
Abstract
Background
Firefighting is a physically demanding and hazardous profession. Work-related musculoskeletal disorders (WMSDs) and declining work ability threaten workforce sustainability and public safety. Despite its critical importance, comprehensive occupational health data on this population remains limited in certain regions.
Objective
This study evaluated the Work Ability Index (WAI) and its occupational health correlates among Turkish firefighters.
Methods
This cross-sectional study examined 428 active-duty male firefighters from major Turkish cities using three validated instruments: the Work Ability Index, Nordic Musculoskeletal Questionnaire, and International Physical Activity Questionnaire. Multivariable linear regression modeling identified independent predictors of work ability.
Results
Mean WAI score was 42.66 ± 5.08, with 11.2% having poor or moderate work ability. High prevalence of overweight/obesity (76%) and WMSDs particularly lower back (16%) and neck (12%) was observed. Age was the strongest independent predictor (β = –0.277, 95% CI: [–0.221 to −0.087], p < 0.001). WMSDs showed robust negative association with work ability (β = –0.200, 95% CI: [–3.080 to −1.187], p < 0.001) when controlling for age and physical activity. Chronic disease was significantly associated with lower WAI scores (p < 0.001).
Conclusion
While the overall work ability of active-duty Turkish firefighters is high, age-related decline and chronic health conditions are significantly associated with reduced capacity. These associative findings highlight the need for targeted health surveillance, though they must be interpreted cautiously due to potential healthy worker survivor bias inherent in such physically demanding occupational cohorts.
Keywords
Introduction
Firefighting is internationally recognized as one of the most physically and psychologically demanding occupations. Firefighters are regularly exposed to extreme heat, toxic substances, unpredictable emergency situations, and physically strenuous tasks that require lifting, carrying, and operating in unsafe or constrained environments while wearing heavy protective equipment.1–4 These occupational hazards contribute to significantly elevated risks of acute injuries and chronic health problems compared to the general workforce. The resulting decline in functional capacity and premature exit from the workforce not only represents a substantial occupational health failure but also imposes a significant societal and economic burden, directly impacting the operational resilience of public safety services globally.5–7
Among the most prevalent occupational health concerns in firefighters are work-related musculoskeletal disorders (WMSDs), which frequently affect the lower back, neck, shoulders, and knees.8–10 Recent global estimates suggest that over 40% of firefighters suffer from at least one form of musculoskeletal complaint, with cumulative exposure increasing the likelihood of early retirement, reduced functional capacity, and diminished quality of life.11–13 In Turkey, similar findings have been reported, with firefighters often citing the lumbar region and neck as the most problematic areas. 14 However, many national studies have remained limited in scope, often focusing solely on self-reported symptoms or specific injuries, without integrating comprehensive assessments of work performance capacity. While localized studies in Turkey have documented the high prevalence of these musculoskeletal complaints, there remains a critical gap in understanding how these physical impairments systematically correlate with overall work performance capacity in this specific occupational cohort.
This brings forward the critical importance of evaluating work ability a multidimensional construct that reflects a worker's current and future capacity to meet job demands, considering physical health, psychological resilience, diagnosed diseases, and job-related stressors. One of the most widely accepted and validated tools to measure this is the Work Ability Index (WAI), developed by the Finnish Institute of Occupational Health.15,16 The WAI serves as a crucial early warning system, aligning with the core principles of the Job Demands-Resources model by providing a holistic measure of the balance between an individual's health resources and the demands of their work environment.17,18 Unlike simple health status measures, the WAI captures the complex interplay between an individual's resources and the demands of their occupation, offering a predictive framework for identifying those at risk of work disability or premature exit from the labor force.18–20
From an epidemiological perspective, the decline in work ability among firefighters cannot be viewed merely as a function of chronological aging. Rather, it represents a complex interplay of cumulative occupational exposures, physiological changes, and musculoskeletal morbidity over the life course. 21 According to the Job Demands-Resources (JD-R) model, an imbalance between the intense physical demands of firefighting and an individual's physiological resources potentially compromised by aging or chronic WMSDs is strongly associated with reduced work ability. 22 Within this framework, we hypothesize that advancing age and the presence of WMSDs are key factors inversely associated with work ability, whereas regular physical activity may act as a supportive resource. However, this relationship is complex; WMSDs may mediate the pathway between aging and reduced work ability, and unmeasured psychosocial stressors or lifestyle factors may act as confounders. 23
Despite its relevance, the WAI remains underutilized in firefighter populations particularly in middle and lower-income countries where occupational health systems may be reactive rather than preventive. Studies that do incorporate the WAI have shown it to be a sensitive indicator of declining work capacity, especially in aging personnel, and have linked lower WAI scores to high physical workload, low physical activity, poor sleep quality, and the presence of chronic conditions.24,25 Moreover, WAI scores have been consistently associated with absenteeism, injury risk, and are a robust predictor of early retirement and premature work exit in physically intensive occupations. 26
Given the essential public safety functions that firefighters perform, preserving their functional capacity through evidence-based monitoring and intervention is not only an occupational health priority but also a matter of societal resilience. The sustainability of emergency services hinges on the long-term work ability of its personnel, making WAI a critical metric for workforce planning and risk mitigation.16,17,27 Integrating the WAI into firefighter health assessments enables early identification of decline, the implementation of targeted preventive measures (e.g., ergonomic training, fitness maintenance programs), and data-informed workforce planning.
Importantly, any cross-sectional evaluation of occupational health in physically demanding professions must account for inherent selection biases, most notably the ‘healthy worker effect’ (HWE) and the ‘healthy worker survivor effect’ (HWSE).28,29 Firefighters are subject to rigorous initial health screening (healthy hire effect) and continuous physical demands. Consequently, individuals who develop severe WMSDs or experience a significant decline in work ability often exit active duty prematurely or transition to administrative roles. 30 This selective attrition leaves a “survivor” cohort of relatively healthier individuals, which can epidemiologically mask the true burden of occupational morbidity and artificially inflate cross-sectional estimates of work ability. 31 Acknowledging these biases is essential for the accurate interpretation of any cross-sectional findings in this occupational group.
Therefore, the present study aimed to evaluate the Work Ability Index (WAI) and its associated occupational health determinants specifically musculoskeletal disorders, body mass index, physical activity levels, and sociodemographic characteristics among professional firefighters in Turkey. By employing an integrated approach that considers both physical and lifestyle-related factors, this research seeks to provide a comprehensive risk profile regarding workforce sustainability. Identifying these key determinants is essential for informing targeted occupational health strategies that promote long-term well-being and operational readiness in this critical public safety cohort.
Method
Study design and participants
This study was designed as a cross-sectional, descriptive investigation aimed at evaluating work ability and musculoskeletal health among professional firefighters in Türkiye. The target population comprised active-duty male firefighters employed by fire departments across major metropolitan municipalities, ensuring representation from distinct geographical regions. Data collection was conducted over a six-month period, from June to December 2023. In Türkiye, professional firefighters employed by metropolitan municipalities typically operate under a rigorous 24-h on-duty, 48-h off-duty shift schedule.
An a priori power analysis (G*Power 3.1; medium effect size f = 0.25, = 0.05, 95% power)α established a minimum requirement of 280 participants. Utilizing a convenience sampling approach during routine station visits, 428 eligible active-duty firefighters were ultimately recruited (85.6% response rate), providing robust statistical power. Eligibility required active-duty status and voluntary consent, while personnel on medical leave or unable to complete the protocol were excluded. It is crucial to acknowledge that this sampling method, which inherently excludes personnel on medical or administrative leave, introduces selection bias. 32 Consequently, this active-duty cohort is subject to the healthy worker survivor effect (HWSE), potentially underestimating occupational morbidities and overestimating average work ability compared to the broader historical population.29,33
Data collection procedures
Data collection was carried out through face-to-face structured interviews conducted by trained research staff, complemented by standardized anthropometric assessments. All interviews were administered in private rooms within fire stations to ensure participant confidentiality and comfort. Each session lasted approximately 20 to 25 min.
A structured questionnaire was used to gather sociodemographic data (e.g., age, marital status, educational attainment), occupational history (e.g., duration of employment, shift schedule, and duty type), and health-related variables, including the presence of chronic diseases, smoking status, and physical activity level.
The questionnaire items were adapted from validated instruments frequently utilized in occupational health studies involving emergency responders. Anthropometric measurements were taken in accordance with World Health Organization (WHO) guidelines. Anthropometric data, including height and weight, were self-reported by participants based on their most recent medical examination records and were documented accordingly.
Body Mass Index (BMI) was subsequently calculated as weight in kilograms divided by height in meters squared (kg/m2) and classified into standard WHO categories: underweight (<18.5), normal weight (18.5–24.9), overweight (25.0–29.9), and obesity (≥30.0).
Assessment of musculoskeletal disorders
The prevalence and location of musculoskeletal symptoms were evaluated using the standardized Nordic Musculoskeletal Questionnaire, which has been validated for use in Turkish populations. 34 This tool systematically assesses the occurrence of pain or discomfort in nine body regions (e.g., lower back, neck, shoulders) over the preceding 12 months and 7 days, making it highly suitable for identifying chronic and recent complaints in physically demanding occupations. 35
Work ability Index (WAI)
To assess the primary outcome, we utilized the Turkish version of the Work Ability Index (WAI), a globally recognized and validated tool for measuring the balance between an employee's health resources and their job demands.15,16,36 This seven-dimension instrument produces a composite score from 7 to 49, which is then classified into four categories: poor (7–27), moderate (28–36), good (37–43), and excellent (44–49). The WAI was selected for its proven predictive validity for long-term work disability and its holistic approach to evaluating work capacity. 15
Assessment of physical activity
Physical activity levels were quantified using the Turkish-validated short form of the IPAQ. 37 This questionnaire estimates the time spent in walking, moderate-intensity, and vigorous-intensity activities over the last seven days. Total physical activity was calculated as a MET-min/week score by summing the products of activity duration, frequency, and standard MET values (3.3 for walking, 4.0 for moderate, and 8.0 for vigorous activity). Participants were subsequently classified as having low, moderate, or high physical activity levels based on established IPAQ scoring guidelines. 38
Ethical considerations
The study was conducted in strict accordance with the ethical principles for medical research involving human subjects, as outlined in the Declaration of Helsinki. The research protocol and all associated procedures were formally reviewed and approved by the Ethics Committee for Social and Human Sciences Research at Kastamonu University (Approval Date: March 29, 2023, Meeting/Decision No: 2023/10-4).
Prior to data collection, all participants were comprehensively informed about the study's objectives, the voluntary nature of their involvement, and their right to withdraw at any stage without any penalty. Consequently, written informed consent was obtained from each individual participant. To ensure the highest standards of privacy and data protection, all participant information was fully anonymized and handled in accordance with institutional data confidentiality guidelines.
Statistical analysis
Data were analyzed using IBM SPSS Statistics for Windows, Version 23.0 (Armonk, NY: IBM Corp). Continuous variables were assessed for normality, and descriptive statistics were presented as mean ± SD for continuous measures and frequencies (%) for categorical data. Given the non-normal distribution of WAI scores, we employed non-parametric tests to compare work ability across groups. The Mann-Whitney U test was used for two-group comparisons while the Kruskal-Wallis H test assessed differences across three or more groups.
Associations between WAI and continuous variables (age, work experience, BMI, physical activity) were examined using Spearman's rank-order correlation, which is appropriate for ordinal outcomes and non-linear relationships. To determine the independent predictors of work ability, we constructed a multiple linear regression model with WAI as the dependent variable and age, work experience, BMI, and physical activity as independent variables. Statistical significance was set at p < 0.05 for all analyses.
Prior to multivariable linear regression, potential multicollinearity among correlated predictors specifically age and work experience was formally assessed using Variance Inflation Factor (VIF) and tolerance statistics. All VIF values were confirmed to be well below the conservative threshold of 5 (maximum VIF = 1.858 for age; VIF for work experience = 1.837), indicating that multicollinearity did not significantly distort the regression estimates. 39
Results
The study cohort comprised 428 male Turkish firefighters, with a mean age of 40.73 ± 9.139 years and an average work tenure of 10.60 ± 7.65 years (Table 1). The demographic profile indicates a mature, experienced workforce, predominantly married (83.9%) and engaged in shift work (97.0%). Physical activity levels demonstrated substantial variability (mean = 6760.42 MET-min/week, SD = 8728.55), with a markedly right-skewed distribution (Supplementary Table S2), necessitating non-parametric analytical approaches. A concerning finding was the high prevalence of excess weight, with 56.8% classified as overweight and 19.2% as obese, resulting in a mean Body Mass Index (BMI) of 27.22 ± 3.70 kg/m (Table 2).
Descriptive characteristics of continuous study variables.
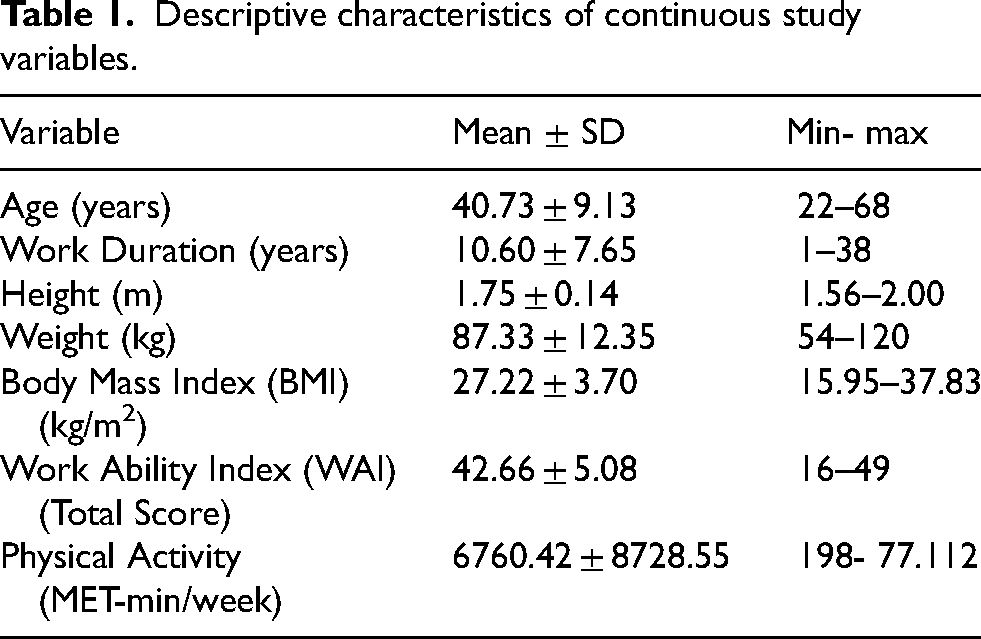
Descriptive characteristics of continuous study variables.
Distribution of categorical variables Among participants.
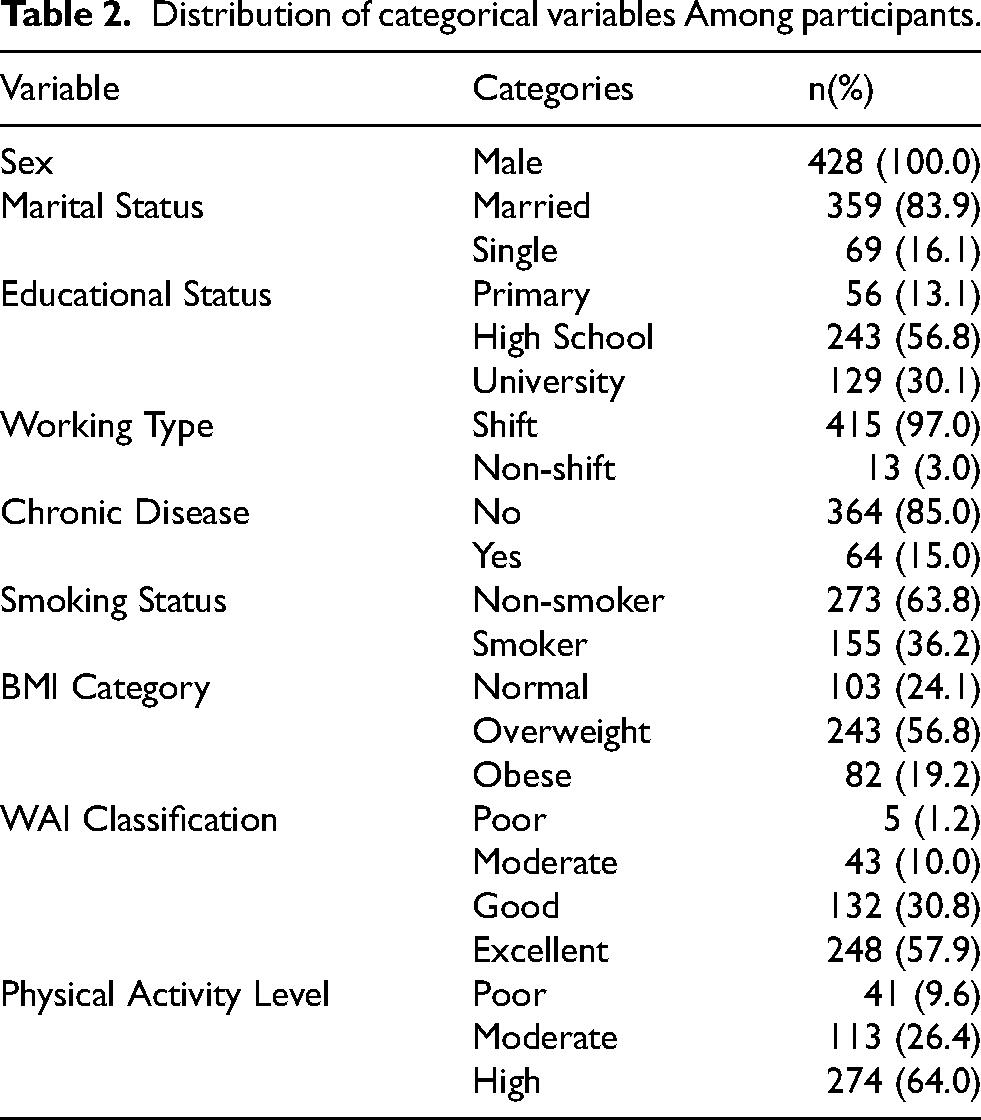
The mean total Work Ability Index (WAI) score was 42.66 ± 5.08. According to the standard WAI classification, 57.9% of the participants demonstrated Excellent work ability, while 11.2% were categorized as having Poor or Moderate work ability (Table 2).
Non-parametric comparative analyses revealed significant differences in WAI scores across several health and occupational subgroups (Table 3). Firefighters reporting a Chronic Disease exhibited significantly lower WAI scores compared to their healthy counterparts (U = 6957.5, p < 0.001), with a medium effect size (r = 0.248).
Group differences in work ability Index (WAI) scores with effect sizes.
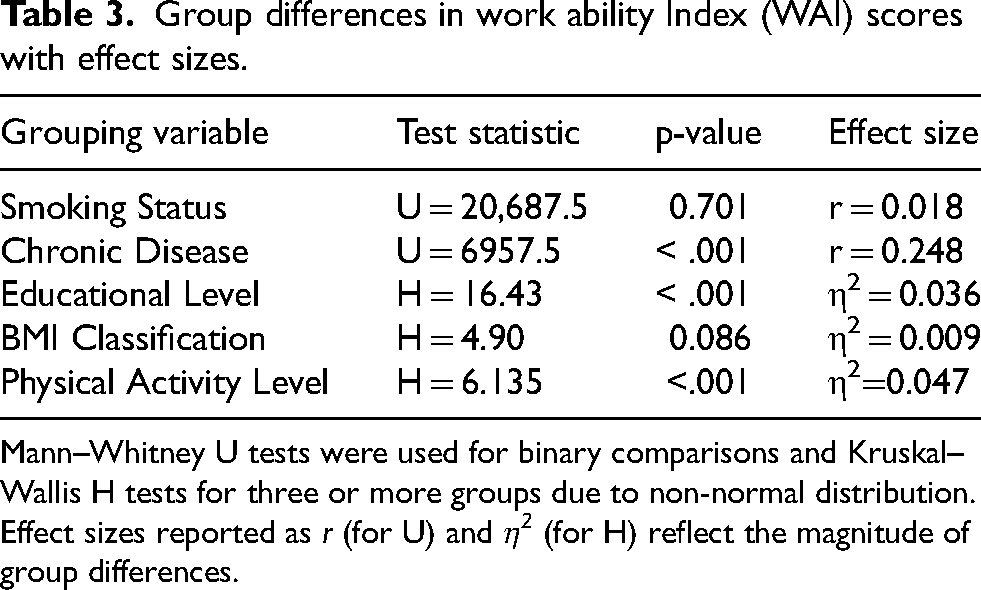
Mann–Whitney U tests were used for binary comparisons and Kruskal–Wallis H tests for three or more groups due to non-normal distribution. Effect sizes reported as r (for U) and η2 (for H) reflect the magnitude of group differences.
Furthermore, WAI scores varied significantly based on Educational Level
Spearman's correlation analysis indicated that the WAI score was negatively correlated with Age (rho = −0.290, p < 0.01) and Work Experience (rho = −0.196, p < 0.01), suggesting a decline in self-assessed work ability with increasing age and tenure (Table 4).
Spearman's rank-order correlations between age, work experience, BMI, physical activity and WAI score.
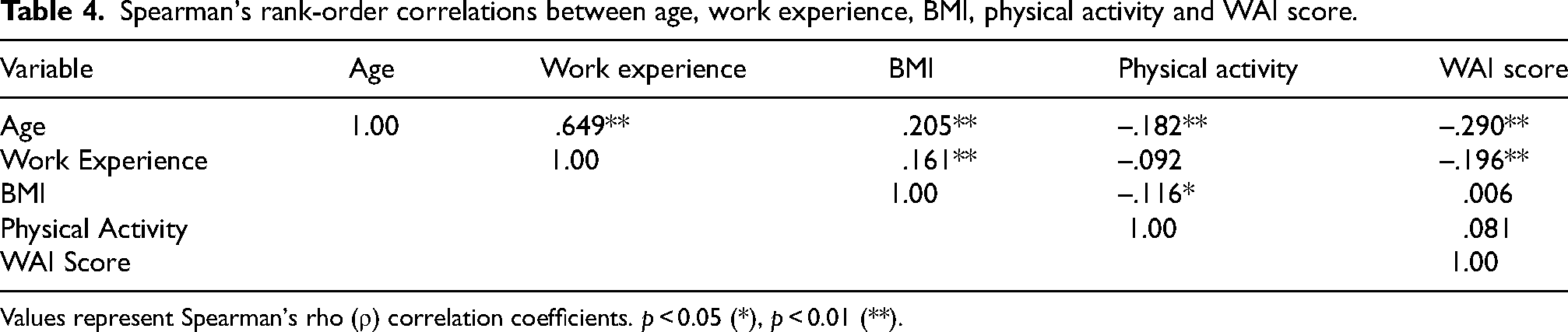
Values represent Spearman's rho (ρ) correlation coefficients. p < 0.05 (*), p < 0.01 (**).
A multivariable linear regression analysis was conducted to identify independent predictors of work ability, incorporating age, presence of WMSDs, physical activity, and work experience as covariates (Table 5). Despite a strong bivariate correlation between age and work experience (ρ = .649, p < .001), collinearity diagnostics indicated acceptable variance inflation factors (VIF < 2.0), confirming that multicollinearity assumptions were not violated. The overall model was statistically significant (F(4, 423) = 18.674, p < .001) and explained 15.0% of the variance in WAI scores.
Multiple linear regression predicting work ability Index (WAI).
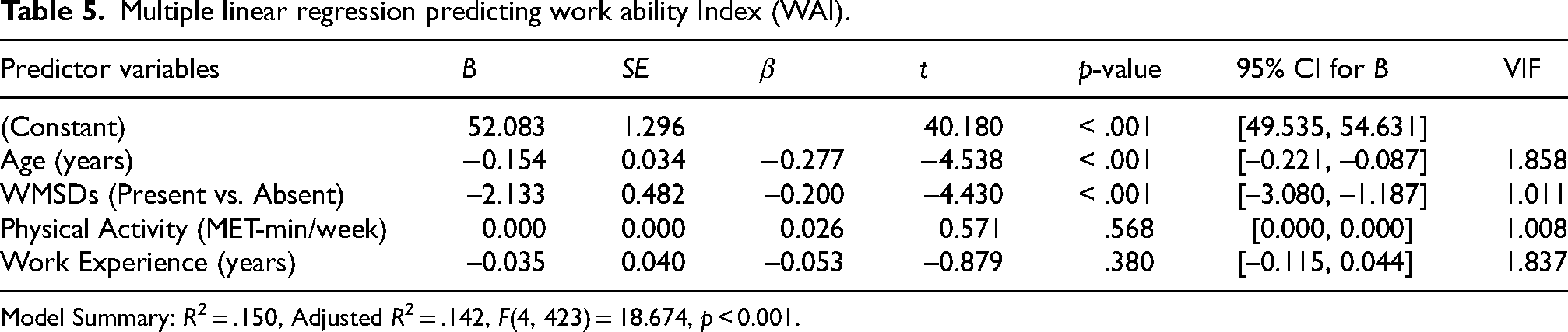
Model Summary: R2 = .150, Adjusted R2 = .142, F(4, 423) = 18.674, p < 0.001.
Age emerged as the strongest independent predictor, demonstrating a significant negative association with work ability (β = –0.277, 95% CI [–0.221, −0.087], p < .001). Crucially, the presence of WMSDs was also identified as a robust independent predictor, significantly associated with lower WAI scores (β = –0.200, 95% CI [–3.080, −1.187], p < .001) even after controlling for age and physical activity. Physical activity (β = 0.026, p = .568) and work experience (β = –0.053, p = .380) did not reach statistical significance in the adjusted model. Although the explained variance is modest (R2 = 15.0%), this is consistent with occupational health studies investigating complex constructs like work ability, where unmeasured psychosocial factors likely account for the remaining variance.
To further elucidate the relationship between age, physical health parameters, and work ability, a hierarchical regression analysis was performed to test for interaction effects (Supplementary Table S1). While the interaction between age and physical activity was not statistically significant (β = 0.123, p = .507), a significant interaction was observed between age and BMI (β = –1.374, p = .003). The inclusion of these interaction terms significantly improved the model fit (ΔR2 = 0.021, p < .001). This significant Age × BMI interaction indicates that the negative association between elevated BMI and work ability is substantially more pronounced among older firefighters, highlighting a compounding occupational health risk in this demographic.
Musculoskeletal complaints were prevalent across the firefighter cohort, with 12-month prevalence rates varying substantially by anatomical region (Figure 1). Lower back pain emerged as the most frequently reported complaint, affecting 16.1% of respondents, followed by neck pain (12.1%) and upper back pain (9.6%). Collectively, spinal regions (lower back, neck, and upper back) accounted for 37.8% of all musculoskeletal complaints. The remaining complaints were distributed across the extremities and joints, with knee pain (8.4%), shoulder pain (8.2%), and foot pain (6.1%) representing the secondary sites of musculoskeletal involvement. Elbow, hip, and hand pain were less frequently reported, each occurring in approximately 3–4% of the cohort.
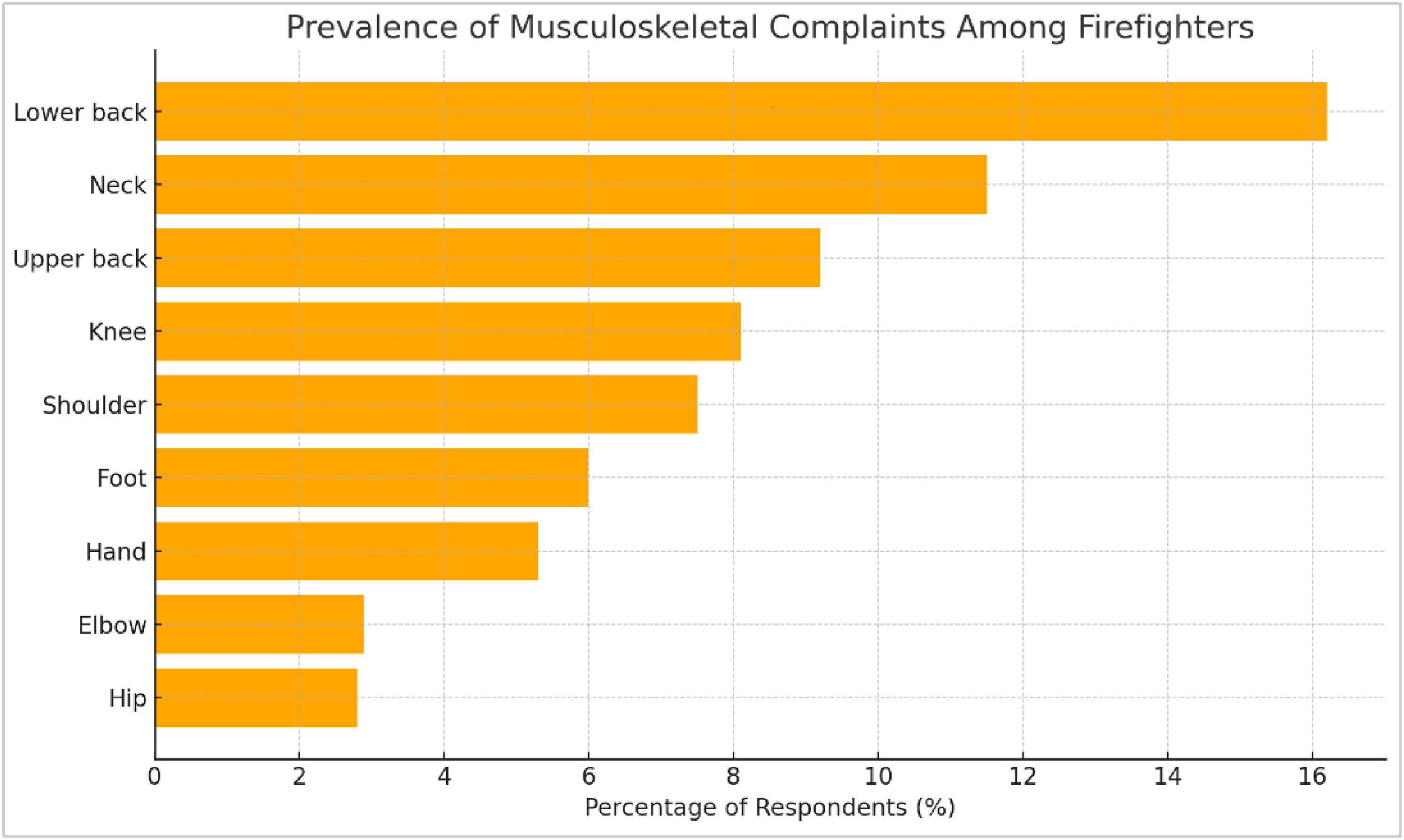
Prevalence of self-reported musculoskeletal complaints among firefighters. Lower back, neck, and upper back were the most frequently affected regions.
This study is one of the first national studies to comprehensively examine the relationship between the Work Ability Index (WAI), musculoskeletal disorders (MSDs), age, body mass index (BMI), and chronic diseases among Turkish firefighters. The mean WAI score for firefighters in our study was determined to be 42.66 ± 5.08, corresponding to the “Good” work ability category. The fact that the vast majority of participants (88.8%) reported “Good” or “Excellent” work ability indicates that the active-duty Turkish firefighting workforce generally possesses a high working capacity. However, these relatively high overall WAI scores must be interpreted cautiously, as they strongly point to the presence of the healthy worker survivor effect (HWSE).29,30 Firefighters who experience severe MSDs or a precipitous drop in work ability typically exit active service prematurely. Therefore, our cross-sectional active-duty cohort represents a “survivor” population, which inherently masks the true severity of age-related occupational decline and musculoskeletal morbidity in the firefighting profession.28,31
The most significant finding of the study is that age is the sole and statistically significant independent predictor of the WAI score (β=–0.304, p < 0.001). This negative relationship clearly demonstrates that the perceived work ability of firefighters decreases as they age. Viewed through the lens of the Job Demands-Resources (JD-R) model and life-course exposure frameworks, the decline in work ability among firefighters is not a sudden acute event, but rather the cumulative manifestation of repetitive biomechanical stress, acute trauma, and chronic physiological wear-and-tear interacting with the natural aging process over decades of service. 40 This finding is highly consistent with recent high-impact studies. For instance, Magnavita et al. (2024) similarly demonstrated a robust inverse relationship between age and WAI scores in the healthcare sector, emphasizing that age-related decline is a universal phenomenon in physically and psychologically demanding occupations. 41 Furthermore, Hanvoravongchai et al. (2024) highlighted that the mismatch between age-related physiological decline and sustained job demands inevitably leads to a decrease in WAI scores, particularly emphasizing that physical fitness becomes a more critical determinant of work ability in older workers. 42
A critical finding is the high prevalence of MSDs, particularly affecting the lower back (16.1%) and neck (12.1%). These findings align closely with the recent comprehensive meta-analysis by Tahernejad et al. (2024), which reported a pooled MSD prevalence of 46.39% among firefighters globally, with the lumbar (34.32%) and cervical (18.36%) regions being the most affected due to the biomechanical overload inherent in firefighting tasks. Firefighters routinely wear heavy protective gear, perform repetitive lifting, and operate in awkward postures under time-sensitive conditions. When these occupational stressors are superimposed on the natural physiological decline associated with aging, the risk of developing chronic, work-limiting musculoskeletal pathology increases substantially. Although MSDs showed a significant association with WAI scores in univariate analysis, they did not emerge as independent predictors in the multivariable model. This suggests that the effect of MSDs on perceived work ability may be confounded or overshadowed by other health-related factors such as age and chronic disease presence.15,17,35
Furthermore, our interaction analysis provides nuanced insights into how age modifies physical vulnerabilities. The significant age-by-BMI interaction indicates that excess body weight exerts a compounding negative effect on work ability in older firefighters. While younger personnel might physiologically compensate for the cardiovascular and biomechanical burden of a higher BMI, this compensatory capacity appears to diminish with age. Interestingly, despite the known protective effects of physical activity,19,42 the lack of an independent predictive value for physical activity in our multivariable model echoes the “physical activity paradox” described by Ko et al. (2023), where high levels of occupational physical exertion may not confer the same protective cardiovascular and work ability benefits as leisure-time physical activity, and in some cases, may even exacerbate physical decline. 43
Practical implications for occupational health
A noteworthy finding is the significantly lower WAI scores among participants with chronic conditions (p < 0.001), including hypertension, diabetes, and cardiovascular diseases. These conditions impair not only physical performance but also functional adaptability. Strauss et al. (2021) demonstrated that higher cardiorespiratory fitness is strongly associated with lower cardiovascular risk factors in firefighters, underscoring that mitigating metabolic risks is as crucial as ergonomic interventions. 44 This highlights the urgent need for proactive, multidisciplinary occupational health programs that go beyond injury prevention and include comprehensive chronic disease management.39–41 Recent European and North American studies emphasize the value of integrating WAI into occupational health surveillance systems for aging firefighter populations, as WAI has been proven by Bethge et al. (2020) to be a highly valid predictor of health-related exit from work, absenteeism, and even mortality. Weight management interventions should be particularly prioritized for aging firefighters, whereas tailored physical fitness programs remain universally applicable across the entire career span. 45
Methodological limitations
Several limitations must be acknowledged when interpreting these findings. First, the cross-sectional design restricts the ability to infer causality and introduces the potential for reverse causation; for instance, declining work ability might lead to reduced physical activity, rather than the reverse. Second, the reliance on self-reported data for musculoskeletal complaints and physical activity introduces potential information bias, including recall bias and social desirability bias, particularly in an occupational cohort where physical fitness is highly valued. The markedly right-skewed distribution of the IPAQ data may partly reflect such measurement artifacts. Third, the use of convenience sampling and the inclusion of only male participants limit the external validity and generalizability of the results to female firefighters or other emergency responder populations.
Finally, the relatively low explained variance in our multivariable regression model (R2 = 11.1%) strongly suggests the presence of unmeasured determinants and residual confounding. 39 Crucial variables such as psychosocial stress, job burnout, sleep quality, detailed ergonomic exposures, and prior injury history were not incorporated into the analytical models. The critical importance of these unmeasured variables is highlighted by Khoshakhlagh et al. (2024), who demonstrated through structural equation modeling that occupational stress significantly impacts musculoskeletal symptoms in firefighters indirectly through depression and job burnout, with depersonalization acting as the strongest mediator. 9 Furthermore, Tinsley Kubala et al. (2025) emphasized in their systematic review that a biopsychosocial approach integrating physical demands with psychological stress and social support is essential for understanding MSDs in firefighters. Future longitudinal studies with more comprehensive exposure assessments that incorporate the “work exposome” concept (Descatha et al., 2025) are warranted to address these limitations, account for the HWSE, and establish the temporal sequence of the observed associations.11,46
Conclusion
This study demonstrated that the work ability of Turkish firefighters is generally at a good level, but that age is the most critical independent determinant of this ability. The high prevalence of MSDs and chronic diseases are significant risk factors for the long-term health of the workforce.
In light of the present findings, several recommendations are proposed to inform and enhance occupational health policies targeting the firefighting profession. First, the implementation of mandatory, age-specific health monitoring programs for firefighters aged 40 and above is warranted. These programs should include regular assessments of work ability through the WAI and objective physical fitness testing to detect early signs of functional decline. Second, tailored ergonomic and physical training interventions should be incorporated into routine professional development, with an emphasis on proper lifting techniques and body mechanics to prevent musculoskeletal disorders, particularly in the lower back and neck. Third, multidisciplinary chronic disease management strategies integrating medical, physiotherapeutic, and nutritional support should be developed to maintain work ability in firefighters diagnosed with chronic conditions. Finally, future longitudinal research is essential to disentangle the temporal effects of aging and cumulative occupational exposure on work ability and to rigorously evaluate the long-term efficacy of targeted interventions in sustaining firefighters’ health and operational performance.
Supplemental Material
sj-docx-1-wor-10.1177_10519815261457100 - Supplemental material for The work ability Index and musculoskeletal disorders in Turkish Firefighters: A cross-sectional study on occupational health determinants
Supplemental material, sj-docx-1-wor-10.1177_10519815261457100 for The work ability Index and musculoskeletal disorders in Turkish Firefighters: A cross-sectional study on occupational health determinants by Nuray Demiralp, Ayşe Ütük, Kemal Demiralp, Büşra Umay and Hürmüz Koç in WORK
Footnotes
Acknowledgements
The author would like to thank all the firefighters who participated in this study for their time and cooperation. Special thanks are also extended to the relevant municipal fire departments for their support during the data collection process.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and was formally approved by the Ethics Committee for Social and Human Sciences Research at Kastamonu University (Approval Date: March 29, 2023; Meeting/Decision No: 2023/10-4).
Informed consent
Written informed consent was obtained from all individual participants included in the study. All participants were briefed on the study's objectives and their right to withdraw at any stage prior to data collection.
Author contributions
Dr Demiralp, Dr Ütük, Kemal Demiralp contributed to study design, data collection, and manuscript revision. Dr Demiralp and Büşra Umay performed the data analysis and wrote the first draft. Dr Demiralp and Dr Koç provided methodological and statistical guidance. All authors contributed to editing and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available on request from the corresponding author (Nuray Demiralp). The data are not publicly available due to privacy restrictions (e.g., containing information that could compromise the confidentiality and identification of the participating firefighters and the relevant municipal fire departments).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.