
Abstract
Background
Dentistry involves prolonged static postures and repetitive movements that place significant strain on the musculoskeletal system, potentially leading to postural alterations, impaired trunk position sense, and increased pain.
Objective
This study aimed to evaluate spinal posture, trunk position sense, and pain levels in dentists and compare them with healthy individuals.
Methods
A total of 36 dentists and 36 age- and sex-matched healthy controls were included. Participants’ pain levels were assessed using the Visual Analog Scale (VAS), sleep quality using the Pittsburgh Sleep Quality Index (PSQI), physical activity levels using the International Physical Activity Questionnaire – Short Form (IPAQ-SF), and quality of life using the Nottingham Health Profile (NHP). Trunk position sense, thoracic kyphosis and lumbar lordosis angles, and core muscle endurance were assessed. Group comparisons were conducted using the Mann-Whitney U test, and statistical significance was set at p < 0.05.
Results
A total of 36 dentists (median age: 29 years; 77.8% female) and 36 age- and sex-matched healthy controls (median age: 29 years; 75% female) were included. Dentists demonstrated significantly lower physical activity levels compared to controls (p < 0.001). Additionally, lumbar lordosis angle (p = 0.003) and core muscle endurance (p = 0.009) were lower in dentists than in controls. Pain levels were higher in dentists both at rest and during activity.
Conclusion
Low physical activity, decreased core muscle endurance, and reduced lumbar lordosis may be associated with increased pain in dentists. Preventive physiotherapy interventions and regular exercise programs are recommended to reduce musculoskeletal complaints in this population.
Keywords
Introduction
Dentistry is a profession that requires prolonged static postures and repetitive fine motor movements, which can negatively affect the musculoskeletal system. Several studies have reported that dentists exhibit poorer spinal posture, trunk position sense, and higher pain levels compared to healthy individuals due to the postural risks associated with their profession.1,2
According to the American Dental Association, at least one in five dentists experiences musculoskeletal disorders (MSDs). 3 Dentists often work in narrow and visually restricted areas while maintaining static positions for prolonged periods. Even in the optimal working position, more than 50 muscles must remain active to stabilize the body, leading to long-term, repetitive muscle contractions and muscle imbalances. 4 The fixed position of the neck and shoulders may also contribute to the development of musculoskeletal disorders (MSDs). In general, workers must maintain balance in the shoulder–neck region during controlled movements of the upper limbs, requiring continuous muscle contraction to sustain a stable posture for the duration of the task. These prolonged contractions can compress nearby blood vessels, reduce blood flow, and ultimately cause discomfort and pain. 5 In particular, neck-tilt rotation, forward bending with loss of cervical and lumbar lordosis, and raised arms working in prolonged static isometric/eccentric contractions are the primary risk factors for musculoskeletal pain. 6
Postural disorders are frequently observed in dentists. During patient treatment, the trunk flexes, the head extends forward, the neck undergoes excessive flexion, and the shoulders round forward. Particularly, the upper cervical muscles (superior fibers of the trapezius, levator scapulae) increase the load on the spinal vertebrae. 7 When a dentist leans toward a patient, cervical and lumbar lordosis flatten. Reduced lumbar lordosis and weakened core muscle endurance can contribute to increased pain levels in dentists. 1
Low postural awareness among dentists is another factor exacerbating these adverse effects. Hayes et al. (2022) reported significantly higher pain and discomfort levels in dentists with low postural awareness. 2 Similarly, Günaydın (2025) highlighted that posture habits and awareness levels affect spinal pain and functional status among medical residents, suggesting that these findings may also apply to dentists. 8
Lumbar lordosis reduction and decreased core muscle endurance are particularly associated with increased pain levels in dentists. For example, Al-Ali et al. (2021) found that musculoskeletal complaints in dentists primarily involved the lower back, neck, and shoulders, mainly due to prolonged static postures. 1
Sleep quality is another important factor affecting dentists’ overall health. Long working hours and high workload may negatively impact sleep patterns. Al-Ali et al. (2021) reported that dentists had poor sleep quality, which was associated with pain and fatigue levels. 1 Similarly, Özkal Eminoğlu et al. (2025) indicated that reduced sleep quality in dentists was linked to overall health status. Poor sleep quality can adversely affect musculoskeletal health and general quality of life. 9
Pain levels directly impact dentists’ professional quality of life and work efficiency. Musculoskeletal pain, particularly in the lower back, neck, and shoulders, can reduce long-term occupational performance.2,10 Therefore, assessing pain and developing preventive strategies are essential.
Despite extensive research on occupational musculoskeletal disorders in dentistry, most studies have focused on isolated outcomes such as pain prevalence or ergonomic posture. Few investigations have simultaneously examined physical activity levels, spinal curvature parameters, and core muscle endurance within a unified comparative framework. This multidimensional approach addresses an important gap by integrating functional, postural, and behavioral factors that may collectively influence occupational musculoskeletal health.
The aim of this study is to evaluate spinal posture, trunk position sense, pain levels, and sleep quality in dentists and compare them with healthy individuals. The findings are expected to identify occupational risks among dentists and contribute to the development of preventive physiotherapy and rehabilitation programs.
Materials and methods
Study design
This study was conducted as a cross-sectional descriptive investigation to evaluate spinal posture, trunk position sense, pain levels, and sleep quality in dentists. The study did not involve an experimental or randomized controlled design.
Participants
The study included 36 dentists working at Necmettin Erbakan University Faculty of Dentistry and an age- and sex-matched healthy control group (n = 36). Dentists were recruited using convenience sampling from the faculty, while controls were recruited from the same community and matched by age and sex. The final analyzed sample consisted of participants aged 21–36 years. All participants provided written informed consent prior to participation. As the sample was recruited from a single institutional setting, the findings may primarily reflect the characteristics of dentists within this context.
Inclusion and exclusion criteria
Eligibility criteria included individuals aged between 18 and 65 years who provided written informed consent and had no history of serious neurological or orthopedic disorders.
Exclusion criteria for dentists included a history of spinal surgery, locomotor disorders (fractures or prostheses) and/or osteoporosis, traumatic orthopedic problems (acute back or nerve issues), inflammatory rheumatic diseases (e.g., ankylosing spondylitis), congenital spinal disorders (scoliosis or hemivertebra), regular exercise, and kyphosis angle greater than 50°. Exclusion criteria for the control group included musculoskeletal, neurological, or rheumatologic disorders, conditions preventing assessment (advanced respiratory or orthopedic issues, fractures, sprains, spinal surgery), regular exercise, refusal to participate, and presence of chronic pain.11–14 Although the eligibility age range was 18–65 years, the final analyzed sample consisted of participants aged 21–36 years.
Data collection procedures and tools
All interviews and physical assessments were conducted face-to-face by a licensed physiotherapist with clinical experience in musculoskeletal assessment. The assessor was trained in the standardized administration of all measurement tools prior to data collection. To ensure consistency, the same evaluator performed all measurements for both groups. A structured sociodemographic data form, developed by the researchers based on relevant literature, was used to collect demographic information (e.g., age, sex, height, weight, BMI).
Pain was assessed using the Visual Analog Scale (VAS). 15 Participants marked their pain on a 10-cm horizontal line, with “0” indicating no pain and “10” indicating unbearable pain. Separate markings were made for pain at rest and during activity. Measurements were recorded in centimeters using a ruler. Fatigue levels were similarly recorded using the VAS.
Sleep quality was assessed with the Pittsburgh Sleep Quality Index (PSQI), a valid and reliable self-report questionnaire measuring sleep quality over the past month. 16 The PSQI scores range from 0 to 21, with higher scores indicating poorer sleep quality. Median and interquartile range (IQR) values of PSQI scores were reported for dentists and controls.
Quality of life was assessed using the Nottingham Health Profile (NHP), a reliable and valid self-report measure of physical, psychological, and social health. The NHP consists of six subscales: energy, pain, emotional reactions, sleep, social isolation, and physical mobility. Scores range from 0 to 100, with higher scores indicating lower quality of life. 17
Physical activity levels were evaluated using the International Physical Activity Questionnaire – Short Form (IPAQ). Participants reported their physical activity over the past seven days, including vigorous and moderate exercise and walking. Activity levels were calculated using the MET method, with reliability and validity of the Turkish version previously established.18,19
Trunk position sense was evaluated using the trunk repositioning error test, which provides a reliable and valid measure of proprioception. 20 Measurements were performed using a Dualer IQ digital inclinometer with primary and secondary sensors. Tests were conducted in three conditions: eyes open–firm surface, eyes closed–firm surface, and eyes open–soft surface, at lumbosacral and thoracosacral regions. Participants performed a 30° trunk flexion, then attempted to return to the neutral position. The difference between the actual angle and 30° was recorded as the repositioning error, and the average of five repetitions was used.
Spinal curvature was assessed at the thoracic and lumbar regions using the Dualer IQ digital inclinometer. Participants were instructed to sway their arms forward and backward to find a natural position before measurement. Thoracic curvature was measured using C7 and sacrum as reference points for T1–T2 and T12–L1 levels, while lumbar curvature was measured using sacrum and iliac crest as references for T12–L1 and L5–S1 levels. The mean of three successful measurements was recorded 21
Core muscle endurance was measured using a stabilization pressure biofeedback device. Participants lay supine with knees flexed and head turned to one side, with the pressure cell placed under the lumbar vertebrae. The manometer was inflated to 40 mmHg, and participants were instructed to draw in the abdominal wall and maintain pressure. Duration of maintained pressure was recorded in seconds, and the mean of three trials was calculated. 22
Statistical analysis
A priori power analysis was conducted using G*Power 3.1.9.7 for a two-group comparison (two-tailed) with a significance level of α = 0.05. Assuming a large effect size (Cohen's d = 0.80), 36 participants were planned for inclusion in each group to ensure adequate statistical power and to account for potential participant loss. With a total sample size of 72 participants, the study achieved an estimated statistical power of approximately 92%.
Data were analyzed using SPSS for Windows, version 21.0 (IBM Corp., Armonk, NY, USA). The normality of the data was assessed using the Kolmogorov–Smirnov test. Normally distributed data are presented as mean ± standard deviation (SD), whereas non-normally distributed data are presented as median and interquartile range (IQR 25/75). Categorical variables are expressed as frequency and percentage (%).
Because group comparisons were conducted using non-parametric methods when the normality assumption was not met (Mann–Whitney U test), homogeneity of variance was not additionally evaluated. For comparisons between groups, the Mann–Whitney U test was used for non-normally distributed continuous variables, and the Chi-square test was used for categorical variables. Correlation analyses were performed using Pearson or Spearman correlation tests, depending on the data distribution. A p-value <0.05 was considered statistically significant.
Results
A total of 72 participants were included in the study, comprising 36 dentists and 36 healthy controls. The descriptive characteristics of the participants are presented in Table 1. No statistically significant differences were observed between dentists and the control group in terms of age, sex, and body mass index (BMI) (p > 0.05).
Descriptive characteristics of the participants.
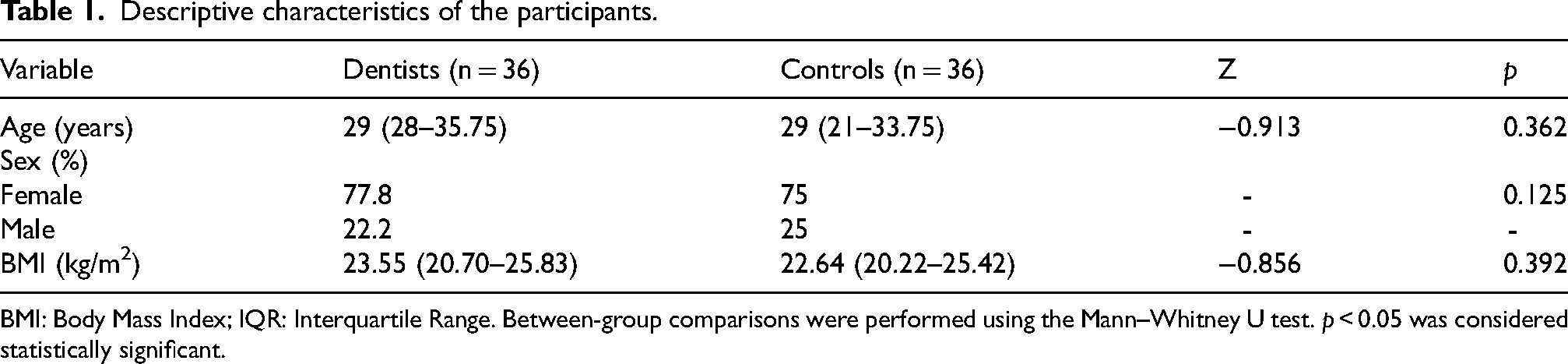
BMI: Body Mass Index; IQR: Interquartile Range. Between-group comparisons were performed using the Mann–Whitney U test. p < 0.05 was considered statistically significant.
Comparisons of pain, fatigue, sleep quality, quality of life, and physical activity levels between groups are presented in Table 2. Median pain scores at rest and during activity were 3 for dentists. No significant differences were found between dentists and the control group in terms of fatigue and sleep quality (p > 0.05). However, physical activity levels were significantly lower in dentists compared to controls (p < 0.001).
Comparison of pain, fatigue, sleep quality, quality of life, and physical activity levels between groups.
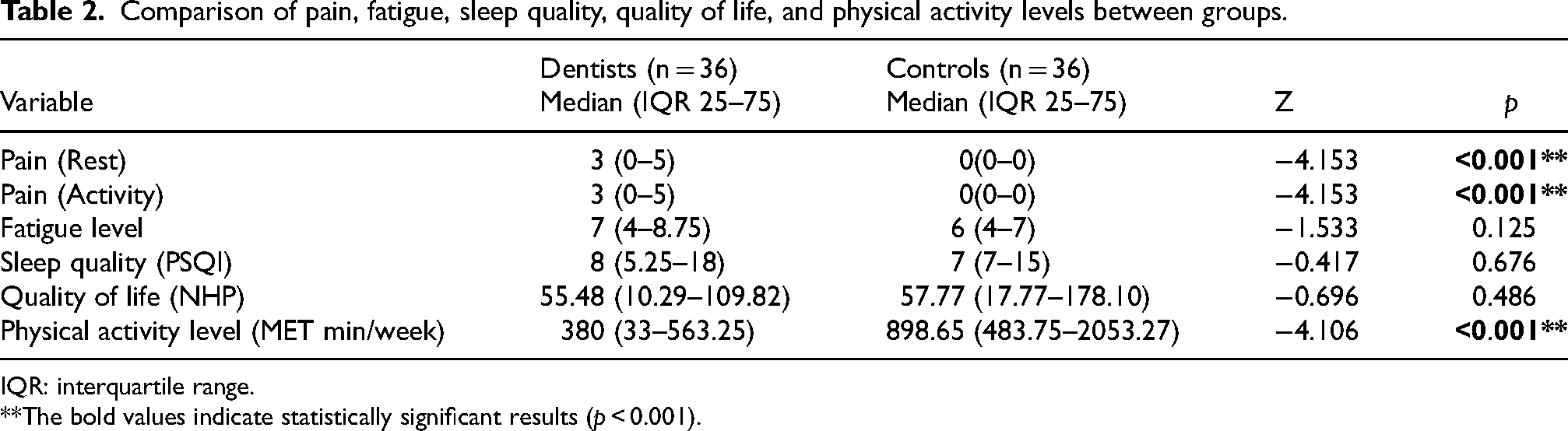
IQR: interquartile range.
**The bold values indicate statistically significant results (p < 0.001).
Comparisons of trunk position sense, spinal curvatures, and core muscle endurance between groups are shown in Table 3. No significant differences were observed between groups for trunk position sense and thoracic kyphosis (p > 0.05). Dentists had significantly lower lumbar lordosis angles and core muscle endurance values compared to the control group (p < 0.01), indicating potential adverse effects on posture and muscle endurance in dentists.
Comparison of trunk position sense, spinal curvatures, and core muscle endurance between groups.
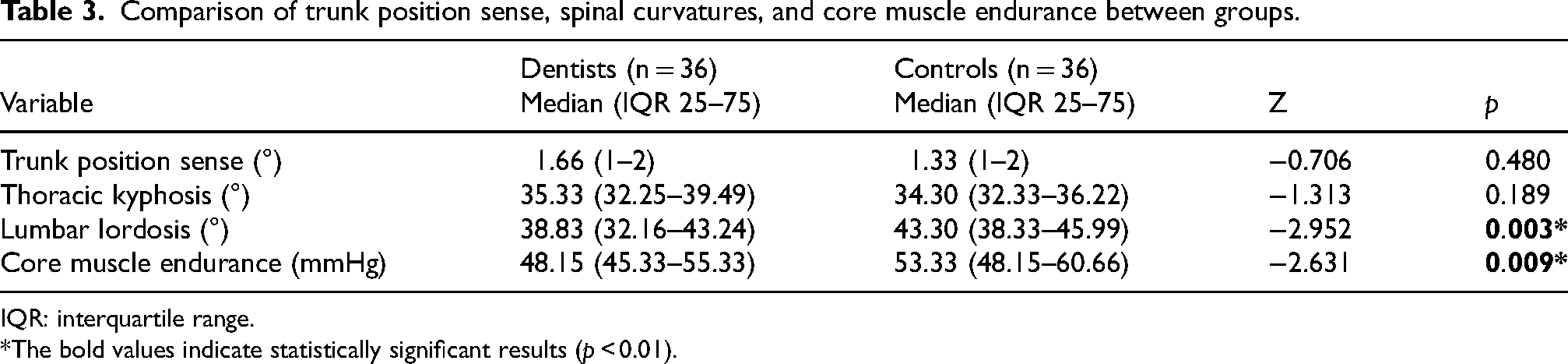
IQR: interquartile range.
*The bold values indicate statistically significant results (p < 0.01).
Discussion
In this study, the spinal posture, trunk position sense, pain level, sleep quality, quality of life, and physical activity levels of dentists were compared with those of a healthy control group.
Several studies have investigated the musculoskeletal health of dental professionals. 23 Other research has examined the prevalence of physical activity (PA) in the general population and among various healthcare professionals, including physicians, physiotherapists, and medical students. However, research specifically addressing PA levels among dental professionals remains limited. 24
Therefore, this cross-sectional study evaluates the prevalence of musculoskeletal disorders (MSDs) and PA levels in Turkish dentists. It also examines spinal posture, trunk position sense, pain intensity, sleep quality, and quality of life, and compares these outcomes with those of a healthy control group.
The findings indicated that dentists had significantly reduced lumbar lordosis angles and lower core muscle endurance. Additionally, physical activity levels were markedly lower compared to healthy individuals. These results suggest that occupational activities of dentists may increase musculoskeletal load and contribute to postural impairments.1,2,9
In this study, the control group was composed of individuals without back pain, independent of occupational workload. This selection allowed for a clear comparison between dentists, who are exposed to prolonged static postures and repetitive movements, and healthy controls, isolating the effects of professional activity on spinal posture, core muscle endurance, and pain levels.
By including only pain-free controls, the study aimed to specifically examine how the occupational demands of dentistry contribute to musculoskeletal symptoms, without confounding factors from pre-existing pain. This approach ensures that differences observed between groups are more likely attributable to occupational exposure rather than general population variability in pain experiences.
However, it should be noted that selecting entirely pain-free controls may not fully represent the general population, where occasional low back pain is common. Future studies could include control participants with minor or transient back pain to better reflect real-world variability while still examining occupational effects.
Regarding pain levels, dentists reported moderate pain at rest and during activity. This finding aligns with the increased risk of pain associated with repetitive movements and prolonged static postures during professional practice9,12,25 Moreover, the relationship between decreased lumbar lordosis, low core muscle endurance, and pain is supported in the literature. 26
Fatigue levels in dentists did not differ significantly from the healthy control group. This suggests that despite long working hours and static postures, dentists’ perception of daily fatigue is not markedly higher than that of controls. Similarly, Ayers et al. (2009) reported that subjective fatigue scores in dentists were not significantly different from the general population. 27 However, prolonged occupational load and musculoskeletal disorders may increase fatigue over time; thus, longitudinal studies are recommended to monitor fatigue levels in the future.
Although no statistically significant differences were observed in sleep quality between dentists and healthy individuals, median PSQI scores were higher among dentists. Al-Ali et al. (2021) and Özkal Eminoğlu et al. (2025) reported associations between poor sleep quality, occupational stress, and pain levels in dentists.1,9 This highlights the potential impact of sleep quality on overall health and work efficiency among dentists.
Evaluation of quality of life using the Nottingham Health Profile revealed that dentists had higher median scores compared to healthy controls, though the difference was not statistically significant. This finding indicates that while pain and postural disorders may affect quality of life, adaptive mechanisms and professional experience could mitigate these effects. 17
The low physical activity levels observed in dentists may negatively affect musculoskeletal health and overall quality of life. According to the Turkish adaptation of the IPAQ, insufficient physical activity, particularly associated with prolonged sitting and static postures, may contribute to increased back and neck pain among dentists. 19
Eminoğlu et al. (2025) reported in their study of dentists that only 10.3% of dentists were physically highly active and 93.1% of dentists had pain complaints. 9 Similarly, in another study by Kandemir and colleagues, 28 the authors found that the prevalence of MSDs among dentists was 82%. In studies by Nokhostin and Zafarmand 29 and Gopinath and colleagues 30 found that 67.5% and 73.9% of dentists, respectively, had musculoskeletal problems. In a study investigating the prevalence of work-related musculoskeletal pain among dentists in Slovenia, it was found that the majority of participants suffered from pain. 31 Our study supports this finding and found that dentists with pain were physically inactive (<0.001).
Trunk position sense is a key factor directly influencing postural awareness and balance. In this study, dentists exhibited slightly higher trunk repositioning errors than the control group, though the difference was not statistically significant. This suggests that despite occupational loading, trunk position sense is largely preserved during short-term static postures. The young age of participants (mean age 29) may have contributed to the low error rates. The literature indicates that prolonged occupational postural loading can impair proprioceptive function and increase pain risk associated with spinal loading.17,32 Continuous activation of thoracic and lumbar muscles may lead to small but repeated repositioning errors over time, potentially causing muscular imbalances and pain. Therefore, exercise and training programs aimed at improving postural awareness could help preserve trunk position sense and support long-term musculoskeletal health in dentists.
The reduction in lumbar lordosis among dentists increases spinal load, particularly during prolonged forward-leaning postures. Letafatkar et al. (2020) demonstrated that trunk exercises improved posture and muscle endurance in dentists with chronic neck pain. This finding underscores the association between postural impairments, decreased muscle endurance, and occupational risk in dentists. 33
Reduced core muscle endurance diminishes spinal stability and predisposes individuals to lower back pain. Ambegaonkar et al. (2014) noted that low core muscle endurance is associated with imbalance and restricted movement. 22 Similarly, in the present study, dentists exhibited significantly lower core muscle endurance compared to controls, highlighting the long-term physiological effects of occupational postures.
In addition, working conditions in dental practice have undergone substantial changes during and after the COVID-19 pandemic. Increased use of personal protective equipment, longer procedural times, heightened infection control measures, and altered patient flow may have further influenced postural load, fatigue, and occupational stress in dentists. Recent studies have reported increased musculoskeletal complaints and elevated physical strain among healthcare professionals during the pandemic period. Therefore, re-evaluating modifiable occupational risk factors such as physical activity, spinal posture, and core muscle endurance remains particularly relevant in the post-pandemic context. 34
Although the findings indicate reduced lumbar lordosis and lower core endurance in dentists, alternative explanations should be considered. Factors such as years of professional experience, daily working hours, ergonomic training background, and individual exercise habits may act as potential confounding variables influencing musculoskeletal outcomes. Moreover, given the cross-sectional design, the observed associations cannot determine whether reduced physical activity leads to postural alterations or whether existing musculoskeletal discomfort results in decreased activity levels. Therefore, longitudinal studies are needed to clarify temporal relationships and causality.
By integrating physical activity, spinal posture parameters, and core muscle endurance within a single comparative design, this study provides a more comprehensive occupational health profile of dentists. This integrative perspective extends existing literature beyond isolated symptom reporting and contributes to a more functionally oriented understanding of occupational musculoskeletal risk.
Previous studies published in WORK have primarily examined musculoskeletal complaints, ergonomic risk factors, or physical activity levels in healthcare professionals and dentists separately.9,10,35 While these studies provide valuable insights into occupational musculoskeletal burden, they generally focus on single-domain outcomes. The present study extends this body of literature by integrating spinal curvature parameters, trunk position sense, physical activity levels, and core muscle endurance within a single comparative framework. This multidimensional assessment provides a broader occupational health perspective that complements and expands prior findings reported in WORK.
From an occupational health perspective, these findings emphasize the need for structured workplace interventions targeting posture correction, core muscle strengthening, and ergonomic risk reduction in dental practice settings. Implementing regular workplace exercise programs, ergonomic training modules, and periodic musculoskeletal screening protocols may help mitigate long-term occupational strain. Furthermore, integrating preventive physiotherapy strategies into institutional health policies could enhance worker well-being and professional performance.
Study limitations
Finally, the limitations of this study should be considered. The research was conducted at a single university with a limited sample size. Moreover, the young mean age of participants (29 years) may limit generalizability, as the effects on trunk position sense and postural awareness could differ in older dentists. In addition, the cross-sectional design of the study precludes causal inferences between occupational exposure and musculoskeletal outcomes. Participants were recruited using convenience sampling from a single institutional setting, which may limit the representativeness of the sample. Furthermore, several variables, including pain, fatigue, sleep quality, and physical activity levels, were assessed using self-reported measures, which may be subject to recall bias or response bias.
Future studies with larger sample sizes, inclusion of older age groups, and multicenter designs may provide more reliable and generalizable data regarding postural disorders, trunk position sense, core muscle endurance, and pain management in dentists.
Conclusion
In this study, the spinal posture, trunk position sense, pain level, fatigue, sleep quality, and quality of life of dentists were compared with a healthy control group. The findings indicated that dentists had significantly lower lumbar lordosis angles and reduced core muscle endurance. This suggests that prolonged static postures and repetitive movements during professional practice may have adverse effects on the musculoskeletal system.
No significant differences were observed between dentists and healthy individuals regarding trunk position sense. However, the young mean age of participants (29 years) may have contributed to the low trunk repositioning error rates. Therefore, studies including older dentists may yield different results.
Pain and fatigue levels were mild to moderate during rest and activity. However, physical activity levels were significantly lower compared to the control group, indicating potential risks for occupational performance and long-term health. Although no significant differences were observed in sleep quality and quality of life, the heavy workload and long working hours of dentists highlight the importance of preventive measures.
Based on these results, ergonomic training programs targeting postural impairments, core and back muscle strengthening exercises, and pain management strategies are recommended for dentists. Additionally, interventions to increase physical activity and support work–life balance are important for occupational health. These findings highlight not only physiological differences but also the occupational health implications of prolonged static postures in dental practice. Addressing these risks through structured ergonomic and preventive strategies may improve long-term worker health, productivity, and professional sustainability. By offering an integrated evaluation of postural, functional, and behavioral factors in dentists, this study contributes to the occupational health literature within WORK by providing a comprehensive and clinically applicable framework for understanding musculoskeletal risk in dental practice.
Footnotes
Acknowledgements
The authors would like to thank the dentists and staff at Necmettin Erbakan University Faculty of Dentistry for their permission and support, and all participants for their contribution to the study.
Ethical approval
Ethical approval was obtained from the Necmettin Erbakan University Health Sciences Scientific Research Ethics Committee (Decision No. 22, dated 07.04.2021). Participants were provided with information about the study and written informed consent was obtained before participation.
Informed consent
The study participants were informed about the study and signed voluntary consent forms.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Confidentiality and anonymity
Any identifying information related to the authors, their institutions, funders, and approval committees has been removed to ensure anonymity and confidentiality in compliance with ethical guidelines.