; C1 age = age at the time of interview.
Procedure
Once University Institutional Review Board (IRB) approval was granted, parents were contacted via a mailed flyer and follow-up phone calls, and asked to participate in a semi-structured interview to determine how they implemented the intervention in their daily lives. After receiving consent from six parents (three who rated the social validity very high and three who rated it slightly lower), the interviews were conducted. Three parents were interviewed face-to-face and three were interviewed via phone due to having moved away since participation in the intervention. Parents who participated in the interviews were compensated with a US$15 gift card following the interview.
Interview development and process
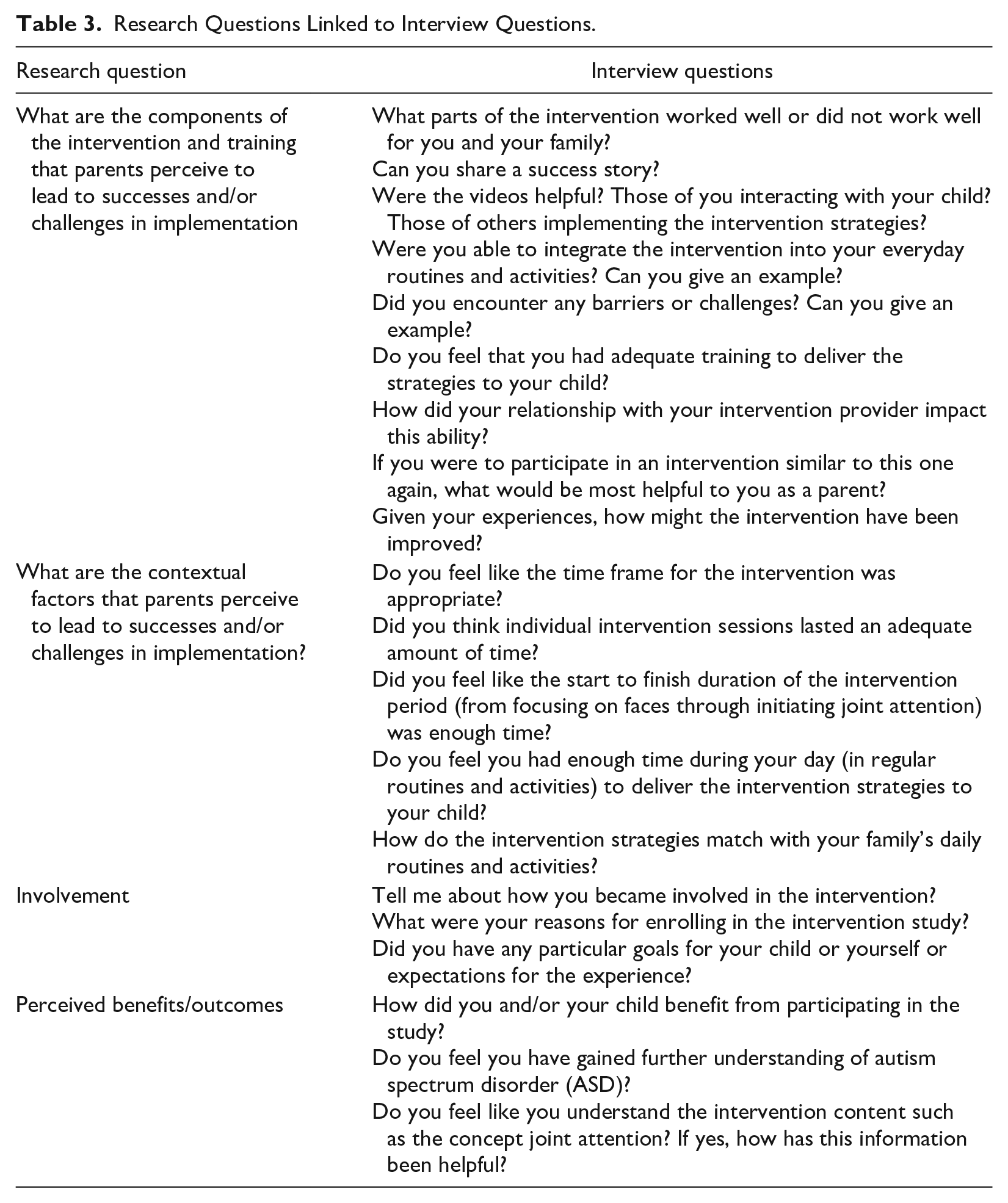
The interview protocol was developed by the first author after a thorough literature review of the social validity of PII. Then, the research team including the home interventionist made suggestions for revisions, and the interview protocol was revised accordingly. Once the protocol was finalized, the interviews were conducted in a casual, conversational manner, and parents were encouraged to discuss what was most relevant to them in regard to their experiences implementing the PII. The interview process involved establishing trust between the interviewer and interviewee (Marshall & Rossman, 2016; Seidman, 2006). Face-to-face interviews were conducted in the families’ homes. The interviewer was an early intervention provider previously so was comfortable conversing and interacting with parents in the home. She had practice piloting the interview with the interventionist on the project, and knowledge of qualitative research methods through participation in focus group studies and serving as a consensus coder for other qualitative studies. She was additionally familiar with available community resources, which was helpful in establishing rapport with parents. The interviewer disclosed her role as a research assistant on the study and shared she had not developed or implemented the intervention. She explained she was only interested in parents’ perceptions of its usefulness in their daily lives. The interviews lasted 25 to 50 min and included questions related to intervention components and contextual factors. Specific prompts related to the intervention were provided when necessary. Parents were also prompted at the end of each interview to share any additional information. See Table 3 for interview questions linked to the research questions and supplemental information for the final interview protocol.
Research Questions Linked to Interview Questions.
To establish member checks, multiple strategies were implemented. First, at the end of each interview, the interviewer summarized the major points parents made to ensure she had understood the major issues raised and to seek clarification, if needed. The interviewer also frequently rephrased parents’ comments throughout the process to make sure data were accurate. Second, parents were offered a copy of the interview transcript for review, although no parents chose to do so. These strategies ensured that the data were an accurate reflection of parental perceptions.
Data Analysis
The interviews were audio-recorded and transcribed verbatim by the first author and a research assistant who was a master’s student in early childhood special education. The first author, who conducted all of the interviews, reviewed all transcriptions for accuracy. The transcribed documents were then systematically coded using qualitative analytic software, Atlas.ti for Mac by the first author. Interview data were coded individually, using descriptive codes, beginning with seven a priori codes that originated from the interview questions (Saldana, 2016). These codes included “Involvement in Study,” “Worked well,” “Did not work well,” “Training, “Time frame,” “Benefits,” and “Improvements.” Notes and memos describing the researchers’ thoughts throughout the analysis were kept while codes were developed and refined, eventually leading to themes and subthemes related to intervention components, training processes, and contextual factors parents perceived as leading to successes and/or challenges (Saldana, 2016). Research questions focused on intervention components and contextual factors, so codes were assigned accordingly. There was inherent overlap between the constructs of intervention components and contextual factors as it is difficult to delineate intervention pieces without considering context. Of note, code and construct overlap is not uncommon in conducting qualitative research (Saldana, 2016).
The questions posed did not determine the ultimate code in all cases. For example, when asked about the videos used in the interview, if the parent spoke about the usefulness of parent–child videos, the code fell under an intervention component, “Helpful Training Approach.” However, if a parent answered this question by speaking of difficulties finishing videos with siblings in the home, the code fell under a contextual factor “Daily Implementation Challenges.” As the data collection and analysis process proceeded, themes and subthemes across transcripts were compared and contrasted and, as necessary, collapsed. Themes were developed when more than one parent expressed a sentiment. Subthemes were developed as more specific concepts related to a main theme. For example, a sample thematic coding process emerged from parent quotes expressing how they learned to use the PII strategies. These quotes were combined into the theme “Effective Training Approach/Process.” Within the theme, subthemes such as parents’ strong relationship with their interventionist and helpful video-recordings during sessions were developed. All data were coded in an iterative fashion and constantly compared to allow for the discovery of the most plausible themes (Marshall & Rossman, 2016). See Table 4 for a summary of themes and subthemes with sample quotations.
Theme and Subtheme Table.
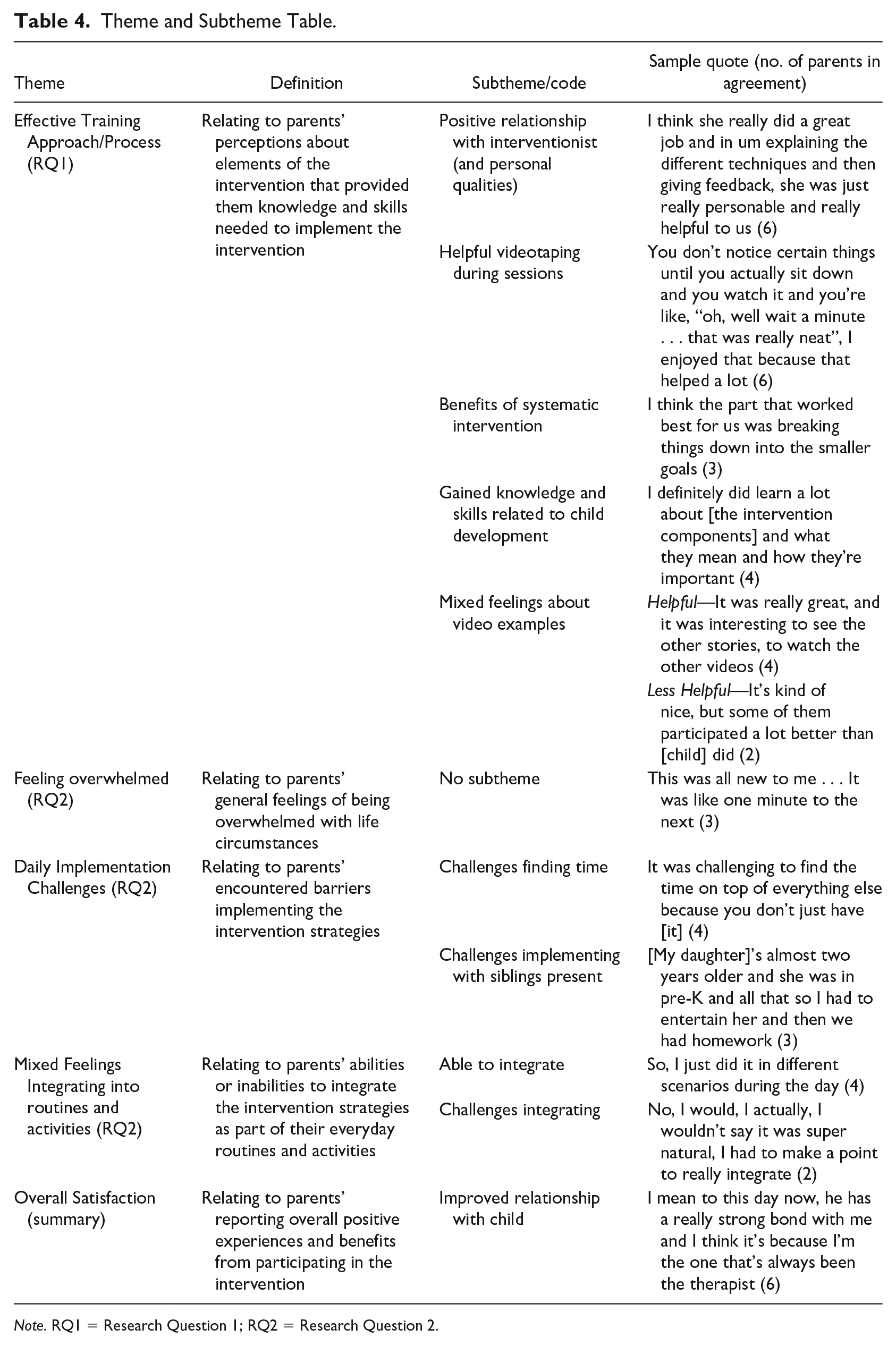
Note. RQ1 = Research Question 1; RQ2 = Research Question 2.
To establish peer debriefing and ensure the data were reliable and valid, a second coder (the second author, who was not involved in the RCT and is not familiar with the intervention) independently coded all of the interview transcripts. The two coders discussed coding agreements and discrepancies to ensure that the first author’s coding was reflective of the concepts, codes, and themes described in the data. The two coders agreed on the majority of codes, although occasionally worded them differently (e.g., “Reason for Enrollment” vs. “Involvement in Study”). On discrepant codes, they reached consensus codes. The consensus coding process was conducted to ensure trustworthiness of the data while maintaining its richness and to avoid interpretations due to researcher bias (Campbell et al., 2013). The combination of the member check procedure described above, peer coding, and debriefing processes between the primary and second coder ensured accountability and trustworthiness in the analysis and interpretation of the data (Maxwell, 2013; Saldana, 2016).
Results
Parents reported overall positive experiences participating in the PII despite some less favorable ratings of a few social validity components. The data analysis did not reveal any trends associated with those parents who rated the intervention’s social validity high in contrast to those who rated the intervention’s social validity lower. There were also no evident differences between those who had completed the intervention more recently than others. Parents proposed a few minor improvements for the intervention. These findings are discussed in detail below in reference to the two research questions regarding intervention components (RQ1) and contextual factors (RQ2).
Intervention Components and Training (RQ1)
Effective training approach/process
The first main theme emerging from the data was parents agreed the training approach was effective in promoting their child’s development. They also described how the training process enhanced the parent–child relationship. Parents highlighted subthemes such as (a) their positive relationship with the interventionist, (b) helpful video-recordings during sessions, (c) mixed feelings about video examples, (d) benefits of systematic intervention, and (e) gained knowledge and skills related to child development.
Positive relationship with interventionist
All parents agreed that the interventionist and the relationship they had with her contributed greatly to their ability to implement the intervention. One parent said the following regarding the interventionist, “She really had a lot of great ideas and was great to work with.” Another parent described her as “the first teacher [to help] me understand my son,” and one more commented, “She was very supportive and was very good at explaining what we’re looking for.” Importantly, these positive feelings toward the interventionist did not differ by family demographics and were consistent across all parents. The parents’ reports of the strong positive relationships with the interventionist reflected one of the foundational tenets of family-centered services (i.e., relationship building) and would facilitate the collaborative problem solving between professionals and parents.
Helpful video recording
All parents additionally agreed that using video-recordings of their interactions with their children was quite helpful. The videos allowed parents to learn a significant amount about themselves and their child, and how to implement the intervention. One mother referred to the videos as her favorite part of the intervention. A parent commented, “It was helpful to have the perspective [of] how my daughter was reacting to me and seeing my own reactions.” Another parent explained she found the videos of herself and her child as encouraging: “And there were some days when I felt like our play time wasn’t going as well . . . But then going back and seeing the video I could see places where we were connecting.” This and other comments suggest that parents perceived video-recordings of themselves as useful tools in learning to implement the intervention strategies.
Mixed feelings about video examples
In addition to the video recording, this intervention used video examples or models of other parents demonstrating how they mediated their toddlers’ learning. Four parents reported the videos were very helpful in demonstrating skills they were being taught. A parent commented, “It was definitely helpful in helping to come up with new activities for the following week.” Another found the video examples to be quite useful and shared, “I think they are a key piece to the study for me to see other parents’ ideas and execution and the children’s responses.” Many parents credited the video examples for helping them decide on activities for the coming week and learn strategies to engage with their children.
Although many parents saw the utility in viewing the video examples and understood the modeled strategies, two parents voiced discouragement as expressed by the following mother: I think having the videos show successful demonstrations of what the principles were, was wonderful and necessary, but it was occasionally discouraging because I would remember somebody in the video doing something and then I’d try to replicate it with my daughter and it was just completely unsuccessful and so I’d think, geez, what are we doing wrong?
Another parent commented that her son was “not quite as ‘high up’ (developmentally) as some who participated a lot better than he did.” This mom agreed that the videos examples were sometimes discouraging, but then went on to say she hopes that videos of her son and herself may someday be helpful to another parent.
Given the above parental quotations, parents reported videos of themselves and their child as useful and supportive coaching techniques. They appreciated the opportunity to reflect on their interactions with their child and receive feedback and support regarding how to better facilitate their child’s communication. However, some parents were uncomfortable with the video examples of other parents modeling strategies, as they were a reminder of their child’s needs and a mismatch with their own parent–child interaction.
Benefits of systematic intervention
Many of the parents commented positively on the intervention’s organization and predictable flow leading to another subtheme related to effective training. Specifically, parents reported they were able to understand the intervention and the target goal because of its simplicity and sequential nature. For example, one parent discussed how the organization and step-by-step nature of the intervention facilitated her ability to implement the intervention: “I think what was most successful was how the study broke down steps and the goals very incrementally . . . otherwise the intervention would have been really overwhelming.” Similarly, one parent appreciated having a single, concrete goal on which to focus. Speaking of her post-PII experience, this parent shared, “There was a goal. Right now, there is not, we have nothing in particular that we work on, but at that time of intervention we had a goal and we worked towards it every week.”
Gained knowledge and skills related to child development
The PII of interest focused on specific content for parents to learn such as Initiating and Responding to Joint Attention. Many of the parents reported that they appreciated and benefited from learning about these concepts, particularly in regard to joint attention. One parent reported that she “had no clue what joint attention was, I didn’t even know that was anything . . . because with children that are just ‘typical’ you don’t have to think about it.” Another mother spoke about the benefits of being able to recognize and understand improvements in their child’s development. She noted, “Since learning those things . . . he’s had joint attention, he’s looking at me, and he’s looking at the toy. And I think, that’s awesome! Now I notice these things that he’s doing and when he improves.” Knowledge about these components, joint attention in particular, seemed to increase parent confidence as described by another parent who said, “I didn’t know that there was such a thing as joint attention, and now, I feel fairly confident in the skill set.” This mother was referring to her understanding this aspect of development and how she could facilitate it in her daily interactions with her child.
Other parents agreed that education related to the PIIs’ components and strategies to target these behaviors contributed to their feelings of empowerment related to engaging and interacting with their children. One parent said, “I think it was really helpful. I think something unique about this approach was that it was teaching me how to do it.” Similarly, one parent shared, “It was almost like I had a tool to do something.” This increased understanding and knowledge of how to interact with their child and facilitate development gave parents a sense of self efficacy and empowerment. The intervention components met parents’ needs for knowledge about and skills for interacting with their children. One parent, while working on the first component of focusing on faces, gave the following example about how just learning to change where she was sitting made a notable difference in engaging her child and said, “I think the first lesson was about positioning yourself where it’s easy to make face to face . . . and that thought never occurred to me before that we can’t make eye contact if I’m sitting behind him!” Another parent gave this example of using a box she received in the mail to work on joint attention with her son: So, [we would], look at him through, a toilet paper roll or a paper towel roll and be like “I see you!” . . . and encourage him to look at us . . . and so sometime that week around that same time I had gotten a huge box . . . and so I was thinking of what I had learned from [the interventionist]. And I was like . . . this is awesome, he can fit in the box, standing. I realized I could convert the box into an elevator . . . so I drew buttons on it . . . and then he would hide inside the box . . . and then, pop out!
In sum, parents gained knowledge about intervention components and reported that this knowledge contributed to the development of usable tools for facilitating their child’s development. And, most importantly, parents were empowered to understand their child’s development and how they could be better facilitators of their child’s developmental successes.
Contextual Factors Influencing Parents (RQ2)
Parents discussed contextual factors such as time and conflicting priorities impacting their participation and ability to implement the intervention. Contextual factors influencing parents’ implementation of the intervention included (a) parents feeling overwhelmed with their child’s diagnosis; (b) daily implementation challenges, including finding time and working around additional children; and (c) difficulties implementing a routine-based approach. They generally agreed that the frequency and duration of home visits was appropriate, and the duration of the study itself was appropriate (although most suggested more or ongoing intervention as a potential improvement, as discussed later).
Feeling overwhelmed
One theme related to contextual challenges parents encountered was feeling overwhelmed. They reported that having their child diagnosed with ASD in addition to accessing early intervention services was challenging. One mother of Hispanic descent was especially sensitive to this and stated, “In this whole process of trying to get into therapies, I had no idea about anything. This was all new to me . . . it was like one minute to the next.” Another mother compared the process of learning her child had ASD and beginning the intervention as starting over, saying, “You don’t know this territory. You don’t.” Alternatively, one mother was pleased because she felt the study provided support to help her in navigating the overwhelming process of an ASD diagnosis and accessing appropriate services. Another mother voiced a desire to include techniques focused on challenging behaviors, which were not a direct feature of the intervention, suggesting that her son’s behavioral challenges may have impacted her ability to implement the intervention.
Daily implementation challenges
Parents expressed some challenges encountered in their abilities to implement the intervention on a daily basis. Subthemes developed as part of daily implementation challenges included finding time to implement the intervention and implementing with siblings present.
Challenges finding time
Another challenge reported by all parents was being able to find time to implement the intervention and some difficulties facilitating their child’s engagement in the activities. As previously stated, it was suggested that parents implement the intervention during focused 30-min-play sessions and also their daily routines and activities. In addition to challenges finding the time, parents discussed their child’s unwillingness to engage and participate in PII activities every day. Thus, parents had to negotiate their daily schedules and routines according to their child’s readiness and willingness to participate. This balancing act was stressful for many parents as they approached their daily caregiving tasks. One parent expressed a sense of being overloaded with day-to-day activities and said, “There were days where it was like I’m not doing this . . . I can’t do this today, I need a nap, we need to go to the pool.” Another mother commented, You know 30 minutes a day doesn’t sound that long . . . but then as I was going throughout the day just trying to think about our schedule and it was really surprising to me that some days, we didn’t really get that much time.
Importantly, at the time of the study, all mothers reported being married, although only one spoke about her husband’s participation in the intervention, which may suggest a need for more targeted involvement of additional caregivers in PIIs to ease the daily implementation challenges.
Challenges implementing with siblings present
Another contextual factor impacting implementation was family dynamics, such as dealing with other children in the home. Several parents discussed their difficulties regarding implementation of the intervention with their toddler with ASD while other siblings were home. A mother with multiple children stated, “I have four boys and it’s just not that easy to say, ‘let’s take a few minutes and play.’” This mother is suggesting that her other children were contributing to challenges implementing the intervention with her son. Other mothers expressed challenges with having young children in the home while trying to interact with their toddler with ASD. One mother with two children shared, “It made it a little crazier . . . a lot crazier, actually. My daughter doesn’t understand why my son with ASD doesn’t understand things the way she does.” These individual family factors seemed to interfere with parents’ perceived satisfaction and success in implementing the intervention.
Mixed feelings integrating into routines and activities
Given the above parent-identified challenges with finding time for intervention implementation, the importance of integrating the intervention strategies into daily routines and activities seems essential. In fact, PIIs often are developed with the intention that parents and families will be able to integrate the strategies into their daily routines and activities (e.g., Brown & Woods, 2015; Wetherby & Woods, 2006). Several of the parents found this integration to be very helpful and natural in their implementation of the PII, and made such comments as follows: I always picked activities that were useful to me . . . when I was doing diaper changes, or when I was feeding him. It was harder for me to think about, “OK, we’re going to sit down on the floor right now and play for ten minutes.”
When asked whether the strategies fit into her daily routine, a mother replied, “I think they matched really well because they were a natural approach.” Another mother reported that the reason she had time to implement the intervention was due to the fact that she was able to integrate it into her routine.
On the contrary, a few parents found this element of the intervention difficult. One mother commented, “I would say they initially just didn’t fit with our routines at all because we weren’t focused on building the types of skills that the study focused on.” This mother explained their day-to-day life prior to beginning the PII did not include building such skills as joint attention and it required an adjustment to their daily routines to do so. She reported once the adjustments were made, she was then able to integrate the intervention into her daily routines. Similarly, a mother shared that before the intervention, “We weren’t doing anything at the time other than just playing or watching TV.” So, for some parents, it was at first a challenge to naturally integrate some of the strategies into already occurring activities. However, parents noted that as they began to understand the intervention more, integration of its components into daily activities became increasingly natural.
Parental Overall Satisfaction
Despite the above implementation challenges, parents reported an overall positive experience participating in the intervention. Most parents additionally reported gains in their child’s social communication skills both on the social validity forms and during the interviews. Importantly, parents reported that following the intervention, they had an improved relationship with their child. One mother commented, “I remember being able to engage with my little guy when I hadn’t been able to in a very long time.” Another mother said, “All of our other therapies and interventions focused on the therapist working with him and this particular [intervention] was really working on building the relationship between him and me.” A mother noted that her changed understanding and skills in interaction made an impact on her son’s responses to her. She described, “It just changed him, he was so much better, he gives hugs and kisses, I got my first hug and kiss after a year.”
Suggestions for Improvements
When asked what would be most helpful to other parents, or if there were anything they felt could be improved, all participants commented on the difficulty of making suggestions for improvement. Many parents said such things as, “Honestly, my experience was so positive, that I can’t imagine changing anything.” These answers suggest parents’ high levels of satisfaction with the intervention led to challenges in suggesting improvements. An additional consideration is that parents were generally unaware of alternative intervention options available to them and their children with ASD. However, with further probes from the interviewer and by highlighting some of the parent comments throughout the interview, the following suggestions seemed most relevant and important for parents. Of note, this question occurred at the end of the interview, and parents were comfortable and had been conversing with the interviewer for a while. So, the slow response is likely not a reflection of the interviewer or interview process. Nonetheless, a few ideas emerged from further discussions with the parents.
More intervention
The most common suggested improvement was simply more intervention. One parent suggested, “Maybe not this particular intervention but the next step maybe, in some kind of social skills groups.” While the desire for more intervention may suggest parents really benefited from the intervention, it seems parents wanted information related to working on next steps in facilitating their child’s social communication. Importantly, the PII had a specific end goal (of joint attention), but perhaps could have included future directions for parents to target more advanced social communication or developmental skills after the children had achieved competence at the preverbal level.
Sibling involvement
Those parents who had other children living in the home suggested that the intervention may be improved by the addition of a sibling component. One mother said, “My children are close in age, they’re 18 months [apart]. So, if we could implement in sibling pairs, that would be great.” Another mother suggested the intervention would be improved if it were to “come up with a way to pull siblings into it to do a little bit more, and to have a sibling role or even a sibling group.” These mothers are highlighting the importance of educating siblings in components and techniques as appropriate based on siblings’ ages. This would help siblings feel more involved with their brother or sister in addition to increasing intervention opportunities for children with ASD.
Parents were overwhelmingly satisfied despite the suggestions noted above following their participation in this intervention which supports the feasibility and acceptability of PIIs in general. By having an increased sense of empowerment and a “tool set” for mutually satisfying interactions, these mothers felt the intervention was feasible, acceptable, and applicable to their daily lives. However, challenges encountered related to contextual factors, such as finding time, implementation with siblings, and easily integrating strategies into daily routines, warrant further exploration to ensure family-centered PIIs.
Discussion
The study’s purpose was to explore parent perspectives regarding the feasibility and acceptability of one PII in their daily lives. Parents reported both successes and challenges related to their home implementation of intervention activities. Parents described the intervention components related to the sequential nature of the goal setting and the focus on joint attention as positive aspects. In addition, parents highlighted the interventionist’s role and video reflections of themselves interacting with their children as important factors in their success facilitating their children’s social communicative learning. However, contextual factors such as family dynamics and finding time to implement the intervention made the implementation challenging for a few parents. The findings also call into question the feasibility of all families truly implementing an intervention for the prescribed 30 min per day. Yet, the overall satisfaction and sense of empowerment gained by parents indicated the promising potential of PII. Providing families with knowledge and skills leading to family capacity building and empowerment is important aspect of family-centered services, yet is often challenging for practitioners to achieve (Bruns & LaRocco, 2019; Rouse, 2012). Based on these participants’ perspectives, the intervention clearly enhanced parental capacity, knowledge, and skills in interacting with and creating stronger bonds with their children. This finding suggests including parents and families rather than relying solely on clinician-delivered services is beneficial for young children with ASD.
In general, the families, regardless of socioeconomic status (SES; as determined by parent education level, employment status, and family income), had very positive things to say about the PII. There were not any perceptions that appeared to come from a singular demographic group. For example, one mother from a higher SES household with a single child reported challenges integrating the intervention into her daily routines and activities. Another mother from a lower SES household with multiple children reported that integrating the intervention into everyday activities was relatively easy and the only way she could participate in the intervention. On the contrary, a mother with one child from a higher SES household also reported success integrating the intervention into daily routines, and a mother with two children from a lower SES household reported challenges. As could be expected, mothers who had other children in their family voiced challenges implementing with siblings. Inclusion of other caregivers and siblings in PII could help ease daily implementation strategies. In addition, the mothers were relatively close in age, ranging from 31 to 40 years at the time of the interview, and the mother’s age did not appear to impact their perceptions relative to technology or any of the reported findings. Specifically, the two mothers who spoke about discomfort and feelings of discouragement after viewing example videos were 35 and 40 years old.
In accordance with others’ findings (Freuler et al., 2014; Stahmer et al., 2017), the relationship with the interventionist appeared to play a large role in parents’ perceived intervention effectiveness. Parents and families in the current study reported feeling that without the relationship and sense of trust that developed between themselves and the interventionist, they would not have been able to implement the intervention. In a study examining factors impacting parent fidelity in a PII with more than one interventionist, individual interventionists’ characteristics made a difference in parents’ abilities to implement the intervention (Wakeford, 2017). This warrants further exploration into ways to ensure that interventionists are equipped to establish a trusting relationship between themselves and families as part of service delivery.
Results support Stahmer et al.’s (2017) findings suggesting parent participants experienced improvements in parent–child relationships following a PII. Parents in the current study also shared they learned ways to relate and interact with their child following the PII. This important outcome supports the use of PIIs for families of young children with ASD. Focused relationship building between a parent and child can be empowering while strengthening the parents’ role in facilitating their child’s development (e.g., Mahoney & Perales, 2003).
The strong support parents reported in reflecting upon and learning from the video-recordings of themselves interacting with their children is noteworthy. Researchers have used video-recorded interactions as part of parent coaching and found improved parent outcomes (e.g., Carter et al., 2011; Green et al., 2010; Poslawsky et al., 2015), but it is unclear how often this approach is applied in early intervention service delivery. There is a need to share this knowledge with community-based early intervention providers and other researchers if using videos is found to be an important strategy in promoting parent learning. The use of video models has similarly been supported by research (e.g., Cox & AFIRM Team, 2018; Odom et al., 2010), and many of the parents agreed with its effectiveness in the present study. Yet, video examples from other parent–child dyads led to a sense of discouragement for some parents. The present PII developers put effort into ensuring that their video examples represent a wide range of skill sets, but perhaps more careful consideration should be used when selecting videos as examples for individual families.
The desire for sibling inclusion is an additional sentiment echoed by other research findings (Stahmer et al., 2011). Siblings pose an extra challenge when trying to implement an intervention with only one child, so it seems natural to include specified roles for siblings who are old enough to participate in such models. This may be particularly salient in families where siblings are close in age as the toddler with ASD may have a strong or close relationship with his or her sibling. As a result, sibling participation in interventions could potentially be very impactful for young children with ASD, which supports the continued use and development of sibling-implemented interventions (e.g., Spector & Charlop, 2018). Notably, in the current intervention, and other PIIs, parents are learning to target skills with their toddlers with ASD. As a result, parents should still be the focus and intervention implementers. However, purposefully incorporating siblings in interactions where appropriate may be feasible in such models. An example strategy for incorporating siblings might include the parent interacting with both children while the typically developing sibling serves as a role model. Again, parents’ careful and purposeful mediation of social learning is important for the young children with ASD.
As Stahmer et al. (2017) found in their work, some parents in the present study experienced challenges integrating the intervention into their everyday routines and activities. As EI services are meant to be delivered in a child’s natural environment, the finding indicates perhaps this approach in PIIs (and perhaps other interventions) needs to be further explored. In the current PII, home visits were generally conducted with a parent in a playroom or living room in their home with skill practice during those sessions. Parents planned to integrate the strategies into routines during intervention sessions, but did not often practice and use the strategies in routines during the intervention sessions. Furthermore, they were not provided specific instructions on how long to spend integrating strategies. Had parents who faced struggles integrating into routines received live coaching during routines, they may have had more success. Furthermore, fidelity of implementation data was not included in this analysis, so firm conclusions on whether strategies were successfully implemented cannot be made. A restructuring of parent support in implementing interventions would include practice sessions (or viewing video-recordings) with coaching during these routines.
Parents in the present sample also reported the desire for extending the intervention’s duration. Although this intervention did have an end point after about 8 months, it is possible some of the learning strategies might be expanded to target additional social communication or child developmental skills. Alternatively, clear “next steps” to target more advanced social communication or developmental skills could be provided as part of intervention packages. Whether parents truly understand the applicability and generalizability of the intervention strategies when participating in PIIs is a component that should be further researched.
Limitations
There are a number of limitations in the present study. First and foremost, the sample size is small and thus not highly generalizable. However, as an exploratory study, the intent is not to assume that these perceptions apply to all parents and families but as a guiding framework for gaining more in-depth information from family members about the usefulness of PIIs. All of the interview participants were mothers. Other family members’ perspectives might have extended mothers’ perspectives. Furthermore, although there was some demographic diversity among participants, five of the six families made over US$60,000 per year. Including perspectives from more families with lower income levels may have led to different findings. The participants also all received the intervention services from a single provider which may have contributed to the lack of variety in some responses. The data are retrospective and qualitative, and by design, assessment scores, parent and interventionist fidelity, and child outcomes are not included. However, had fidelity data been included, it may have been more clear whether the interventionist was adhering to the program and whether parents were implementing the intervention strategies the way they were intended. This also may have informed some of the discrepant findings.
There was also a notable amount of time between the completion of the intervention and the interviews which could have impacted parent recollection. However, the parents were able to recall the interventionist’s name and many of the details of strategies used during the intervention period. Comparisons between parents who had completed the intervention more recently did not indicate any differences in their ability to recall information. In addition, the interviewer was familiar with the intervention, so could pull from her knowledge to assist parents’ recollection of specific intervention processes if necessary.
Those mothers who agreed to participate in the study had consented for further contact and were likely satisfied with the intervention. This also was reflected in the minimal variation of social validity perceptions. Despite attempts for a purposive sample using social validity ratings, the overall satisfaction may have hindered these attempts. Although the interviewer played a small role on the RCT as an assessor in its final year and revealed to participants her independence from the project, some parents may have associated her with the study and framed their answers differently than they would have to someone uninvolved in the study. Parents may have been hesitant to criticize the intervention as a result.
Future Directions
Further research regarding parent implementation of evidence-based interventions is needed to gain a better understanding of families’ perceived experiences in EI and in PIIs. First, obtaining perspectives of families that choose to exit interventions could potentially introduce new challenges and barriers. In addition, there is merit in gaining multiple family members’ perspectives regarding their experiences. For example, interviewing partners who are ultimately impacted by the other partner’s changed interactions with their child may be beneficial. Collecting ongoing parent or other caregiver perspectives as they go through a PII could also provide new insight. This would allow researchers to understand whether perceptions and expectations change as parents and caregivers participate, and whether multiple caregivers view their role in PIIs differently. Furthermore, due to the limited variety of responses related to social validity, using alternative demographic characteristics in recruitment such as (a) parent education level, (b) family income, and (c) employment status may lead to increased diversity in perceptions of implementation experiences.
Future directions additionally might include applying a more direct implementation science approach, including parents and families from the initial stages of intervention development (e.g., Dingfelder & Mandell, 2011; Elsabbagh et al., 2014). To be more specific, in designing studies, researchers may include (a) an exploration phase with parents and families to ensure acceptability and goodness-of fit for PIIs; (b) an installation phase during which time is dedicated to ensuring supports and resources are in place to use a PII; (c) an initial implementation phase during which parents could begin trying the PII, and adjustments are made as needed; and (d) a full implementation phase during which parents and caregivers use PIIs as part of their daily lives (Bertram et al., 2015). This approach would allow for adjustments and improvements to the intervention models as parents participate in a PII.
Conclusion
PIIs hold promise for infants and toddlers with ASD and their families. Following participation in PIIs, parents are perceiving benefits relative to their own skills and knowledge, and, perhaps above all else, in their improved relationships with their children. PIIs have been conducted for some time, yet we are just beginning to closely study parent perceptions of their intervention experiences. Perhaps a next step in early intervention service delivery is to ensure that intervention models are not only family-centered but also family-driven by obtaining family input about their implementation and participation experiences in these interventions at the outset. This approach would warrant a true partnership with parents and other caregivers in the design and implementation of such models.
Supplemental Material
Interview_Protocol_supplemental – Supplemental material for Parents’ Voices Regarding Using Interventions for Toddlers With Autism Spectrum Disorder
Supplemental material, Interview_Protocol_supplemental for Parents’ Voices Regarding Using Interventions for Toddlers With Autism Spectrum Disorder by Jessica Amsbary, Harriet Able, Hannah H. Schertz and Samuel L. Odom in Journal of Early Intervention
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Institute of Education Sciences (IES), U.S. Department of Education through Grant Number R324A120291 awarded to Indiana University, and by the Office of Special Education Programs (OSEP), U.S. Department of Education through Doctoral Leadership Grant Number H325D13004 awarded to the University of North Carolina at Chapel Hill.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.