
Abstract
Background
Parkinson's disease (PD) is a neurological disorder that significantly impacts individuals, their families, and the healthcare system. Alongside drug therapies and surgical interventions, exercise has shown potential in improving motor and non-motor symptoms. This study explored perspectives of individuals with PD, care partners, and program providers regarding a community-based exercise program for PD.
Methods
Individuals with PD (Hoehn & Yahr stages I-III), on a stable medication regime, who participated in a PD-specific community-based exercise program twice weekly for at least 12 weeks, along with care partners and program providers were recruited. In-depth interviews were conducted with individuals with PD (n = 17), care partners (n = 7), and program providers (n = 3) from January to May 2024. Data were analyzed using an interpretative phenomenology analysis and mapped onto a behavior-change model. Two patient advisors and care partners assisted in data analysis and interpretation.
Results
Participants highlighted the PD-specific nature of the program and group exercise benefits as key motivators. Pre-program challenges included difficulties obtaining a diagnosis, adapting to non-motor symptoms, medication side effects, and finding motivation. Post-program outcomes included symptom improvement, mutual motivation, community support, and reduced self-consciousness, prompting the recommendation of greater community awareness. Barriers to participation included transportation difficulties and cost. These findings suggest addressing barriers is essential to enhance accessibility and program benefits.
Conclusions
The PD-specific exercise program was perceived as beneficial to overall health and wellness, providing physical, emotional, and social benefits. A lack of awareness about the significance of exercise in PD remains a critical challenge.
Background
Parkinson's disease (PD) is recognized as the “fastest-growing neurological disorder” and a leading cause of disability worldwide (Dorsey & Bloem, 2018; Schiess et al., 2022), contributing to 5.8 million disability-adjusted life-years (DALYs) in 2019 (Ou et al., 2021). Motor and non-motor symptoms associated with PD progressively worsen over time (Crighton et al., 2024; Dorsey & Bloem, 2018), leading to functional limitations and disability (Chaudhuri et al., 2024; Crighton et al., 2024; Dorsey & Bloem, 2018; Jankovic, 2008; Schiess et al., 2022).
Drug and surgical therapies can provide symptomatic relief for motor symptoms (e.g., tremors, slowness, and stiffness) and some non-motor symptoms (e.g., sleep and mood disturbances) (de Bie et al., 2020; Dijk et al., 2020; Foltynie et al., 2024; Mahlknecht et al., 2022). Non-drug treatments, such as exercise interventions, have also shown promise in improving both motor and non-motor symptoms and enhance quality of life in individuals with PD (Alberts & Rosenfeldt, 2020; Irons et al., 2024; Ramaswamy et al., 2018).
Emerging evidence suggests that exercise may have disease-modifying effects (Ahlskog, 2018; Schootemeijer, van der Kolk, Bloem et al., 2020), with different forms and intensities of exercise interventions offering distinct benefits (Choi et al., 2020). Aerobic and resistance training exercises, particularly when combined, have been shown to improve both physical and cognitive function, with recent evidence supporting multimodal exercise programs that integrate balance and cognitive training (Corcos et al., 2013; David et al., 2012; Falvo et al., 2008; Ferrusola-Pastrana et al., 2023). However, the evidence shows that long-term adherence is essential to maximize exercise benefits, as discontinuation of exercise, even for 6 months, results in regression of benefits (Booth et al., 2012). Despite this, maintaining long-term adherence to exercise programs can be challenging due to barriers such as disease progression, changing response to medications, apathy, impact of motor and non-motor symptoms, fluctuation in motivation, and lack of awareness about exercise benefits (Schootemeijer, van der Kolk, Ellis et al., 2020).
Behaviour-change theories and models are valuable for understanding some of the factors that influence adherence and motivation to exercise. The capability, opportunity, motivation, and behavior (COM-B) model is particularly useful in examining health behaviours across various contexts, as it identifies facilitators and barriers to participation and adherence (Michie et al., 2011; Webb et al., 2022; Yang et al., 2024). Qualitative research is essential for understanding patients’ perspectives (Aspers & Corte, 2019), yet relatively few studies (Hunter et al., 2019) have explored the experiences of individuals with PD, their care partners, and program providers within PD-specific community-based exercise programs.
This study addresses these gaps by exploring the experiences of individuals with PD, their care partners, and program providers about a PD-specific community-based exercise program and its impact on motor and non-motor symptoms, as well as quality of life. It also investigates motivating factors, barriers, and facilitators to exercise adherence through the lens of the COM-B framework. Findings may provide insights that can inform the design and implementation of more effective and sustainable community-based exercise programs for PD.
Methods
Study Design and Setting
A phenomenological qualitative approach was used (Creswell & Poth, 2016; Guetterman et al., 2015), a research method that seeks to explore and interpret phenomena as consciously experienced by individuals (Flood, 2010). The findings of this qualitative study were presented in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ), 32-item checklist designed to ensure thorough and transparent reporting of qualitative research (Tong et al., 2007). The University of Alberta's Human Research Ethics Board approved this study (Ethics ID: Pro00122937).
Participants and Recruitment
Participants who attended a PD-specific community-based exercise program were purposively recruited between January and May 2024, based on age, sex, Hoehn and Yahr stages, and years since PD diagnosis (Stratton, 2024). Care partners who provided care and assistance, were also purposively sampled. Additionally, three staff members involved in program development and delivery were recruited to provide insights into program design, implementation, and opportunities for improvement. Inclusion criteria for individuals with PD included: a diagnosis of PD, age 50 years or older, Hoehn and Yahr stage of I–III, a self-reported stable drug regimen, and participation in the community-based exercise program under study for at least 12 weeks. Exclusion criteria included having another medical condition other than PD or being unable to communicate in English to be able to participate in the interviews.
Community-Based Exercise Program
The Parkinson Association of Alberta (PAA) offers both in-person and virtual PD-specific exercise programs through its Edmonton-based center, which serves the entire province. One such program is a 12-week, twice-weekly exercise intervention that combines structured and unstructured physical activity, with a focus on neuromuscular strength training. The program consists of 24 one-hour sessions, costing approximately $65 per hour. Participants in the exercise program are encouraged to attend all sessions, with no drop-in option available. However, participants may miss classes sporadically due to health issues, vacations or other personal reasons. The focus of the exercise program includes postural orientation, lower extremity strength, and functional exercises such as stepping lunges, step-ups, squats, and sit-to-stands. Led by an exercise specialist with expertise in PD, the program progresses in difficulty under supervision, incorporating manual resistance, weights, and unstable surfaces. Following a physiotherapist's assessment, participants are assigned to one of the following groups based on their abilities: 1)
Data Collection
Semi-structured interviews were conducted with participants either in-person (n = 15) at the PAA or via Zoom (n = 2) depending on their preference (Gray et al., 2020). One researcher (AK) led participant interviews, while a second researcher (VEE) was involved with interviewing staff members. The research team had no role in the development or delivery of the exercise program and no affiliations with the PAA. Interview questions were collaboratively developed by researchers, patient advisors, and through a literature review and field observations at the PAA (Råheim et al., 2016; Sanjari et al., 2014; Wa-Mbaleka, 2020). These questions explored participants’ views on exercise benefits and challenges, enrollment facilitators, and perceptions of the program. Interview guides for individuals with PD, care partners, and program providers are presented in Online Supplement Tables 1.1–1.3. Each interview was done in-person or by Zoom and lasted approximately 20–50 min. In one instance, a participant's spouse contributed to the interview due to some difficulty with communication, otherwise participants and their care partners were interviewed separately. Researchers created field notes after each interview, reflecting on observations and key insights. Interviews were audio-recorded, transcribed using Otter.ai (Mountain View, California USA (https://otter.ai)) and the generated transcripts were reviewed for accuracy by the researchers. Saturation was reached when additional interviews with individuals with PD no longer provided new insights to inform the themes. This occurred after the 15th interview, with two additional interviews reinforcing existing themes (Hennink & Kaiser, 2022).
Data Analysis
Data analysis followed the principles of interpretative phenomenological analysis (IPA) which takes an inductive approach (Smith, 2017; Tindall, 2009). The process began with multiple readings of transcripts to build familiarity with the data, followed by identifying significant statements and meaningful segments for coding. This bottom-up approach allowed themes to emerge organically from participants’ narratives. Using NVivo 14 software, transcripts were analyzed line by line, generating initial codes that captured participants’ perceived experiences (Mortelmans, 2019). Themes identified from each transcript were refined and analyzed for recurring patterns across the dataset. This iterative process ensured that findings were deeply grounded in participants’ perspectives. To enhance rigor, two researchers (AK, VE) independently coded the transcripts to ensure consistency and reliability in the analysis. Patient advisors provided insights to validate the findings and ensure alignment with the lived experiences of individuals with PD and their care partners (Jackson et al., 2020). Senior researchers (CAJ, MW) contributed detailed feedback to refine the analytical process and ensure methodological rigor. Data triangulation was achieved by integrating multiple sources, including field notes, researcher observations during visits to the PAA, interviews with individuals with PD, care partners, and program providers (Noble & Smith, 2015; Smith, 2017). The barriers and facilitators identified were mapped to the COM-B model as capabilities (physical and psychological factors), opportunities (physical and social factors), and motivations (automatic and reflective).
Results
A total of 27 interviews were conducted for this study (individuals with PD, n = 17; care partners, n = 7; program providers, n = 3). The demographic characteristics of individuals with PD are presented in Table 1. The mean (standard deviation, SD) age of care partners was 70.6 (7.7) years and 70% were females. The program providers included two staff members with administrative roles (actively engaged with the PAA participants) and one exercise instructor.
Demographic Characteristics of Participants with PD.
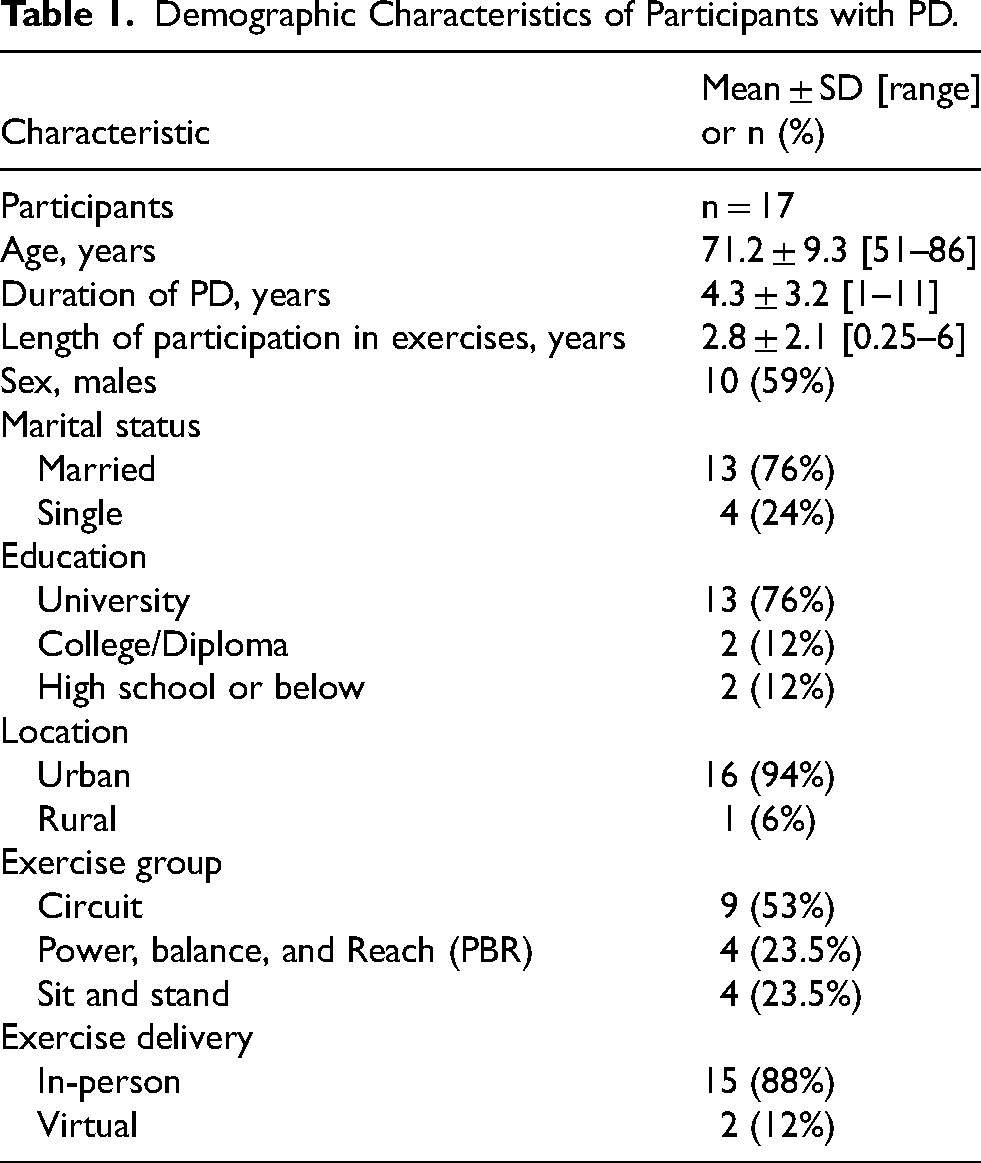
Fifteen individuals with PD attended in-person classes, while two participated in the virtual Circuit-2 class. One virtual participant living in the urban center chose online sessions due to transportation challenges, while the other was from rural Alberta. Although most participants renewed their memberships and attended regularly over the years, they occasionally missed sessions due to factors such as inclement weather, illness, or personal vacations.
Themes
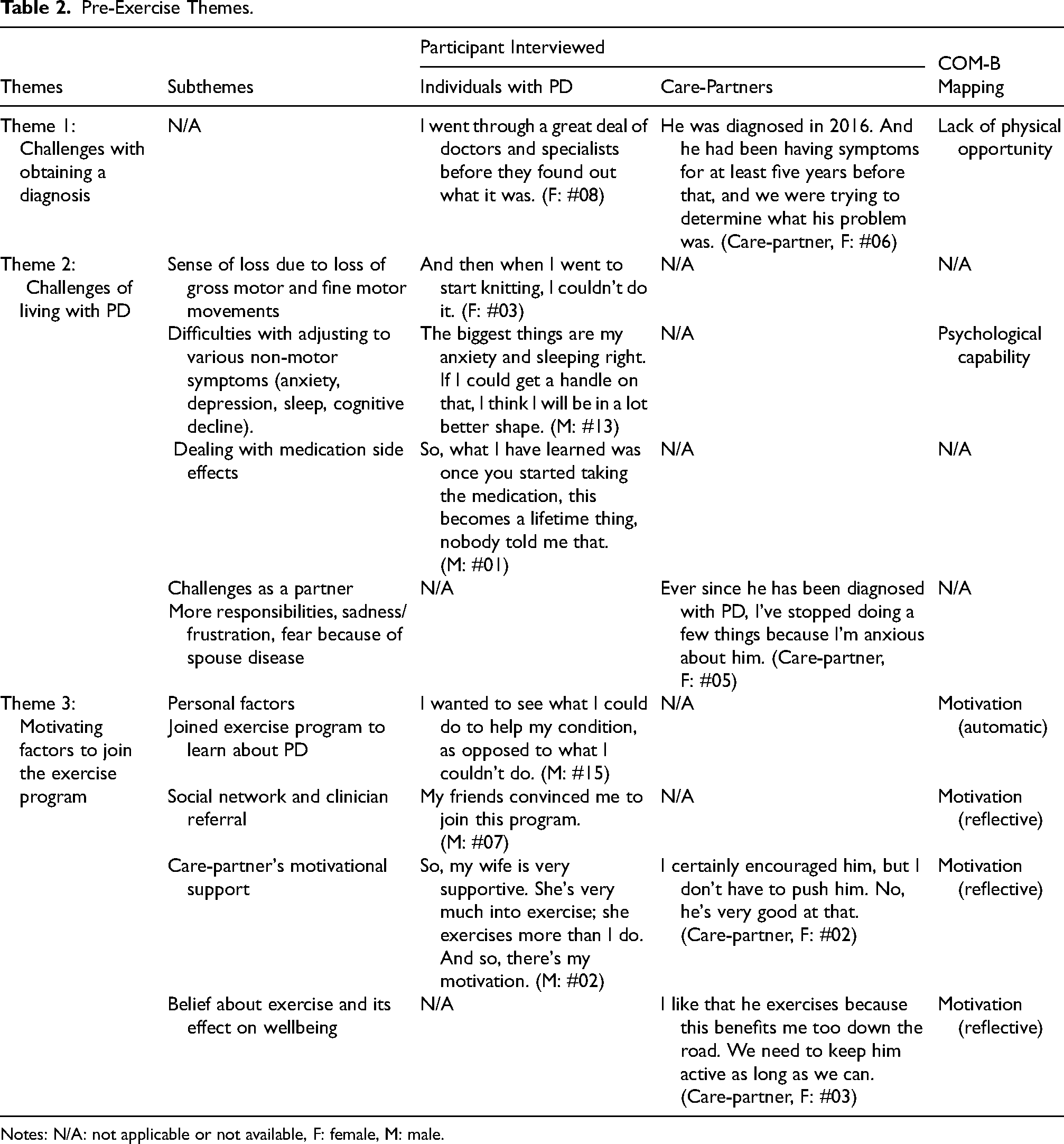
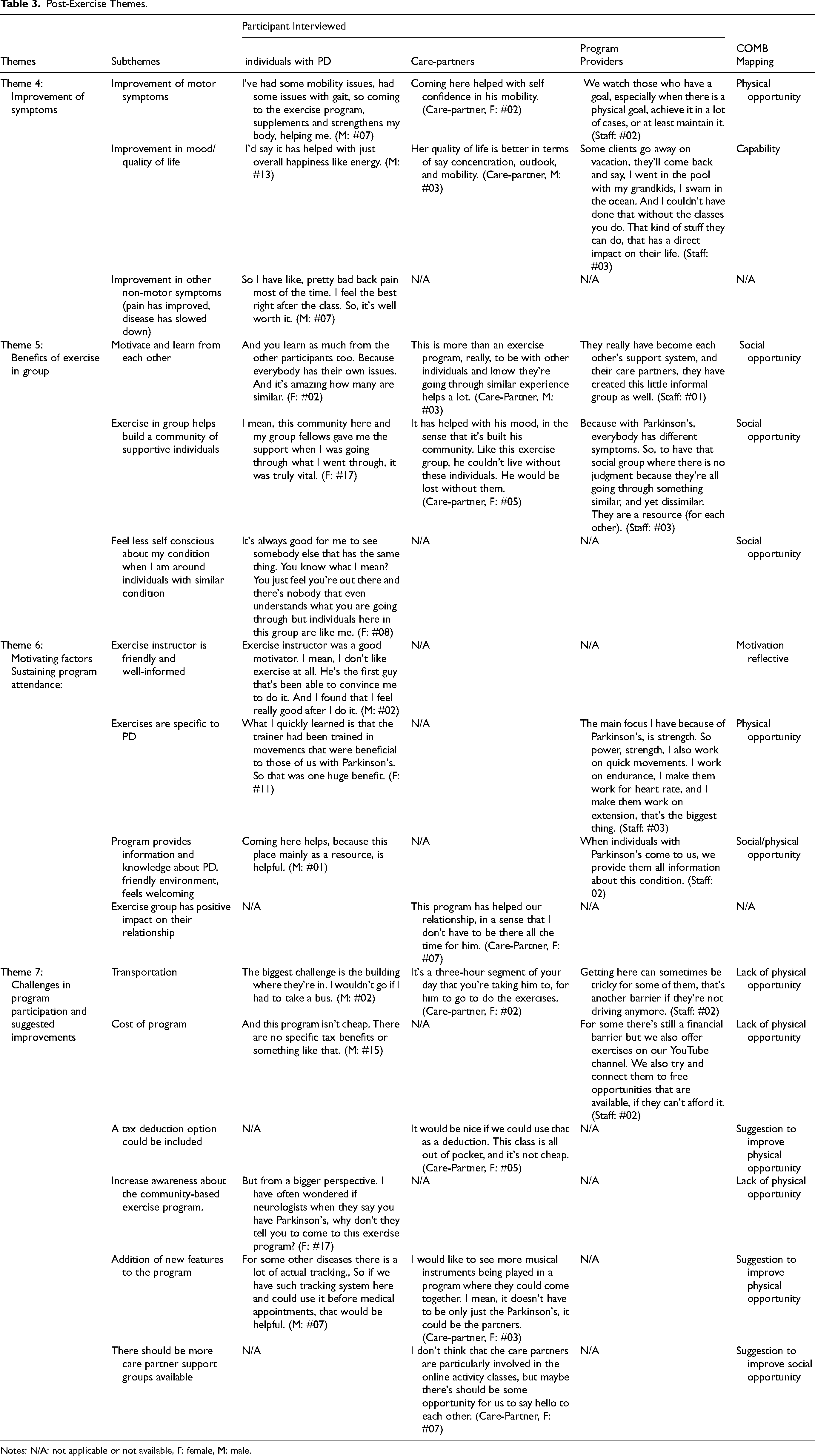
A total of seven themes were identified and categorized into two groups: pre-exercise and post-exercise themes, as shown in Tables 2 and 3. Each group of themes alongside their subthemes and supporting quotes are presented. Additionally, each theme was mapped to the COM-B model, where applicable, to indicate the presence or absence of relevant factors within the framework.
Pre-Exercise Themes.
Notes: N/A: not applicable or not available, F: female, M: male.
Post-Exercise Themes.
Notes: N/A: not applicable or not available, F: female, M: male.
Pre Exercise Challenges and Motivators (Themes 1–3)
Table 2 presents the themes that emerged as significant motivational factors influencing the participation of individuals with PD in exercise groups. Pre-exercise themes focus on motivators that encourage individuals to participate in the exercise program. Notably, nearly all (n = 15), participants expressed motivation to engage in exercise programs. For some participants (n = 5), their care partners played a crucial role in encouraging and supporting their exercise routines.
One theme demonstrated that few individuals were directed to community resources for PD, such as the PAA, by their neurologist or physician (n = 7), while many individuals independently discovered these resources (n = 10). Additionally, two themes appeared, that were not directly related to the study's objectives. One of them was delay in diagnosis of PD and associated challenges. Both individuals with PD (n = 14) and their care partners expressed that the diagnostic process for PD is often lengthy and frustrating. This prolonged period can be emotionally challenging due to the uncertainty involved. Furthermore, the delay in diagnosis indirectly causes delays in treatment and disease management, including exercise interventions.
Another theme was the challenges associated with living with PD. Within this theme, a prominent subtheme emerged—a sense of loss. This subtheme was illustrated through unique narratives of participants (n = 13) who described the loss of hobbies or aspects of their lifestyle. As PD causes a decline in fine motor and gross motor movements, many hobbies such as knitting, woodworking, and swimming may no longer be possible. This sense of loss can contribute to a decline in mood among individuals with PD.
Post Exercise Themes
Table 3 highlights the four post-exercise themes that were identified. The first two themes identified encompass the perceived benefits of exercise program participation. While the other two themes represent the motivational factors that promote long-term adherence, the barriers and suggestions for improvements reported by both individuals with PD, care partners, and program-providers. A brief description of each theme is provided below.
Theme 4: Improvement of Symptoms
Most participants with PD reported overall subjective improvement in mobility, strength, and endurance. Additionally, eight participants noted enhanced flexibility and reduced rigidity, while five participants observed better balance since joining the exercise program. Nine participants reported improved mood since joining the exercise program, while six participants noted increased confidence in their ability to walk and move and felt more hopeful about their mobility. Six participants reported overall improved pain since they joined the exercise program, while five of them perceived that participation in the exercise program may have played a role in slowing down the progression of the disease. Six care-partners reported that the program helped their partners to stay active and has enhanced their mobility confidence. One care-partner emphasized that the exercise increased strength. Some care-partners mentioned that participating in the exercise program uplifted their partner's mood and had a positive effect on their quality of life. Program providers reported that they often observed a noticeable improvement in overall mobility of the individuals with PD after a few months of joining exercise program. Program providers also reported that they often receive feedback from participants that the program helped to bring a positive change in quality of life of individuals with PD.
Theme 5: Benefits of Exercise in Groups
Fourteen participants with PD reported that group exercise provides mutual motivation to maintain physical activity. When exercises were challenging, emotional support from peers helped maintain self-esteem, fostering a supportive and encouraging environment. Participants highlighted that the sense of community from the group is crucial for their well-being. The exercise program's community helped them discuss challenging issues, such as diverse symptoms and medication side effects. Many noted that this sense of community indirectly improved their mood and overall well-being. Participants expressed that they feel less self-conscious when exercising with individuals who have the same disease, compared to exercising with a non-PD population. This shared experience is an important motivating factor that sustains their ongoing participation in the exercise program. Five care partners noted that the exercise group motivated their partners, as it included others with similar disease severity, fostering mutual encouragement and shared learning. Five care-partners stated that individuals in the exercise group understand their partner's health condition, making them happy that their partner is finally in a place where they can express their problems, feel heard and understood. Program providers also expressed that the community these individuals with PD have built play a vital role in terms of providing them support and motivation. Program providers mentioned that individuals with PD provide unwavering emotional support to each other.
Theme 6: Motivating Factors Sustaining Program Attendance
Fifteen participants with PD (including both in-person and online classes) appreciated the instructor's PD-specific knowledge and encouragement in fostering a supportive atmosphere. Thirteen participants valued the exercise program's design in enhancing their health and quality of life. Five care partners noted its positive impact on their relationships and respite from responsibilities. Providers emphasized the program's tailored services for different stages of PD, including education and exercise. Participants appreciated the PAA for providing PD-specific information, program management, and a supportive environment.
Theme 7: Challenges in Program Participation and Suggested Improvements
Participants generally reported few challenges with program participation. However, seven participants with PD identified commuting as a significant barrier, often relying on partners due to their inability to drive. Although three participants noted that transportation is not currently an issue, they acknowledged it could become a challenge in the future possibly due to deteriorating health status. Both care partners and program providers identified transportation as a challenge, with care partners specifically reporting difficulties in transporting their partners, particularly during adverse weather. Nevertheless, they recognized the program's importance and ensured attendance. Five participants identified the program's cost as a financial challenge but deemed the benefits substantial enough to justify the expense, emphasizing the positive impact on their health. After learning that cost was a concern for participants, providers acknowledged it as a potential barrier to participation. To address the financial burden of out-of-pocket expenses, a few participants suggested tax deduction options, as the program is not covered by government funding.
Participants made various suggestions, including some additional recommendations that did not emerge as main themes. Nine participants recommended enhancements to the PAA program, such as tracking symptoms to monitor disease progression, incorporating dance and music classes, providing access to diet consultants, organizing more social events, and including tailored cognitive exercises. Some of these existed previously but may have been trimmed down due to funding barriers. Care partners emphasized the necessity for additional support groups specific to care partners, both in-person and online, to foster mutual support among care partners. They also supported the addition of music and dance classes for individuals with PD and their care partners.
Discussion
In this study, people with PD perceived a PD-specific community-based exercise program as a positive experience, noting improvements in physical symptoms and psychological well-being. Seven themes, classified as pre-exercise and post-exercise, show program benefits, challenges, motivations, and perceived changes in quality of life. These themes provide valuable insights into the PD journey from the perspectives of individuals with PD, their care partners, and program providers.
Pre-exercise themes primarily highlight the motivational factors that encouraged individuals with PD to join the exercise program. According to the COM-B model, motivation—both automatic and reflective—is essential for behaviour change (Yang et al., 2024). Our findings showed that participants were intrinsically motivated to exercise (Webb et al., 2022; Yang et al., 2024), demonstrating automatic motivation (Webb et al., 2022). While participants showed automatic motivation, care partners ongoing support contributed to reflective motivation. This combined motivation is crucial for long-term program adherence (Webb et al., 2022; Yang et al., 2024). Furthermore, our study identified that the extended period before diagnosis (a prerequisite for program enrollment) and the associated uncertainty often led to mental frustration for both individuals with PD and their care partners, aligning with previous research (Krieger et al., 2024). Within the COM-B model, this may indicate a lack of opportunity. The diverse symptoms of PD can disrupt hobbies and alter lifestyles, leading to a sense of loss. This, in turn, often contributes to a decline in mood which may already be part of the disease process - negatively impacting quality of life for individuals with PD (Ahern et al., 2024; Islam et al., 2022).
The post-exercise themes in this study show that participants perceived several benefits from participating in a PD-specific community-based exercise program. Multicomponent programs incorporating aerobic, stretching, resistance, and cognitive exercises play an important role in improving quality of life, mobility, pain, and mood in individuals with PD (Ahern et al., 2024; Duchesne et al., 2015; Lamotte et al., 2015; Langeskov-Christensen et al., 2024). These programs also positively impact relationships between individuals with PD and their partners (Dekawaty et al., 2019; Glover et al., 2023), an important, yet underemphasized aspect of PD. Adherence to the exercise program was influenced by the nature of the PD-specific exercises, supportive instructor, and the group setting (Crizzle & Newhouse, 2012; Schootemeijer, van der Kolk, Ellis et al., 2020). Social interactions and community support provided by the PAA were crucial for enhancing mood and well-being (Cleary et al., 2020; Ferrusola-Pastrana et al., 2024; Spink et al., 2010). These factors provide both physical and social opportunities, supporting long term adherence, as indicated in the COM-B model. In our study, grouping individuals based on disease severity made them feel “less self-conscious” and more motivated to exercise with people at same level of functioning in line with the capability aspect of the COM-B model (Yang et al., 2024). This suggests that the perception of how people with PD engage in exercise may vary with disease severity (Flynn et al., 2022), highlighting the psychological aspect of capability. Assessing the severity of the condition before group assignment may be essential for participation and long-term adherence to the exercise program. Notably, in PAA, pre-assignment screenings ensured appropriate group placements, which participants found satisfactory, underscoring the significance of physical capability.
Our findings demonstrate that the COM-B model provides a valuable framework for understanding the factors that support long-term adherence to community-based exercise programs for individuals with PD. Tailoring exercise programs based on disease severity emerged as a critical factor for engagement. Participants who underwent physiotherapist-led assessments were placed in appropriate groups, which enhanced both their physical and psychological confidence in exercising. This personalized approach may improve long-term adherence by ensuring that exercises are appropriately challenging, yet manageable (Flynn et al., 2022; Williams et al., 2018; Yang et al., 2024).
Opportunities for participation were influenced by both physical and social factors. Access to exercise equipment, knowledgeable instructor, and structured programs encouraged consistent engagement (Crizzle & Newhouse, 2012; Flynn et al., 2022; Yang et al., 2024). Group-based activities fostered social connections, which participants found highly motivating. However, logistical barriers such as transportation challenges, program costs, and limited awareness of available community resources may restrict participation, highlighting areas for improvement (Ellis et al., 2013; Schootemeijer, van der Kolk, Ellis et al., 2020). Motivation played a central role, with participants demonstrating an inherent drive to stay active (automatic motivation). This was further reinforced by structured goal-setting, educational support, and encouragement from both care partners and exercise leaders (reflective motivation) (Crizzle & Newhouse, 2012; Yang et al., 2024). The combination of these motivational factors likely contributed to sustained participation and overall improvements in well-being (Cleary et al., 2020; Crizzle & Newhouse, 2012; Williams et al., 2018). By addressing these elements—ensuring appropriate exercise tailoring, improving accessibility, and fostering motivation—community-based exercise programs can better support individuals with PD, enhancing both physical function and quality of life. Also, our study showed that PD-specific community-based programs can positively impact the relationships of individuals with PD and their partners, which may play a role in improving their mental health.
A limitation of this study was a relatively small sample size, which may affect the generalizability of the results. However, we achieved thematic saturation, and our sample size is sufficient for a qualitative study of this nature. Another limitation is that only people who regularly attended the program were interviewed. Different perspectives may be captured by those who dropped out of the program or who were not interested in exercising. Factors such as lack of social support, worsening of PD-related symptoms, and lack of awareness of the role of exercise in PD have been previously documented as contributing to a lack of interest in exercise among individuals with PD (Schootemeijer, van der Kolk, Ellis et al., 2020).
Conclusion
This study explored perspectives on a PD-specific community-based exercise program for individuals with PD, identifying benefits and barriers using the COM-B model. Both automatic and reflective motivation are essential for sustained participation. Assessing baseline capability and placing individuals in appropriate groups support long-term adherence. Participants reported that group exercise fosters a sense of community, while tailored programming enhances engagement in a community-based exercise program. However, barriers such as transportation, cost, and limited awareness of the benefits of exercise remain challenges. Addressing these factors through targeted education and accessible programming may optimize participation and long-term health outcomes in PD. Future research should examine the perspectives of people with PD and their care partners who do not participate in PD-specific community-based exercise programs to identify barrier to participation.
Supplemental Material
sj-docx-1-nre-10.1177_10538135251348365 - Supplemental material for Community-Based Exercise Programming for Individuals with Parkinson's Disease: A Qualitative Study
Supplemental material, sj-docx-1-nre-10.1177_10538135251348365 for Community-Based Exercise Programming for Individuals with Parkinson's Disease: A Qualitative Study by Aiza Khan, C Allyson Jones, Marguerite Wieler and Victor E Ezeugwu in NeuroRehabilitation
Supplemental Material
sj-pdf-2-nre-10.1177_10538135251348365 - Supplemental material for Community-Based Exercise Programming for Individuals with Parkinson's Disease: A Qualitative Study
Supplemental material, sj-pdf-2-nre-10.1177_10538135251348365 for Community-Based Exercise Programming for Individuals with Parkinson's Disease: A Qualitative Study by Aiza Khan, C Allyson Jones, Marguerite Wieler and Victor E Ezeugwu in NeuroRehabilitation
Footnotes
Acknowledgements
We extend our gratitude to all the participants and the Parkinson Association of Alberta for all the support received throughout this study.
Ethical Considerations
The University of Alberta's Human Research Ethics Board approved this study (Ethics ID: Pro00122937).
Consent to Participate
All participants provided written informed consent before enrollment.
Consent for Publication
Informed consent for publication was received from the participants.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AK received MITACS Accelerate studentship (# IT37143). The funding body had no role in the study's design, collection, analysis, and interpretation of data, or in writing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.