
Abstract
Background
Many rural households in South Africa still experience significant challenges regarding provision of potable water even though government policy and legislative framework prioritises delivery of such infrastructure to rural households. Water collection which requires both physical effort and time, is a significant occupation in rural contexts such as in the Limpopo Province.
Objective
This paper describes the physical capacity and time demands of water collection for rural dwellers and the implications of this occupation for occupational therapist conducting Functional Capacity Evaluations (FCEs).
Methods
A descriptive single case study research methodology was utilised, and data collected during visits to rural homesteads were analysed.
Results
The findings revealed that all study participants collected water daily from sources outside of their homesteads, including taps in the adjacent streets, village water tanks or nearby rivers. The physical capacity and time required for this occupation exceeds safe limits for industrial manual handling with water collection
Conclusions
Many rural dwellers in South Africa and globally continue to need to collect water for survival and hygiene tasks. Occupational therapists conducting FCEs should consider the cumulative impact of unpaid work including water collection in rural settings when evaluating physical capacity and making recommendations regarding compensation.
Introduction
Occupational therapy encompasses the concepts of occupational performance and occupational engagement as a means of promoting health and wellbeing. 1 The focus of occupational therapy intervention is on enabling and optimising performance in all occupational areas. These include Basic Activities of Daily Living (bADL) and Instrumental Activities of Daily Living (iADL) tasks that all people engage in to care for themselves, others and their environment as part of their normal daily routine. Engagement in these tasks can be affected when an individual becomes disabled. 2 Therefore, understanding the environmental barriers that may impact the potential of individuals and communities to engage in meaningful occupations of their choice should direct context-appropriate occupational therapy assessment and intervention.3,4
South African occupational therapists working in the medico-legal field have increasingly made a particular contribution to the quantification of the consequences of disability for each claimant's unique circumstances. Functional Capacity Evaluations (FCEs) and occupational therapy reports include an assessment of the ability to carry out bADL and iADL tasks, as a prerequisite to work or generate income. 5 Comprehensive evaluations enable occupational therapists to establish the claimant's occupational performance and engagement in bADLs and iADLs. The findings should provide an accurate picture of each claimant's unique circumstances and the environment in which they live, with appropriate recommendations related to their physical capacity to independently complete these tasks with or without adjustments or accommodations.5,6
In South Africa however, there is limited evidence for assessment of the physical capacity required to execute bADLs and iADLs in rural environments where 20.2% of households still access water from outside their yards and 8.2% have no access to piped drinking water. 7 An understanding of the physical capacity required for performance of occupations unique to the rural areas such as water collection is therefore essential if appropriate recommendations for accommodations are to be made for adequate compensation.8,9 However, there is a lack of suitable bADL and iADL assessment instruments which include these elements. Consequently, occupational therapists practicing in the rural context may not have a clear understanding of environmental factors such as the rough terrain and limited infrastructure that impact on their clients’ ability to perform daily tasks. 10 The current study was conducted to investigate the physical capacity and time demands of water collection in rural South Africa with a view to providing baseline data for the development of a contextual assessment instrument for medico-legal practice.
Functional capacity evaluation (FCE) is the gold standard for measuring functional capacity to engage in occupations.5,6,11–14 Demand by the medico-legal and insurance fraternities for occupational therapy services including FCEs has increased markedly in South Africa in recent years.5,6,15 Occupational therapists practicing in this field apprise the court or the compensation authority as to the impact of injuries or illness, the extent of the impairments and their implications in terms of the person's functional ability. Evaluations of occupational performance in bADLs and iADLs form an important part of the medico-legal evaluation process to determine potential for return to work (RTW). They are of particular importance when formulating recommendations regarding the future planning for the claimant, where differentiation is required between curatorship, institutional living, supported living and independent living. 8
In order to provide assessment results that can withstand rigorous interrogation, occupational therapists in the medico-legal field make use of standardised FCE tools to evaluate the functional abilities of claimants. 5 This battery of standardised assessments provides information regarding physical capacity, including walking and manual handling tasks like the demands of their job or everyday life activities. Evaluation of the performance of manual handling tasks allows for recommendations both regarding work ability when the claimant's job entails such tasks and those required for bADLs and iADLs.5,6,16,17
Manual handling tasks
There is abundant literature pertaining to the measurement of manual handling tasks in industrial settings, particularly in the Global North (examples shown in Table 1). The normative data in the Snook Tables, the Liberty Mutual Guidelines, the Revised NIOSH Equation and the standardised FCE protocols all stipulate the conditions under which manual handling task evaluations can be performed, including the dimensions of the objects to be handled and the surfaces of the environment in which the evaluation is to take place.
Summary of studies showing manual handling weights and loads in industrial settings.
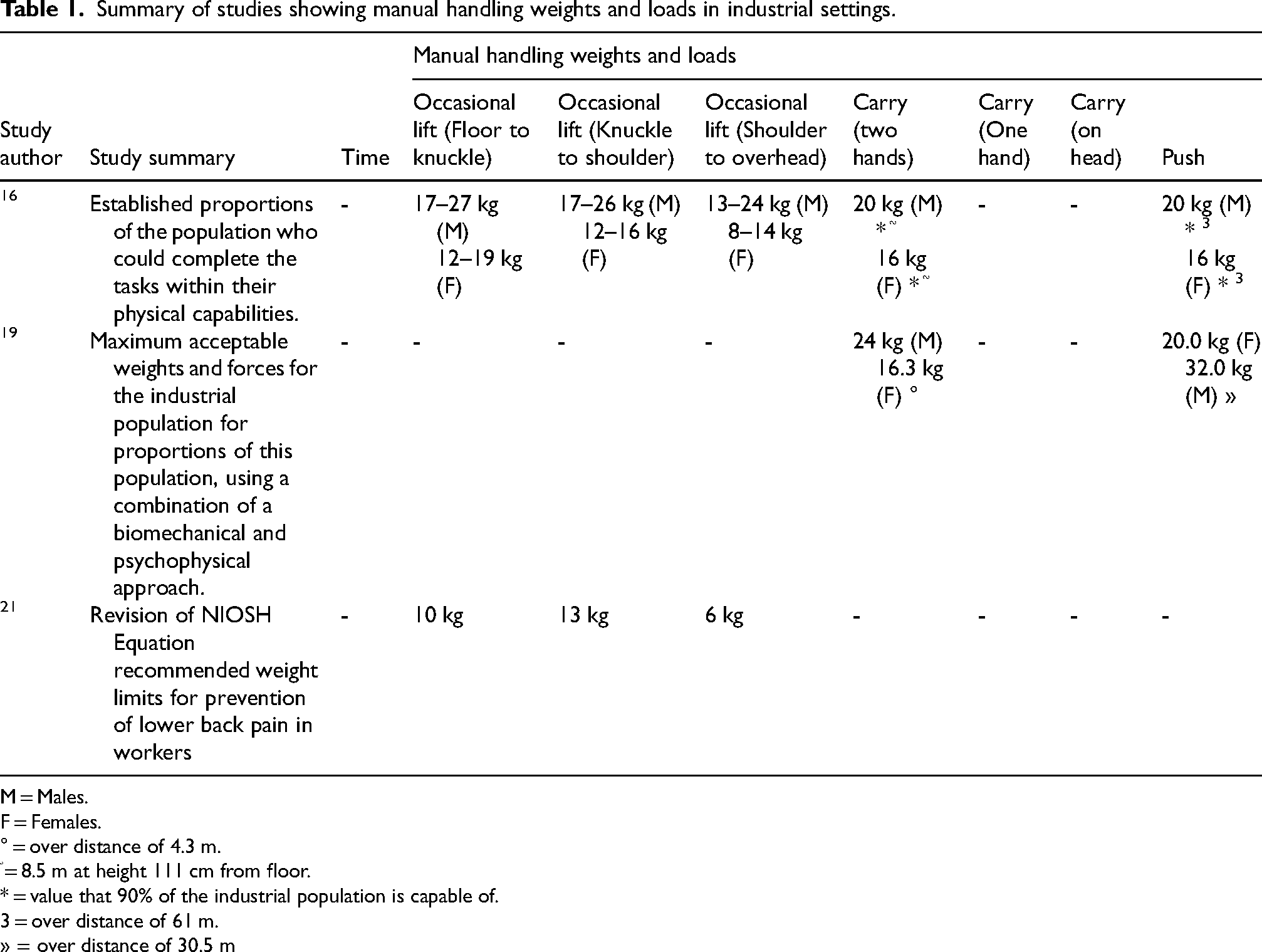
M = Males.
F = Females.
° = over distance of 4.3 m.
֘ = 8.5 m at height 111 cm from floor.
* = value that 90% of the industrial population is capable of.
= over distance of 61 m. » = over distance of 30.5 m
Historically, manual handling tasks were defined as including lifting, lowering, pushing, pulling and carrying.16,18,19 Long-term ergonomic studies were conducted to quantify the spectrum of human ability in these tasks and make the necessary adjustments to redesign everyday household and work tasks, to minimise the incidence of injury. These studies involved manual handling tasks being conducted using varying weights and frequencies, heights of lifts, carry and push distances, task duration and sizes of objects being handled.15,18,20 Several studies have been also conducted to ascertain the safe limits for manual handling in industrial settings. The best estimate of maximum weights and forces appropriate for the male and female populations in the industrial workforce are shown in the Snook Tables revised in 1991. 16 The NIOSH equations also provide guidance regarding recommended limits for lifting and were revised in 1991. 21 Furthermore, the Liberty Mutual studies provided information regarding the limitations and maximum capabilities for each manual handling task, created for industry, to minimise disability resulting from lower back injuries. 18 Most recently, the International Standards Organisation (ISO) has revised the safe limits for lifting, lowering and carrying with lower maximum load weight and carrying distance thresholds. 22
Evaluation of manual handling
The standard heights from the floor to which objects are lifted or from which they are lowered, as well as the distances over which objects are carried or pushed have been stipulated.16,18,20,21 The manual handling capacity of an individual can thus be measured in the clinic and the results compared to the percentage of the industrial population able to perform the same task as a regular part of their daily work duties.23–26
Most commercially available FCE test batteries, such as the Isernhagen Work Systems Functional Capacity Evaluation (IWS FCE Workwell System), Ergo-Kit FCE and ErgoScience, include systematic evaluation of performance of walking and all components of manual handling tasks.23,24,27 The individual's performance in lifting is classified according to the Dictionary of Occupational Titles (DOT) into physical demand categories, namely sedentary, light, medium, heavy and very heavy, based on the intensity of the lifting, carrying and pushing tasks. 17 Physical capacity performance can be extrapolated to the whole workday, demonstrating whether the individual would be able to maintain the task at the required frequency for the entire workday. 26 A lifting task performed at a frequency of less than 33% of an eight-hour workday is defined as occasional lifting, one performed for 34% to 66% is defined as frequent, whereas one performed for 67% to 100% of the workday is termed constant lifting.17,28 of all manual handling tasks, two-handed lifting has shown to have the strongest association with lower back injuries and lower back pain in industrial settings. This finding led to the development of assessment instruments, such as the Progressive Isoinertial Lifting Evaluation (PILE) and the Isoinertial Lifting Protocol, to evaluate and measure lifting ability in the clinic. The study by Lee (2005) added a detailed order of difficulty in terms of physical demand regarding different types of lifts. So-called floor to knuckle lifts from the floor to the height of the knuckles when the arms are hung loosely at the side, are the least physically demanding. Lifts become more physically demanding the higher the object must be lifted, with difficulty increasing from knuckle to shoulder to the most physically demanding shoulder to overhead lifts.16,24,25,29,30 The performance in floor to knuckle lifting has been found to be the strongest predictor of ability to complete functional activities and return to work.25,30,31
However, no physical capacity performance assessment instrument can be compared to the physical demand requirements of the individual's bADL and iADL tasks. The resultant epistemic gap can arguably contribute to inadequate or inappropriate evaluation, thereby compounding the true impact of injuries or disability on the individual's quality of life. Thus, occupational therapists have a limited appreciation of the significant manual handling demands in personal and household tasks; this is particularly relevant in the rural context, where limited infrastructure and amenities mean heavy water containers need to be carried over considerable distances.
Constraints to accessing water in rural South Africa
Against the background of limited access to potable water for billions globally, the Sustainable Development Goal 6 expresses the commitment of the United Nations to this basic human right that is essential for survival, health, hygiene and poverty reduction. 32 Despite significant improvements in water access since South Africa's first democratic elections in 1994, many rural-dwellers continue to engage in water collection from sources outside of their homes daily.33–36 The Reconstruction and Development Programme (RDP) made provision for all South Africans to have equitable, sustainable and efficient access to water for their basic needs including drinking, cooking, and personal and household hygiene. This basic water supply was defined as a minimum of 25 litres per capita per day, within 200 m from the household, at a flow rate of 10 litres per second and at a 98% level of reliability of service delivery. 37 The implementation of economic development policies showed that access to piped drinking water within homestead yards had initially almost doubled since 1996 but has subsequently declined in six provinces between 2002 and 2021 (the largest decline was observed in Limpopo Province; −4,4 percentage points). More positively many more households were provided with water in 2021 than two decades earlier. 7
Many rural communities experience the newly installed water services as unaffordable and reverted to collection of water from free sources such as rivers. Although the Free Basic Services Policy of 2000, made provision for 6 kilolitres of free municipal water per household per month 38 investment in infrastructure, maintenance backlogs have become a systemic challenge. High proportions of households in the Mpumalanga and in Limpopo Provinces remain without basic services or uninterrupted water supply. 39
Thus, the distance from water sources remains a constraint facing many rural households, affecting the quantity and quality of water accessed. Collecting water is still a common task, presenting a significant time and physical demand cost. A study in 24 Sub-Saharan African countries demonstrated that 20% to 50% of rural households spent more than 30 min per day collecting water in more than half of the countries. 40 The extent of the physical demands inherent in water collection are highlighted in studies that have shown that musculoskeletal disorders (MSDs) and physical injury are common sequelae of the poor ergonomics implicit in carrying water from a water source to the home.35,40–42
Ergonomics in rural settings
Ergonomics studies of agricultural occupations have identified numerous job components that pose high risk for development of MSDs for farmworkers, including sowing new plants, weeding, harvesting and picking, and packaging produce.43,44 Instruments such as the Rapid Entire Body Assessment (REBA), the Rapid Upper Limb Assessment (RULA) and the Agricultural Lower Limb Assessment (ALLA) have been used to investigate associated ergonomic challenges, such as stooping or bending over for extended periods, lifting and carrying heavy items, and repetitive movements in awkward postures with limited availability of suitable farming equipment and infrastructure.45–48 In some instances, study results have been utilised to inform advocacy regarding design changes for agricultural equipment. 43 While these developments continue to impact positively on policy reforms affecting formally employed farmworkers, they fall short in their application to unpaid work tasks in support of rural households, including water collection, which has similar ergonomic demands.49,50 The International Labour Organisation (ILO) acknowledges unpaid work as being a significant contributor to economies globally which disproportionately affects women and girls. 51 Similarly, the SDG 5.4 identifies water collection as a particularly gendered unpaid work task in Sub-Saharan Africa and proposes progressive provision of water infrastructure as an indicator of reducing the impact of unpaid labour in such contexts. 52 It is therefore timely to explore the ergonomic demands of unpaid labour tasks typical of resource-constrained rural settings.
This paper formed part of a larger study with the aim of developing an ADL assessment instrument relevant to individuals who live in rural resource-constrained South African contexts. The current article reports the FCE implications of manual handling in bADLs and iADLs with a view to capacitating occupational therapists to make realistic recommendations to the courts regarding reasonable accommodations, assistive devices, personal assistance and home adaptations for claimants living in rural areas.
Methods
Study design
A descriptive single case study with embedded units research methodology was utilised as it enables investigation of the real-life phenomenon of individuals in their living environment.53,54 The case was the water collection strategies of the individuals living in four villages in the Greater Tzaneen and the Maruleng sub-districts of the Mopani District in the Limpopo Province, South Africa (see Figure 1 for geographical location of the study). The area is characterised by rural villages, where many households have limited or inconsistent access to piped municipal water. The implementation of the Free Basic Water Policy is apparent in these districts, with 1295 households in Greater Tzaneen and 2 405 households in Maruleng being beneficiaries.55,56 The case was bound by definition and context, as a district associated with individuals living in resource-constrained rural area where completion of bADLs and IADLs involves manual handling tasks requiring extra effort and time. 57
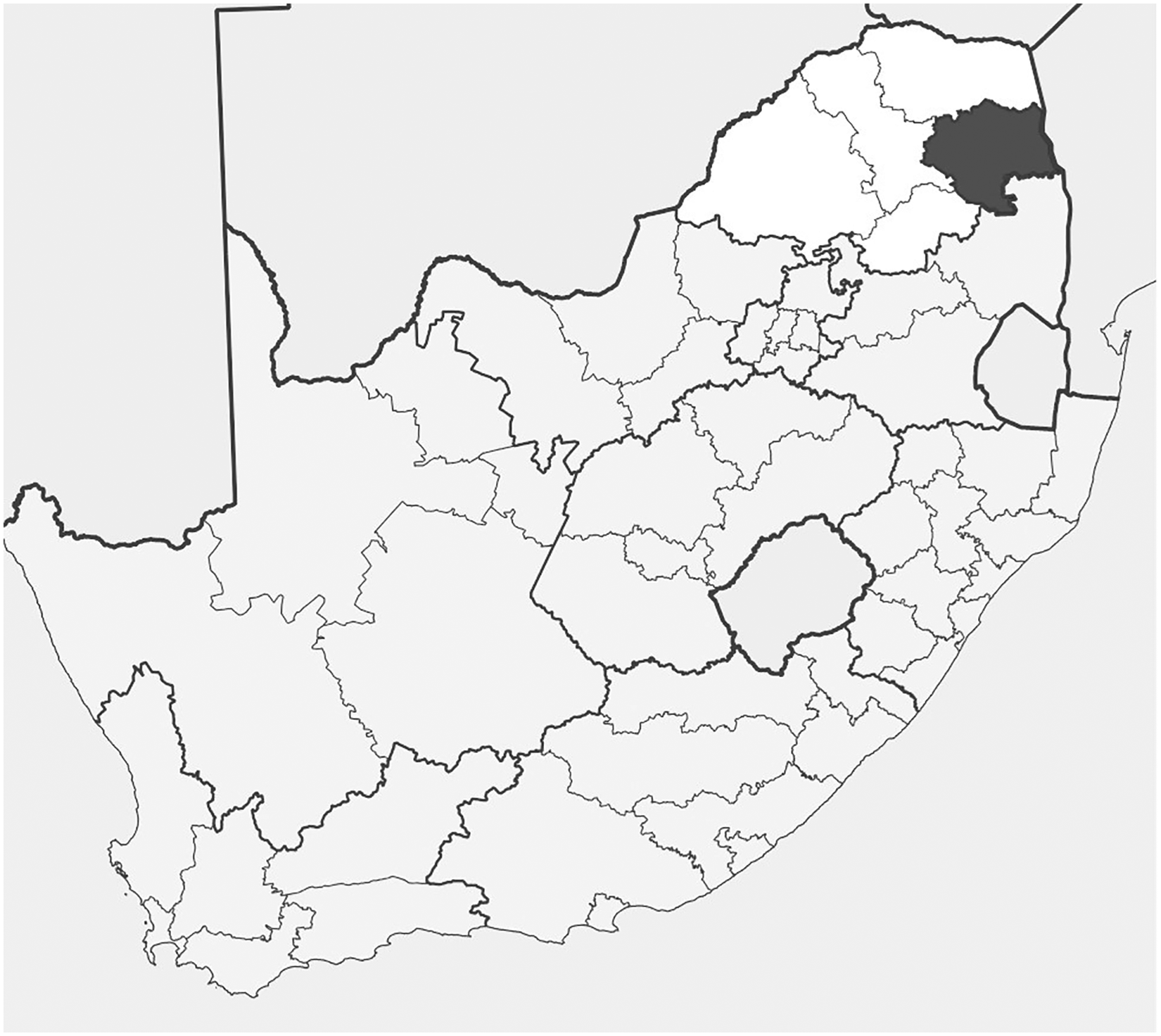
Location of research site.
Structured survey interviews about the methods and frequency of water collection were carried out during home visits. Water collection behaviour about which little is known was observed in the natural context of the participants’ homes and the frequency with which it occurs was determined. Measurements of the distances walked, weights lifted, carried and pushed, and times taken collecting water were recorded, with the observations and measurements made allowing for detailed interrogation of the household amenities.58,59
Study population and sample
Four villages in the geographical area surrounding the town of Tzaneen in Limpopo Province, South Africa were selected for the study since they typify rural, resource-constrained locations where completion of bADL and iADL tasks is associated with manual handling tasks that require effort and time. Community liaison assistants were requested to identify community members for inclusion in the study who lived in resource-constrained homesteads typical of the community and were aged between 18 years and 75 years.
Purposive convenience sampling to identify and recruit research participants according to the inclusion criteria was used. A target of 8-12 participants was set to achieve data saturation using triangulation of multiple data sources from interviews and home visits.
Research procedure
The study was approved by the Human Research Ethics Committee (Medical) of the University of the Witwatersrand (approval certificate M150925), as well as the Research Ethics Committee of the Limpopo Department of Health.
Training community liaison assistants
Community liaison assistants, who were community members, were identified and trained regarding the data collection procedure by the first author. They were selected as they were known to the first author in the community and resided in one of the four villages included in the study.
The background and purpose of the study were explained and written informed consent, including permission for photographs and videos, was obtained from participants prior to the start of each respective home visit. The information sheets provided were translated verbally into the home language of those participants with limited literacy or English language skills. The home visits took place in two different villages in each sub-district according to the protocol developed for the study. The researcher accessed the community through the community liaison assistant, and they travelled together to the identified homesteads. The community liaison assistant and the participants were invited to communicate in their home language during the home visits and the community liaison assistant assisted with translation if necessary.
Data collection
Data were collected on the biographical information sheet and survey checklist through a semi-structured interview conducted during a home visit. The biographical information sheet and survey checklist were developed by the first author, with items informed by the previous stage of the larger study, during which community care workers identified typical daily occupations through participatory mapping. 60 Member checking was completed with community care workers to ensure face validity of the survey checklist. 37 In-depth discussions were facilitated with the member of the households who was available at the time of the home visits using open-ended prompt questions to investigate the household and community amenities available for water collection. To mitigate for observer bias, the first author trained the community liaison assistants in the data collection methods and followed a set data collection format ensuring the home visits and interviews were carried out as similarly as possible. Additionally, photographic and video material allowed for automated confirmation of survey checklist data. Triangulation of data from multiple sources also contributed, with the distances walked during water collection, as well the weights lifted, carried and pushed, measured using a measuring wheel and a standard luggage scale respectively. A stopwatch was used to measure the time taken to complete water collection.
Data analysis
The biographical, home visit and measurement data were analysed using descriptive statistics, including frequencies, means and medians. The images in the photographs and videos were organised and labelled per participant and according to the nature of the material recorded. These visual records of observations were triangulated with the home visit checklist and measurement data to develop a complete home visit data set. The data were utilised to quantify the loads pushed in wheelbarrows by taking into consideration the design of a wheelbarrow, which was defined as having a Class 2 lever. The calculation of the total load being pushed required the use of a formula that included the weight of the wheelbarrow itself, the weight of the load, the type of surface on which the wheelbarrow was being pushed and the integrity of the wheel. 61
Results
Biographical information
The biographical information regarding the research participants in the four villages can be viewed in Table 2. The mean age of the participants was 55 years, with the youngest being 19 years old and the oldest being 72 years old. Most of the participants were female (n = 10).
Demographic information for home visit participants.
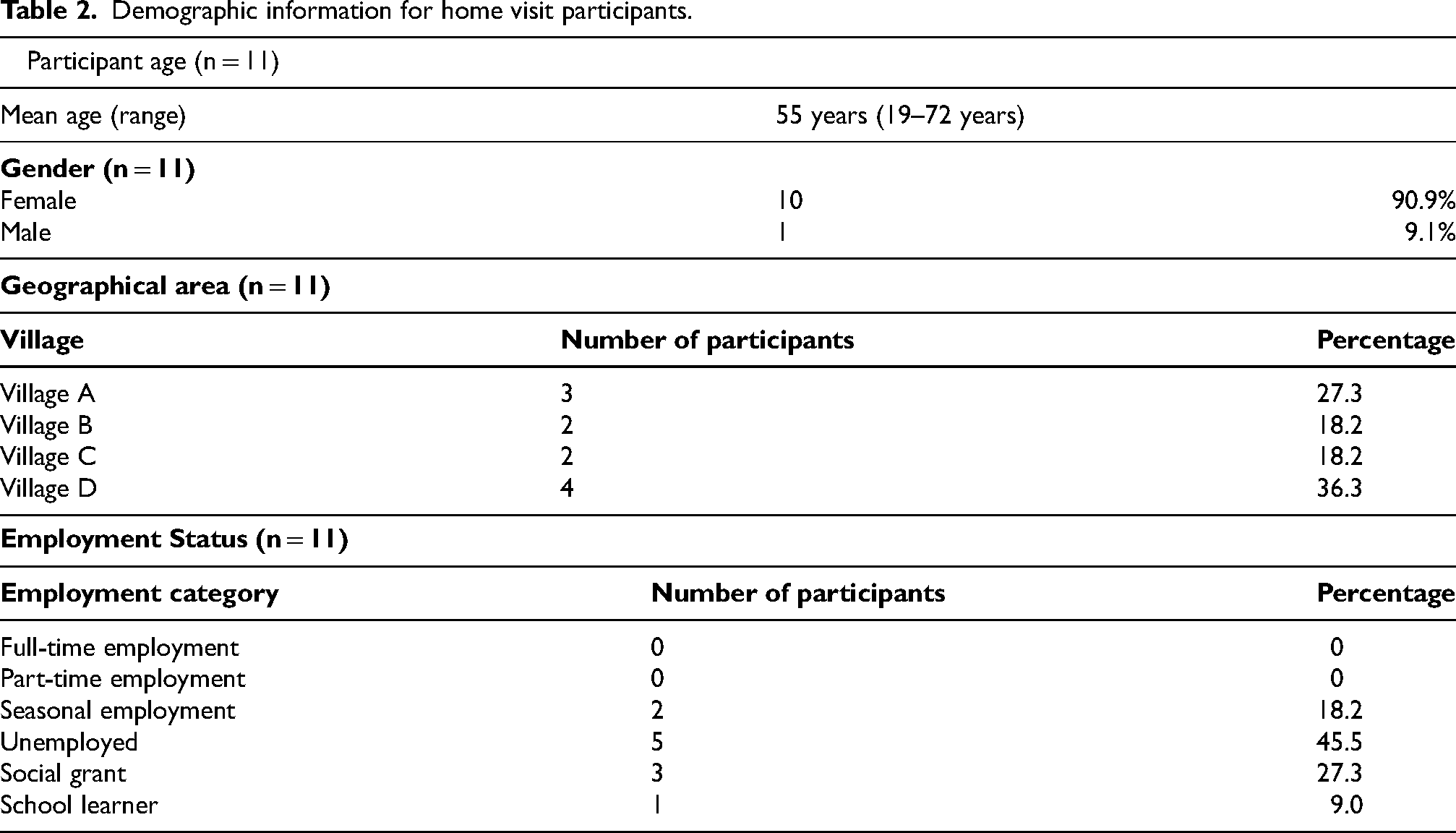
Most participants reported that they were unemployed (n = 5), while 2 participants indicated that they engaged in seasonal employment. A further 3 participants obtained income from social grants, while one participant was a school learner.
Five of the participants’ homes were in the Greater Tzaneen Municipality, with three living in village A and two living in village B respectively. The remaining six participants lived in the Maruleng Municipality, with 2 of them in village C and four of them in village D respectively. Three water sources were identified in the research sites, namely a communal tap in a nearby street, a communal tap in the village and a nearby river.
Water sources and distances walked to collect water
None of the participants were found to have indoor piped municipal water, as shown in Table 3. Two of the participants had taps within their yards but reported that there had been no water available in the municipal system for many months prior to the data collection. All 11 participants thus accessed water from a communal water source outside of their homesteads. One participant collecting water from the nearby river, two participants collected water from a municipal tap in the street near to their homes, while most of the participants (n = 8) accessed water from the sole tap in their villages.
Water collection: sources, physical capacity demands, equipment and household member.
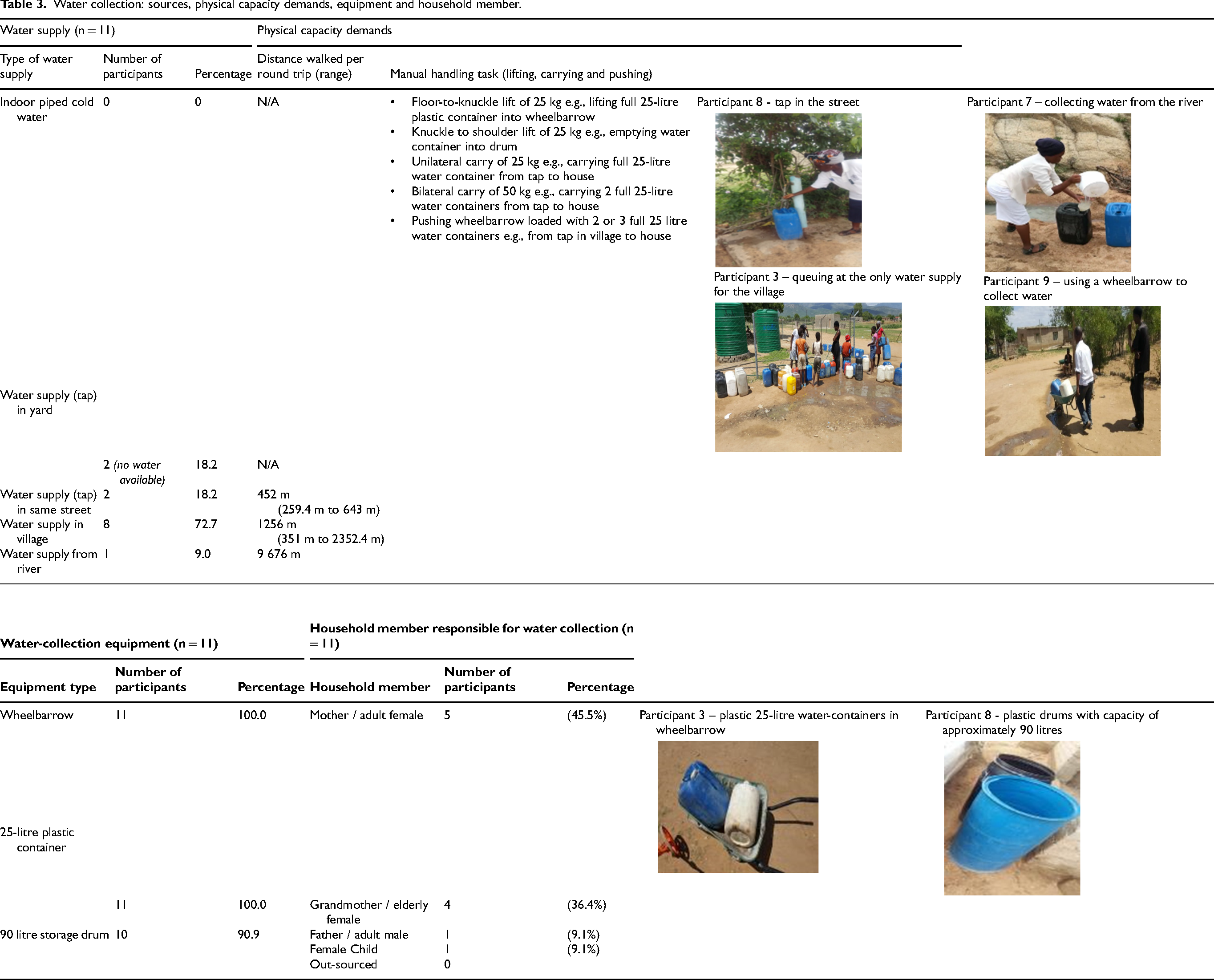
The results shown in Table 3 indicate that the participants (n = 8) were walking a median distance of 1 502 m per round trip when collecting water from the communal water source in the village. Those participants who were found to collect water from a tap in the street nearby to their homes (n = 2) walked a median distance of 452 m per round trip. The participant who collected water from the nearby river walked a distance of 9 676 m per round trip.
Equipment for collecting and storing water
Data relating to the types of equipment utilised for water collection is reflected in Table 3. All the participants (n = 11) were found to make use of 25-litre plastic containers for the collection, while most of the participants (n = 10) were found to use 90-litre plastic or metal drums for the storage of water. All participants (n = 11) were found to make use of a wheelbarrow to transport the 25-litre plastic water-containers.
The semi-structured interview, photographic and video data supported the finding that participants typically lifted full 25-litre water containers weighing 25 kg each from the ground onto wheelbarrows (floor-to-knuckle lifts) and from the wheelbarrow to the lip of storage drums when emptying collected water for storage (knuckle to shoulder lift). Some were also observed to carry one or two of these same containers over the relatively short distances, such as from a tap in the untarred street back to the homestead. The quantity of water transported by wheelbarrow per trip varied depending on the physical strength of the participant and the terrain. Most participants opted to transport two or three 25-litre plastic water-containers at a time in a wheelbarrow when accessing water from the village taps. Thus, participants were pushing between 50 and 75 kilograms of water in their wheelbarrows per trip.
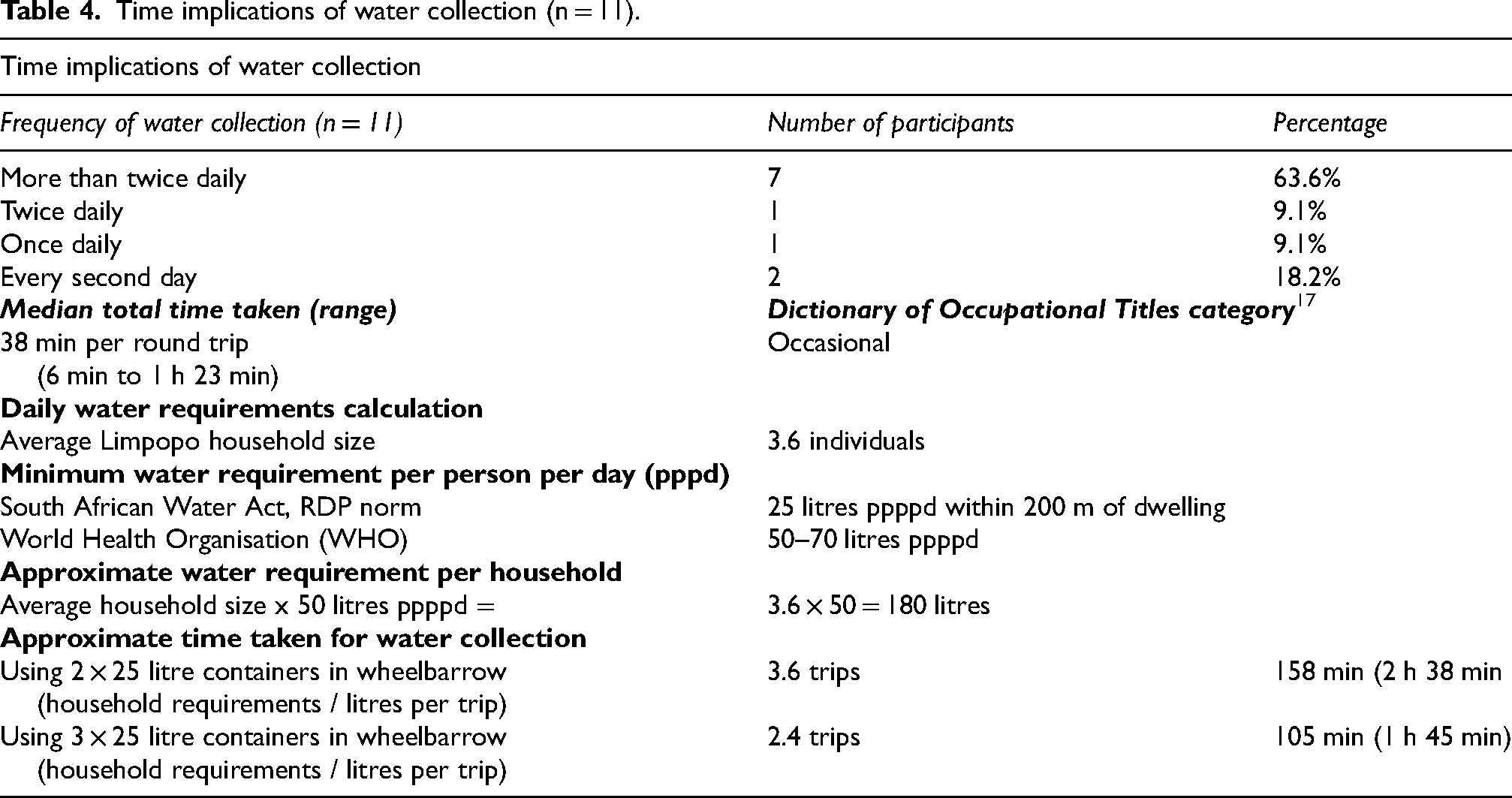
Frequency of performance, distances walked and times taken to collect water
Table 4 shows that most of the participants collect water more than twice per day (n = 7), while one participant collected water once daily or and another collected water twice per day. Collection of water was found to take a median time of 38 min per round trip. However, the measurements of the times taken for water collection were negatively impacted by the presence of the research team members; participants accompanied by research team members did not have to wait their turn and were invited to fill their water containers immediately upon reaching the communal water points.
Time implications of water collection (n = 11).
Discussion
Demographic information
The data shown in Table 3 aligns with numerous studies documenting that women are predominantly responsible for water collection in rural South Africa.42,62 The gendered performance of domestic bADLs and iADLs, including water collection, was also borne out by the 2010 time use survey, which found that South African women spent a mean of 3 h and 15 min per day on domestic tasks, which is 2.2 times longer than the mean of 1 h and 28 min spent on these tasks by their male counterparts. The same survey also showed that women are more likely to collect water, regardless of the distance of the water source from the homestead. 63 Similarly, the ILO recognises that women do approximately two and a half times more unpaid household work than their male counterparts globally, with this gap even wider in the Global South due to the additional essential tasks of sourcing household amenities like water manually. 51
Distances walked for water collection
The study findings illustrated that participants walked varying distances from their homesteads to access water daily (Table 3). When considering the finding that the distance of a one-way trip from the household to the street taps was 226 m, the RDP standard of 200 m to a water source is only slightly exceeded. 64 While this finding is somewhat less than has been reported in a previous study conducted in a different part of Limpopo Province which found that the mean distance that water was carried was 330 m, this distance is nonetheless of concern for people with mobility impairments. 36 The current study found that most households did not have street taps but rather had to use the sole village water supply. They were thus accessing water much further afield, walking median distances far more than the abovementioned RDP standard. This latter finding is supported by a study in the Mopani District, which reported that women walk distances of up to 4 kilometres to collect water for survival and domestic use. 65
Water collection method
The equipment typically used to collect water from sources outside of their homesteads provides a further indication of the physical difficulties faced by community members when collecting water. As the quantity of water transported depends on the physical strength each community member, most participants made use of wheelbarrows to transport filled water containers rather than carrying them; the fulcrum design of a wheelbarrow presumably makes pushing such heavy weights less strenuous than carrying an identical weight. The findings highlighted a significant manual handling burden associated with water collection for household members living in rural communities with limited household amenities.
Comparison of manual handling demands with industrial norms
There is a paucity of literature regarding the load-carrying of rural dwellers in the developing world.66,67 It is of importance to note that literature pertaining to the standardised tests used in South Africa for evaluation of manual handling, are based on the maximum loads and forces for industrial settings, excludes one-handed lifting and carrying, as well as pushing objects other than loaded trolleys, such as a wheelbarrow. 18 Furthermore, one-handed lifts, such as when carrying a 25-litre water container in one hand, are regarded as being the most physically demanding and are not recommended from an ergonomic perspective, as uneven spinal loading is associated with an increased risk of back injury.18,22,68 The heavy loads being lifted, carried and pushed by water collectors reported in this current study place them at risk of developing MSD symptoms and fatigue. 43
The loads carried and pushed during water collection described in this study, as shown in Table 5, exceed the maximum safe loads and forces for carrying and pushing described in the FCE literature.18,20 For example, the assessment of carrying ability in a clinical setting involves the individual carrying a maximum weight of 16 kg for females or 20 kg for males, with both hands at a height of 111 cm from the floor over a distance of 8.5 m. Similarly, evaluation of pushing ability in a clinical setting has the individual pushing a trolley with a maximum initial force of 16 kg for females and 20 kg for males over a smooth surface. 20 Furthermore, they exceed the maximum safe loads recommended by the ISO. 22
Lifting, carrying and pushing demands of water collection.
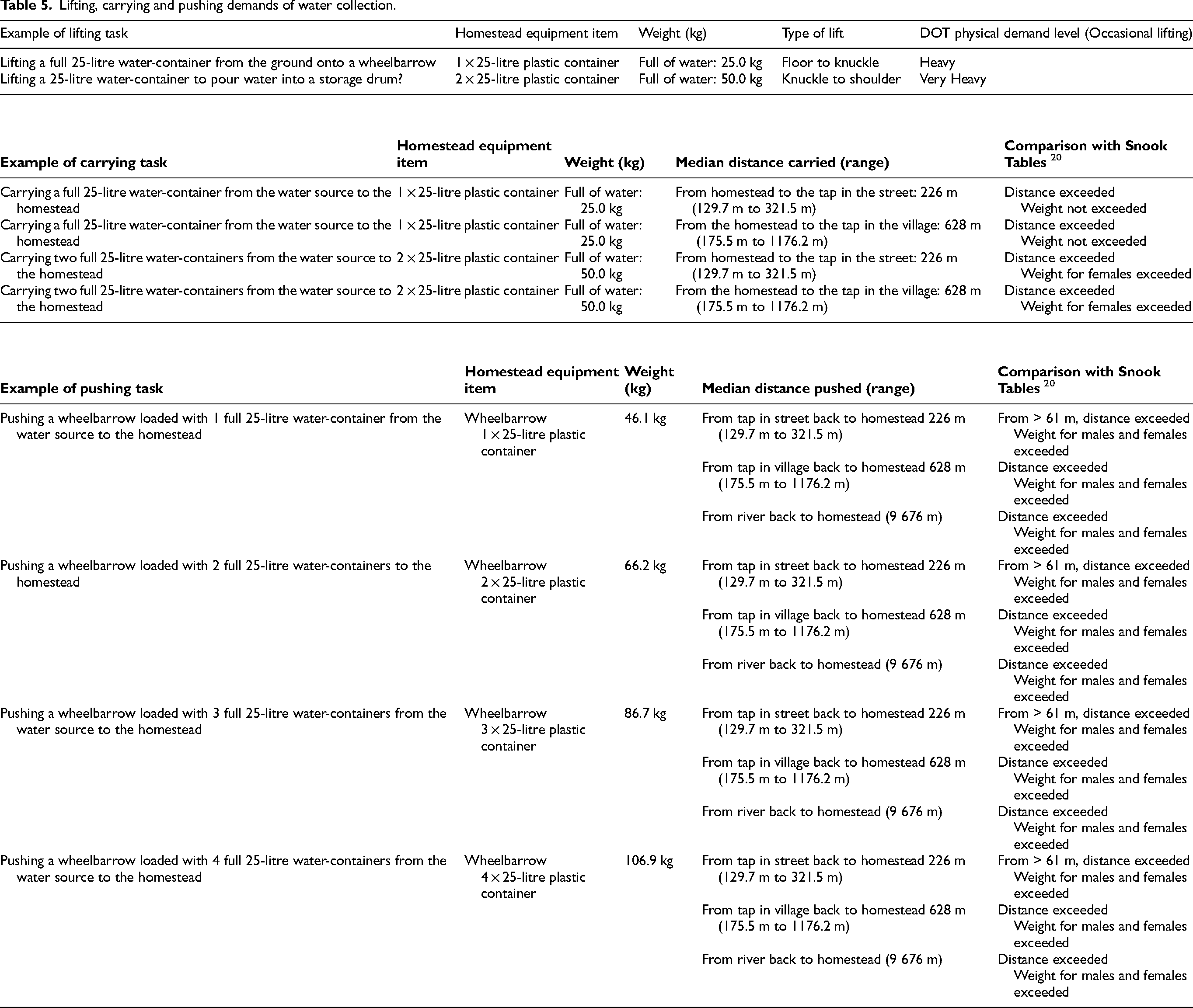
The findings in the current study are largely consistent with other studies rural Limpopo.34,42,65,70 As an alternative to using a wheelbarrow, individuals carrying heavy water containers on their heads had raised risk of developing MSDs and sustaining injury. Furthermore, the heightened risk in rural dwellers of developing MSDs associated with collecting water is supported by numerous studies carried out elsewhere in the world.36,42,63,64 The associated loads exceed capacity for adaptation or repair, leading to fatigue, accumulation of fatigue, damage or early degenerative changes to bone or soft tissue.
In industrial settings, individuals required to manoeuvre such heavy and asymmetrical loads are regarded as being at high risk for work-related injury and ergonomic adjustments to reduce the loads would be implemented.22,46 Similarly, advocacy and policy directives emerging from SDG 5.1 to implement strategies to reduce the disproportionate burden of unpaid labour on women, could drive provision of more ergonomic and accessible water services infrastructure.47,51,52 However, for occupational therapists to play a meaningful role in raising awareness and mitigating risks associated with water-collection, discourse regarding our foundational theoretical frameworks and models needs to be inclusive of occupations typical of non-Western Global South settings.8,10 The water collection occupation could align with the emerging occupational science concept of resource seeking and be defined as an iADL sub-category in the Occupational Therapy Practice Framework (OTPF IV). 69 Alternatively, if water collection is viewed primarily as unpaid work, then it could be defined as a component of work occupations.
Time implications
The findings of this current study show that most participants made multiple daily trips to collect water (Table 4). Ownership of storage drums by all participants enabled them to re-use the 25-litre plastic water containers for further trips to collect water to accumulate an adequate water supply for the needs of the household. Numerous other South African studies and reports supported the finding of multiple daily water collection trips, 63 but one study also conducted in the Mopani District found that community members mostly collected water only once daily. 70 Furthermore, numerous authors have reported that water collectors spend extensive time waiting for their turn at communal water sources.71,72 Similar long waiting times at communal water points were reported by the participants in the current study and were observed and photographed by the research team. These findings align with the Survey of Time Use of 2010 which reports that time spent on housework is significantly greater in households where water is sourced from outside of the homestead. 63
It is of value to calculate the practical time implications of these findings (Table 4). There are numerous international standards regarding the minimum daily water requirement, ranging between 25 and 75 litres per person per day. 7 Using the South African RDP standard for a basic water supply is 25 litres per person per day 37 and the average household size in Limpopo Province of 3.6 people 7 this translates into each household needing to collect at least 90 litres per day. Transporting two 25-litre water containers at a time by wheelbarrow would require four trips per day, with a total time of 152 min per day. This is similar to the mean time of 75 min per day spent on water collection from sites further than one kilometre from homesteads, as reported in the 2010 time use survey. 63 It is also similar to the finding of another study conducted in the Mopani District, which reported a mean of 76 min for daily water collection. 64 Similarly pushing three water containers at a time in a wheelbarrow would require three trips per day, with a total time of 114 min per day. The results of this current study differ from the findings of a study in Senegal, which reported that women and girls spend up to 7 h per day collecting water. 74 Similarly, a study on water collection in rural India found that individuals spent up to 6 h per day on water collection. 75
The time calculation for transportation of two 25 litre water containers at a time in the current study correlates with the mean time of 75 min per day spent on water collection from sites further than one kilometre from homesteads as reported in the 2010 time use survey. 63 It is also very similar to the finding of another study conducted in the Mopani District which reported that a mean of 76 min for daily water collection. 65 The ILO highlights water collection as a significant category of unpaid domestic work which often excludes individuals from participation in other occupations; this limits their access to employment and educational opportunities that could otherwise potentially contribute towards poverty alleviation.51,76 The limited provision of household amenities, particularly piped water, contributes to occupational injustice in rural communities. 34
Implications for medico-legal occupational therapy practice
The study findings have significant implications for occupational therapy practice in the medico-legal and other fields of practice in South Africa where services are provided to females living in rural under-resourced areas. Engagement in water collection on an ongoing basis exposes rural dwellers to MSDs secondary to poor ergonomics and significant occupational imbalance, marginalisation and deprivation ensue. For individuals formally employed, also engaging in water collection can place the cumulative daily MET level into the heavy load category which has bearing on occupational performance in employment settings. 79 While the impact of these excessive physical demands poses health risks for any rural dwellers, it is particularly significant for those who have sustained injury, illness or disability. Such individuals may no longer be able to perform ADLs necessary for survival, personal hygiene and care of home in an environment without adequate access to water. It is therefore feasible that an injury or illness may result in a greater degree of disability or participation restriction for an individual living in a rural context compared to an individual having the identical condition in a well-resourced setting. Similarly, water collection places women at additional risk of exclusion from economic and educational opportunities. 72
Medico-legal occupational therapists need to take cognisance of this for their recommendations regarding patients’ work ability to be accurate. For example, a patient presenting for a medico-legal FCE may be found capable of returning to their previous job as a domestic worker, which has a medium physical demand level according to the DOT, 17 however, if the patient resides in a rural resource-constrained context, they may be collecting water for their own family before work each day. The cumulative effect of collecting water at home over and above their normal work duties may impact negatively on occupational performance at home and work contributing to negative performance appraisal and placing them at further risk of occupational injury and promotional opportunities. By the time an employed individual gets to their workplace, having collected water in the early mornings, they have in effect already completed the equivalent of work equating to a heavy or very heavy physical demand level according to the D.O.T. 17 Contextually relevant assessment of ADLs of rural claimants by medico-legal occupational therapists can therefore be regarded as a mechanism of enhancing access to occupational rights and minimising occupational deprivation and injustice.77,78
In Western well-resourced contexts, the cumulative load of the claimant's bADL and iADL responsibilities as well as the demands of their job are taken into account by the occupational therapist. It can be advisable to advise adjustments in the home setting to minimise the demands of bADLs and iADLs on the claimant, so that their endurance at work can be optimised. In rural settings where households have limited access to amenities, this becomes far more significant. Not taking the physical demands of these tasks into account can skew the FCE results. Furthermore, the burden of care of disabled individuals in a rural context takes on a different dimension when the demands of collecting resources needed for survival are considered. The recommendations presented in Figure 2 can enhance the contextual application of FCE findings by occupational therapists. In response to the findings of the current study and the limited suitable assessment instruments, the researcher furthermore developed an ADL assessment instrument (the Rural ADL Manual Handling Sort) that takes the context of households in rural, resource-constrained areas in South Africa into account.73,79 It is envisaged that implementation of the newly developed instrument that will stand up to scrutiny in court will enable occupational therapists to minimise omissions in FCE reports regarding adaptations and compensation for bADLs and iADLs that require extensive manual handling.
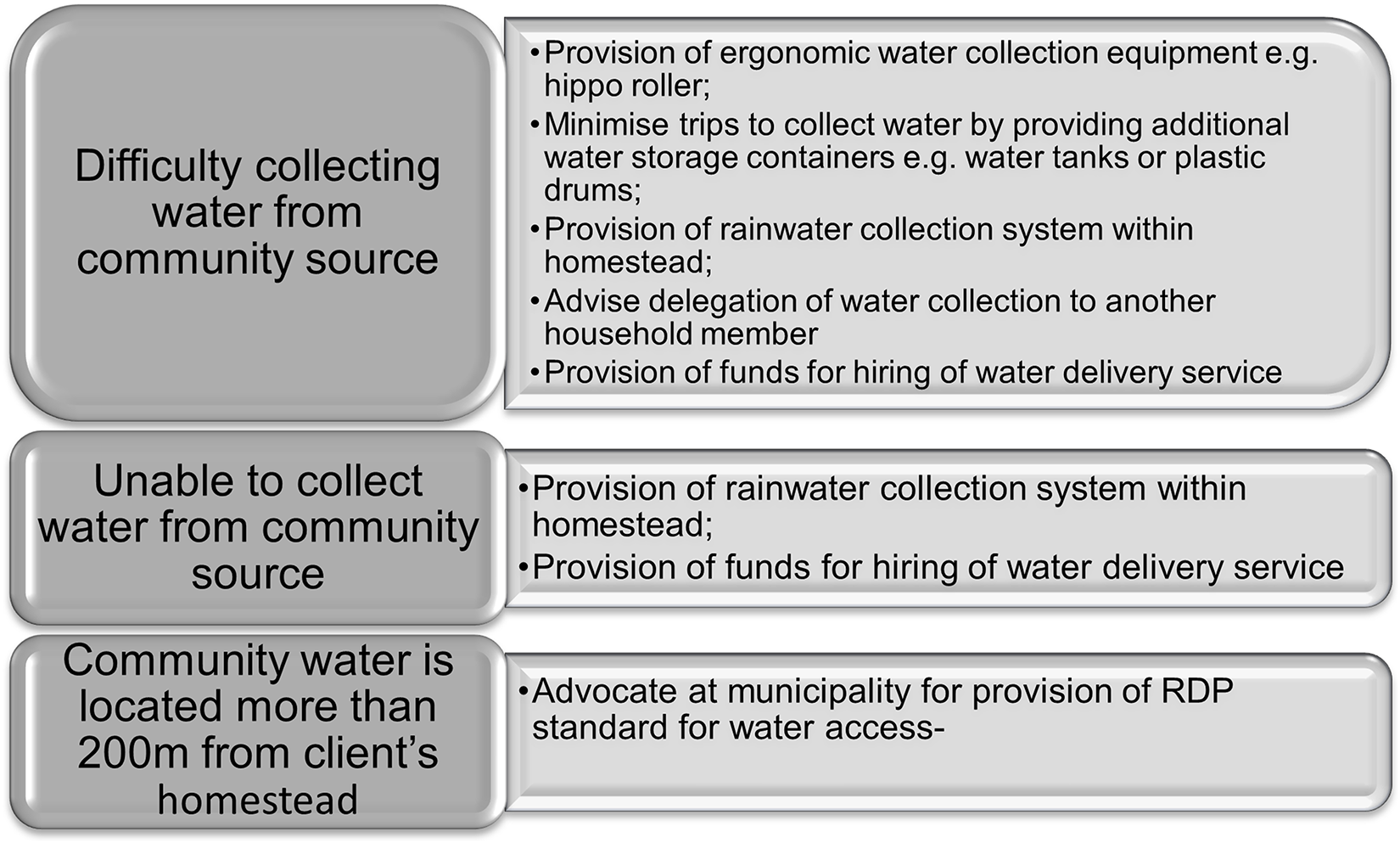
Possible FCE findings regarding water access and reasonable accommodations for inclusion in compensation.
Limitations of the study
While there is extensive evidence that demonstrates limited household access to water as a global challenge, there remains a paucity of literature regarding the ergonomics, manual handling and time demands of the water-collection occupation. The geographical area of the data gathering in the study was too small for the findings to be generalised to the entire population residing in rural resource-constrained areas of South Africa; the generalisation of results for individuals living in other rural resource-constrained contexts is therefore limited. Additional occupational therapy studies in other rural resource-constrained communities could mitigate this limitation and confirm whether the ergonomics and manual handling demands of water collection identified in the current study are typical of other rural or resource-constrained urban South African contexts. Future such studies should include longitudinal methodologies and utilise a larger, stratified sample that includes men, women and children from varied geographic locations and socioeconomic groups.
The exclusion of the other bADLs and iADLs that have significant ergonomic and manual handling demands is also regarded as a limitation of the current study. The measurement of performance of bADL and iADL tasks with significant physical capacity and manual handling demands in rural contexts using electronic data collection methods to reduce observer bias would be more comprehensive and include all bADLs and iADLs.
A history of musculo-skeletal problems or previous injuries may have affected the manual handling capacity of the participants in this study. The possible role of these variables requires further investigation and not recording the presence of these factors or excluding participants based on a medical diagnosis is a limitation of the current study.
Conclusion
Access to potable water remains a challenge to billions globally despite efforts aligned to SDG 6. While there have been significant improvements in terms of access to piped water throughout South Africa since 1994, many homesteads in rural villages in Limpopo Province still have limited water access.
The finding that collection of water in a rural resource-constrained context has considerable ergonomic, physical capacity and time implications is important for the practice of occupational therapy in South Africa and internationally. The study produced initial normative data for the manual handling demands of the water collection iADL by rural dwellers, which had not previously been reported. The extended time and effort required for water collection significantly exceeds safe limits in a typical employment context and arguably constitutes an ongoing social and occupational injustice. The findings and associated recommendations could be used to improve the accuracy and contextual relevance of FCE assessments conducted by occupational therapists for medico-legal and insurance purposes to guide appropriate compensation for rural dwellers. Furthermore, they prompt the global occupational therapy fraternity to expand discourse regarding theoretical frameworks to include unpaid work occupations typical of rural settings.
Footnotes
Acknowledgments
The authors have no acknowledgements.
Ethical approval
The study was approved by the Human Research Ethics Committee (Medical) of the University of the Witwatersrand (Approval certificate M150925), as well as the Research Ethics Committee of the Limpopo Department of Health.
Consent for participate
The background and purpose of the study were explained and written informed consent, including permission for photographs and videos, was obtained from all participants prior to the start of each respective home visit.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.