
Abstract
Introduction
This study examined the effect of a single treatment of Active Release Techniques (ART®) on resting stiffness of the medial gastrocnemius (MG), resting tension of the triceps surae unit, plantar-flexion strength, and active ankle range of motion (ROM).
Methods
Twenty-four healthy participants (14 females, mean (SD) age: 24.8 (4.6) years) were randomised to 4 min of ART® applied to one leg. With the foot fixed in 5° plantar-flexion, shear wave velocity (SWV) was measured using ultrasound elastography and resting tension was measured using a dynamometer, acquired before, immediately, and 5 min post intervention. Active ankle ROM and plantar-flexion maximal voluntary isometric strength (MVIC) were measured before and after ART®. Repeated measures ANOVAs with factors of limb and time were used.
Results
MG SWV of the intervention limb decreased immediately following ART® (mean % change = −5.65% [95%CI: −2.05 to −9.26], p = 0.003) and at 5 min (mean % change = −5.50% [95%CI: −1.22 to −9.78], p = 0.017). There was no difference post ART® for resting tension of the triceps surae unit, plantar-flexion MVIC, or active ankle ROM for either the intervention or control limb.
Conclusion
Four minutes of ART® applied to the MG induces a significant reduction in resting MG SWV, which persisted for 5 min, but was not coupled with a change in resting tension of the triceps surae unit, plantar-flexion MVIC, or ROM.
Introduction
Active Release Techniques® (ART®) were developed by Dr P. Michael Leahy in the 1980's and uses palpation to locate and apply sustained compression over an area of soft tissue tension or adhesion while that tissue is actively shortened and lengthened using voluntary muscle contractions. 1 ART® is proposed to release adhesions within the targeted soft-tissue 2 to improve tissue mobility, reduce pain, and improve performance. While several studies have examined the effects of ART® applied to muscle tissue on joint range of motion (ROM), pain, and performance,1,3,4 no studies have examined whether such changes are accompanied by changes in muscle stiffness.
Several studies have examined the effect of ART® on lower limb ROM. For instance, ART® applied bilaterally to the hamstrings and dorsal sacral ligament of healthy active male participants improved the sit-and-reach test. 1 While this finding suggest that ART® may increase active ROM, the sit-and-reach test does not measure isolated changes of the hamstrings as movement during this test is influenced by elongation of several major muscle groups (e.g., erector spinae, hip rotators) and major lower limb nerves (e.g., sciatic). 5 In addition, a single session of ART® applied unilaterally to the hamstrings of participants with a 20° restriction in their straight leg raise also improved the popliteal knee angle. 6 While these findings may suggest a localised change in hamstring ROM and subsequent reduction in muscle stiffness, direct measures of local and global muscle stiffness were not included and are required to examine the effect of ART® more thoroughly.
Shear wave elastography offers a valid, reliable, and non-invasive approach to quantify localised muscle stiffness.7,8 Shear wave elastography utilises the assessment of shear-wave velocity (SWV) which is positively correlated to tissue stiffness, such that low SWV is associated with low tissue stiffness, and vice versa. 9 Using shear wave elastography one study has reported that seven minutes of passive massage (i.e., effleurage and petrissage) was sufficient to cause a significant, but short-term (< 3 min) reduction of 5.2% in local muscle stiffness of the medial gastrocnemius (MG). 10 While this study suggests that passive soft tissue techniques can reduce local muscle stiffness, extrapolating such findings to active soft tissue techniques, such as ART®, may be questionable given the addition of active cyclic stretching during the intervention, which in and of itself, can cause an immediate reduction in resting muscle stiffness. 11 Therefore, the combination of sustained mechanical pressure plus active cyclic stretching of a muscle may induce greater changes in muscle properties, compared to each technique in isolation.
The ability for soft tissue therapy to improve measures of performance and/or strength is equivocal with some studies showing an increase in muscle strength, while others show no effect, and even a decrease.12,13 Evidence from studies including active cyclic stretching, incorporated in the ART® intervention, have revealed significant immediate increases in maximal power in asymptomatic participants14,15; however, the mechanism(s) underlying acute changes in muscular strength following treatment remain unclear. To date, only one study has examined the immediate effects of ART® applied to the quadriceps on knee extensor torque and quadriceps muscle inhibition in participants with persistent anterior knee pain (n = 9), revealing no significant differences post intervention. 3 While this finding may suggest that ART® does not increase maximal strength in individuals with pain, no studies have examined the effect of ART® in healthy recreationally active individuals.
The primary aim of this study was to examine whether ART® induces an immediate and short-term (up to 5 min) change in SWV (i.e., stiffness) of the MG muscle and whether such effects are linked to changes in resting tension and strength of the triceps surae muscle-tendon unit. We hypothesised that ART® would induce an immediate but transient decrease in local MG muscle SWV measured using shear wave elastography that would be coupled to a reduction in triceps surae resting tension (at a fixed ankle angle). The secondary aim of this study was to investigate whether ART® maintains active maximum voluntary isometric contraction (MVIC) of the triceps surae complex and improves ankle dorsiflexion (DF) and plantar flexion (PF) active ROM.
Materials and methods
Participants
Participants were recruited from Southeast Queensland using social media, recruitment posters, and university emails. Participants were included if they were between 18 and 35 years of age and self-reported no pain or injury within their lower limbs or lower back in the last three months. Exclusion criteria included any self-reported previous major lower limb or lower back injury (e.g., fractures, dislocations, surgery), pregnancy, taking pain relieving medications, major allergies to skin adhesives, neurological or systemic medical conditions (e.g., stroke, cardiovascular disease, diabetes), or deep vein thrombosis. The institutional Human Research Ethics Committee (HREC) approved the study, all participants signed an informed consent form, which included consent to publish, prior to participating (Approval number REDACTED – appears in the title page).
Active release techniques® intervention
The details of the ART® intervention are reported according to the Template for Intervention Description and Replication (TIDieR). 16 An ART® certified instructor with over 25 years’ experience performed the intervention. Participants were positioned in prone with their feet hanging off the end of the plinth. During the intervention the practitioner applied contact to the MG muscle belly, within the scanned area assessed by elastography. During the ART® intervention the practitioner maintained contact with the MG muscle belly using a reinforced thumb with firm pressure, and the participant actively moved their ankle through full ROM (i.e., PF to DF), known as a ‘pass’. During the intervention, each participant rated their level of discomfort at the halfway point (i.e., 2 min) and at the end (i.e., 4 min) on an 11-point numerical rating scale, where 0 indicated “no pain” and 10 indicated “the worst pain imaginable”. The ART® intervention was not designed to be painful, thus where the participant rated their self-reported level of discomfort ≥4 out of 10 at the halfway point the ART® practitioner reduced their pressure. The practitioner moved the contact point to treat the area of MG scanned by the ultrasound transducer and the participant performed ∼4–5 ‘passes’ per minute. The intervention was randomised to the left or right leg and performed for four minutes, resulting in a total of 16–20 ‘passes’. The 4 min application was selected to balance the feasibility of the study as well as mirror a similar soft tissue contact time of the medial gastrocnemius in previous research. 10 Although short in duration and localised to a relatively small portion of the muscle the intervention reproduced for this research was an authentic ART® application.
Outcome measures
Shear wave velocity
A Siemens Healthineers ACUSON Sequoia ultrasound system (Siemens Healthineers, Issaquah, WA, USA), with a 10L4 linear array transducer (2.9–9.9 MHz bandwidth) was used to measure SWV (Software Revision VA40A) in metre per second (m/sec) of the MG muscle belly. SWV was selected based on current recommendations for data presentation. 17 All sonographic imaging was completed by an Accredited Medical Sonographer with 11 years’ experience in musculoskeletal imaging. Blinding of the sonographer was not possible due to the know effect of erythema due to increased skin blood flow and temperature at the intervention site following soft tissue therapy. 18 For all imaging, participants lay prone on an examination plinth with their knees extended and their feet overhanging the end of the plinth 10 (Figure 1). B-mode imaging was initially used to identify the mid portion of the muscle belly, approximately 3–4 cm medial to the division between the medial and lateral gastrocnemius. 10 To estimate stiffness aligned to the long axis of the muscle fibres, B-mode imaging was used to determine muscle fibre orientation ensuring several fascicles could be observed without interruption 19 and the region of interest for SWV measures was free from blood vessels and muscle fascia. 20 To facilitate consistency between SWV measures, the position of the ultrasound transducer was outlined onto the skin of both limbs using a permanent marker.
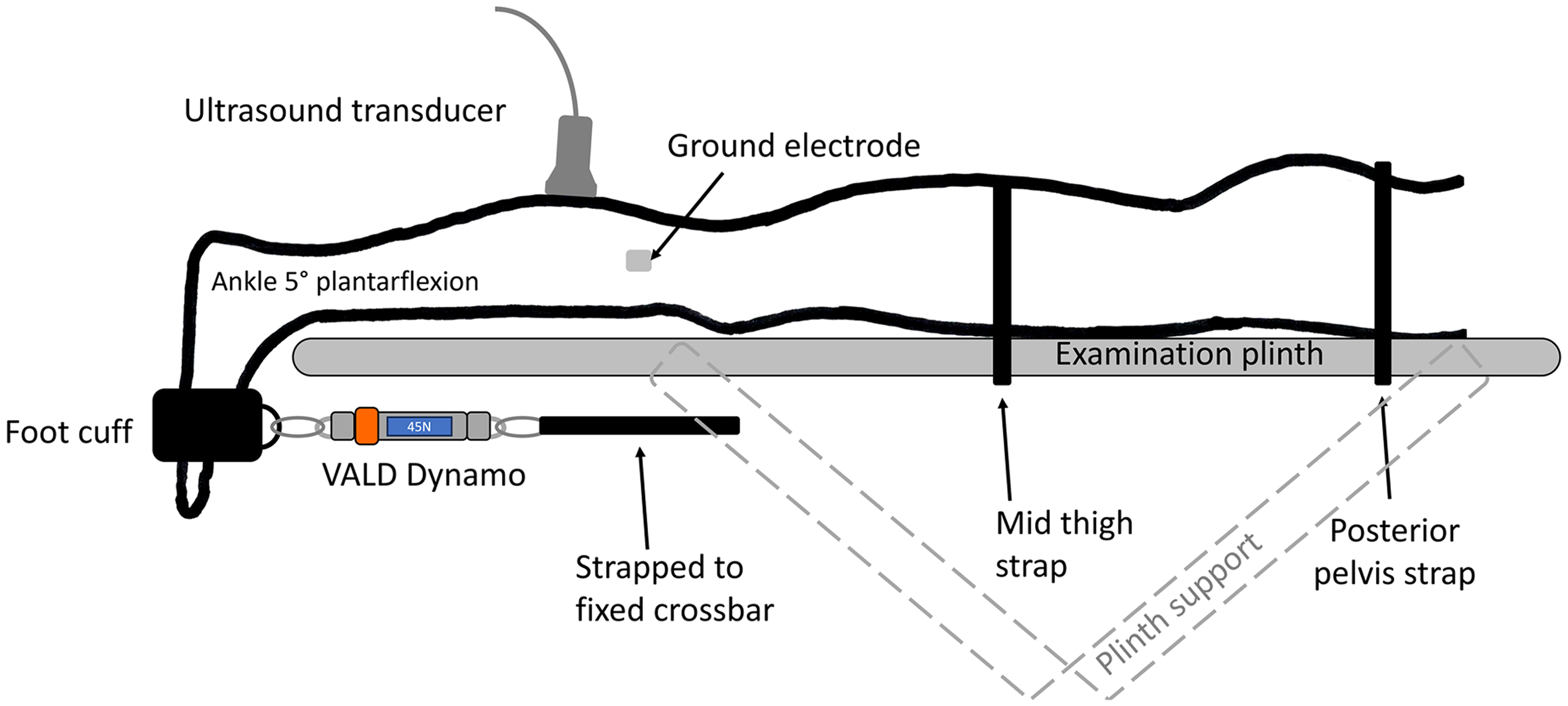
Experimental set up for the measurement of medial gastrocnemius shear wave velocity and triceps surae resting tension, as well as the plantar-flexion maximum voluntary isometric contraction with the ankle positioned in 5° of plantar flexion. Passive tension and plantar-flexion maximum voluntary isometric contraction was measured using a VALD Dynamo connected to a steel crossbar via a non-elastic strap and to the foot via a foot and ankle cuff placed over the distal end of the participant's foot.
The ultrasound settings for the SWE measures were set to detect a velocity range of 0.5 m/sec to 13 m/sec with transparency set at 70%. A 2D shear wave elastography colour box (15 × 15 mm, 225 mm2) was placed over the middle of the MG muscle belly and a single circular region of interest (ROI) (10 mm diameter, 78.5 mm2) was placed within the colour box to measure the mean SWV. SWV measures were acquired from both limbs (intervention and control) before (i.e., baseline), immediately after (i.e., immediate timepoint), and 5 min after (i.e., 5 min timepoint) the ART® intervention (Figure 2). 10 Five SWV measures were recorded from the same muscle location at each timepoint with the average of all five measures used in the analysis. 21 Measures of muscle SWV were acquired from both limbs in a randomised order, except immediately after the ART® intervention where the intervention limb was always measured before the control limb to account for the highly transient nature of the massage effect. 10

Protocol of the data collection with three time points for measurements of shear elastic modulus (baseline, immediate, 5 min). ROM – range of motion, MVIC – maximum voluntary isometric contraction, SWE – shear elastic modulus, PT – passive tension of the triceps surae muscle-tendon unit, ART® - Active Release Techniques.
To control for ankle angle and thus muscle-tendon length during measurements of SWV, the participant's ankle was fixed at 5° PF (confirmed using a universal goniometer, 0° = foot perpendicular to shank) using the VALD Dynamo dynamometer and ankle attachment (VALD Performance, Brisbane, Australia) (Figure 1). This ankle position was consistent with previous work 10 and was above the slack angle of 25° PF enabling sufficient tension within the MG to enable detection of a change in stiffness. 22 Surface electromyography (EMG) sensors (Bagnoli EMG System, Delsys, Natick, MA, USA) were placed over the MG of both the intervention and control limb. EMG activity was visually inspected during each SWV measurements to confirm the MG remained relaxed. Where EMG activity visually increased above resting baseline values during measurement of the SWV the trial was excluded and repeated, which occurred 12 out of 720 (1.7%) trials.
Resting tension of the triceps surae muscle-tendon unit
A VALD Dynamo dynamometer and ankle attachment was used to measure resting tension of the triceps surae muscle-tendon unit at a fixed ankle angle of 5° PF that was confirmed prior to each measurement using a universal goniometer (Prestige Medical, Northridge CA, USA) (Figure 1). Five measures of resting tension were recorded in Newtons at the same time as measures of SWV occurred (Figure 2). The average of all five measures were used in the analysis.
Active range of motion
Maximal active DF and PF ROM was measured before (i.e., baseline) and after the ART® intervention (i.e., follow-up) using a universal goniometer with the participant positioned prone and their knee flexed to 90° (Figure 2). The average of three measurements taken at the maximal AROM were used for analysis.
Plantar flexion maximum voluntary isometric contraction
Participants lay prone with their feet overhanging the examination table and the VALD Dynamo was set up in the same way as the SWV measures (Figure 1), with PF MVIC recorded before (i.e., baseline) and after the ART® intervention (i.e., follow-up) (Figure 2). A mark was placed on the participants skin at the level of the foot and ankle cuff to ensure consistency of cuff placement between measurements. To minimize participant movement during testing non-elastic straps were placed across the mid-thigh and posterior pelvis at the level of the posterior superior iliac spine (Figure 1). Participants performed a standardized warm-up consisting of one PF muscle contraction at 50% and 75% of their self-estimated maximum, followed by one practice attempt at 100% (i.e., MVIC). All warm-up/practice attempts were held for 3–5 s, with 30 s rest between each trial and 60 s rest at the end. Following the warm-up/practice, participants performed three MVICs with 60 s between each trial. Participants were provided with strong verbal encouragement during maximum contractions. 23 The average of all three MVIC trials were used for analysis. To minimize any effect of the MVICs on SWV, the participant remained in a relaxed prone position for 10 min prior to the baseline SWV measurements being recorded (Figure 2). To minimise protocol bias we alternated which limb was measured first (i.e., intervention or control) for the ROM and MVIC throughout the data collection.
Statistical analysis
Statistical Package for the Social Sciences (SPSS) Version 26.0 (IBM Corp, Armonk, NY, USA). was used for data analysis. Prior to statistical analysis, SWV data were inspected for outliers using the cut-off of two standard deviations above or below the mean. This resulted in two participants being removed from all analyses. Intraclass correlation coefficients (ICC), standard error of the measurement (SEM), and minimal detectable change at 90% confidence (MDC90) were calculated to determine the intra-session reliability of all outcomes across baseline measures. 24 A two-way mixed effects model based on absolute agreement was used for ICC calculations. ICC values were considered ‘poor” when <0.61, “good’ between 0.61 to 0.80, and excellent between 0.81 to 1.00. 25 The SEM was calculated using the following formula (SEM = SDbaseline×√1-ICC). The MDC90 was calculated using the following formula (MDC90 = 1.64×SEM×√2). 24
Data distributions consistently passed the Kolmogorov-Smirnov normality test and thus all data were reported as mean (SD) and mean difference (MD) and 95% confidence interval (95%CI). Two separate, two-way repeated measures analysis of variance (ANOVA) were used for the outcomes of SWV and resting tension using within-subject factors of limb (intervention, control) and time (baseline, immediate, 5 min). PF MVIC and PF and DF active ROM were analysed using separate one-way repeated measures ANOVAs using a within-subject factor of limb (intervention, control). Post-hoc analyses were performed using the least significant difference (LSD) test. ANOVA outputs including interaction and main effects are reported using the F-statistic, p-value, and partial eta squared (ηp2). Cohen's d effect sizes were calculated using ηp2 values from post-hoc tests and interpreted as small = 0.20, moderate = 0.50, and large = 0.80 effect sizes. 26 Statistical significance was set at an alpha <0.05.
Results
Participants
Twenty-six participants were recruited into the study and twenty-four participants were included in the data analysis (demographics for the 24 included participants: 20 right leg dominant, 14 females, mean (SD) age 24.8 (4.6) years; BMI 23.6 (3.3) kgm2). The intervention limb was randomised to the right limb in 13 participants. There were no adverse events or modifications to the planned intervention.
Intra-session reliability
Intra-session reliability of the included outcomes was considered excellent with ICC scores ranging between 0.85 and 0.99 for all outcome measures (Table 1).
Intra-session reliability of primary and secondary outcome measures using baseline data.
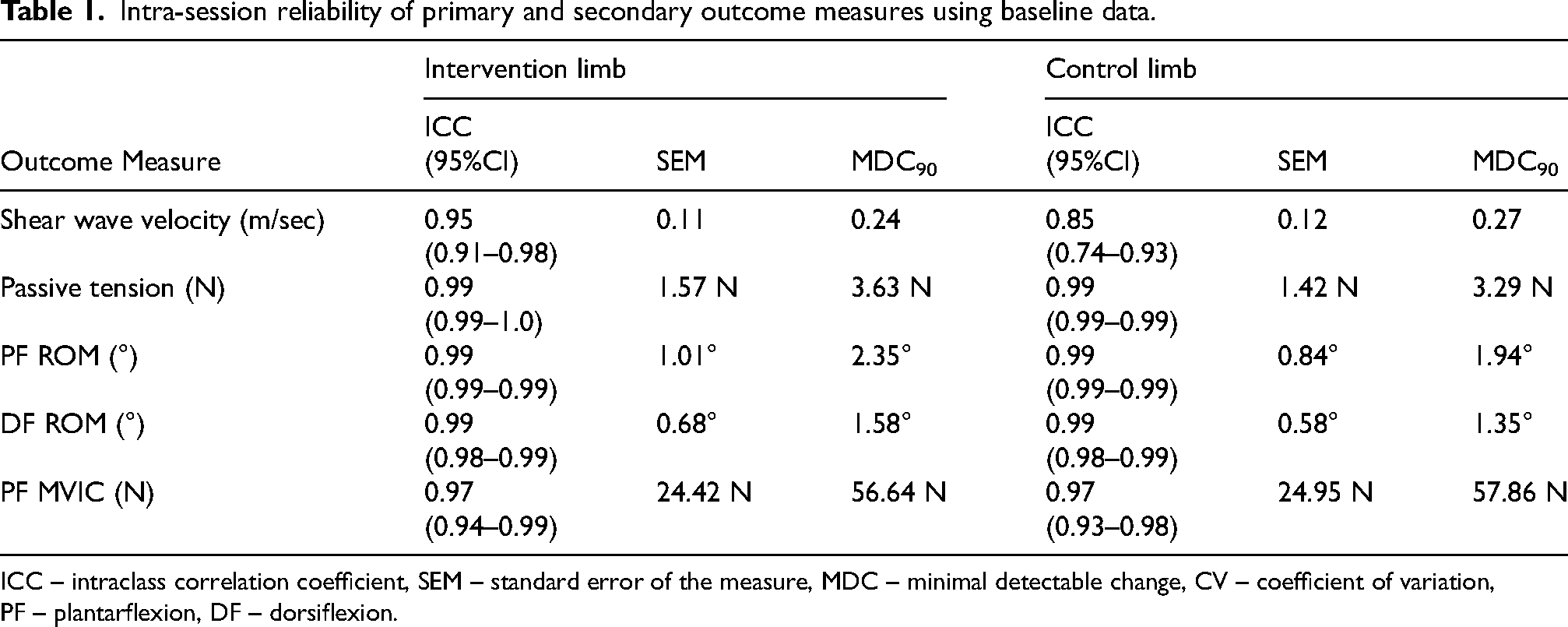
ICC – intraclass correlation coefficient, SEM – standard error of the measure, MDC – minimal detectable change, CV – coefficient of variation, PF – plantarflexion, DF – dorsiflexion.
Medial gastrocnemius resting shear wave velocity
Mean (SD) SWV values are presented in Table 2. A significant limb-by-time interaction was found for MG SWV (F1,23 = 3.745, p = 0.031, ηp2 = 0.140). There was no significant difference in MG SWV between limbs at baseline (p = 0.06). Post-hoc analysis revealed that MG SWV of the intervention limb was significantly lower both immediately following (MD −0.25 m/sec [95%CI −0.41 to −0.09], p = 0.004) and 5 min post ART® (MD −0.25 m/sec [95%CI −0.45 to −0.05], p = 0.016), compared to baseline. Compared with baseline SWV reduced by an average of −5.71% (95%CI: −2.10 to −9.31) immediately following and −5.70% (95%CI: −1.42 to −9.98) at 5 min follow up and was considered a ‘moderate’ effect size (ηp2 = 0.304, Cohen's d = 0.64) (Figure 3). No significant differences were identified for the control limb between any timepoints (p > 0.05). Figure 4 presents the individual variation for the SWV across all three timepoints for both limbs.
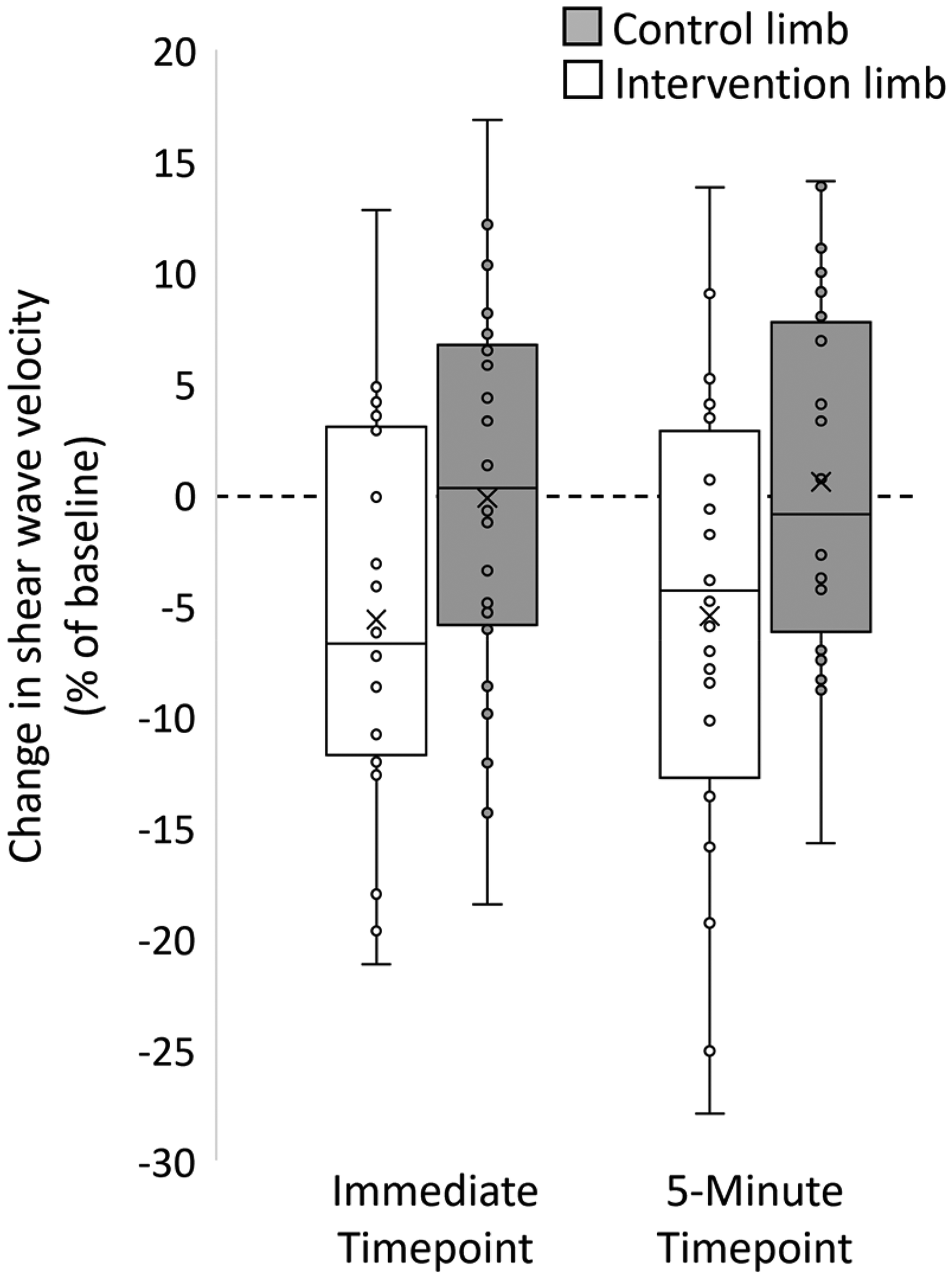
Box and whisker plot presenting the change in shear wave velocity expressed as a percentage of their baseline values. Circles represent individual data points. Error bars denote the minimum and maximum values, the box denotes the 25th and 75th percentiles, with the midline representing the median and the x representing the mean.
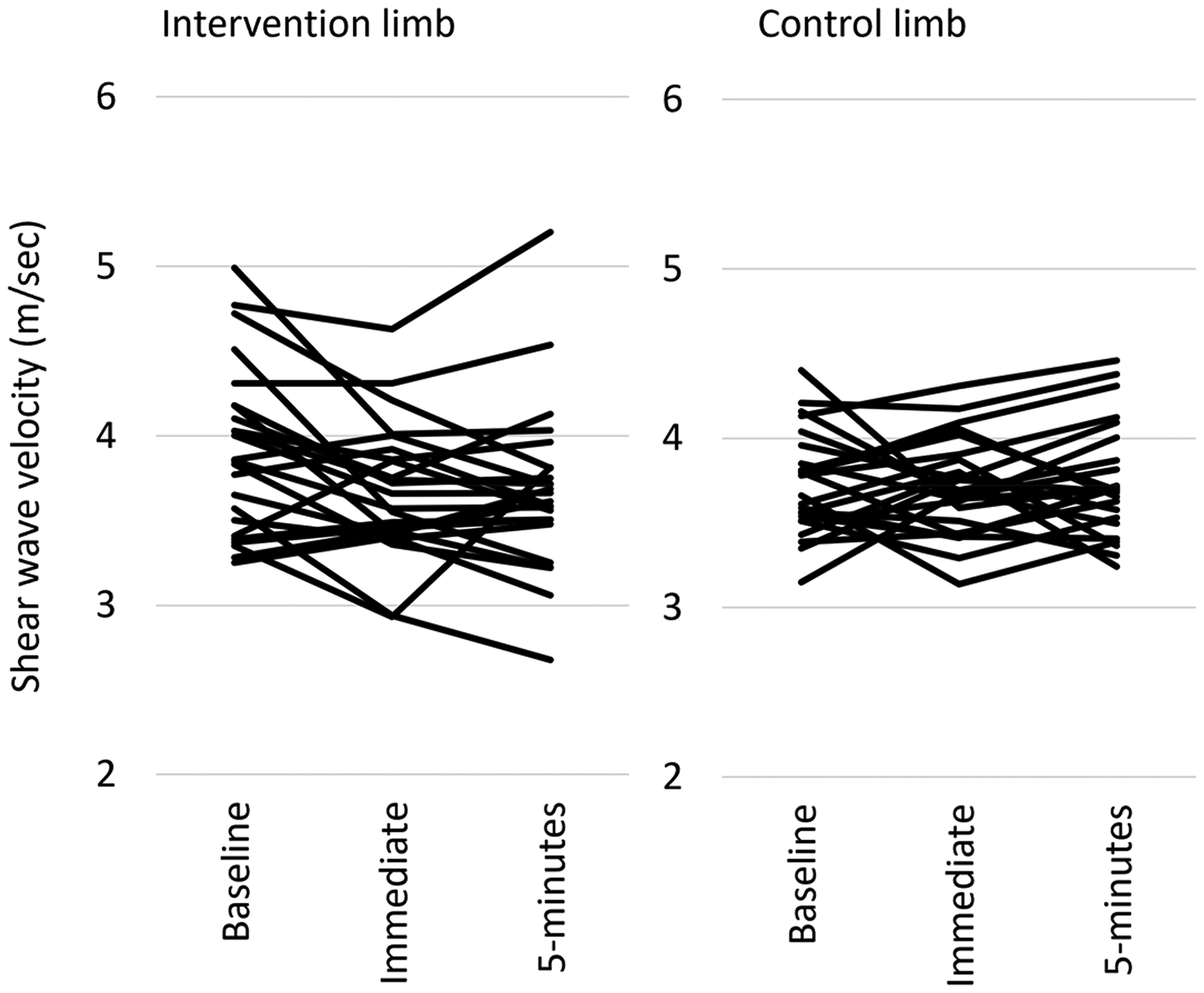
Individual data of shear elastic modulus measured at baseline, immediate timepoint, and 5 min timepoint in the intervention limb and control limb.
Mean (SD) values for primary and secondary outcome measures at baseline, immediate timepoint, and 5 min timepoint.
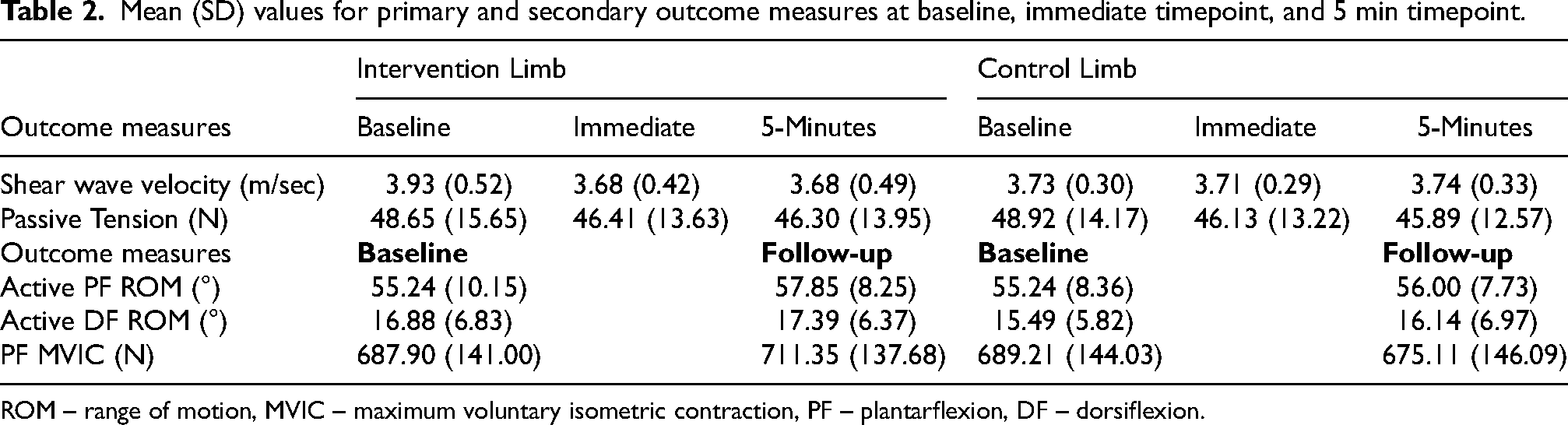
ROM – range of motion, MVIC – maximum voluntary isometric contraction, PF – plantarflexion, DF – dorsiflexion.
Triceps surae muscle-tendon unit resting tension
Mean (SD) values of resting tension of triceps surae muscle-tendon unit are presented in Table 2. There was no significant limb-by-time interaction (F1,23 = 0.158, p = 0.855, ηp2 = 0.007) or main effect of limb (F1,23 = 0.023, p = 0.880, ηp2 = 0.001). There was a main effect of time (F1,23 = 6.547, p = 0.003, ηp2 = 0.222). Post-hoc tests revealed that compared to baseline resting tension of the triceps surae muscle-tendon unit was significantly lower immediately following ART® (MD −2.51 N [95%CI −4.54 to −0.49], p = 0.17) and 5 min post (MD 2.69 N [95%CI 0.50 to 4.87], p = 0.004) when both limbs were collapsed. No other statistically significant differences were observed.
Maximum voluntary isometric contraction
Mean (SD) PF MVIC values are presented in Table 2. There were no main effects of limb (F1,23 = 1.072, p = 0.311, ηp2 = 0.045) or time (F1,23 = 0.282, p = 0.600, ηp2 = 0.012). However, a significant limb-by-time interaction was found on the PF MVIC (F1,23 = 6.056, p = 0.022, ηp2 = 0.208). Post-hoc analysis revealed that PF MVIC following ART® intervention was not different in the intervention limb compared to baseline (MD 23.44 N [95%CI −4.01 to 50.89], p = 0.09); however, the intervention limb had a greater PF MVIC than the control limb following ART® intervention (MD 36.24 N [95%CI 0.16 to 72.31], p = 0.049).
Ankle active range of motion
Mean (SD) active PF and DF ROM are presented in Table 2. For active DF ROM there was no significant limb-by-time interaction (F1,23 = 0.019, p = 0.892), main effect of limb (F1,23 = 1.242, p = 0.277), or main effect of time (F1,23 = 1.796, p = 0.193). For active PF ROM, there was no significant limb-by-time interaction (F1,23 = 3.835, p = 0.062) or main effect of limb (F1,23 = 1.920, p = 0.179). There was a significant main effect of time (F1,23 = 5.596, p = 0.027).
Pain ratings
The mean (SD) level of discomfort experienced at the end of ART® was 2.96 (1.92) out of 10. There was no correlation between the self-rated level of discomfort at the end of the intervention and the change in SWV of the intervention limb immediately following ART® (r = 0.061, p = 0.776).
Discussion
This study examined the immediate effect of a single ART® intervention on measures of resting muscle stiffness, resting tension, muscle strength, and joint range of motion. Our results showed that 4 min of ART® applied to the MG induced a statistically significant reduction in resting muscle SWV in the intervention limb, which remained present for at least 5 min. This observed reduction in muscle stiffness may particularly benefit individuals with neuromuscular disorders, movement restrictions, or post-injury where concomitant changes in perceived or actual muscle stiffness could be transiently improved with ART® intervention. However, the reduction in local muscle stiffness assessed using SWV was not accompanied by an equivalent change in resting tension of the triceps surae muscle-tendon unit or active DF or PF ROM, suggesting the treatment effects were isolated to the muscle belly and insufficient to change the mechanics of the muscle-tendon unit. Although there was a small difference in PF MVIC between limbs after ART, there was no difference in MVIC of the intervention limb immediately after treatment. Overall, our results suggest that the effects of 4 min of ART® applied to a small portion of the MG muscle may be specific to the muscle belly, with no concomitant change in resting tension of the triceps surae muscle-tendon unit measure within our study.
Our study revealed a moderate effect (Cohen's d = 0.67) with a 5.65% reduction in muscle stiffness of the MG muscle belly immediately following the ART® intervention, which was sustained for at least five minutes. Importantly, this reduction in MG muscle stiffness was greater than the SEM and MDC90, suggesting a true change. Our finding appears consistent with a similar study 10 that reported an equivalent reduction in MG muscle stiffness (MD = 5.2%; Cohen's d = 0.66) following 7 min of therapeutic massage. Interestingly, the effect of massage on muscle stiffness had returned to baseline at the 3 min follow up, 10 whereas muscle stiffness remained significantly reduced at 5 min following ART®. Although speculative, there are several possible explanations for differences between previous massage work 10 and our ART® intervention which may influence the observed prolonged effect of ART®. First, massage and ART® are fundamentally different techniques thus the application time and amount of compression applied to the target muscle may have differed. For instance, despite a similar total intervention time dedicated to the MG muscle belly, the massage study included a 7 min intervention with three different techniques (effleurage – applied to the entire calf, and wringing and deep circular frictions – applied to the MG). 10 In contrast, our ART® intervention utilised deep digital pressure focused entirely on the area where SWV was measured. Given that muscle stiffness may be reduced by manual contact of the muscle tissue breaking the resting linkages between actin and myosin filaments 10 or by an increased muscle temperature, 27 it is possible that deeper or more focused manual contact of the muscle tissue may result in a prolonged decrease in muscle stiffness seen in our study. Second, ART® includes a combination of active cyclic stretching of the muscle-tendon unit through full ROM with short-duration therapist applied overpressure at the end of range. 1 This differed to the massage technique applied in the study by Eriksson Crommert et al., 10 where the foot remained in a relaxed PF position. The addition of cyclic stretching with short-duration overpressure (i.e., static stretch) may prolong the effect of ART® to that of massage, with evidence using real time elastography showing that 2 min of that cyclic or static stretching significantly reduced MG muscle stiffness with a moderate effect size (0.75) compared to a control condition. 11 In addition, 5 min of static stretching resulted in a significant reduction in MG muscle stiffness that lasted for 15 min post intervention. 28 Although difficult to compare between massage and ART®, and ART® and stretching interventions due to difference in methods (e.g., techniques, contact time, and stretching protocols – static vs cyclic), our findings suggest that ART® may result in an equivalent but longer lasting reduction in muscle stiffness compared to massage, which may be predominately driven by the cyclic and static stretching components of the technique.
Resting tension of the triceps surae muscle-tendon unit significantly decreased in both limbs immediately and 5 min post intervention, likely due to viscoelastic changes (e.g., load-relaxation) in muscle and tendon force-length due to the ankle being held in 5° PF for the duration of the testing. Importantly, resting tension of the triceps surae muscle-tendon unit did not differ in the intervention limb pre-post ART®, suggesting our observed reduction in MG muscle stiffness was insufficient to induce a measurable change the muscle-tendon unit resting tension. The lack of significant changes in resting tension and active ankle ROM was unexpected, therefore, we propose several possible explanations for this observation. First, the treatment area was localised to a relatively small portion of the MG muscle belly. Given that the MG makes up approximately 26% of the total physiological cross-sectional area of the triceps surae muscle complex, 29 it may be reasonable to expect that changes in muscle stiffness isolated to MG may not be of sufficient magnitude to change the resting mechanical properties of the triceps surae muscle-tendon unit and subsequent active DF ROM. Previous work revealing an increase in hamstring muscle length using the 90–90 test in participants with hamstring ‘tightness’ following ART®, applied treatment along the entire length of the hamstring muscles including the origins and insertions, as well as other surrounding muscles (e.g., adductors and gluteal muscles). 6 An extended treatment time and greater treated area may be required to reveal changes in resting tension and/or ROM. Second, we chose to measure resting tension of the triceps surae muscle tendon unit with the ankle position fixed at 5° PF, and so the total passive forces applied to the triceps surae muscle-tendon may have been too small to detect changes following treatment. This is in line with previous work revealing that differences in ankle joint passive torque were not observed on the passive length tension curve until 10–25° DF following 5 min of static stretching. 30 In addition, measuring active ankle DF with the knee flexed to 90° may have limited our ability to observe changes in active DF ROM linked to change in gastrocnemius muscle stiffness, as this position preferentially loads the soleus muscle-tendon component of the triceps surae. 31 Future studies examining the effect of treatment on static measurements of ankle stiffness should include measurements obtained at several ankle positions (low and high passive forces) and with the knee flexed and extended. Finally, the use of a handheld-dynamometry and goniometry may not have been sensitive enough to identify small changes in resting tension or active DF and PF ROM. Although all outcome measures were reliable (i.e., ICCs >0.85) and SEMs were consistent with previous work, 32 there was variability between participants and within the measurements.
Following 4 min of ART® PF MVIC was not significantly different compared to baseline for either the intervention or control limb, suggesting that ART® does not alter PF MVIC. There was, a small but statistically significant difference between the intervention and control limbs post ART® intervention, which was bigger than the SEM but smaller than the MDC90 suggesting the finding be viewed with caution and may be a possible placebo effect or measurement error. Our lack of observed differences pre-post ART® in the intervention limb is consistent with previous work which revealed no immediate changes in quadriceps MVIC or muscle inhibition (measured using the interpolated twitch method) following an ART® intervention applied to the four quadriceps muscles and the patellar tendon in participants with anterior knee pain. 3 In addition, several systematic reviews have highlighted variability within the literature showing that maximal strength output may increase, decrease, or not change following soft tissue therapy,12,13,33 with one meta-analysis revealing that sports massage does not improve maximal strength output. 34 Given that our study assessed only healthy participants, future research is required to investigate whether ART® may increase maximal strength output in those with and without musculoskeletal conditions.
There are several methodological considerations when interpreting the results of this study. First, given the ART® intervention caused some minor skin redness following treatment we could not blind the sonographer to the intervention limb; however, adherence to our strict protocol during measurements should have minimised potential bias. Second, our treatment time was relatively short (i.e., 4 min) and concentrated to a small area of the MG muscle compared to clinical application, thus future research with a longer treatment duration and greater treatment area is warranted to more broadly examine the effect of ART®. Clinical application of ART® often involves a longer duration, wider treatment area, and multiple treatment sessions, which may explain our lack of observed results in range of motion and resting passive tension of the triceps surae muscle-tendon unit in this single-application study. Third, our follow up period of 5 min limits conclusions about the sustained effect of ART® and future research should examine the length of the effect of ART® intervention. Fourth, the use of a universal goniometer and a hand-held dynamometer to measure ROM and MVIC, respectively, may not have been sensitive enough to detect minor changes in range of motion and resting tension of triceps surae muscle-tendon unit in our experimental setup. Future studies may look to use more advanced methods of measuring resting tension and ROM (e.g., isokinetic dynamometer). Fifth, we did not measure the physical activity level of each participant and thus between subject differences may result from differences in physical activity levels. Lastly, our study included participants without musculoskeletal conditions; thus, limiting generalisability to other injured populations (e.g., muscle strain, Achilles tendinopathy). Examination of the effects of ART® on muscle stiffness in those with pain and pathology is warranted.
Conclusion
Findings from our study show that 4 min of ART® induced a moderate reduction in SWV of MG which lasted for at least 5 min and was larger than the SEM and the MDC90, suggesting a true effect. The reduction in muscle stiffness following ART® was consistent with previous work examining 7 min of massage therapy 10 ; however, the effects of ART® remained at 5 min post intervention, which was not observed post massage. This observation may suggest that ART® results in a longer treatment effect than massage; however, future studies utilising longer follow up periods are required to confirm this. The reduction in MG muscle stiffness was insufficient to cause a reduction in resting tension of the triceps surae muscle-tendon unit or to increase DF or PF ROM. This was unexpected but may be due to our short duration and targeted intervention to a small portion of the MG muscle. In addition, PF MVIC was not significantly increased following ART® intervention which is consistent with previous work examining the effect of ART® on quadriceps muscle strength. 3 Lastly, our findings cannot be generalised to individuals with musculoskeletal injury and is limited to the short duration of intervention used in this study. Further research should examine the temporal effect of ART® intervention with longer and repeated dosages, longer follow-ups, and in clinical populations.
Footnotes
Acknowledgements
The authors would like to acknowledge Siemens Healthineers for the provision of the elastography licenses that were used in this study. The authors would also like to acknowledge Citiscan Radiology, Brisbane, Australia, for the loan of the ACUSON Sequoia ultrasound system and office space.
Ethical considerations
Central Queensland University Human Research Ethics Committee (HREC) approved the study, and all participants signed an informed consent form prior to participating (Approval number 0000022940).
Consent to participate
All participants signed an informed consent form prior to participating.
Consent for publication
All participants signed an informed consent form, which included consent to publish, prior to participating
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was independently funded by Active Release Techniques LLC and ART Corporate Solutions Inc. (ART®).
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Active Release Techniques LLC and ART Corporate Solutions Inc. (ART®) had no input into the study design, data collection methods, data analyses, interpretation, or write up of the manuscript. The clinician that applied the ART® technique within the study is a subcontracted instructor for ART® and had no input into the study design, data collection methods, data analyses, interpretation, or write up of the manuscript, and is not a listed author. JP is a subcontracted instructor for ART® conducting courses within North America. JP was involved in initial discussions surrounding study design and project funding. JP was not involved in the data collection or data analysis but did contribute to the final manuscript editing.
Data availability statement
Data generated during the current study are available upon request, subject to the terms of a licensing agreement. For access to proprietary data or further inquiries, please contact the corresponding author.