
Abstract
Background
Severe and persistent mental illnesses often lead to long-term psychosocial disability, affecting work participation, recreation, relationships, and community integration. Vocational rehabilitation is recognized as a key pathway to recovery.
Objective
This study explored the perspectives of mental health service providers and service receivers on facilitators of and barriers to vocational rehabilitation for people with mental illness in coastal Karnataka, India, through thematic analysis.
Methods
A descriptive qualitative design was employed, and data were collected through in-depth interviews with people with mental illness, their caregivers, and employers. A focus group discussion with rehabilitation professionals was also conducted. The transcribed verbatims were thematically analyzed by trained qualitative researchers.
Results
Twenty-one participants provided insights into vocational rehabilitation experiences. Various themes emerged as facilitators and barriers. The findings highlight the role of supportive networks; clinical stability, such as compliance with medication, workplace accommodations, individual motivation, and acquired skills enabling vocational rehabilitation; and clinical vulnerabilities, such as cognitive deficits, stigma, systemic gaps, and high expectations, which remain significant barriers.
Conclusion
Strengthening community-based and culturally tailored vocational rehabilitation models, enhancing employer sensitization, and expanding government support systems are critical to improving employment outcomes for people with mental illness in India.
Keywords
Introduction
The unemployment rate of people with mental illness (PWMI) is almost 90% (Erim et al., 2019; Franke et al., 2024) reflecting high prevalence of occupational dysfunction, “a negative experience related to engaging in daily activities (Teraoka & Kyougoku, 2015). Despite the high unemployment rates, evidence suggests that many of these individuals desire to work (Khare et al., 2021; Phutane et al., 2012; Waghmare et al., 2016). Being employed shows positive associations with clinical and psychosocial outcomes such as alleviating psychiatric symptoms, increasing levels of disability, promoting community integration, promoting mental well-being, improving quality of life, and facilitating recovery (Durgoji et al., 2019; Jagannathan et al., 2020; Vukadin et al., 2021). However, challenges in employment or lower rates of employment among these people are attributed to numerous barriers, such as poor mental health conditions, social skills deficits, a lack of choice and opportunity, stigma, disincentives to employ in the system, and a lack of workplace support (Corbière et al., 2011; Erim et al., 2019; Hanisch et al., 2017; Lockett et al., 2018; Netto et al., 2016; Rangarajan et al., 2020).
There are many factors facilitating the employment of PWMIs, such as clinical factors, medication adherence, support from others, the presence of work skills, past work experience, modified work strategies, workplace accommodations and the availability of employment opportunities (Filia et al., 2021; Meera et al., 2024; Morwane et al., 2021; Noteboom et al., 2024; Subramaniam et al., 2022). However, overcoming challenges and using facilitating factors are important for the implementation of vocational interventions.
In general, there is a need for service integration and the involvement of stakeholders such as service users, caregivers, employers and the government in vocational rehabilitation programs (Modini et al., 2016). Despite this, service providers have varied views on the employment of PWMIs; clinicians are unaware of employment services in the community, have negative views on functional recovery or help their patients work as a core part of their roles (Costa et al., 2020; Pogoda et al., 2011). However, service consumers view employment as status and acceptance within society, structured use of time, a sense of purpose, opportunities for social contact and personal development (Axiotidou & Papakonstantinou, 2021; Lannigan, 2014; Torres Stone et al., 2018). The literature has concluded that engaging various stakeholders could help in the early identification of rehabilitation needs and early initiation of rehabilitation services and create equitable work opportunities (Chimara et al., 2025).
With respect to the Indian context, there are few studies on vocational rehabilitation, as there are challenges in applying various vocational rehabilitation models due to inadequate resources and different sociocultural contexts (Sivakumar and Thirthalli, 2023; Thekkumkara et al., 2024). The available studies are restricted to participants from urban areas and are attached to tertiary care centers. This qualitative study aimed to understand service providers’ and service receivers’ views on factors associated with facilitators and barriers to vocational rehabilitation.
Methodology
Study Design
This study adopted Braun and Clarke's thematic analysis (Braun & Clarke, 2006) to identify facilitators of and barriers to vocational rehabilitation for PWMI through in-depth interviews and focus group discussions.
Participants
All participants were above 18 years of age and met specific eligibility criteria based on their respective roles. The researchers conducted in-depth interviews with 13 participants, including five PWMIs, three caregivers, and five employers. Furthermore, the researchers carried out a focus group discussion with eight rehabilitation experts during the period between May 2023 and March 2024 from the study setting. The demographic details of the participants are presented in Table 1. The participants were selected based on the eligibility criteria. For PWMIs, the inclusion criterion was that they had received vocational training for at least three months and were willing to participate in the study. Participants who were unable to express their viewpoints or experiences were excluded. Caregivers were eligible if they had a minimum of two years of caregiving experience. Employers were included if they had experience providing opportunities for patients to participate in vocational training within their respective agencies. Heterogeneous focus group discussions were conducted among the rehabilitation experts, who were selected based on a minimum of two years of experience in delivering vocational rehabilitation services. The details of the participants in the focus group discussion are presented in Table 1.
Socio-Demographic Profile of the Participants.
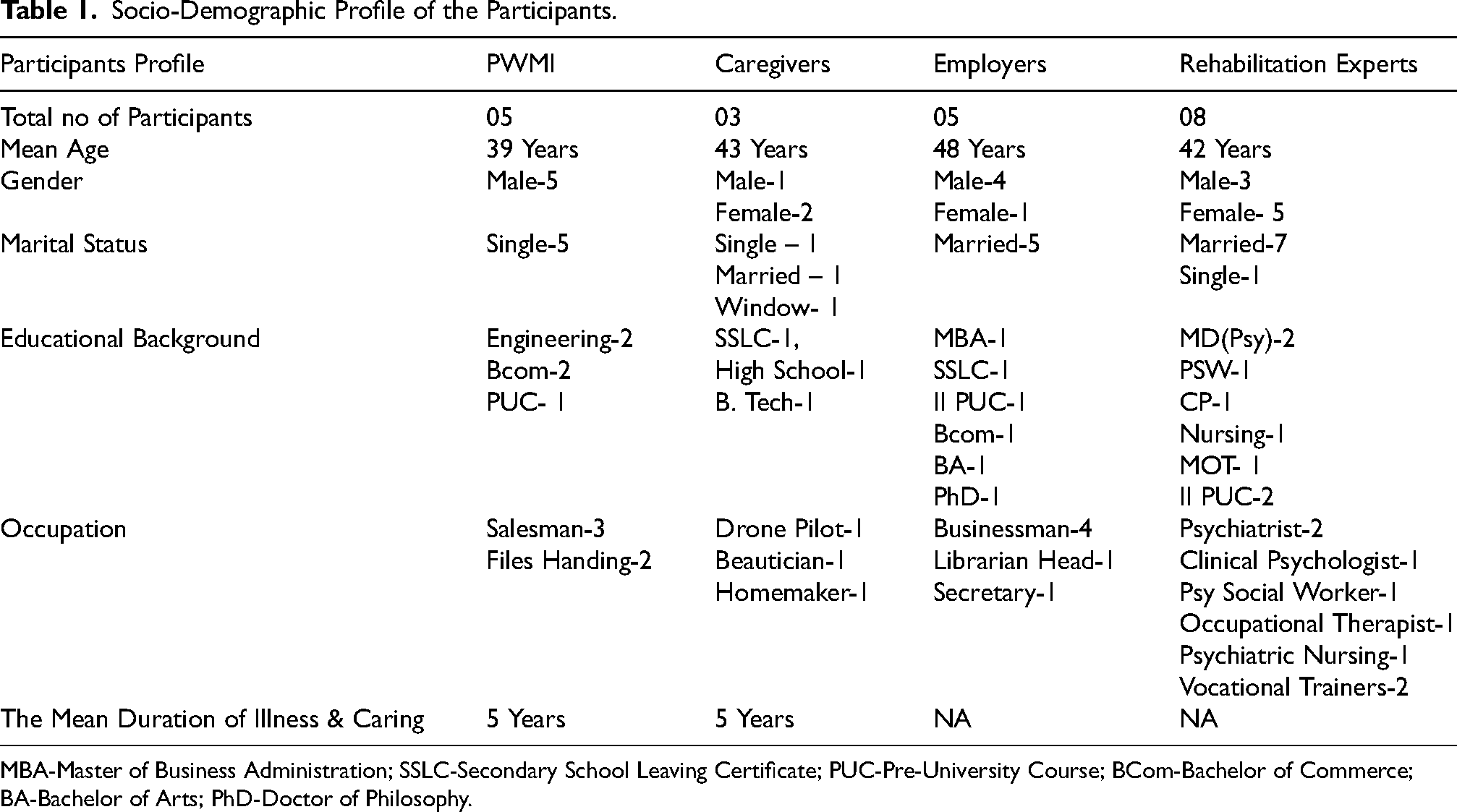
MBA-Master of Business Administration; SSLC-Secondary School Leaving Certificate; PUC-Pre-University Course; BCom-Bachelor of Commerce; BA-Bachelor of Arts; PhD-Doctor of Philosophy.
A priori sample size calculation was not adopted, as the study design was emergent. The sample size for the in-depth interviews with PWMIs, caregivers, and employers was determined by data saturation (Renjith et al., 2021), whereby further recruitment was stopped once no new themes or insights emerged. The sample size for the heterogeneous focus group was a priori fixed at eight participants.
Setting
The study setting was a residential rehabilitation center in coastal Karnataka, India, which caters to PWMIs. In-depth interviews were conducted in the participants’ preferred languages, i.e., Tulu (local language), Kannada (state language), or English.
Data Collection
A semistructured interview guide [Supplementary Table 1] was prepared by the authors and refined on the basis of feedback from subject experts and pilot interviews with three PWMIs. This was used to conduct face-to-face interviews for thematic analysis. The in-depth interviews with the PWMI, caregivers and employee facilitators were conducted by two experienced researchers, PA and RY, who were both fluent in the local language. The PA is a faculty member in psychiatric social work who is trained in qualitative research, whereas the RY is a psychiatric nursing faculty member and qualitative research expert who serves as a master trainer for qualitative research studies. The interviews were held in private spaces, ensuring a comfortable and distraction-free environment. Focus group discussions were conducted in English and moderated by SM, a psychiatric social worker trained in conducting focus group discussions. Responses were recorded verbatim via a Sony-IC recorder (Sony, Tokyo, Japan), a portable digital recording and playing device. Each interview lasted approximately one hour, providing in-depth exploration and rich qualitative data.
The Rigour of the Study
The study adopted Lincoln and Guba's trustworthiness (Lincoln et al., 1985) criteria to establish this study's rigour. Credibility, dependability, transferability, and confirmability were the key factors of these criteria. We conducted peer scrutiny of the patient data and sought participant feedback on the findings to enhance credibility. The participants confirmed that the findings accurately reflected their experiences. The interviewers maintained memos to record their thoughts, reflections, and biases, which might have influenced their interactions during the interviews to foster reflexivity and minimize potential biases.
Data Analysis
Data analysis was carried out by RY and PA. The process involved becoming familiar with the data, generating initial codes, searching for themes, reviewing and refining themes, defining and naming the themes, and producing the final report. Transcripts from both the in-depth interviews and the focus group discussions were analyzed inductively to allow themes to emerge directly from the data. The experts listened to the audio data via headphones and transcribed the interview data. Codes were generated manually via Excel and Microsoft Word. The experts then carefully read and reread the data to familiarize themselves with the material and obtain a sense of the whole. Codes were identified and grouped into subthemes on the basis of their shared concept, which were then clustered into themes on the basis of their relationships. Any discrepancies or differences in coding or theme interpretation between the two experts were discussed and resolved through consensus, with input from a third qualitative expert (SP), a consultant psychiatrist and a qualitative expert who served as an adjudicator to ensure rigor and credibility.
Ethical Considerations
Approval was obtained from the Institutional Ethics Committee (IEC:107/2023) of Kasturba Medical College and Kasturba Hospital, Manipal and from the Clinical Trials Registry- India (CTRI/2023/06/054190). Following the committee's guidelines, the participants were informed about the study and provided written informed consent for the interviews. To ensure confidentiality, participants were identified via codes instead of names. Participation in the study was entirely voluntary, and no monetary or material compensation was offered.
Results
Sociodemographic Characteristics of the Participants
The Table 1 shows that all participants from the patient population were males and unmarried: with varied educational backgrounds. The total mean duration of illness and caregiving was five years. The rehabilitation team consisted of experts, including two vocational trainers.
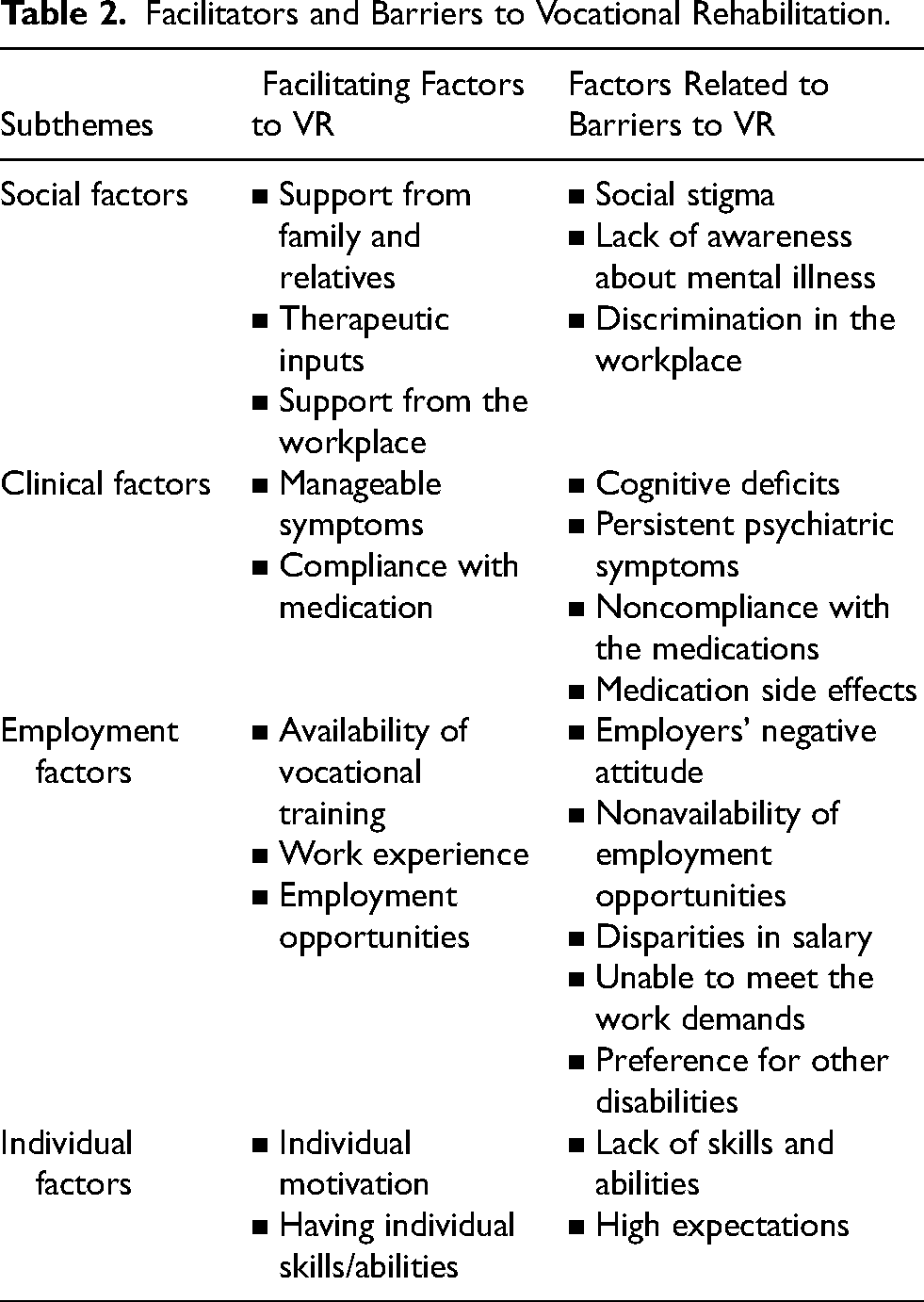
The inductive analysis of data from the in-depth interviews conducted among PWMI, caregivers, and employers, as well as the focus group discussion with rehabilitation experts via thematic analysis, led to the emergence of the theme ‘facilitators and barriers to vocational rehabilitation’ with several subthemes, including social factors, clinical factors, employment factors, and individual factors. The subthemes are mentioned in Table 2.
Facilitators and Barriers to Vocational Rehabilitation.
Facilitators for Vocational Rehabilitation
In addition to pharmacological intervention, many other factors play vital roles in enabling successful vocational rehabilitation services for PWMI. Many factors are derived from the four subthemes under the theme of facilitating factors for vocational rehabilitation programs. The subthemes are described below.
The study participants expressed several factors, such as the presence of support from others, ongoing therapeutic inputs and support in the workplace, which play crucial roles in facilitating employment opportunities.
“Sometimes they (work supervisors) help us to give medicine in the afternoon in the workplace. In a few incidents when patients had medicine in the afternoon, the people in the workplace cared for them… However, they help us in the workplace if any medications are present”. -FGDP 06
Many participants highlighted manageable symptoms and compliance with medication under the subtheme of clinical factors. Good adherence to medication helps prevent relapses and helps in the management of symptoms. Hence, the severity of symptoms plays a crucial role in determining the employment status of PWMI.
“…how symptomatic they are (need to be assessed) …. if they are going to harm themselves or a threat to harm others (need to evaluate) …”. -FGDP 05 “I hear voices… they say I am a fool… you cannot do anything… but I ignore and focus on the work… and mainly I take medications regularly… it helps mam.” -PTP 01
Some employment-related indicators emerged during the analysis. The availability of vocational training services, previous work experience, and availability of employment opportunities were the common factors.
“… we investigate the previous jobs that they have held and in terms of whether they can go back to the same level of job or maybe a level lower also maybe how they would their relationship with their job in the past as well… Therefore, I think that is an important point we keep in mind when we are exploring for job opportunities”. -FGDP 03
Many participants shared that individual factors such as individual motivation and having individual skills/abilities help in successful vocational rehabilitation or employment.
“…for work assessment, what we do is we talk to the client what is the working interest… in case the client is interested in doing a certain specific kind of job, we try to see whether the existing skills are matching the demands of that job”. -FGDP 03
Barriers to Vocational Rehabilitation
The goal of vocational rehabilitation programmes is to assist people with mental health issues or impairments in finding, keeping, or regaining employment. Nonetheless, several obstacles may prevent efforts for successful vocational placement of PWMI. Multiple subthemes and codes emerged as barriers in the VR program, as displayed in Table 2.
Several subthemes related to clinical factors are reported as barriers to vocational programs. Impairment caused by the illness, acute symptoms or persistent psychotic symptoms, noncompliance with drugs, and side effects of the medications are viewed as common clinical barriers to employment placement by the study participants. The common factors under this subtheme are described below.
“Finding difficult to concentrate, ma'am. I cannot understand and pay attention to cloth folding steps… A healthy person can understand within a week. I am a patient, and I cannot understand the multiple steps at one time when taught”. -PTP 01 “…patient behavior changes sometimes… they scream, some people get stuck in the bathroom…they talk to themselves, and through this, the customers will have a problem…if they have problems in the workplace, owners will tell us not to send the patient from next day”. -FGDP 07 “…every job I have tried doing is a flop…. multiple admissions… I was not taking medications properly. Every six months relapse used to happen…that affected my work life significantly”. PTP-05 “It (side effects of medications) hurts…. The problem with these illnesses is that doctors must also keep them on a trial-and-error basis. The medicines are trialled on an error basis… Therefore, it hurts sometimes. The medication causes dizziness… you cannot listen to others (in the workplace) owing to this”. -PTP 02
The participants expressed multiple social factors, which are barriers to vocational rehabilitation. Social stigma, lack of awareness about mental illness and discrimination in the workplace are the common factors that emerge under the subtheme of social factors.
“Everyone thinks that you need to be fine… challenges in getting a job again once you labeled as schizophrenia… if you say you have got this illness, you will not get it because they will think that you have come from some other world”. -PTP 02 “Mental illness is taboo here only…… If you are working for a company and then you say that you have an illness, they will throw you out whether you are performing well or not. They do not understand PWMI”. -PTP02 “(Supervisor will say) learn speed, you are so dull. Learn speed. Otherwise, they (Owner) will remove you from work if you cannot work like other (normal) people”. -PTP 01
The participants highlighted some barriers concerning employment. Employers’ negative attitudes, nonavailability of employment opportunities, salary disparities and inability to meet work demands were common factors identified under the subthemes of employment-related factors.
“When I went for one place to ask for a job for my brother… the owner asked me, can he be able to work continuously without any rest or not…by seeing itself, they are judging him…most people say we cannot give him a job… we cannot ever take him to the office”. -CGP 01 “…we are given some work training, but the training provided I did not get similar jobs, which is upsetting… I got trained in a retail shop… I got the job was the textile company…the company sees whether he is useful to our company or not. Within seconds, they are judging me. They fired me.” -PTP 01 “…every time I enquired them about that (salary), they said he does a good job…After six months, I requested their salary, saying since they are doing a good job…. They (the manager) directly responded by saying get out of here”. -FGDP 07 “The first one is speed…second is hard work and concentration. I cannot understand the steps… even in my previous job also, I was removed because I was not speedy enough to take the food orders and deliver on time”. -PTP 01 “The only thing that is there is reservation in government jobs which is shared by all types of disabilities, and more often the preference is given for people with other disabilities rather than for psychiatric disabilities… one or two percent to be reserved for that and remaining 3–4% other disabilities”. -FGDP 02
The participants expressed individual-related factors that could be barriers to vocational rehabilitation services, which included a lack of skills and abilities, impractical expectations, and a preference for other disabilities over mental illness.
“He cannot do more work or fast now. He gets tired when he does less work. Therefore, he can perform only light jobs. He gets tired easily. he cannot communicate with people or coworkers”. -CGP 01 “Sometimes the family's expectation might also be very different, like if the person previously has attained some degree of functioning and now, because the illness has deteriorated, they expect him to work with a similar background. They do not accept some kinds of jobs; they feel it is inferior” -FGDP 03
Discussion
The current study captured the factors associated with facilitators of and barriers to vocational rehabilitation from the stakeholder's perspective. Most PWMIs can do some work when the barriers are decreased (Falkum et al., 2017). The key stakeholders of the vocational rehabilitation program, including the patients, caregivers, rehabilitation experts and employers, participated in the study. The involvement of stakeholders in mental health research is increasingly recognized, and their engagement helps improve the relevance of research, identifying the needs of diverse populations and designing interventions (Forsythe et al., 2016; Murphy, 2022; Pellegrini & Lovati, 2025).
In addition to pharmacological interventions, many other aspects enable successful vocational rehabilitation services for PWMI. Many factors are derived from the four subthemes of facilitating and overcoming barriers to vocational rehabilitation programs.
Under the subtheme of social factors, most of the participants expressed the need for support from various sources, such as relatives, friends, treatment teams or the government, to help them gain employment opportunities. Multiple studies have highlighted the importance of support from primary and secondary support systems in the process of vocational rehabilitation, such as exploring job opportunities, providing employment opportunities for people with disabilities, and facilitating need-based emotional support (Jäckel et al., 2020; Maddineshat et al., 2022; Samuel et al., 2020; Smeets et al., 2019). These types of support can offer guidance and practical assistance throughout vocational rehabilitation (Alatawi, 2024; Almalki et al., 2022). Two cross-sectional studies among both service receivers and providers reported that social support improved vocational outcomes and social integration (Hoter Ishay et al., 2025; Widiyawati et al., 2021). A pilot study by Cheng & Yen, (2021) highlighted that providing social support through peer-led vocational rehabilitation improved occupational functioning. In line with the current study findings, the importance of support from tertiary level such as organizations, government sectors or vocational agencies for vocational rehabilitation services has been reported (Boeltzig-Brown et al., 2013; Maddineshat et al., 2022).
The current study revealed that a preference for other disabilities in the employment sector is highlighted as a barrier to the participants’ employment. Atilola et al., (2014) also noted the disparity between mental illness and other disabilities with respect to job reservations or the provision of employment opportunities and the allocation of resources. A study by (Maddineshat et al., 2022) suggested that having government policies for people with disabilities enables employment opportunities for PWMIs.
With respect to barriers to employment under the subtheme of social factors, the participants viewed social stigma and discrimination in the workplace as barriers to vocational rehabilitation. Prior studies have highlighted the stigma attached to mental illness, lack of awareness about mental illness and discrimination in the workplace as barriers to vocational rehabilitation programs (Atilola et al., 2014; Corbière et al., 2011; Maddineshat et al., 2022; Netto et al., 2016; Samuel et al., 2020; Thomas et al., 2019; van Niekerk, 2016).
A qualitative study by Koletsi et al. (2009) noted concerns about the disclosure of mental illness among study participants in their workplace due to the stigma and fear of being labeled “disabled”. Similarly, disclosing the client's mental health condition to the employer would make it difficult to recruit for the job because of stigma and prejudice about mental illness (Brouwers et al., 2020; Vukadin et al., 2021).
The analysis revealed that clinical factors could act as both barriers to and facilitators of vocational rehabilitation. Previous studies have reported that clinical factors such as clinical symptoms and cognitive deficits (Khare et al., 2021; Maddineshat et al., 2022; van Niekerk, 2016), relapse of illness, side effects of medications and continuing symptoms of illness (Boo et al., 2014) are the major clinical barriers to vocational rehabilitation. Similarly, studies have well documented the association between clinical stability and successful vocational placement across mental health conditions (Netto et al., 2016; Samuel et al., 2020).
The consumers expressed the impact of medication side effects on employment. Notably, psychotropic medications are a common mode of treating PWMIs. These medications are effective in managing clinical symptoms, which can cause various side effects. Hence, studies have recommended identifying and managing side effects, educating consumers and utilizing reasonable accommodations (e.g., modifications in work schedules and supportive employer policies) if medications are interfering with employment (Collins et al., 2024; Deenik et al., 2018; Rangarajan et al., 2020; Thomas et al., 2019).
In support of the findings of the present study, the availability of vocational training, employment opportunities, and access to suitable work are viewed as the determining factors for both facilitating and barriers (Boyce et al., 2008; Khare et al., 2021; Larsson et al., 2022). A qualitative study by Marwaha & Johnson, (2005) among consumers reported a number of concerns, including minimal employment opportunities and challenges in suitable work. Notably, most unemployed PWMI desire to work and indicate a variety of job support, including help finding a job (Khare et al., 2021). Studies have suggested various strategies to facilitate employment opportunities or access to suitable work among mentally ill individuals, such as the utilization of social firms, the involvement of nongovernmental organizations, and the utilization of various approaches to supported employment (Morant et al., 2021; Paluch et al., 2012).
In India, while vocational interventions for PWMI are considered, vocational services must be designed on the basis of two major factors. First, options for social firms and vocational models are not available in the Indian context. Second, the role of the family in facilitating employment opportunities, as many PWMIs work for family-owned businesses or obtain their jobs through family contacts (Khare et al., 2021), and the inclusion of family members in delivering such services is essential. Considering the importance of the family to work and life in general in India and the fact that many participants were working for family-owned businesses or obtained their jobs through family contacts, the inclusion of family members in providing such adapted services would be critical (Khare et al., 2021; Thekkumkara et al., 2024).
Furthermore, the Rights of Persons with Disability Act 2016 (Ministry of Law and Justice, Government of India. (2016)) provided empowering PWMIs by offering vocational training, a special employment exchange, and job reservation. Studies have also recommended the need for culturally appropriate vocational rehabilitation models (Andrade et al., 2023; Jagannathan et al., 2020).
Research has revealed that negative attitudes in the workplace and disparities in salaries are viewed as major barriers to employment. Studies on consumers’ perspectives on supportive work environments have highlighted that workplace accommodations, support from coworkers, and workplace relationships are associated with greater job satisfaction (Lanctôt et al., 2012; Villotti et al., 2012). A qualitative investigation among social firm managers and clinicians highlighted the importance of social support, workplace accommodations, and an accepting working environment for PWMIs for successful employment (Morant et al., 2021). Studies have recommended various strategies to mitigate workplace concerns, such as knowledge exchange between rehabilitation stakeholders, reasonable accommodations and supportive employer policies for persons with disabilities (Larsson et al., 2022; Rangarajan et al., 2020; Thomas et al., 2019).
In alignment with previous studies, the current study revealed that individual factors such as skills and abilities and personal motivation can either facilitate or affect employment (Iwanaga et al., 2019; Maddineshat et al., 2022; Thomas et al., 2019; van Niekerk, 2016). A collaborative approach that provides work incentives and psychological interventions could help facilitate employment opportunities among PWMIs (Crowther et al., 2001; Noteboom et al., 2024). Considering the need for ongoing support, skills training and equal wages, the individual placement and support (IPS) model of supported employment was developed for PWMIs, and IPS has consistently led to higher rates of overall vocational outcomes (Drake et al., 2012; Frederick & VanderWeele, 2019). However, there are numerous limitations for implementing various employment models in resource-limited countries (Thekkumkara et al., 2024).
Strengths and Limitations
The major strength of this study is that the data was collected from vocational service providers and consumers. The views of four key stakeholders- the rehabilitation team, the employer, PWMI and their caregivers—were triangulated via a range of methodologies. The integration of all stakeholder perspectives in a single qualitative study is distinctive and enhances the importance and depth of this research.
The study has several limitations. The data were collected from single rehabilitation center with a relatively small sample size, the findings may not be fully generalizable to all settings or populations, and it limit the transferability of findings to those not engaged in such rehabilitation services. Furthermore, potential regional differences in vocational rehabilitation outcomes among PWMI may limit the generalizability of the findings. Gender imbalances were noted among the PWMIs due to lack of eligible female participants during data collection. Despite these limitations, the study provides valuable insights that can inform the development of culturally tailored, stakeholder-driven vocational rehabilitation models in India.
Implications for Practice
The results highlight the roles of each stakeholder in vocational rehabilitation, and collaborative dialog between these stakeholders benefits the outcomes of the vocational results. Incorporating family-centered approaches strengthens the vocational rehabilitation programs for PWMIs. Findings highlighted the limited availability of vocational rehabilitation models in developing countries and underscores the need for collaboration among community leaders, NGOs and government agencies to promote skill development and workplace inclusion.
Conclusion
The process of recovering from mental illness is complex, and employment is commonly acknowledged as a crucial component. PWMI can resume and stay employed with the support of vocational rehabilitation. The current study listed various factors that facilitate or hinder vocational rehabilitation programs. There is an enormous need for support from families, employment firms, government institutions and mental health care providers for a successful vocational rehabilitation program. Hence, strategies such as creating awareness among stakeholders about the importance of vocational programs and designing community-based and individually tailored employment programs could help maintain ‘persons’ employment status in the community.
Supplemental Material
sj-docx-1-jvr-10.1177_10522263261430693 - Supplemental material for Facilitators and Barriers to Vocational Rehabilitation for People with Mental Illness: A Qualitative Study of Perspectives from Mental Health Service Providers and Consumers
Supplemental material, sj-docx-1-jvr-10.1177_10522263261430693 for Facilitators and Barriers to Vocational Rehabilitation for People with Mental Illness: A Qualitative Study of Perspectives from Mental Health Service Providers and Consumers by Sneha Murali, Praveen Arahanthabailu, Rajeshkrishna P Bhandary, Renjulal Yesodharan and Podila Satya Venkata Narasimha Sharma in Journal of Vocational Rehabilitation
Footnotes
Acknowledgments
Not applicable.
ORCID iDs
Ethical Statement
Approval was obtained from the Institutional Ethics Committee (IEC:107/2023) of Kasturba Medical College and Kasturba Hospital, Manipal and from the Clinical Trials Registry- India (CTRI/2023/06/054190). Following the committee's guidelines, the participants were informed about the study and provided written informed consent for the interviews. Researchers visited participants at their homes for the interviews. To ensure confidentiality, participants were identified via codes instead of names.
Informed Consent
Written informed consent to participate was obtained from all individual participants included in the study. Participants were assured of confidentiality and the right to withdraw at any stage without penalty.
Consent for Publication
Written informed consent for publication of anonymized excerpts of participants’ responses was obtained from all participants. No identifying personal details, images, or videos have been included in this manuscript.
Author Contributions
SM, PA, and RPB were involved in the conceptualization of the study. PA and RY conducted the interviews; both were experienced qualitative researchers fluent in the local language. The PA is a faculty member in psychiatric social work trained in qualitative research, whereas RY is a psychiatric nursing faculty member and qualitative research expert who also serves as a master trainer for qualitative research studies. SM, PA, SP and RY contributed to the data analysis and thematic coding. The original draft was prepared by SM and PA, while RPB, SP, and RY contributed to reviewing and editing the manuscript. RPB and SP provided overall supervision. All the authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The qualitative data generated and analysed during this study are not publicly available due to the presence of sensitive personal information and ethical restrictions. Participants were assured of strict confidentiality, and consent was not obtained for public data sharing. This is in accordance with SAGE's data sharing policy, which allows restrictions where data contain sensitive personal or confidential material. However, a detailed description of the methodology and anonymized excerpts supporting the findings are provided within the article.
Supplemental Material
Supplemental material for this article is available online.