
Abstract
Objective
To examine the effect of heel elevation using a tilting plate on sit-to-stand performance in Parkinson's disease (PD) patients, evaluate the influence of different tilt angles, and identify clinical factors associated with this effect.
Methods
Thirty-six PD patients participated in a randomized crossover trial. Half started in a flat position, and half in a heel-elevated position, using three tilting angles. The time to complete five times sit-to-stand tests (FTSST) was measured under flat and heel-elevated conditions.
Results
The fastest FTSST in the heel-elevated condition was reduced by a median decrease of 2.3 s and a median reduction of 14.0% when compared to the flat condition. Neither tilt angle nor ankle dorsiflexion range of motion was not associated with the reduction in FTSST duration. Multivariable regression analyses revealed that the time of FTSST under the flat condition and the standing subscale in the Unified Parkinson's Disease Rating Scale Part III exhibited significant positive associations with the observed shortening effects of FTSST induced by heel elevation.
Conclusions
The use of a heel-elevation intervention reduces the duration of transitioning from a seated to a standing position among patients with PD, particularly among those with a more pronounced disability. (UMIN000048428, https://center6.umin.ac.jp/cgi-open-bin/ctr/ctr_view.cgi?recptno=R000055160)
Keywords
Introduction
The sit-to-stand movement in patients with Parkinson's disease (PD) is impaired by factors that are intrinsic to the disease, including compromised balance, akinesia, muscle rigidity, and postural abnormalities. Additionally, the aging process introduces its own set of limitations such as restricted joint mobility, muscular weakness, and cognitive decline (Mak & Hui-Chan, 2002; Rocchi et al., 2002; Wright et al., 2010; Yu et al., 2000). Longer sit-to-stand time is associated with recurrent falls in patients with PD (Mak & Pang, 2010), and impairment of this movement severely limits their daily activities of the patients. One study found that patients with PD exhibited a posterior deviation of their center of gravity in the standing posture relative to their center of pressure (Oku et al., 1991). Thus, heel elevation in patients with PD has been documented to yield beneficial effects on stability of standing posture and gait through anterior displacement of the center of gravity and improved postural alignment (Oku et al., 1995; Uno et al., 2021). The limitation of ankle dorsiflexion range of motion (ROM) is thought to contribute to the posterior deviation of the center of gravity in patients with PD; therefore, heel elevation was adjusted according to three grades of ankle dorsiflexion ROM (Uno et al., 2021). Nevertheless, the effect of heel elevation on disequilibrium, as represented by the sit-to-stand action, and whether this effect depends on ankle dorsiflexion ROM, have not been clarified. In this study, we aimed to elucidate the effect of heel elevation on sit-to-stand movement and its association with heel-elevation angles in a randomized crossover trial.
Previous studies have set heel elevation within the range of 1–3 cm (Oku et al., 1995) or used three grades of angle depending on ankle dorsiflexion ROM (Uno et al., 2021). Following the previous studies, we prepared tilting plates with three angles and corresponding heights (5°: 1 cm, 10°: 2 cm, 15°: 3 cm).
The Five-Times Sit-to-Stand Test (FTSST) (Bohannon, 2011; Makizako et al., 2008; Petersen et al., 2017), a well-established metric commonly employed in assessing frail elderly individuals, serves as an indicator of lower limb muscle strength and is a reliable method for evaluating sit-to-stand performance in patients with PD (Janssen et al., 2002). The sit-to-stand motion assessment has substantial utility in gauging an individual's physical functioning level and has been recognized as a predictive measure of the risk of falls (Duncan et al., 2011). We used FTSST to clarify the effect of heel elevation on disequilibrium during movement and its potential role in fall prevention.
Therefore, this study investigated the effect of heel elevation using tilting plates on the performance of patients with PD on the FTSST.
Methods
Participants
Participants were recruited from the neurology outpatient clinic of Kochi Medical School Hospital. The inclusion criteria encompassed individuals diagnosed with PD by a qualified neurologist. The exclusion criteria included: (1) individuals unable to independently rise from a chair with a seat height of 52 cm even with upper limb assistance using both hands on their knees; (2) individuals with pronounced cognitive impairment rendering them incapable of comprehending the study procedures or following instructed actions; and (3) minors.
The sample size was estimated using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan). The minimum detectable change of FTSST in the PD population is approximately 2.4 s (Paul et al., 2012). This study set the target difference for detection as 2.4–3.0 s, which is considered a clinically meaningful improvement. In a crossover trial, assuming an intra-subject standard deviation of 4–6 s, the minimum number of participants required was calculated to be 34 at an α error of 0.05 and 80% power. Given the utilization of three distinct heel-elevated conditions for the intervention, and considering the need for randomization of participants into these three conditions within each group, the target sample size was set at 36 participants, a multiple of three, and 18 participants were allocated to each group.
For the simple randomization procedure, a random number table was created in Excel and a third party was given control to check the results of the random assignment.
This study was conducted in accordance with the “Declaration of Helsinki” and the “Ethical Guidelines for Life Sciences and Medical Research Involving Human Subjects” and was approved by the Ethical Review Board of Kochi Medical School (approval number: 2022–36, Ethics Committee Review Date: July 12, 2022). The study protocol was registered in the clinical trial registration system of the University Hospital Medical Information Network before study initiation (UMIN000048428). The clinical trial registration was prospective and performed prior to recruitment of the first study participant. Patient registration began on July 21, 2022 and ended on July 22, 2023. Before participating in the study, participants were informed of its purpose and content, that their personal information would be kept confidential, and that their free will would be respected in participating in the study. Their written informed consent was obtained. We confirm that we have read the journal's guidelines on issues involved in ethical publication and affirm that this work is consistent with these guidelines.
Study Design
Figure 1 shows a flowchart of the randomized crossover study. Clinical data were collected and pre-intervention assessments were conducted on participants who provided written informed consent. Subsequently, participants were randomly and evenly assigned to two groups: Group A (“flat condition prior”) and Group B (“heel-elevation condition prior”). Three types of titling plates with tilts of 5°, 10°, and 15° tilts, were employed for the heel elevation. Within each group, the participants were randomly allocated to three subgroups: (1) 5 to 10 to 15°, (2) 10 to 15 to 5°, and (3) 15 to 5 to 10°, thereby mitigating potential order effects.
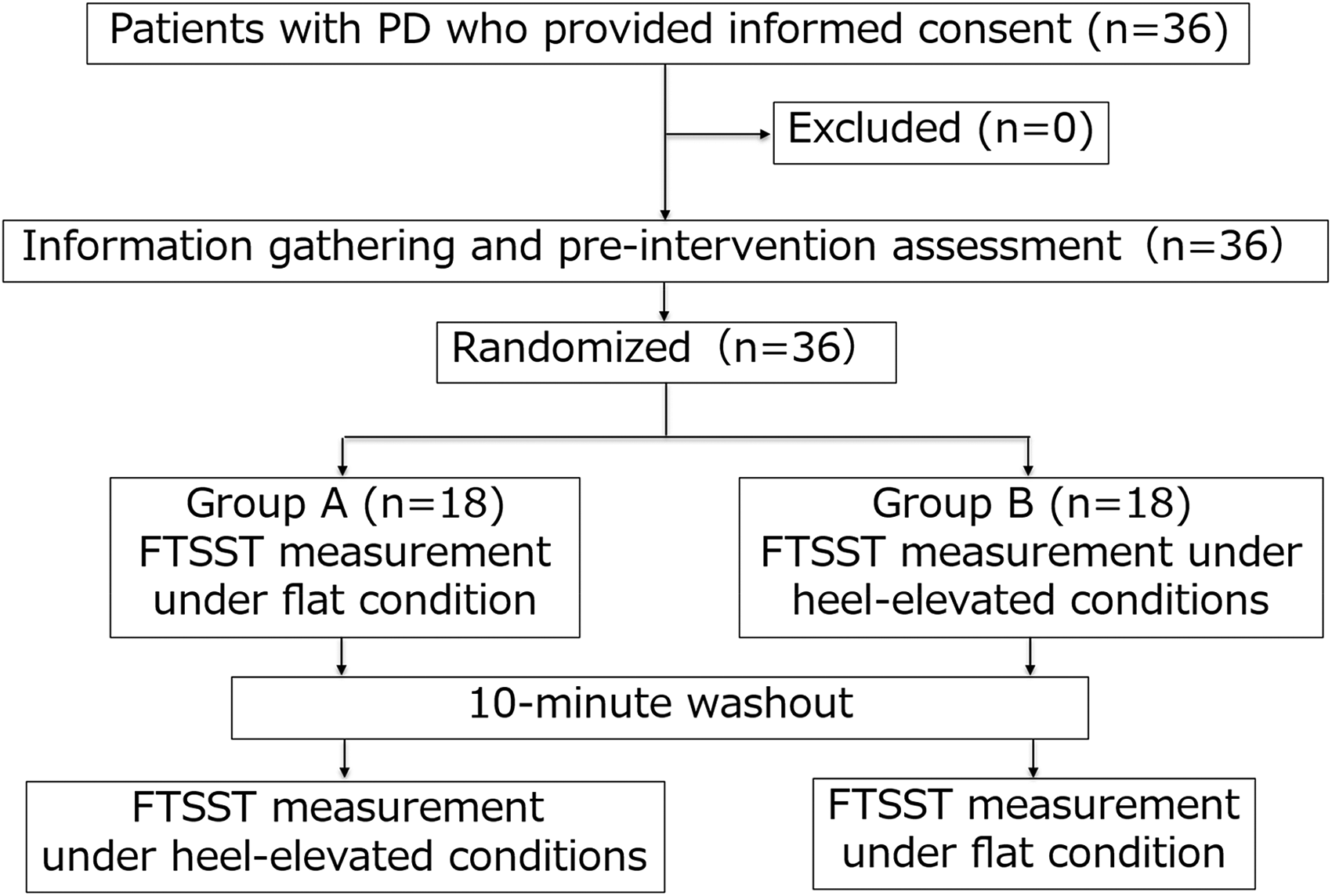
Flowchart of a Randomized Crossover Trial of FTSST in 36 Patients with PD. FTSST, The Five Times Sit-to-Stand Test; PD, Parkinson's Disease.
A 10-min rest interval was interposed between the FTSTS measurements under flat and heel-elevated conditions, serving as a washout period to alleviate carryover and fatigue effects associated with repetitive sit-to-stand motion practice. A 10-min rest period was adopted to ensure the practicality of single-session assessment to avoid intra- or interday fluctuation of symptoms in PD.
FTSST measurements were conducted on the same day during the “on” phase, occurring within 3 h after the L-dopa formulation administration to account for intra- and inter-day fluctuations in PD symptoms.
Tilting Plates
Three variations of the tilting plates designed for heel elevation were crafted. These tilting plates included a 5° tilt with a 1 cm height, 10° tilt with a 2 cm height, and 15° tilt with a 3 cm elevation.
FTSST Measurement
FTSST measurements were performed as reported by Makizako, Ota, Setaka, Harada, Nakamura, and Muraoka (Makizako et al., 2008). The measurement of FTSST in one case is shown in Video 1. The publication of this video has been explained to the individual, and the written consent has been obtained.
Initially, the participants assumed a seated position on a chair with a seat height of 42 cm and both hands resting on their knees. The floor surface was covered with a non-slip sheet to ensure stability and the participants were barefoot. Each participant was seated with their feet flat on the floor or a tilting plate, aligning the long axis of the lower leg to tilt forward, and positioning the knees approximately 10 cm (equivalent to the width of one clenched fist) ahead of the chair's front edge. The participants received orientation and engaged in three to five practice sessions to familiarize themselves with the procedure. The participants were instructed to stand up and sit down as quickly as possible, and the time required to complete five cycles of this activity was recorded. During the test, participants were allowed to use both hands when standing up from the chair under all conditions.
The observer instructed the participants to fully extend their knee and hip joints while attempting to sit, before extending their joints in the standing position.
Under flat conditions, FTSST measurements were conducted twice, following three to five practice runs, and the shorter duration was selected for analysis. Conversely, the FTSST measurements in the heel-elevated condition involved positioning the posterior edge of the heel at the highest point of the inserted tilting plate after three to five practice sessions with each plate variant. Before each FTSST measurement, the absence of fatigue was confirmed verbally after the practice runs. A brief rest interval of approximately 2 min was allowed between assessments at each inclination level depending on subjective complaints or fatigue. All trials were evaluated by one physical therapist (T. N.).
Outcome Measures
The primary outcome measure was the change in FTSST duration between the flat and heel-elevated conditions.
Clinical data were extracted from the medical records to investigate the factors influencing the change in FTSST duration induced by heel elevation. This included details regarding age at examination, disease duration, sex, Hoehn and Yahr Stage and the prescribed L-dopa dosage, and results of dopamine transporter single-photon emission computed tomography, metaiodobenzylguanidine myocardial scintigraphy and brain magnetic resonance imaging. Additionally, a single physical therapist (T. N.) examined the Unified Parkinson's Disease Rating Scale Part III (UPDRS III), Mini-Mental State Examination, knee extension muscle strength employing μ-TAS F1 (Anima Corp. Tokyo) (Katoh & Isozaki, 2014; Katoh & Yamasaki, 2009), and the ROM of the knee and ankle joints using ImageJ (NIH) (Nakayama et al., 2023) before initiating the intervention. All data collection, including FTSST measurements, was performed at Kochi University Hospital.
Statistical Processing
In the statistical analysis, tests of normality (Shapiro–Wilk test) were performed on subject attributes, pre-intervention assessment results, and FTSST measurements. Data that were normally distributed were presented as mean ± standard deviation, and data that were not normally distributed were presented as median (25th–75th percentile).
Following normality verification, Fisher's exact test, Two-sample t-test, and Mann-Whitney test were conducted to examine the differences in the clinical features and pre-intervention assessment results of the participants in Groups A and B.
Wilcoxon's signed rank sum test was employed to compare the FTSST duration in the flat condition with that in the heel-elevated condition to evaluate the impact of heel elevation on the entire participant cohort as well as on Groups A and B. Analyses were corrected for multiple comparisons using Holm's method.
We estimated Spearman's rank correlation coefficient between the heel-elevation angle producing the fastest FTSST time and ankle dorsiflexion ROM.
Spearman's rank and Pearson's product-moment correlation coefficients were used to explore the factors influencing the magnitude of change, which was defined as the disparity between the FTSST duration in the flat condition and the quickest FTSST duration achieved with heel elevation. Furthermore, multivariable regression analysis employing the stepwise BIC method was conducted. Variables demonstrating significant correlations were incorporated as explanatory variables with the magnitude of change serving as the dependent variable. To adjust for carryover effect on changes of FTSST durations, we conducted multivariable regression analysis including the order of FTSST measurements (Group A or B) as a covariate.
All statistical analyses were performed using the Modified R Commander 4.1.2, which extends the functionality of R and R Commander. The predefined significance level for all statistical analyses was set at 5%.
Results
A total of 36 participants were enrolled between July 21, 2022 and July 22, 2023, with random assignment to either Groups A or B. All participants successfully completed all FTSST measurements under flat and heel-elevated conditions. Measurements were taken in a 42-cm high chair for all participants except one; this participant was unable to rise from a 42-cm chair, so a 47-cm chair was used for the measurements. None of the participants met the exclusion criteria. In this study, there was no harm and zero events. Table 1 presents the clinical characteristics and results of the preintervention assessments. Group A exhibited a higher score on the standing item within the UPDRS III, whereas the knee extension muscle strength-to-weight ratio was lower than that of Group B.
Clinical Characteristics of the Participants.
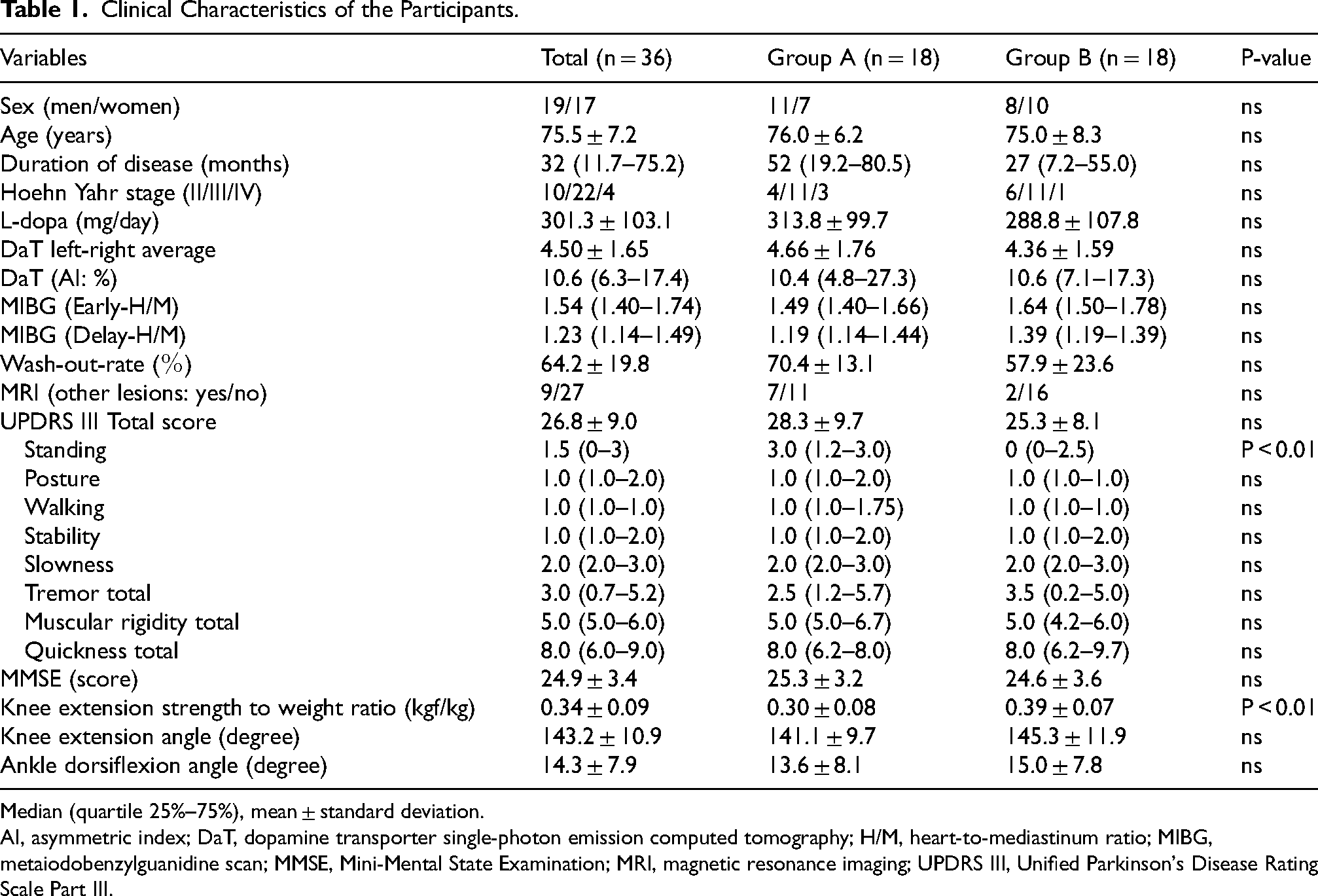
Median (quartile 25%–75%), mean ± standard deviation.
AI, asymmetric index; DaT, dopamine transporter single-photon emission computed tomography; H/M, heart-to-mediastinum ratio; MIBG, metaiodobenzylguanidine scan; MMSE, Mini-Mental State Examination; MRI, magnetic resonance imaging; UPDRS III, Unified Parkinson's Disease Rating Scale Part III.
Figure 2A shows the heel-up effect observed in all participants (n = 36). The median FTSST duration in the flat condition was 14.5 (interquartile range [IQR]: 12.7–20.2) s. Under the heel-elevated condition, the FTSST durations were as follows: 13.8 (IQR: 10.5–17.2) s for 5° tilt, 14.6 (IQR: 11.7–16.4) s for 10° tilt, and 13.6 (IQR: 11.4–16.3) s for 15° tilt (Table 2). The differences in the FTSST duration among the three heel-elevation conditions were statistically insignificant. Overall, the FTSST duration was reduced in the heel-elevated condition compared to the flat condition, with a median difference of 2.3 (IQR: 0.5–5.4) s and a percentage reduction of 14.0 (IQR: 6.7–27.1) %. A significant reduction in the FTSST duration was observed for the 5° tilt (corrected P < 0.01), 10° tilt (corrected P < 0.05), and 15° tilt (corrected P < 0.01) conditions compared to the flat condition. When excluding one participant who performed the FTSST on a high chair (47 cm), FTSST duration was significantly reduced under all heel-elevated conditions (P < 0.05); therefore, this participant was included in the subsequent analysis.
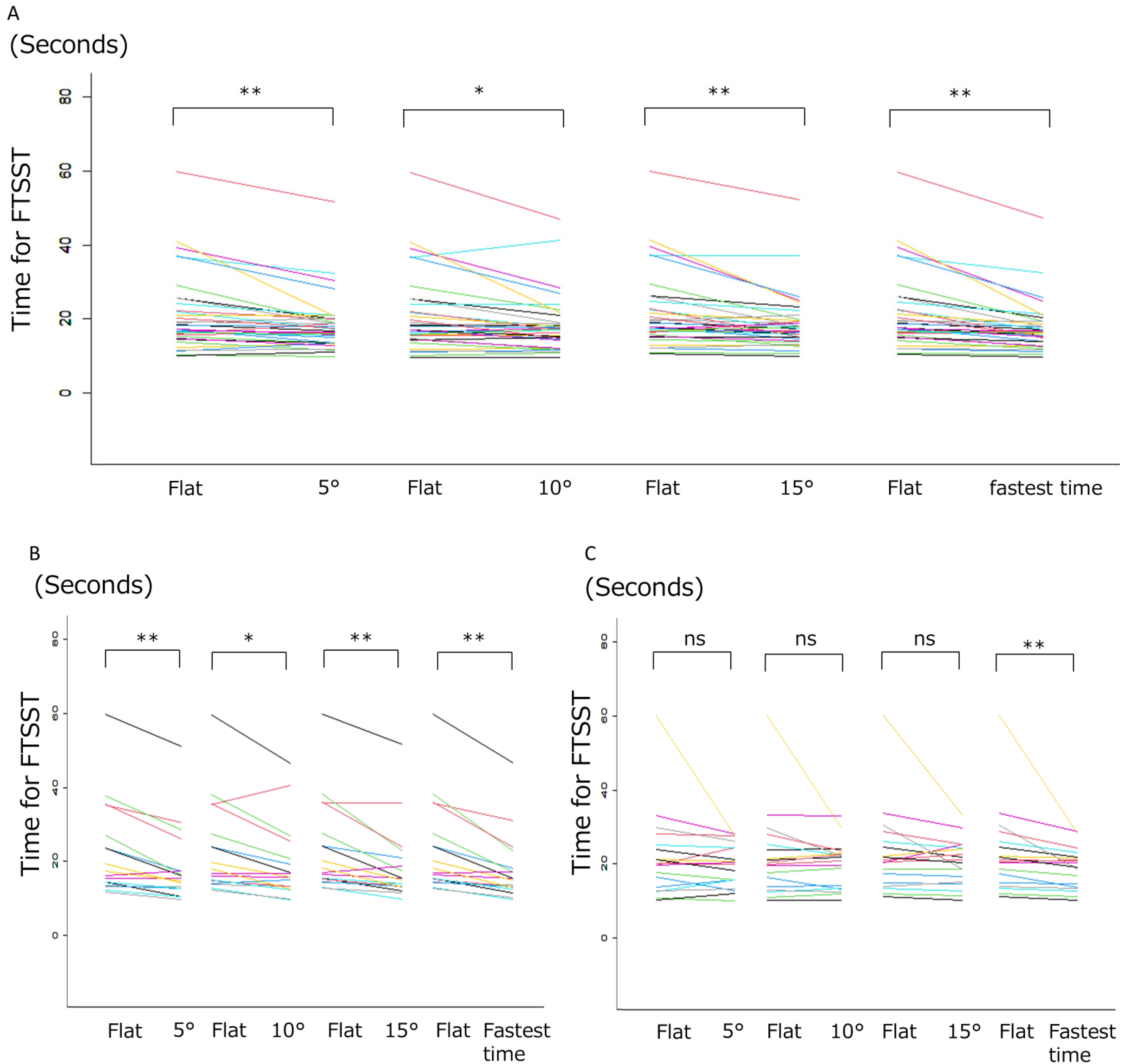
Heel-Elevation Effect in all 36 Participants (A), Groups A (B) and B (C). The Line Indicates the Change in FTSST Duration Between the Flat and Heel-Elevation Conditions in Each Participant. *: P < 0.05, **: P < 0.01; FTSST, The Five Times Sit-to-Stand Test.
Heel-Elevation Effect in all 36 Participants (Total), Groups A and B.
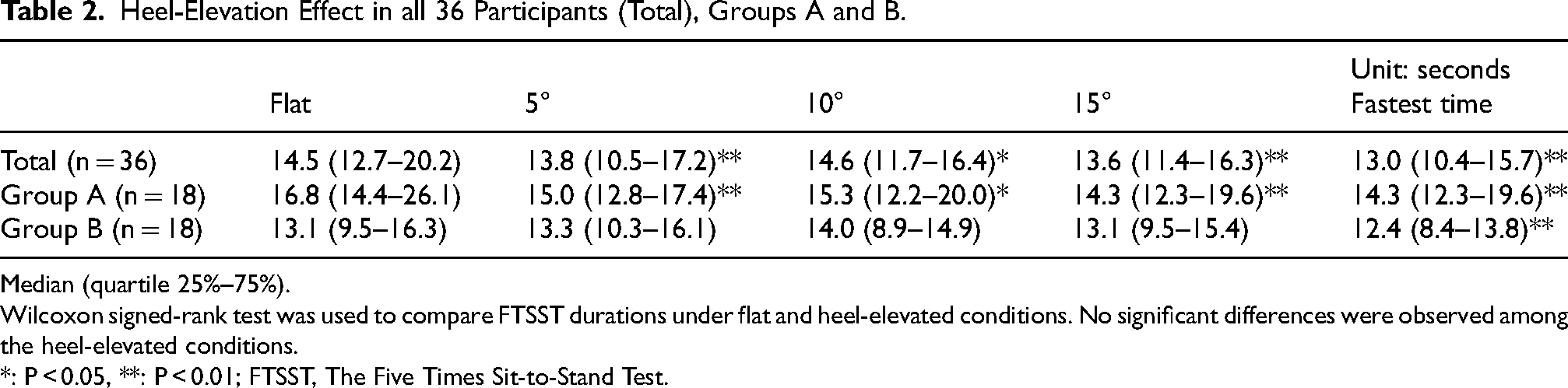
Median (quartile 25%–75%).
Wilcoxon signed-rank test was used to compare FTSST durations under flat and heel-elevated conditions. No significant differences were observed among the heel-elevated conditions.
*: P < 0.05, **: P < 0.01; FTSST, The Five Times Sit-to-Stand Test.
Figure 2B demonstrates the heel-elevation effect observed in Group A (n = 18). The median FTSST duration in the flat condition was 16.8 (IQR: 14.4–26.1) s. Under the heel-elevated condition, the FTSST durations were: 15.0 (IQR: 12.8–17.4) s for 5° tilt, 15.3 (IQR: 12.2–20.0) s for 10° tilt, and 14.3 (IQR: 12.3–19.6) s for 15° tilt (Table 2). The differences in the FTSST duration among the three heel-elevation conditions were statistically insignificant. The changes in FTSST duration between the heel-elevated and flat conditions did not differ among the three heel-elevated conditions. The median difference in the FTSST duration between the fastest heel-elevated condition and the flat condition was 4.3 (IQR: 2.2–8.2) s, corresponding to a reduction rate of 24.2 (IQR: 13.6–30.0) %. The FTSST duration was consistently reduced under all heel-elevated conditions.
Figure 2C shows the effect of heel elevation observed in Group B (n = 18). The median FTSST duration in the flat condition was 13.1 (IQR: 9.5–16.3) s. Under heel-elevated conditions, the FTSST durations were 13.3 (IQR: 10.3–16.1) s for 5° tilt, 14.0 (IQR: 8.9–14.9) s for 10° tilt, and 13.1 (IQR: 9.5–15.4) s for 15° tilt (Table 2). FTSST durations and the differences between the flat and each heel-elevated condition did not differ significantly among the three heel-elevated conditions. The differences in the FTSST duration among the three heel-elevated conditions were statistically insignificant. The fastest FTSST duration in the heel-elevated conditions was reduced compared to the flat condition, with a median change of 0.9 (IQR: 0.3–2.3) s and a reduction rate of 10.3 (IQR: 2.4–15.0) %. However, the changes for any of the individual tilt conditions were insignificant.
Figure 3 shows ankle dorsiflexion ROM at each heel-elevation angle producing the fastest FTSST time. Among the 12 cases with the fastest time under the 5° heel-elevated condition, the median ankle dorsiflexion ROM was 15.3° (IQR: 5.2–21.7). Among the 10 cases with the fastest time under the 10° heel-elevated condition, the median ankle dorsiflexion ROM was 12.5° (IQR: 9.0–21.1). There were 14 cases with the fastest time at a heel-elevated condition of 15°, and the median ankle dorsiflexion was 15.9° (IQR: 10.2–18.9). Spearman's rank correlation coefficient was 0.08 (P = 0.63), indicating no significant correlation.
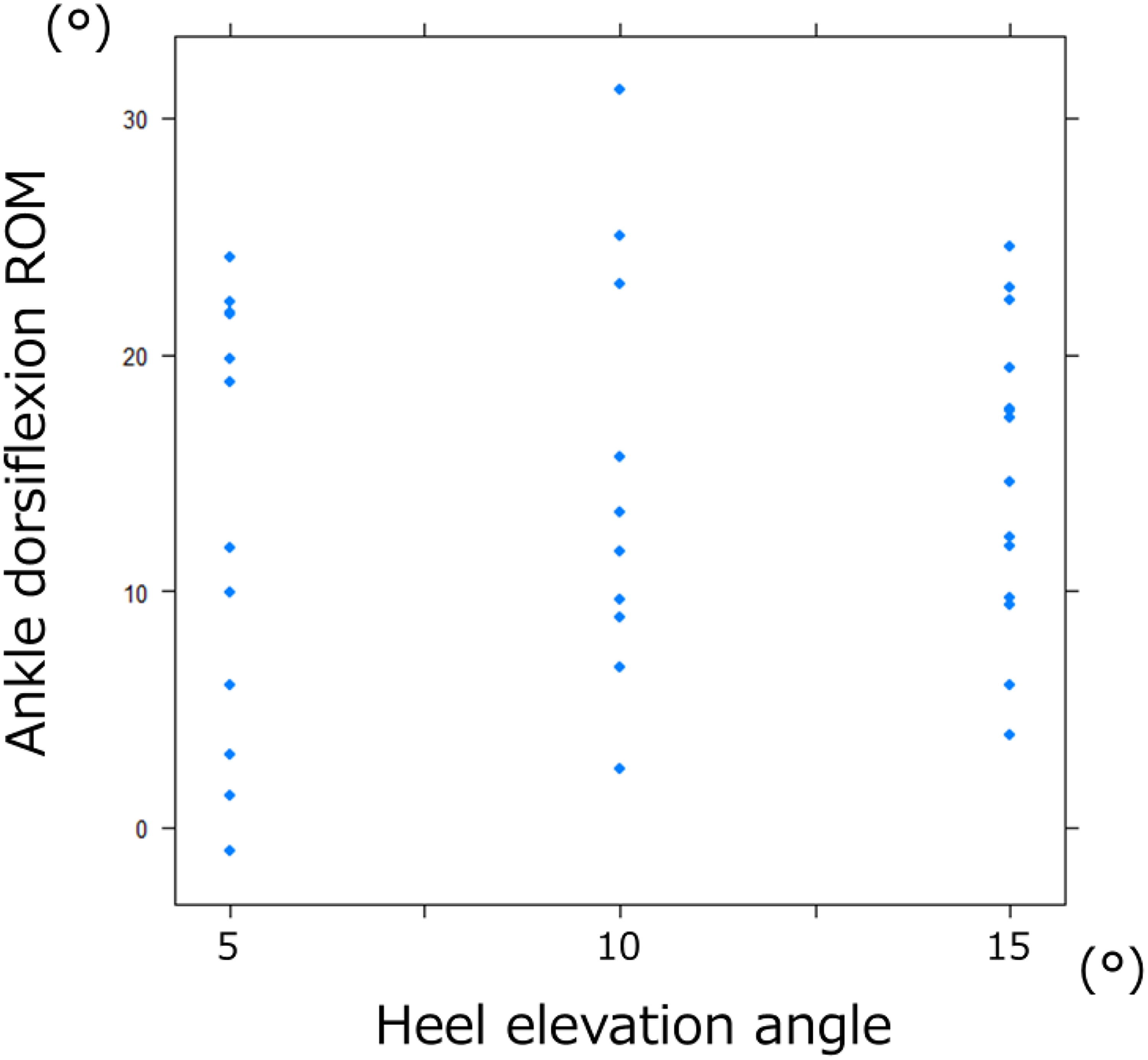
Relationship Between Heel-Elevation Angle and Ankle Dorsiflexion ROM Producing the Shortest FTSST Time. No Significant Correlation is Observed Between Heel-Elevation Angle and Ankle Dorsiflexion ROM (Correlation Coefficient r = 0.08, P = 0.63). FTSST, The Five Times Sit-to-Stand Test; ROM, Range of Motion.
Since these results indicated that the effect of heel elevation on sit-to-stand movement was independent of the tilt angle, we used the fastest FTSST time as the representative measure of heel elevation. Variables that exhibited correlations with changes in FTSST duration between the fastest heel-elevated and flat conditions were scores related to quickness (r = 0.38), standing (r = 0.86), walking (r = 0.41), slowness (r = 0.49), posture (r = 0.50), and the total UPDRS III score (r = 0.50). Additionally, correlations were observed between knee extension strength-to-weight ratio (r = −0.61), Hoehn and Yahr Stage (r = 0.47), and FTSST duration in the flat condition (r = 0.73). The test procedure—performing the heel-elevated condition before (Group B) or after (Group A) FTSST measurement in the flat condition—was also associated with changes (median: Group A, 4.35 s; Group B, 0.95 s; P = 0.0078), suggesting a carryover effect of multiple tests under the heel-elevated condition. Multivariable regression analysis using the stepwise method revealed that the FTSST duration in the flat condition and the standing score on the UPDRS III were significantly associated with the observed shortening effects induced by heel elevation (Table 3). The slower the FTSST duration in the flat condition and the greater the standing function impairment, the more pronounced the effect of the heel elevation on standing (standardized partial regression coefficient of FTSST time in the flat condition: 0.66, 95% confidence interval 0.43–0.90; P < 0.01; standardized partial regression coefficient of standing score in UPDRS III: 0.26, 95% confidence interval 0.03–0.49, P < 0.05). The FTSST duration of the flat condition exhibited the most substantial influence under flat conditions. The coefficient of determination was 0.73, and it remained at 0.72 after adjusting for the degrees of freedom. To account for potential carryover effects, the test procedure was included in the regression model, and the two factors remained significantly associated with the shortening effect of FTSST duration (standardized partial regression coefficient of FTSST time in the flat condition: 0.68, 95% confidence interval 0.45–0.91; P < 0.01; standardized partial regression coefficient of standing score in UPDRS III: 0.31, 95% confidence interval 0.061–0.56, P < 0.05).
Factors Associated with the Effects of Heel-Elevation in Multiple Regression Analysis.
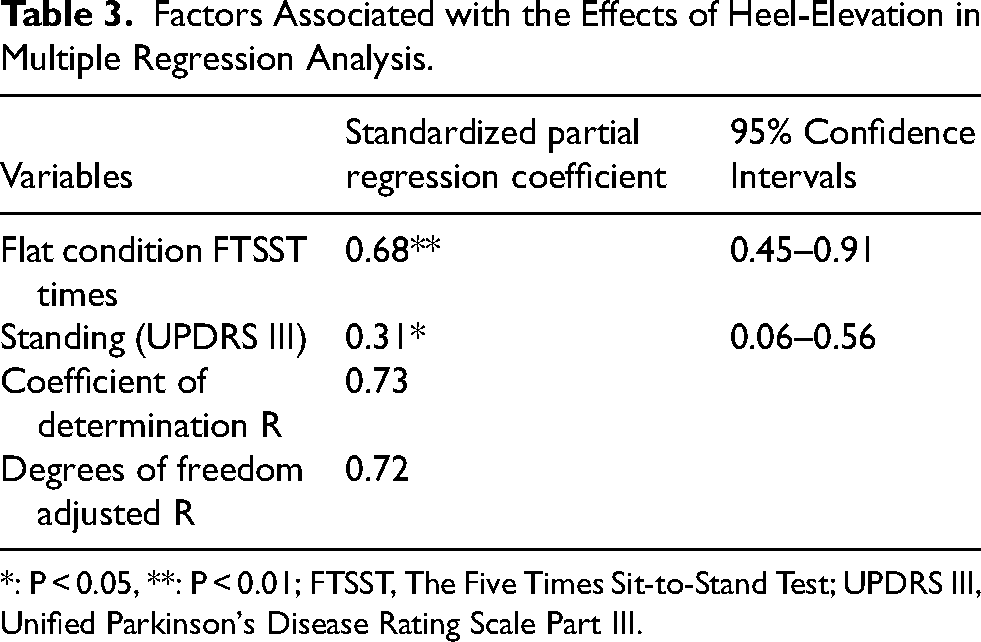
*: P < 0.05, **: P < 0.01; FTSST, The Five Times Sit-to-Stand Test; UPDRS III, Unified Parkinson's Disease Rating Scale Part III.
Discussion
This randomized crossover trial revealed that heel-elevation intervention effectively reduced the duration of the sit-to-stand transition in patients with PD. No changes were observed in the effects among plates with different tilt angles, and the optimal heel-elevation angle for sit-to-stand movement was independent of ankle dorsiflexion ROM. The fastest FTSST duration under the heel-elevated conditions was reduced by 14.0% when compared to the flat condition, and this effect was replicated in both groups. Heel-elevation effects were positively associated with the PD severity and FTSST duration in the flat condition and negatively associated with knee extension strength. Multivariate regression analyses revealed that individuals with more pronounced standing dysfunction experienced a more substantial impact of heel elevation. Overall, the more severe the standing impairment in patients with PD, the more pronounced the effectiveness of the heel-elevation intervention on rising time.
In Group A, where the flat condition was the initial setting, heel elevation was effective in reducing the duration of sit-to-stand movements under all tilt-up conditions compared with the flat condition. In contrast, in Group B, in which the heel-elevated condition was initially implemented, the fastest FTSST duration in the heel-elevated condition was shorter than that in the flat condition. However, the effects were not statistically significant between the flat and tilted conditions. The attenuated effect in Group B may partly reflect a carryover effect, as repeated FTSST measurements (three trials) likely shortened the FTSST duration in the flat condition. Indeed, the median time for the 1st, 2nd, 3rd, and 4th (flat condition) tests showed a gradual decrease, and the FTSST duration in the flat condition was significantly shorter in Group B than in Group A.
Patients with PD exhibit less forward movement of their center of gravity during the transition from a seated to a standing position than healthy individuals (Inoue, 1992). Furthermore, the more severe the PD, the more posterior the center of pressure on the soles of the feet is shifted (Guehl et al., 2006; Oku et al., 1991). This means that patients with PD tend to stand without fully transferring their center of pressure to the forefoot. In severe PD cases, patients position their center of gravity toward the posterior side, even in the standing position while extending their lower limbs and trunk, making it difficult to control their posture in the sitting position from the standing position. Oku, Amimoto, and Yamasaki reported that patients with moderate-to-severe PD (those beyond Hoehn and Yahr stage II) could effectively move their center of gravity forward, reduce postural sway in the standing position, and enhance their ability to deliberately shift their center of gravity in various directions using heel-elevation supplementation (Oku et al., 1995). In this study, we did not directly measure center of gravity sway; therefore, this interpretation remains speculative and should be viewed with caution. Nonetheless, heel elevation may have allowed patients with PD to shift their center of gravity onto the forefoot during the hip elevation phase at the initiation of standing from the flexed position. Moreover, they appeared able to maintain their center of gravity on the forefoot while standing, which may have contributed to more stable sitting action.
Optimal heel-elevated conditions were not established in this study. When exploring the relationship between ankle dorsiflexion ROM and the height of the elevation plate, which resulted in the most effective reduction in FTSST duration, no association was observed. The reduction in FTSST duration was also comparable across the three heel-elevation angles. Although the small sample size may have influenced the results, the optimal angle of heel elevation does not appear to depend solely on ankle dorsiflexion ROM, nor does it show a linear relationship between angle and effect. Oku, Amimoto, and Yamasaki employed a method in which the heel elevation height was gradually increased until the standing posture of the patients became stable (Oku et al., 1995). More severely affected patients typically require a higher degree of heel elevation to stabilize the standing posture. However, the optimal heel-elevation height may vary for each individual, depending on their specific case and needs.
The effects of heel elevation on the sit-to-stand action were associated with the disability level while standing, which is in accordance with previous studies (Oku et al., 1995). Additionally, we revealed that exercises involving movements such as turning over and getting up, guided by visual cues and graded by difficulty, improved the agility of these movements in patients with PD. These effects are more pronounced in patients with greater disability levels (Nakayama et al., 2022).
Heel-elevation intervention may support rehabilitation of sitting-to-standing movements in PD patients and reduce impairments in activities of daily living. Although this study used tilting plates for heel elevation, the use of insoles cut into the shape of the heel may yield similar effects in daily activities. However, it is necessary to evaluate safety in the living environment under the supervision of an expert. In particular, the height of the heel lift should be adjusted gradually with careful consideration of each individual case. Additionally, heel-elevation intervention was more effective in individuals with weak knee-extension strength in this trial. Given that sarcopenia is more prevalent among patients with PD than among non-PD controls (Peball et al., 2019), this intervention could be particularly beneficial in a considerable proportion of patients with PD who have lower limb weakness. Interventions to further improve the ability of patients with PD to perform sit-to-stand movements may be synergistically effective if visual and auditory cues are provided in addition to heel elevation (Mak & Hui-Chan, 2008).
Limitations
This study had several limitations. While a crossover trial design was employed to minimize the required sample size, the multiple trials conducted in various tilt conditions may have introduced the carryover effect, potentially diminishing the true effects of the heel-elevation intervention. Furthermore, as three different tilt conditions were included in the heel-elevated condition, the effects may have interacted and been influenced by the trial order, making it challenging to identify the optimal angle. This result may be due to insufficient detection power to capture angle-specific differences.
The washout period in this study was set to 10 min to account for intra- and interday variations in disease and fatigue resulting from repetitive sit-to-stand movements. However, the lower improvement rate in Group B than in Group A indicates that the washout period in this study may not have adequately mitigated the carryover effect between trials.
In this study, we did not conduct a center of gravity sway test, so the effect of heel elevation on forward center of gravity shift is only speculative. Further research is needed to investigate this mechanism.
Conclusion
This randomized crossover trial demonstrated that heel-elevation improves sit-to-stand performance in patients with PD by reducing the FTSST duration. The effect tended to be more pronounced in individuals with more severe standing dysfunction under flat conditions and slower transition from sitting to standing. The effect of heel elevation on sit-to-stand movement did not appear to depend solely on ankle dorsiflexion ROM or on the degree of heel elevation. The findings suggest that individualized heel-elevation strategies may enhance mobility and functional independence in patients with PD.
Supplemental Material
Footnotes
Ethical considerations and Consent to Participate
This study was conducted in accordance with the “Declaration of Helsinki” and the “Ethical Guidelines for Life Sciences and Medical Research Involving Human Subjects” and was approved by the Ethical Review Board of Kochi Medical School (approval number: 2022-36, Ethics Committee Review Date: July 12, 2022). The study protocol was registered in the clinical trial registration system of the University Hospital Medical Information Network before study initiation (UMIN000048428). The clinical trial registration was prospective and performed prior to recruitment of the first study participant. Patient registration began on July 21, 2022 and ended on July 22, 2023. Before participating in the study, participants were informed of its purpose and content, that their personal information would be kept confidential, and that their free will would be respected in participating in the study. Their written informed consent was obtained. We confirm that we have read the journal's guidelines on issues involved in ethical publication and affirm that this work is consistent with these guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the present study will be available from the corresponding author based on the guidelines of the Ethics Committee of Kochi Medical School upon reasonable request from any qualified investigator.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.