
Abstract
Background
Sleep deprivation, common among physicians working long shifts, affects sensory integration, motor coordination, and cognitive performance. While its impact on cognitive and motor skills is well-documented, its effect on gait remains largely unexplored.
Objective
This study investigated the effects of a 24-h shift on the gait parameters of interns to understand the impact of sleep deprivation and recovery.
Methods
Twenty-eight interns (10 men, 18 women) participated. Gait analysis was performed before the shift, immediately after, and after 24 h of rest. Sleep duration during rest was recorded. Data from the three analyses were compared to assess gait symmetry and the relationship between sleep duration and gait parameters.
Results
No significant changes were observed in gait parameters immediately after the 24-h shift compared to pre-shift measurements. After the rest period, significant changes were found: right-sided foot rotation (p = 0.033) and single support line (p = 0.049) increased, while left-sided foot rotation decreased compared to pre- and post-shift measurements (p < 0.001). A positive correlation was noted between daytime sleep duration and the single support line on both sides (right: r = 0.51, p = 0.005; left: r = 0.397, p = 0.037). A negative correlation existed between nighttime sleep and step width (r = –0.451, p = 0.016).
Conclusions
While 24-h acute sleep deprivation did not significantly affect gait, partial sleep deprivation during recovery influenced certain parameters. These findings underscore the importance of adequate rest for maintaining physical performance in physicians. Future research with larger, diverse samples is recommended to confirm these results and explore broader implications.
Keywords
Introduction
One of the most demanding aspects of being a physician is enduring lengthy working hours, which is frequently exacerbated by the high demand for medical care and scarcity of resources. These factors often compel doctors to work selflessly, pushing them beyond their physical limits. 1 The rigorous schedule makes it challenging for them to obtain sufficient sleep, particularly during night shifts. Sleep deprivation, defined as sleeping less than 7–8 h per night on average for adults, is a prevalent issue among doctors.2,3
Sleep deprivation leads to several changes in the central nervous system that can significantly impair a doctor's performance.4–6 It disrupts sensory integration and motor coordination by affecting the metabolism of key brain structures, such as the thalamus, cerebellum, and basal ganglia. 7 Activation in the thalamus and insula increases and the thickness of the precuneus and posterior cingulate cortex decreases. 4 Additionally, the connections and functionality within and between the amygdala, anterior cingulate, and medial prefrontal cortex are compromised, which leads to emotional dysregulation.
According to research, inadequate sleep leads to a decrease in the activity of the intraparietal sulcus and dorsolateral prefrontal cortex, which in turn impairs the ability to maintain attention. 6 The neurological changes resulting from sleep deprivation significantly impact performance. Individuals with poor sleep display reduced and slower responses to the stimuli. 5
Several studies have investigated the impact of sleep deprivation on physicians, particularly on those working long night shifts.1,2,6,8 Studies suggest that after a 24-h shift, physicians experience significant declines in psychomotor skills, reaction times, attention, and concentration, as well as reduced manual dexterity, all of which can be attributed to sleep deprivation. 2 For instance, intubations performed by emergency physicians during night shifts have been observed to take longer. 6
Additionally, sleep deprivation has been shown to negatively affect simulation performance, with studies reporting decreased overall performance in arthroscopy simulations after 24 h of work and increased errors, longer procedure times, and heightened stress during laparoscopy simulations.1,8 Attention deficits appear to be a key factor underlying many of these performance impairments associated with sleep deprivation. 5
According to previous research, the negative consequences of sleep deprivation extend beyond emotional and attentional deficits, as it also impairs the integration of visual, vestibular, and somatosensory inputs, which can lead to weakened muscle function and compromised postural orientation.5,9 Research by Batuk et al. demonstrated that sleep deprivation can adversely affect postural control and visual processing, thereby increasing the risk of accidents. 10
In light of these findings, our study aimed to investigate the effects of sleep deprivation on gait parameters of physicians. Spatiotemporal measures derived from the butterfly diagram have been shown to reflect neurological impairment and cerebellar dysfunction in clinical populations. 11 However, no previous study has specifically examined the impact of an acute 24-h shift followed by natural rest on gait parameters in physicians. As walking is an essential aspect of both daily and professional life, it is surprising that there is a noticeable gap in the literature regarding the effect of sleep deprivation on gait. We therefore hypothesized that a 24-h shift would affect gait symmetry, and that these changes might partially recover after rest. Our research sought to address this gap by examining how sleep deprivation influences physicians’ gait and the extent to which how much this effect changes after 24 h of rest.
Materials and methods
The present study was carried out in accordance with the ethical principles outlined in the Declaration of Helsinki and received approval from the Non-Interventional Scientific Research Ethics Committee of Trakya University Faculty of Medicine (approval date: 08/08/2022, approval no: 16/21).
Study design
The present study was designed to evaluate gait symmetry and changes in gait parameters across three time points in participants. The first measurement was conducted at the beginning of a 24-h shift, the second immediately after the shift, and third, following a 24-h rest period. All measurements were conducted in the movement analysis laboratory of the anatomy department at Trakya University Faculty of Medicine. The first measurement took place between 7:30 AM and 7:45 AM, while the second measurement was conducted between 8:15 AM and 8:30 AM. Participants who slept during their shift were excluded from the study. During the final measurement, participants were asked about their sleep duration during the 24-h rest period, both during the day and night. The data obtained were used to analyze the relationship between sleep duration and gait parameters after rest, as well as to evaluate gait symmetry for each measurement and to analyze the changes in all data across the three measurements.
Participants
Participants in the study consisted of interns working in the obstetrics, gynecology, and general surgery departments at Trakya University Faculty of Medicine. These individuals were invited to participate and were required to sign an informed consent form prior to being enrolled in the study. The Pittsburgh Sleep Quality Index was administered to assess the sleep quality of the volunteers. Those with a score of 5 or above, individuals with medical conditions that could affect walking ability, individuals taking medications that could impact sleep, and those who had slept less than 7 h the night before the study were excluded from the study. A total of 28 volunteer interns, comprising 10 male and 18 female participants, completed the study. An a priori power calculation indicates that approximately 33 participants would be required to detect a medium within-subject effect (Cohen's d = 0.5) with 80% power at α = 0.05 (two-tailed); therefore, the present sample may have been underpowered to reliably detect small-to-moderate differences. Accordingly, the findings should be considered preliminary and interpreted with caution.
Gait analysis
Gait analysis was performed using force platforms (Zebris© FDM system type FDM 3.5), which had dimensions of 158 × 60.5 × 2.5 cm and a sensor area of 149 × 54.2 cm. The Zebris FDM system has been validated for reliability and accuracy in measuring spatiotemporal gait parameters. 12 The force platforms were combined to create a walkway, and wooden blocks were placed at both ends to compensate for the height difference between the floor and the platform, resulting in a walking path measuring 636 cm in length. However, data recording was limited to only 298 cm of this path. The information obtained from the force platforms was transferred to a computer using the WinFDM software (Zebris Medical GmbH, Isny, Germany).
The study analyzed several gait parameters, including geometric data such as foot rotation (°), step width (cm), step length (cm), and stride length (cm). Time data such as step time (sec), cadence (strides/min), and velocity (km/h) were also analyzed. Additionally, the study looked at phases such as stance phase (%) and swing phase (%). The butterfly diagram data included gait line length (mm), single support line (mm), anterior/posterior position (mm), anterior/posterior variability (mm), lateral symmetry (mm), and lateral variability (mm) (Figure 1).
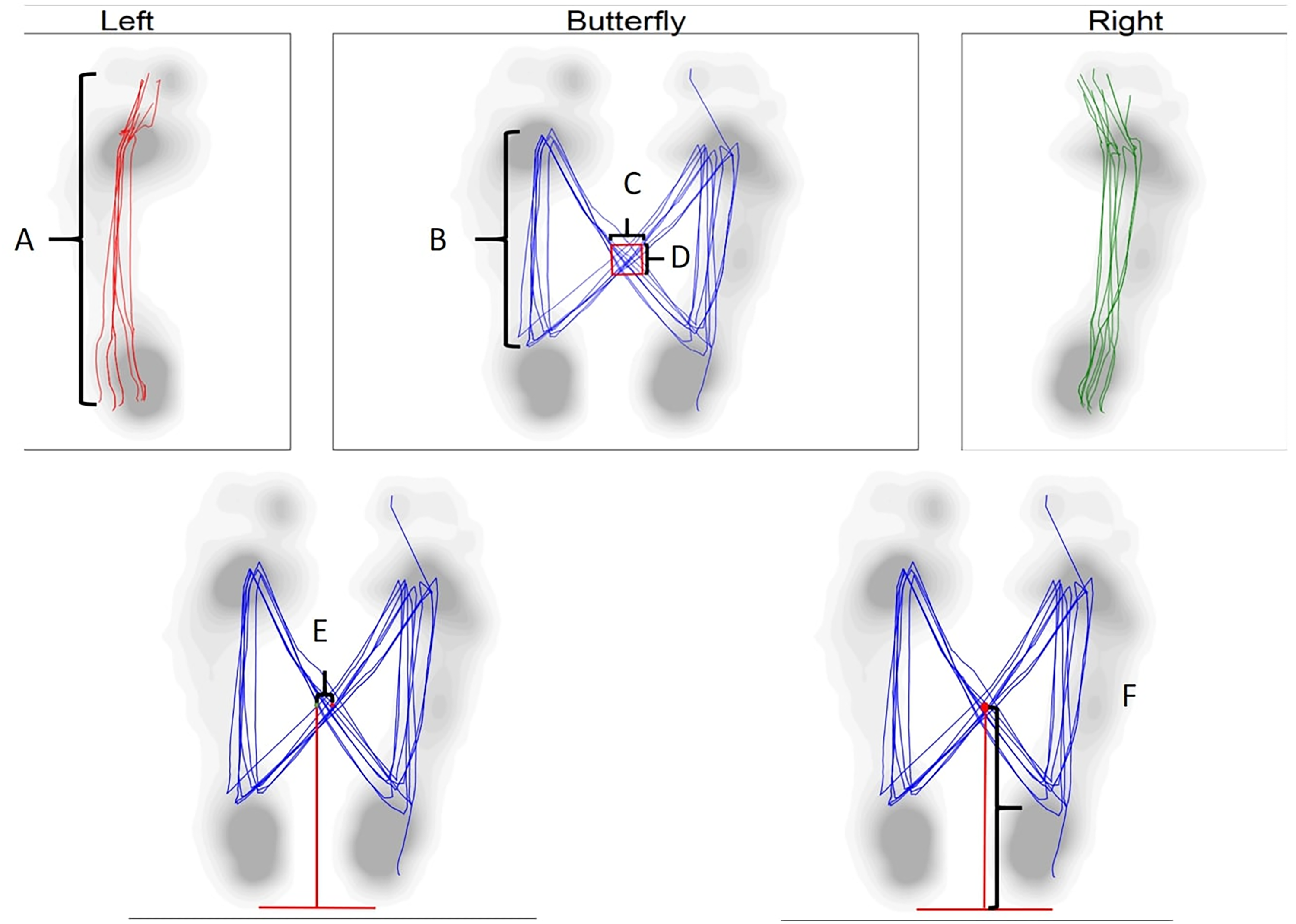
Butterfly diagram. A: Gait line length B: Single support line C: Lateral variability D: Anterior/posterior variability E: Lateral symmetry F: Anterior/posterior position.
Statistical analysis
Statistical analysis was conducted using the SPSS software program (Version 25.0, Armonk, NY, USA). The normal distribution of the data was evaluated using the Shapiro-Wilk test. A paired t-test was employed to compare data obtained from the right and left sides for gait symmetry, utilizing the normal distribution of data, while the Wilcoxon test was used for non-normally distributed data. Repeated measures analysis of variance (ANOVA) was used to analyze pre-shift, post-shift, and post-rest data, with normal distribution data being assessed using a repeated measures ANOVA and non-normally distributed data being assessed using the Friedman test. The Spearman correlation test was utilized to assess the relationship between the parameters of the final gait analysis and sleep durations. A p-value of less than 0.05 was considered statistically significant.
Results
Demographic characteristics
The average age of the participants was 24.7 ± 1.69 years, with an average height of 168.9 ± 8.73 cm and an average weight of 66.3 ± 13.8 kg.
Gait symmetry
No significant differences were observed between the right and left sides in gait parameters before and after the shift. However, after the rest period, significant differences were noted in foot rotation (p = 0.033) and single support line (p = 0.049), which were both higher on the right side (Table 1).
Gait symmetry.
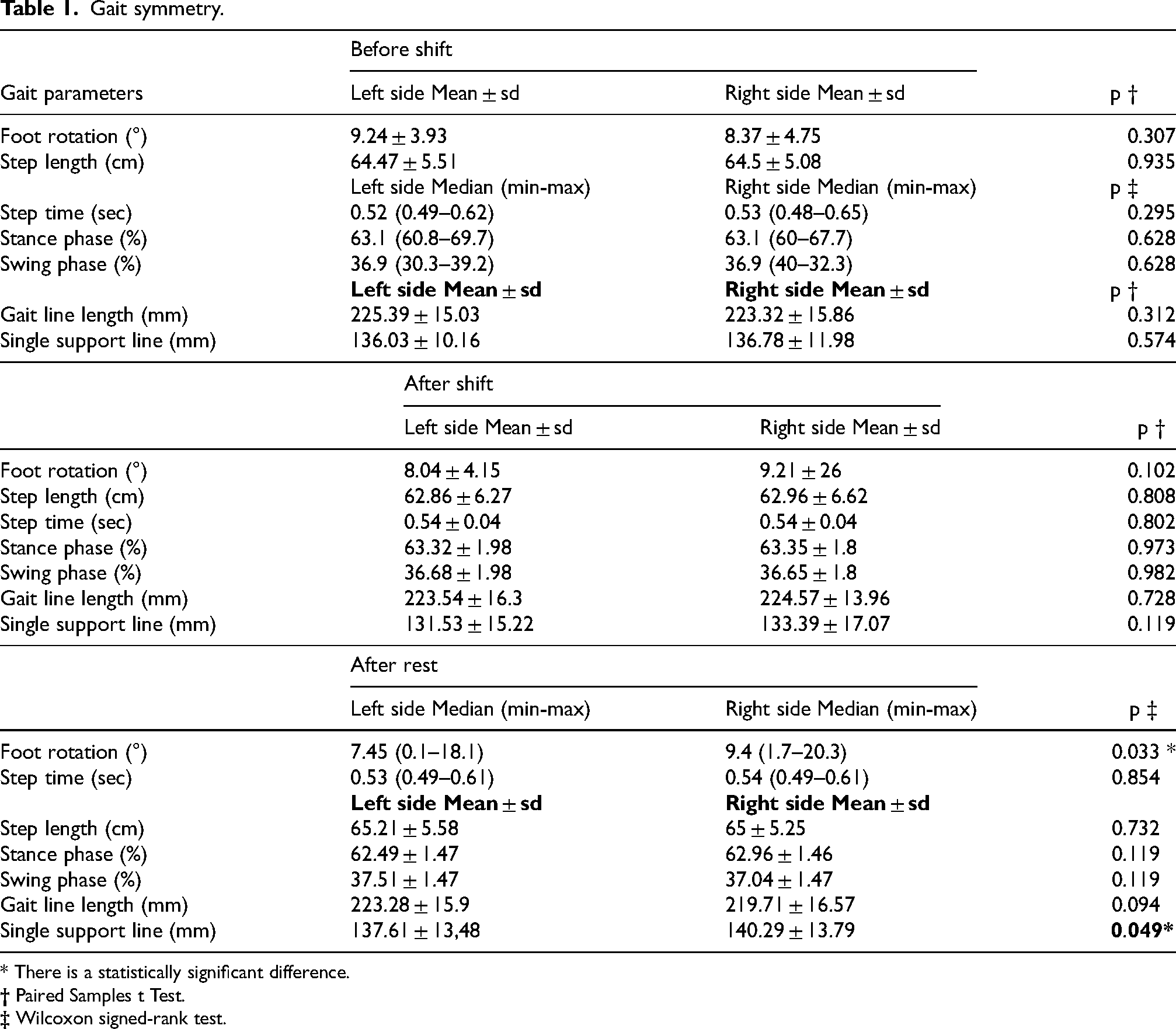
* There is a statistically significant difference.
Comparison of data from three measurements
When comparing the data obtained from the pre-shift, post-shift, and post-rest measurements, it was found that the degree of left-sided foot rotation was significantly lower after the rest period compared to both the pre- and post-shift measurements (p < 0.001). Additionally, the single support line on the right side was higher after the rest period than after the post-shift measurement (p = 0.028). No significant differences were observed in other gait parameters (Table 2).
Comparison of data from three measurements.
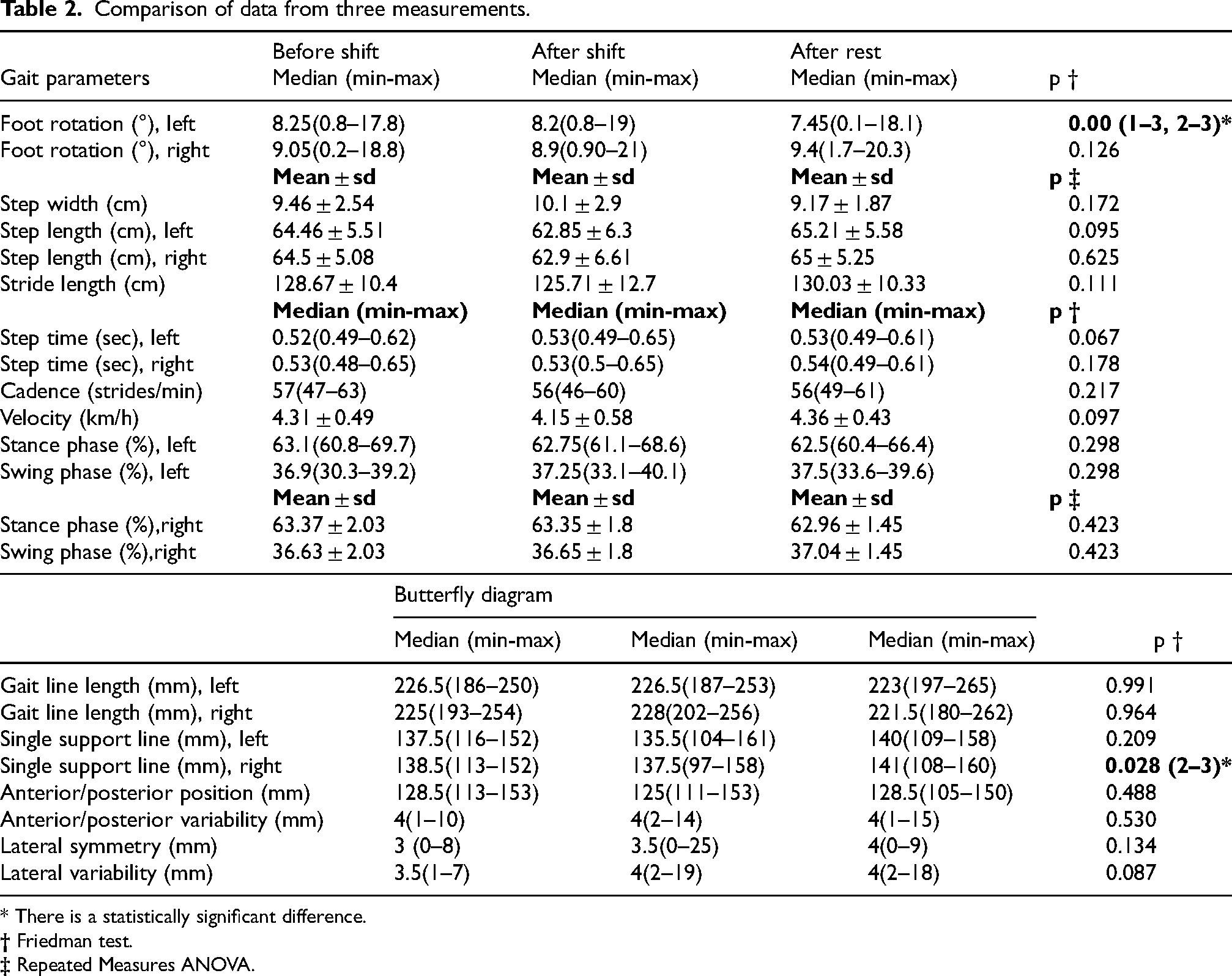
* There is a statistically significant difference.
Correlation between sleep duration and gait data
During the rest period, the median (minimum-maximum) sleep durations for the participants were 3.5 (1–7) hours during the day and 6.8 (5.5–10) hours during the night. The relationship between participants’ sleep duration during the rest period and their gait parameters was analyzed. A negative correlation was found between nighttime sleep duration and step width (r = −0.451, p = 0.016). In contrast, a positive correlation was observed between the duration of daytime sleep and a single support line on both sides. The correlation was weak on the left side (r = 0.397, p = 0.037) and moderate on the right side (r = 0.51, p = 0.005) (Table 3).
Relationship between sleep duration and gait parameters.
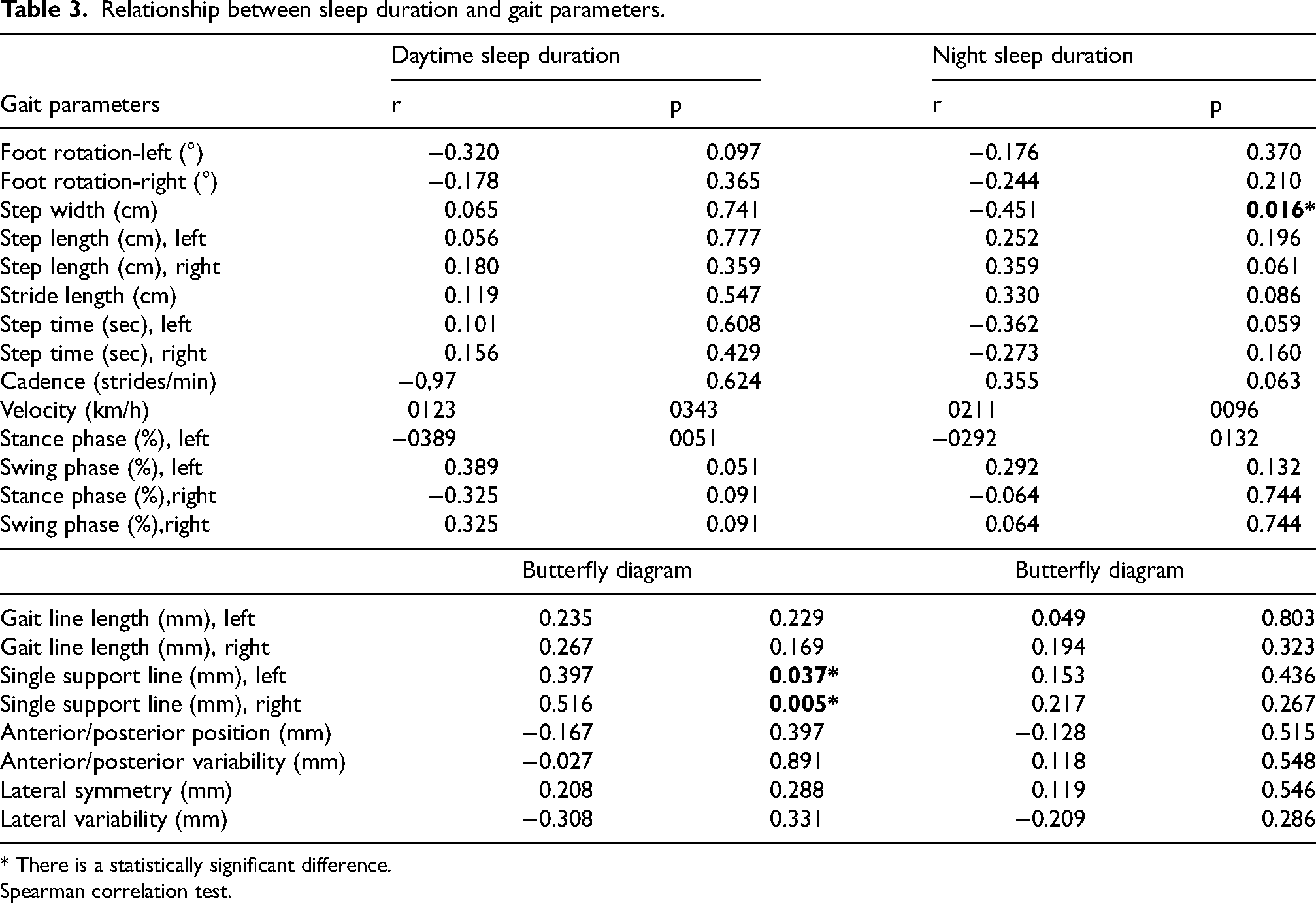
* There is a statistically significant difference.
Spearman correlation test.
Discussion
The primary objective of this research was to investigate the impact of sleep deprivation on interns during a 24-h shift and the subsequent changes in gait parameters following a 24-h rest period. The three phase design offers comprehensive insight into the temporal effects of sleep deprivation and recovery on intern's gait. Although all participants were required to have adequate sleep before the study began, we did not enforce this requirement for post-rest measurements, allowing participants to rest naturally without interference. Surprisingly, acute total sleep deprivation did not significantly affect the gait parameters.
Sleep deprivation has been known to result in various changes in the central nervous system, which are reflected in both cognitive and physical performance.13–15 For physicians whose professional lives require optimal cognitive and physical functioning, sleep deprivation imposed by demanding work schedules poses a significant challenge. Previous studies have demonstrated that physician performance in simulation training decreases following night shifts, with lack of attention being the primary contributing factor to this decline in job performance.1,5,8 Although research on the consequences of sleep deprivation on gait parameters is limited, existing studies have not concentrated on physicians or their working hours. This study fills a critical gap in the literature, which has previously overlooked the specific impact of sleep deprivation on gait parameters in the context of physicians’ demanding work schedules.
Boolani et al. discovered that individuals who received sufficient sleep maintained their gait speed better while displaying greater gait asymmetry. They reported that stride length, gait rhythm variability, and transverse plane range of motion were higher in the sleep-deprived group. The authors recommended that clinicians assess gait performance by inquiring about an individual's sleep quality the previous night. 16 Similarly, Umemura et al. found that sleep-deprived individuals performed worse in gait tasks than a control group, further supporting the notion that sleep deprivation adversely affects gait parameters. 17 In contrast, no immediate change in walking speed or step length was seen in our intern cohort after a 24-h shift, but some changes occurred after a subsequent rest period. This discrepancy may be related to physicians’ possible adaptation to long working hours; however, shift-work experience and subjective fatigue were not directly measured in the present study, and this interpretation should therefore be considered with caution. Methodological differences and the relatively small sample size of our study may also have contributed to this finding. Adequate sleep is critical for maintaining performance in complex tasks, likely because of the role of sleep in integrating visual, vestibular, and motor functions.18–21
Based on the existing literature, we anticipated that sleep deprivation would negatively impact gait. However, contrary to our expectations, no significant differences in gait parameters were observed immediately before and after the shift. As recommended by experts, the optimal sleep duration for young adults is 7–9 h; sleeping less or more than this can lead to sleep deprivation or extended sleep, respectively. 22 In our study, we observed that only 13 participants had adequate sleep, 14 experienced acute partial sleep deprivation, and one had extended sleep. This observation indicates that rest, particularly the quality and duration of sleep, may influence certain gait parameters, underscoring the complexity of sleep's impact on physical performance.
Interestingly, we did not observe any differences after total sleep deprivation; however, changes were observed after partial sleep deprivation. There are two possible explanations for this observation. First, participants might have tolerated one night of total sleep deprivation, but subsequent partial sleep deprivation could have been more challenging. Second, participants’ daytime sleep could have influenced their recovery. Our findings suggest a correlation between daytime sleep duration and a single support line, indicating that daytime sleep can partially explain the observed changes in this parameter. The single support line represents the load transfer during the single support phase. 23 The positive correlation between daytime sleep and single support line suggests that daytime sleep may contribute positively to balance. Conversely, a wider step width is a known compensatory strategy to increase dynamic stability. 24 The negative correlation we observed between nighttime sleep duration and step width suggests that insufficient sleep during the recovery period may negatively affect balance mechanisms. However, the reason for the difference in foot rotation remains unclear. This correlation did not result in significant changes in gait symmetry or in the comparison of the data from the three measurements. From a clinical perspective, the absence of acute gait changes should not be interpreted as the absence of risk. The decreased symmetry of foot rotation after rest may reflect changes in sleep rhythm and fatigue. 25 However, given the absence of a time-matched control group, these findings should be interpreted with caution, as circadian or diurnal influences cannot be fully ruled out.
This study had several limitations. First, the evaluation of sleep duration was subjective, relying solely on participants’ self-reported sleep duration, which may have weakened the reliability of our findings. In future studies, more objective evaluations can be made using objective sleep monitoring tools such as actigraphy to measure sleep duration and quality. Second, since the participants were interns, their average age was relatively young, which could have influenced the results. Finally, the small sample size of 28 participants limits the generalizability of our findings; therefore, future studies with larger and more diverse samples are required to confirm these exploratory results before applying them to broader populations. Moreover, a time-matched control group was not included in the study design; therefore, the observed changes cannot be definitively distinguished from potential circadian or diurnal variations over the 48-h testing period. Additionally, including participants from different medical institutions and specialties would enhance the originality, generalizability, and practical utility of the study's findings.
Conclusion
In this study, we found that completing a 24-h shift without sleep did not significantly affect the gait of interns. However, during the subsequent rest period, most participants experienced poor sleep quality at night. A notable finding was that left-sided foot rotation decreased as a single parameter of gait symmetry after rest, a change that was consistent across all three measurements. Specifically, left-sided foot rotation was the lowest in the final measurement. We believe that these changes in foot rotation represent transient fatigue related adjustments rather than a stable biomechanical asymmetry. Additionally, the right-sided single support line increased after the rest period compared to post-shift measurements. Although there were correlations between daytime and nighttime sleep durations and certain gait parameters, only the aforementioned right-sided single support line displayed a corresponding change in gait, whereas other correlations were not reflected. To yield more substantial outcomes, future studies should involve participants from diverse age groups and larger sample sizes. Our study indicated that acute sleep deprivation, such as that resulting from extended shifts, does not have a discernible impact on gait among physicians. However, the changes observed following the rest period may be related to variations in sleep duration and quality rather than recovery alone. Given the observed correlations between sleep duration and certain gait parameters, ensuring adequate recovery sleep after extended shifts may be important for maintaining motor performance. Further research is needed to define appropriate recovery sleep durations.
Footnotes
Acknowledgments
We would like to thank the staff of Trakya University Faculty of Medicine, Department of Anatomy, for their assistance in the data collection process.
Ethical approval
The present study was carried out in accordance with the ethical principles outlined in the Declaration of Helsinki and received approval from the Non-Interventional Scientific Research Ethics Committee of Trakya University Faculty of Medicine (approval date: 08/08/2022, approval no: 16/21).
Informed consent
Informed consent was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.