
Abstract
Background
Chronic neck and back pain is a prevalent issue among caregivers of individuals with special needs, often worsened by the physical and emotional demands of caregiving. Telerehabilitation has emerged as a promising alternative to conventional physiotherapy, offering accessible, home-based interventions.
Objective
To compare the effectiveness of telerehabilitation and conventional physiotherapy in reducing pain, fatigue, and caregiver burden while improving quality of life in caregivers with chronic neck and back pain.
Methods
Thirty caregivers aged 20–60 with chronic neck and back pain were enrolled in a randomized, controlled trial. Group 1 (telerehabilitation) received a structured, digitally monitored exercise program for 12 weeks. Group 2 (conventional physiotherapy) received 4 weeks of supervised in-person treatment, followed by 8 weeks of unsupervised home exercises. Group 3 served as a control group.
Results
The telerehabilitation group demonstrated greater improvements across all outcomes compared to both the conventional physiotherapy and control groups. However, differences in follow-up intensity and supervision may have contributed to these findings.
Conclusions
Telerehabilitation appears to be an effective and practical alternative to conventional physiotherapy for caregivers, particularly when in-person access is limited. Interpretation of findings should consider variations in delivery and monitoring across groups.
Keywords
Introduction
Pain is one of the most significant human experiences and a prevalent issue encountered in clinical settings. In consequence of the studies conducted by the International Association for the Study of Pain (IASP), the definition of pain accepted by the IASP Council was determined to be “an uncomfortable sensory and emotional experience linked to actual or potential tissue damage”. This definition supports more effective pain management in clinical practice and research. 1
Chronic neck pain is defined as pain in the neck that persists for a minimum of 12 weeks, with or without concomitant pain in one or both upper extremities. 2 Neck pain is a prevalent health issue that markedly impacts an individual's quality of life. It can be attributed to a multitude of underlying causes and frequently evolves into a chronic condition. Chronic neck pain has the potential to negatively impact an individual's daily activities and work performance, ultimately reducing their standard of living and placing an additional burden on the healthcare system, both physically and psychosocially. While not the most prevalent musculoskeletal disorder, the economic impact of neck pain is significant, encompassing treatment costs, reduced productivity, and a loss of the workforce. 3 The prevalence of neck pain among working individuals in Türkiye exhibits considerable variation, with estimates ranging from 20.5% to 47.8%. Additionally, the annual disability rate associated with neck pain is reported to be between 2% and 11%. These data underscore the significant impact of neck pain on both health and socioeconomic outcomes. To effectively manage and treat neck pain, more comprehensive and systematic research is necessary. 4
Most pain complaints are musculoskeletal, with back pain being the most common. The widespread prevalence and significant impact of back pain have resulted in a growing array of tests and treatments, such as physiotherapy, injections, surgeries, implantable devices, and medications. 5 Back pain can be classified as acute or chronic. Acute pain typically manifests over a period of 3–4 weeks, whereas chronic pain is defined as pain that persists for at least 3 months. This distinction is crucial for determining appropriate treatment approaches and optimizing patient management. Acute back pain is usually a temporary condition, whereas chronic back pain is linked to long-term health issues and a significant reduction in quality of life. Consequently, both conditions necessitate comprehensive assessment and the implementation of suitable treatment strategies. 6
The objective of conservative treatment for neck and back pain is to control pain, reduce inflammation, reduce reflex muscle spasm, accelerate healing by protecting the damaged area, and normalize function in activities of daily living by restoring muscle strength and range of motion. This is achieved through the use of various methods, including rest and orthoses, medications, physical therapy modalities, injections, manipulation, exercises, and surgery. 7
Caring for a child with a disability is a prolonged and demanding journey for parents. During this process, mothers, fathers, or other caregivers invest substantial effort, often face sleep deprivation, and experience fatigue while attending to, transporting, and actively participating in the child's rehabilitation. Consequently, it has been documented that the physical health of mothers and fathers is adversely affected. 8 In a study, musculoskeletal pain and related factors were examined in mothers with children with cerebral palsy and mothers with healthy children. The results indicated that musculoskeletal pain and depression scores were statistically significantly higher in mothers with children with cerebral palsy compared to other mothers. 9
The onset of the Coronavirus Disease 2019 (COVID-19) pandemic has sparked a growing interest in remote healthcare models, especially telerehabilitation. Telerehabilitation is a novel approach that leverages information and communication technologies (ICTs) to facilitate the remote delivery of rehabilitation services. This innovative method offers several advantages, including enhanced accessibility to care and cost-effectiveness. Although telerehabilitation has the potential to overcome some of the obstacles faced by patients who have difficulty accessing traditional, in-person services, the use of technology can also introduce new challenges and influence the perceived value of rehabilitation services. 10 A significant proportion of patients have restricted access to in-hospital or outpatient rehabilitation services. Following the conclusion of their treatment, many patients encounter difficulties in performing home exercise programs. Research findings indicate that the majority of patients either do not perform or only partially perform traditional home exercise programs. 11 Alternative models of care, such as telerehabilitation, have the potential to overcome some of the barriers to engagement that are encountered, particularly in the case of patients who are unable to participate in face-to-face treatment with their physiotherapist. 12
Despite growing evidence on telerehabilitation for musculoskeletal conditions, the literature remains notably limited in studies targeting caregivers of individuals with special needs, a population highly vulnerable to chronic spinal pain due to prolonged physical strain and postural stressors. To our knowledge, no prior randomized controlled trials have directly compared telerehabilitation versus conventional physiotherapy in this specific demographic. Moreover, existing studies often lack longitudinal follow-up and do not report clinically meaningful metrics such as effect sizes and confidence intervals.
This study addresses these gaps by evaluating both the short- and long-term effectiveness of telerehabilitation in caregivers with chronic neck and back pain, while incorporating robust clinical outcomes and statistical rigor. By doing so, it not only expands the scope of telerehabilitation research but also offers practical insights for accessible and sustainable rehabilitation models tailored to caregiver populations.
Given the information above, the aim of this study was to assess the effectiveness of telerehabilitation versus a traditional physiotherapy program for individuals with chronic neck and back pain, while also exploring the challenges experienced by caregivers of individuals with special needs. The findings may also inform the planning and standardization of services for caregivers and patients in newly established rehabilitation centers, as well as the development of physiotherapy interventions.
We hypothesized that telerehabilitation would be superior to conventional physiotherapy and no treatment in reducing pain and fatigue, improving quality of life, and decreasing caregiver burden in individuals with chronic neck and back pain.
Materials and methods
Study design and participants
In this prospective, randomized, single-blind, controlled study, caregivers of individuals with special needs, aged 20–60, with chronic neck and/or back pain, were included. The study adhered to the principles of the Declaration of Helsinki, and ethical approval was obtained from the relevant institutional review board. Prior to enrollment, participants received detailed information about the purpose and procedures of the study and provided written informed consent. The trial was conducted and reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines. 13
Chronic neck and/or back pain was defined as musculoskeletal spinal pain persisting for more than three months, in accordance with the International Association for the Study of Pain (IASP) criteria. Prior to inclusion, all participants were clinically evaluated by a qualified physician. The diagnostic process included detailed medical history-taking, standardized pain mapping (e.g., body diagrams), and a physical examination assessing spinal mobility, posture, tenderness, and muscular tension. Individuals presenting with red flag symptoms—such as neurological deficits, systemic illness, or recent trauma—were excluded. In line with current clinical practice guidelines, imaging studies (e.g., X-ray, MRI) were not performed routinely but were reserved for cases where clinical findings warranted further investigation.
Exclusion criteria were as follows: history of cervical surgery; caregiving for individuals with hearing or visual impairments; inflammatory or infective arthritis of the cervical spine; congenital spinal anomalies, malignancy, or neuropathic pain; neurological conditions such as radiculopathy or myelopathy; chronic pulmonary or vestibular disorders; ongoing pharmacologic treatment for pain; prior physiotherapy or exercise participation within the last three months; illiteracy preventing completion of questionnaires; inability to adhere to the treatment protocol; diagnosis of a new condition requiring intervention during the study period; or voluntary withdrawal.
The CONSORT flow diagram (Figure 1) illustrates the flow of participants throughout the study.

Consort flow diagram of the study.
Sample size of the research
The sample size was determined using G*Power 3.1.7 software (Heinrich-Heine-Universität, Düsseldorf, Germany). Based on a minimal clinically important difference of 10 points on the Bournemouth Neck Pain Questionnaire (BNPQ), as reported by Gay et al., 14 with α = 0.05 and β = 0.20 (80% power), the required sample size was calculated to be 12 participants per group (total N = 36). To account for potential dropouts and ensure adequate power for longitudinal follow-up, a total of 39 participants were ultimately recruited.
Randomization
Participants were randomly assigned to one of three groups (telerehabilitation, conventional physiotherapy, control) using a computer-generated block randomization sequence with a 1:1:1 allocation ratio. Block sizes of six were employed to maintain balanced group sizes throughout recruitment. The randomization sequence was generated prior to study initiation by an independent biostatistician using the RAND function in Microsoft Excel, and group assignments were concealed using sequentially numbered, sealed opaque envelopes. Each envelope was opened only after the participant's eligibility was confirmed and written consent was obtained.
Allocation concealment was ensured by having a third party not involved in enrollment or outcome assessment handle the envelope system. The randomization and allocation procedures adhered to the CONSORT 2010 and ICH-GCP guidelines to minimize selection bias and ensure methodological transparency.
Outcome assessors and statisticians remained blinded to group allocation throughout the study. Participants were instructed not to reveal their group assignments during follow-up evaluations. The physiotherapists delivering telerehabilitation interventions were distinct from those involved in data collection to further reduce performance and detection bias.
Interventions implemented in the study
Exercise program structure
A structured, progressive 12-week exercise protocol was implemented in both intervention arms, designed in accordance with established rehabilitation guidelines for chronic spinal pain. The program targeted spinal mobility, postural control, and muscular endurance—key deficits commonly observed in caregivers with chronic neck or back pain.
Frequency and Duration: Participants in both intervention groups were prescribed exercise sessions three times per week, lasting 30–40 min, with each movement performed in three sets of 10–15 repetitions.
The telerehabilitation group received automated SMS reminders during each exercise day and were asked to confirm completion via digital response. Upon completing each session, participants replied “completed” via SMS. These responses were timestamped and logged in an encrypted digital spreadsheet, which was monitored weekly by the research team to assess protocol compliance. Although this self-report confirmation provided a basic measure of adherence, its limitations—such as recall bias and the potential for overreporting—are acknowledged and discussed in the Limitations section. Future studies should incorporate objective adherence tracking tools (e.g., wearable sensors or app-based monitoring systems) to enhance data accuracy and internal validity.
The conventional physiotherapy group received in-clinic supervision for the first four weeks only; the remaining eight weeks were unsupervised and relied on self-directed exercise via printed and video materials. The control group received no structured physical intervention.
Intervention delivery by study arm
Participants received video-based exercise instruction via CD. The telerehabilitation program was delivered using a hybrid model, combining both asynchronous and synchronous components to optimize flexibility and supervision. Pre-recorded exercise videos were provided for home use, allowing participants to complete sessions at their convenience while ensuring consistency in exercise delivery.
Additionally, live interactive sessions were conducted via Zoom on alternating days during the first week of each 3-week phase. These sessions were supervised by a licensed physiotherapist, who provided real-time feedback and correction to ensure proper technique and engagement. A brief Zoom orientation was provided at baseline to familiarize participants with the platform, and technical support was made available throughout the study via phone and email. Participants were encouraged to report any platform-related issues to the study team.
Throughout the intervention, participants received digital SMS reminders on each exercise day and were instructed to reply “completed” upon finishing the session. These responses were timestamped and logged in an encrypted spreadsheet, which was monitored weekly by the research team to assess protocol compliance. Although this self-report system offered a basic adherence measure, its limitations were acknowledged and further discussed in the Limitations section.
Exercise content mirrored the structure described in section 2.4.1, and participants were asked to perform the prescribed routines three times per week over the 12-week intervention period.
The initial phase (Weeks 1–4) consisted of 20 in-person sessions (5 sessions/week) including:
Infrared heat (20 min) Transcutaneous electrical nerve stimulation (TENS) Therapeutic ultrasound (3 MHz, 1 W/cm2 for 5 min) Superficial heat therapy via hot packs (20 min)
All therapies were administered in the prone position.
In the second phase (Weeks 5–12), participants were provided with a home exercise brochure and instructed to continue the program independently. Unlike the telerehabilitation group, there was no remote supervision or adherence monitoring during this phase. The divergence in supervision intensity and adherence tracking between the two intervention arms was acknowledged as a potential confounding factor and is further addressed in the Discussion section.
No intervention was applied to the control group. Participants were advised to maintain their usual daily routines and physical activity levels throughout the study period.
(See Figure 2 for illustrative examples of the exercises used.)

Examples of exercises given to the telerehabilitation group.
Data collection
Following the baseline assessment, participants in the telerehabilitation group performed their exercises three times per week, for 30 min per session, completing three sets of 10 repetitions over a 12-week period.
Outcome assessments were conducted at three time points: prior to the intervention, at the end of the 12th week, and at six-month follow-up.
The efficacy of the treatment modalities was evaluated based on differences observed across these time points.
Ethical aspects of the study
This study was approved by the Malatya Clinical Research Ethics Commitee during its meeting on the March 3, 2021, under decision number 2021/85 and was registered in ClinicalTrials.gov under the identifier NCT06095336. Written informed consent was obtained from all participants before their involvement in the study. The study adhered to the principles of the Declaration of Helsinki.
Assessment tools
Demographic information form
The questionnaire form, which was prepared by the researcher in accordance with the existing literature, includes a number of items pertaining to the patients’ names, surnames, backgrounds, family histories, ages, heights, weights, occupations, dominant sides, smoking habits, alcohol consumption, and any additional symptoms that may be relevant.
Qualitative questions form
A form was administered to assess the number of individuals with special needs in the caregiver's care, the amount of time spent daily with these individuals, the presence of other children in the home, the availability of assistance, and the presence and nature of any concurrent physical, mental, or dual impairments.
Pain assessment
Pain intensity was measured using the Visual Analogue Scale (VAS), a widely validated and reliable tool for assessing subjective pain levels in clinical and research settings. The scale consists of a 10-centimeter horizontal line, where “0” indicates no pain and “10” represents the worst imaginable pain. Participants were instructed to mark the point that best represented their pain level at the time of assessment. The distance in centimeters from the zero point to the mark was recorded as the VAS score. The VAS has demonstrated high test-retest reliability and sensitivity to clinical changes in musculoskeletal pain populations. Its Turkish version has also been validated with strong psychometric properties..15,16
Fatigue assessment
Fatigue was assessed using the Functional Assessment of Chronic Illness Therapy–Fatigue Scale (FACIT-F), a psychometrically robust instrument designed to evaluate fatigue experienced over the past week. The scale includes 13 items rated on a 5-point Likert scale, ranging from 0 (“not at all”) to 4 (“very much”), with a total score range of 0–52. Higher scores reflect less fatigue, while a score of ≤30 indicates clinically significant fatigue. The FACIT-F has demonstrated strong internal consistency, construct validity, and responsiveness in populations with chronic conditions. The Turkish version of the FACIT-F has also been culturally adapted and validated with high reliability and content validity.17,18
Bournemouth neck pain questionnaire (BNPQ)
The Bournemouth Neck Pain Questionnaire (BNPQ) was used to evaluate the multidimensional impact of neck pain. The scale consists of 7 items assessing pain intensity, functional limitations in social and family roles, emotional well-being (including anxiety and depression), fear-avoidance beliefs (kinesiophobia), and coping strategies. Each item is rated on an 11-point numerical rating scale (0 = no problem, 10 = worst imaginable). The total score ranges from 0 to 70, with higher scores indicating greater severity. The BNPQ has demonstrated strong construct validity, internal consistency (Cronbach's α > .85), and sensitivity to change in musculoskeletal pain populations. The Turkish adaptation of the scale has also been validated with acceptable psychometric properties.19,20
Short form-36 (SF-36)
The Short Form-36 Health Survey (SF-36) is a widely used, comprehensive instrument designed to evaluate health-related quality of life. It comprises 36 items grouped into eight domains: physical functioning, role limitations due to physical health, role limitations due to emotional problems, bodily pain, general health perceptions, vitality (energy/fatigue), social functioning, and mental health. Each subscale is scored from 0 to 100, with higher scores indicating better perceived health status. The SF-36 has been validated across diverse populations and demonstrates robust psychometric properties, including strong internal consistency, test-retest reliability, and construct validity. The Turkish version has also been culturally adapted and psychometrically validated for use in clinical and research settings.21,22
Caregiver burden scale (CBS)
The Caregiver Burden Scale (CBS) is a 14-item instrument developed to assess the multidimensional impact of caregiving on individuals. Each item is scored on a 5-point Likert scale, ranging from 0 (never) to 4 (nearly always), reflecting the frequency with which the caregiver experiences burden in specific domains such as emotional strain, physical fatigue, social limitation, and time-dependence. The total score is obtained by summing the responses, with higher scores indicating greater perceived caregiver burden. The CBS has demonstrated satisfactory levels of internal consistency and construct validity in both international and Turkish caregiver populations.23,24
Statistical analysis
The data collected for the research were analyzed using SPSS 25.0 software. In the initial stage of data analysis, the suitability of the quantitative data for normal distribution was evaluated through the examination of skewness and kurtosis values. All values ranged between −2 and +2, indicating that the data were normally distributed.
Accordingly, a parametric test — repeated measures analysis of variance (ANOVA) — was conducted to compare outcomes across three time points (pre-treatment, post-treatment, and six-month follow-up) and across the three study groups (telerehabilitation, conventional physiotherapy, control). Main effects of time and group × time interactions were analyzed to detect statistically significant differences in treatment response over time. The significance level was set at p < 0.05. Data analysts were blinded to group assignments during the statistical analysis to minimize bias.
While repeated measures ANOVA revealed statistically significant group-by-time interactions, no formal post hoc test (e.g., Bonferroni correction) was applied due to the exploratory nature of the study and limited sample size. However, descriptive comparisons and effect size calculations (Cohen's d) were employed to interpret the direction and magnitude of between-group differences. These decisions and their limitations are further discussed in the Discussion section. Future studies with larger samples are encouraged to incorporate multiple comparison corrections for increased statistical rigor.
Results
A total of 45 participants were assessed for eligibility. Six participants were excluded—two for not meeting the inclusion criteria and four who declined to participate. Thirty-nine participants were subsequently randomized equally into three groups (n = 13 per group). All 39 participants completed the study without any dropouts or protocol deviations, resulting in 100% retention and intervention adherence across all groups.
Descriptive statistics of participants’ baseline demographic and clinical characteristics are presented in Table 1, revealing no significant between-group differences.
Frequency and percentage distributions of participants’ demographic information.
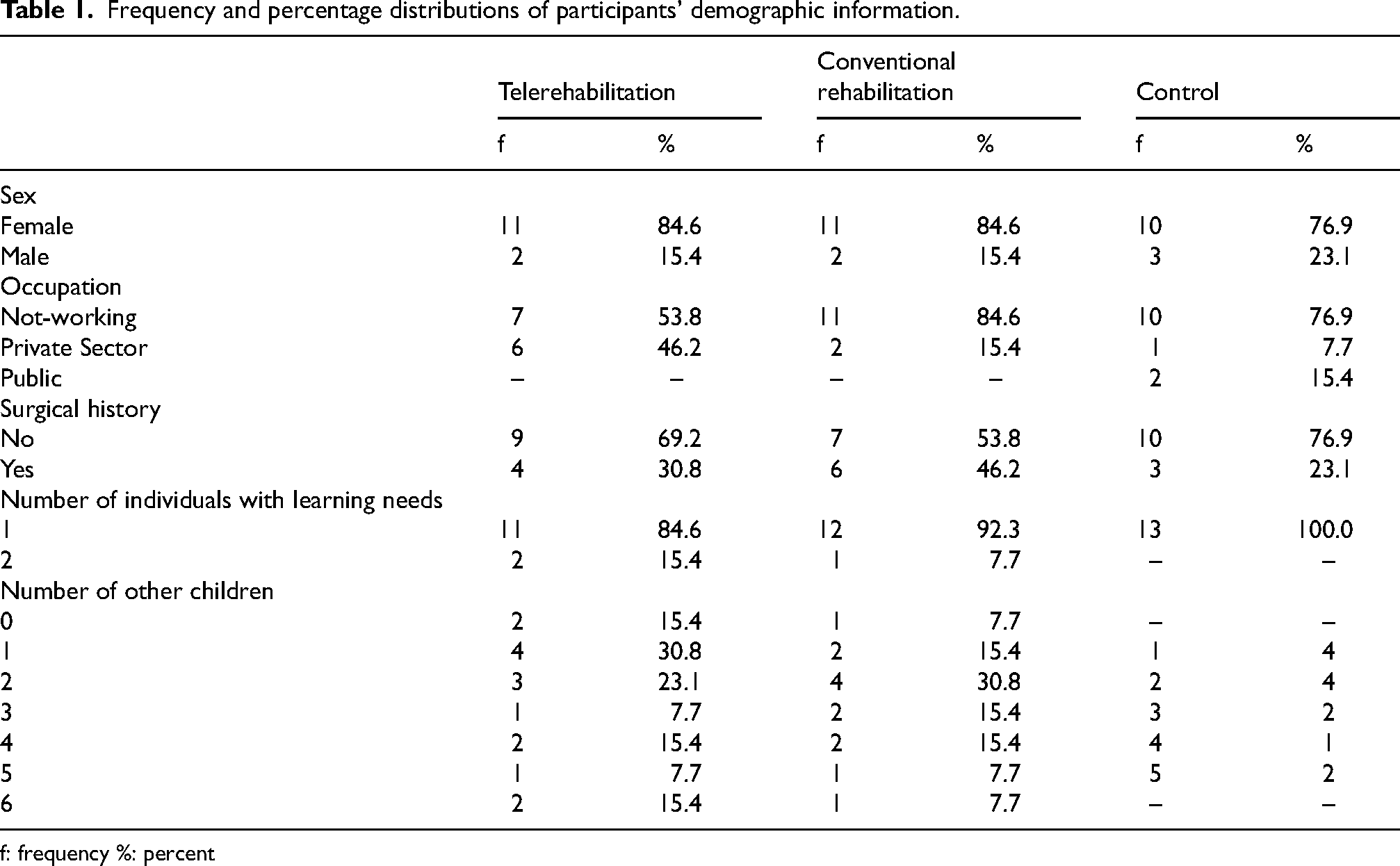
f: frequency %: percent
Table 2 illustrates the distribution of pain localization across time points. Notably, the conventional rehabilitation group exhibited a shift in pain localization patterns at both post-treatment and six-month follow-up assessments. In contrast, the telerehabilitation and control groups maintained stable pain localization profiles over the same period, suggesting differential trajectories of symptom modulation.
Distribution of pain localization across three time points and study groups.
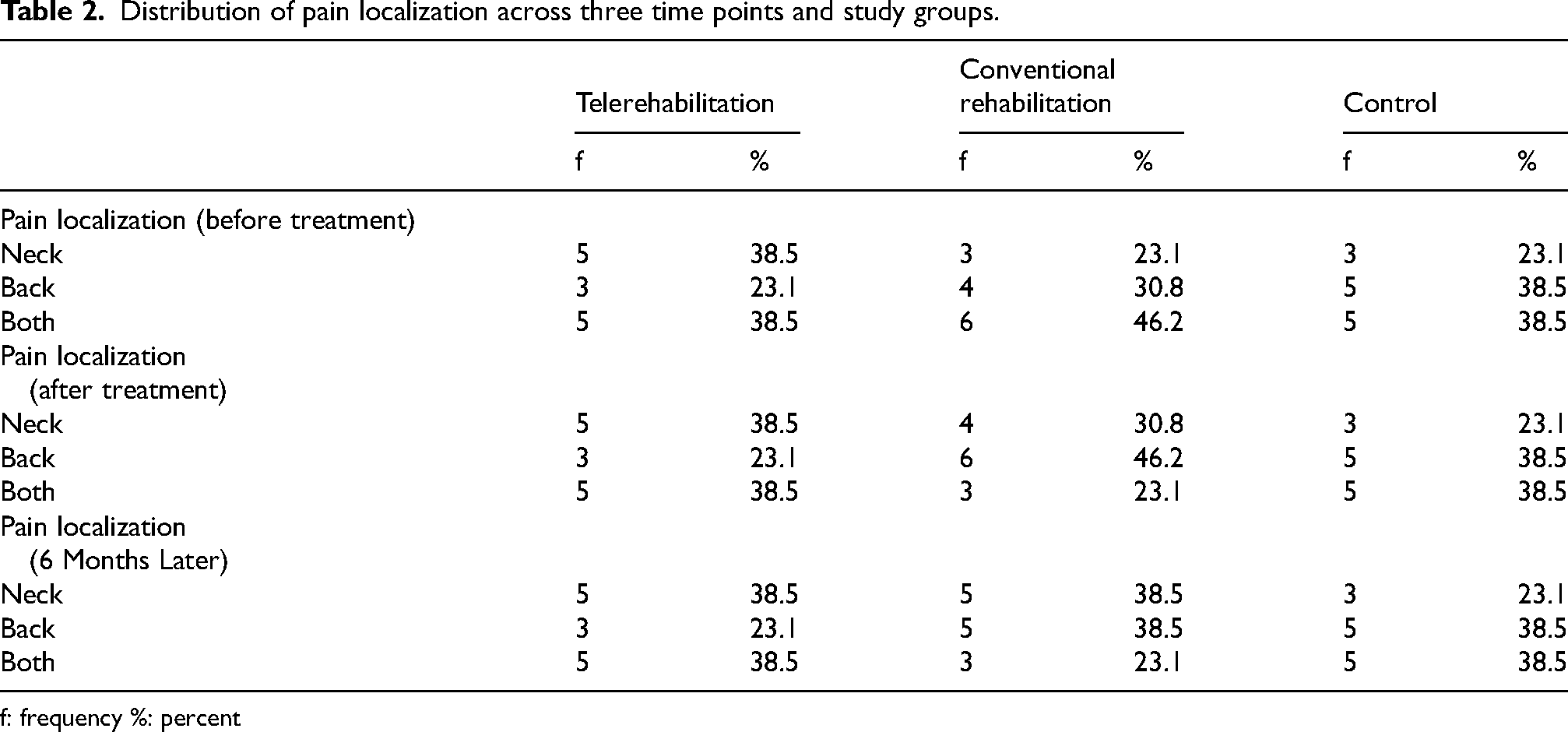
f: frequency %: percent
As shown in Table 3, the demographic characteristics (age, height, weight, BMI, and caregiving time) were comparable across the telerehabilitation, conventional rehabilitation, and control groups.
Averages of participants’ age (years), height (cm), weight (kg), BMI (kg/m2), and time spent with a child with special needs (hours/day).
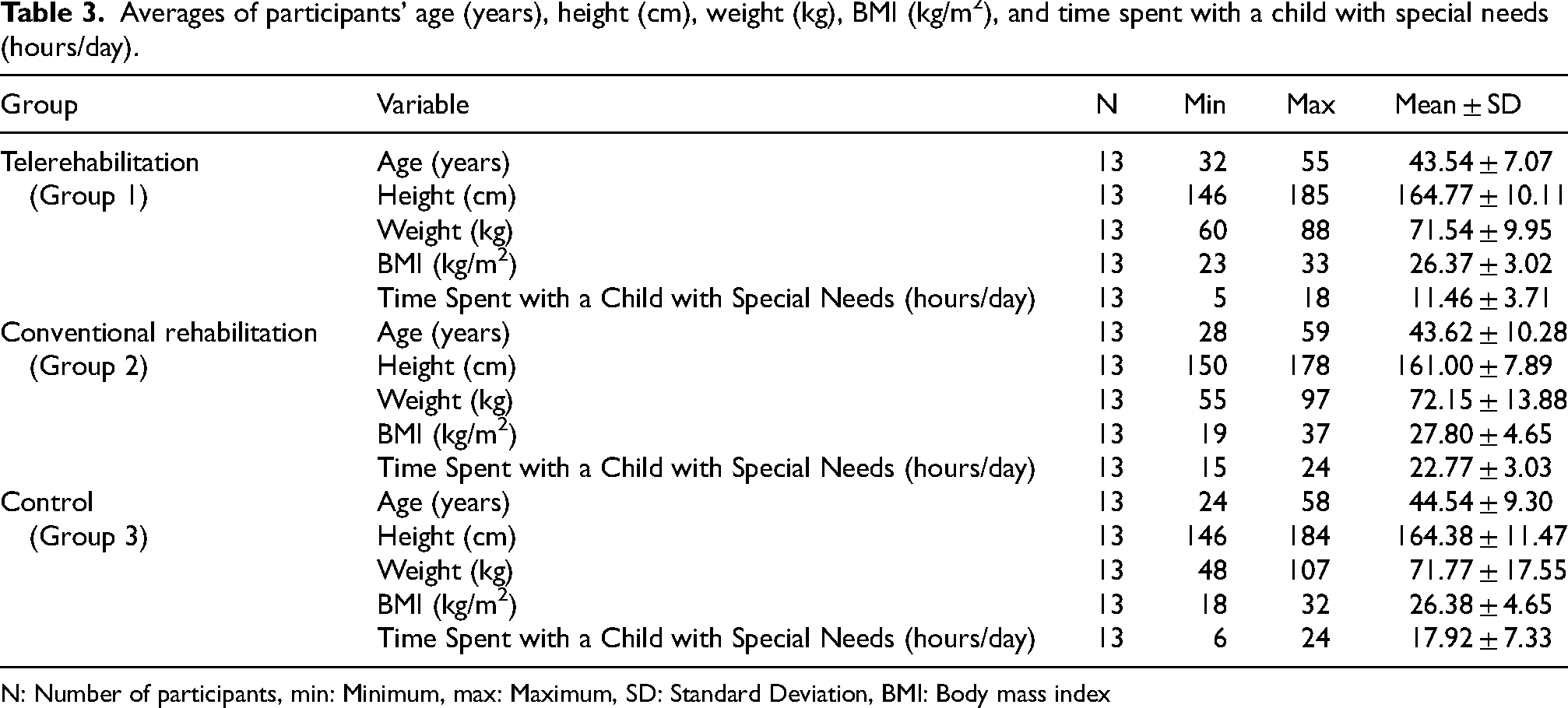
N: Number of participants, min: Minimum, max: Maximum, SD: Standard Deviation, BMI: Body mass index
Table 4 presents the results of repeated measures ANOVA, indicating statistically significant main effects of time and group-by-time interactions (p < 0.001) across all outcome measures, including pain (VAS), fatigue (FACIT-F), quality of life (SF-36), and caregiver burden (CBS).
Comparison of changes in measurement results of groups according to time and group * time.
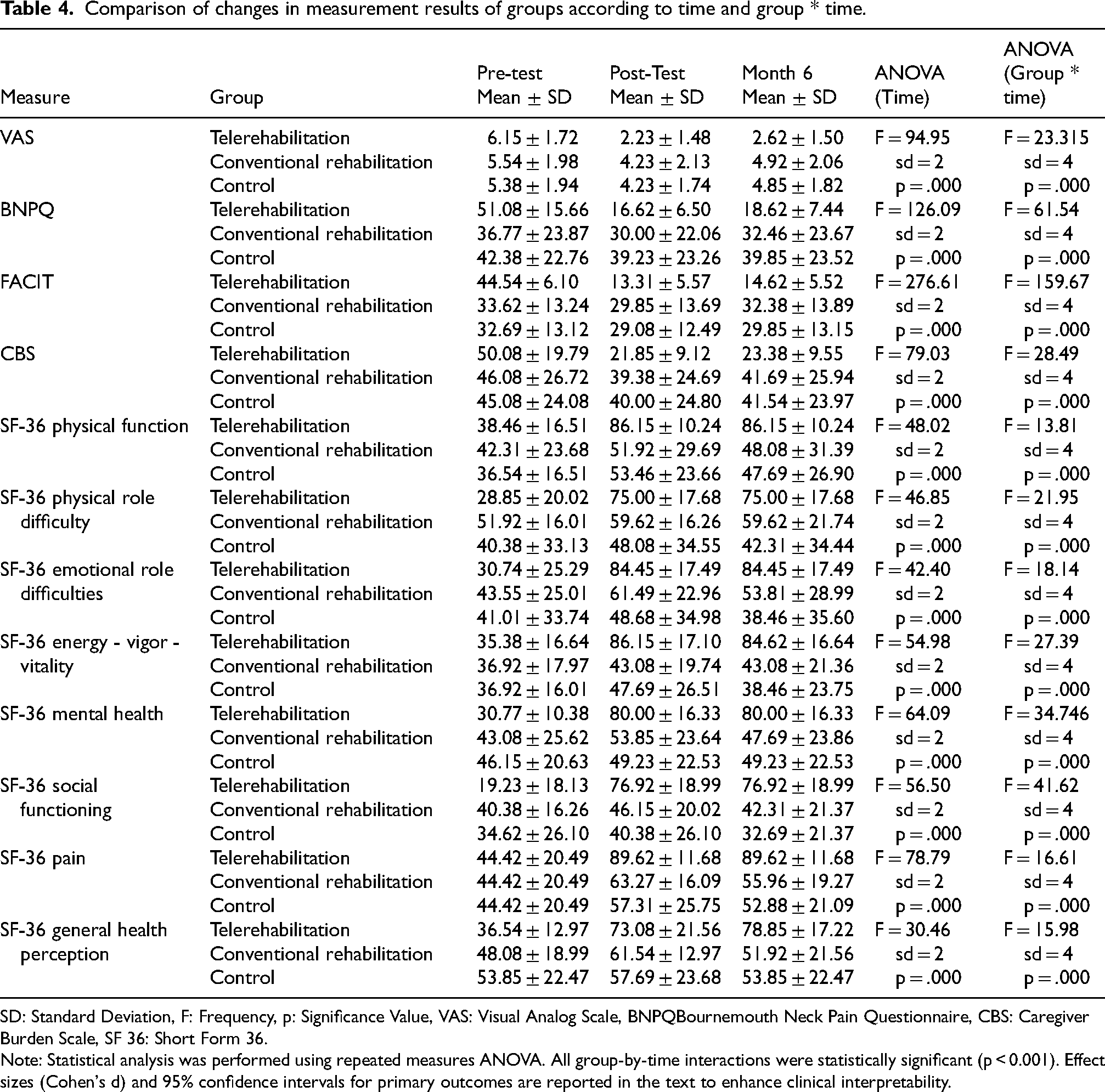
SD: Standard Deviation, F: Frequency, p: Significance Value, VAS: Visual Analog Scale, BNPQBournemouth Neck Pain Questionnaire, CBS: Caregiver Burden Scale, SF 36: Short Form 36.
Note: Statistical analysis was performed using repeated measures ANOVA. All group-by-time interactions were statistically significant (p < 0.001). Effect sizes (Cohen's d) and 95% confidence intervals for primary outcomes are reported in the text to enhance clinical interpretability.
To assess clinical relevance beyond statistical significance, between-group effect sizes (Cohen's d) and 95% confidence intervals (CI) were calculated and are summarized below:
Pain (VAS): Mean difference = −2.61, 95% CI: −4.02 to −1.20; Cohen's d = −1.42 Fatigue (FACIT-F): Mean difference = −27.46, 95% CI: −35.49 to −19.43; Cohen's d = −2.63 Caregiver Burden (CBS): Mean difference = −21.53, 95% CI: −35.84 to −7.22; Cohen's d = −1.16 SF-36 Physical Function: Mean difference = + 38.08, 95% CI: 21.01 to 55.15; Cohen's d = + 1.71
These findings demonstrate that the telerehabilitation intervention produced large to very large effect sizes across key outcomes, confirming both statistical and clinical significance. No adverse events or protocol deviations were observed throughout the study.
Discussion
In the study investigating the effects of telerehabilitation and conventional physiotherapy methods on chronic neck and back pain in caregivers of individuals with special needs, it was observed that the changes in the telerehabilitation group were more significant compared to the other groups. Furthermore, these improvements were largely preserved after six months.
While telerehabilitation has been previously studied in musculoskeletal pain, this study is, to our knowledge, one of the first to directly compare a structured, hybrid telerehabilitation protocol with conventional physiotherapy in caregivers of individuals with special needs—a population that is often overlooked in rehabilitation research. By incorporating validated outcome tools and digital adherence tracking over a 6-month follow-up, the study provides new insight into long-term intervention efficacy in an underserved and clinically unique population.
It was found that the majority of the caregivers participating in the study were female. Upon examination of the relevant literature, it was reported that a similarly high proportion of female participants was observed in the study conducted by Candiri et al.. 25 The caregiving role in most families is assumed by women. This responsibility contributes significantly to chronic neck and back pain, severe fatigue, and reduced quality of life—especially during physically demanding tasks such as lifting, transferring, and prolonged flexed postures required in caregiving. A review of the pre-treatment measurements reveals a correlation between the severity of the observed symptoms and the physical health of the caregivers. In the existing literature, the physical health of caregivers is assessed using a variety of methods, including three-dimensional posture assessments, computer-assisted sensors, the Nordic Musculoskeletal Rating Scale, and specialized scales. While assessment parameters may vary, a review of the literature reveals that caregivers frequently cite pain, fatigue, and quality of life as significant concerns.26,27,28,29 In caregivers of individuals with special needs, postural anomalies and incorrect biomechanics resulting from the interventions they provide, such as meeting the physical needs, assisting with self-care, and transferring the individuals in their care, can lead to chronic neck and back pain and fatigue. These factors impact the daily life of the caregiver, ultimately reducing the quality of life. In this study, telerehabilitation-based exercise training and conventional physiotherapy were employed to enhance the caregiver's quality of life and alleviate symptoms, and their short- and long-term effects were analyzed. Although neck and back pain have distinct clinical and biomechanical profiles, in this caregiver population they often stem from overlapping postural and physical stressors—such as prolonged forward flexion, repetitive lifting, and sustained asymmetric loading. These shared occupational demands justify a unified analytical approach in this preliminary investigation. Nonetheless, this methodological choice may limit condition-specific interpretations, and future research should incorporate stratified analyses to delineate differential responses more precisely.
Given the complex and multifactorial nature of chronic neck and back pain, the therapeutic resources employed in the rehabilitation of these patients are diverse. The literature remains inconclusive on the best treatment approach. In a clinical context, there is a growing tendency to employ therapeutic exercise as a treatment for patients suffering from chronic neck and back pain. 30 The study revealed that there is moderate-quality evidence indicating that exercise during treatment may result in potential clinical benefits. 31 In addition to the existing literature, the findings of this study indicate that patients who received telerehabilitation-based exercise training and a home exercise program exhibited significantly improved outcomes—specifically in pain, fatigue, and quality of life—compared to the control group, who did not engage in any form of exercise. The telerehabilitation group showed meaningful improvements both post-treatment and in long-term follow-up, outperforming the conventional physiotherapy–home exercise group.
Moreover, a significant challenge for caregivers is the difficulty in accessing physical therapy units due to constraints such as time limitations, responsibilities associated with special needs individuals, the necessity of remaining at home, and financial burdens. The findings of this study support that telerehabilitation-based exercise training, delivered remotely without requiring in-person visits, can improve physical health, reduce pain and fatigue severity, and enhance quality of life. A randomized controlled trial reported that telerehabilitation yielded outcomes comparable to those of traditional in-person exercises, suggesting it could be a viable alternative where in-person treatment is not feasible. 32 Other studies have similarly demonstrated comparable outcomes in pain, function, and quality of life when comparing telerehabilitation to conventional rehabilitation.33,34 A meta-analysis on telerehabilitation for neck pain further confirmed its potential to reduce pain intensity and improve disability; however, further research is still needed to fully understand its scope. 35
Notably, a review of the literature revealed no studies offering telerehabilitation-based exercise training specifically for caregivers of individuals with special needs. This study fills that gap by addressing a previously unstudied aspect. Being the first of its kind, it emphasizes the need for further investigation in this population.
Our findings are consistent with prior research demonstrating that telerehabilitation interventions significantly improve pain, fatigue, and quality of life in individuals with musculoskeletal disorders.36,37 Moreover, our study uniquely highlights its effectiveness among caregivers—a population that remains underrepresented in the telerehabilitation literature.
In line with the growing body of literature, recent high-quality studies further support these findings. A 2024 umbrella review by Bargeri et al. demonstrated that telemedicine interventions, including telerehabilitation, provide comparable outcomes to conventional physiotherapy in reducing pain and improving function across various musculoskeletal disorders, including chronic neck and back pain. 38 Similarly, a 2023 randomized controlled trial protocol by Neves Antonio et al. highlighted the potential of telerehabilitation exercises as a non-inferior alternative to traditional care in managing chronic neck pain, emphasizing its feasibility and clinical relevance. 39 Moreover, a 2025 systematic review and meta-analysis by Shi et al. examined mHealth-based physiotherapy interventions for chronic non-specific low back pain and reported significant improvements in both physical and psychological outcomes, supporting the effectiveness of remotely delivered physiotherapy interventions. 40 These results align with the outcomes of our study, underscoring the viability of telerehabilitation as an effective intervention for managing chronic neck and back pain, particularly in caregiver populations who may face access barriers to in-person therapy. Importantly, our study contributes to this growing body of literature by being one of the first to specifically evaluate telerehabilitation in caregivers of individuals with special needs, a group that remains underrepresented in telerehabilitation research.
While subgroup analyses were not feasible due to the limited sample size, the study lacked sufficient power to detect differences across gender, age, or caregiving context.
Telerehabilitation offers a practical solution for caregivers with limited access to in-person physiotherapy services due to time constraints, caregiving responsibilities, or financial limitations. By eliminating the need for frequent facility visits and reducing the logistical burden of transportation, it effectively addresses common barriers to care in this population. Moreover, recent systematic reviews have demonstrated that telerehabilitation can significantly reduce overall healthcare costs while maintaining clinical outcomes comparable to conventional physiotherapy approaches.41–42 Although a formal cost-effectiveness analysis was not conducted, preliminary comparisons of resource utilization suggest that telerehabilitation may offer substantial economic advantages. This finding supports its consideration as a scalable and sustainable intervention model. The telerehabilitation group received fully remote, video-guided exercise training with no use of facility-based resources, staff time, or physical equipment, effectively minimizing operational costs. In contrast, the conventional physiotherapy group required 20 in-person sessions involving supervised electrotherapy and physical modalities, representing a significantly higher consumption of clinical time, infrastructure, and materials. Based on resource use alone, telerehabilitation could reduce direct treatment delivery costs by over 80% compared to conventional interventions. While these are approximate estimations, they underscore the economic feasibility of telerehabilitation and justify the inclusion of structured economic evaluations in future trials.
Additionally, the study employed a comparative approach, contrasting telerehabilitation-based exercise training with conventional physiotherapy. The conventional physiotherapy program included the use of electrotherapy and superficial heat agents. At the end of the treatment phase, the conventional physiotherapy group received a brochure detailing the exercises to continue at home.
Previous studies evaluating the efficacy of electrotherapy and heat agents in chronic neck pain have concluded that, although these modalities may be effective, the level of evidence remains low. Moreover, the results have been inconsistent, underscoring the need for further randomized controlled trials with larger sample sizes to validate these findings.43–48
A comparison of pre- and post-treatment outcomes revealed notable differences between the telerehabilitation and conventional physiotherapy groups, with telerehabilitation demonstrating more favorable results. These findings are in line with existing literature, suggesting that exercise programs delivered via telerehabilitation can exert significant clinical benefits.
In the conventional physiotherapy group, changes in pain localization were observed post-treatment and at follow-up. However, the lack of sustained improvement in fatigue at the six-month follow-up suggests that the effects of conventional therapy may be transient. To ensure long-term treatment efficacy, consistent follow-up and continued engagement with prescribed exercises should be encouraged.
While both groups underwent interventions over the same 12-week period, only the telerehabilitation group received structured supervision and ongoing support throughout the entire duration. In contrast, the conventional physiotherapy group received in-person supervised sessions for just the initial four weeks, followed by eight weeks of unsupervised home exercises without remote monitoring or check-ins. This discrepancy in follow-up intensity and structure may have contributed to the differential outcomes observed between groups and must be taken into account when interpreting the findings.
Although the overall calendar duration was identical, the continuity and depth of supervision varied significantly. This introduces a ‘dosage bias’—a common challenge in pragmatic rehabilitation studies—whereby the telerehabilitation group's superior outcomes may be partially attributed to sustained engagement and oversight, rather than the delivery method alone. Future studies should aim to match supervision intensity across intervention arms or adopt adaptive protocols that account for engagement variability, thereby enhancing internal validity and ensuring balanced treatment exposure.
Moreover, while the inclusion of a non-intervention control group allowed for clearer comparisons with standard care and reflected real-world caregiver challenges, it may have inadvertently contributed to the magnitude of between-group differences due to a lack of therapeutic contact. Future trials could strengthen internal validity by including minimally active comparators—such as digital health education, general wellness programs, or attention-matched teleconsultations—to better account for placebo and expectancy effects and isolate the specific contributions of telerehabilitation. Such designs may also enhance ethical acceptability by ensuring that all participants receive some form of supportive intervention, particularly in vulnerable caregiver populations.
The non-intervention control design, while ethically considerate in minimizing caregiver burden, introduces an inherent expectation bias. Future designs may benefit from attention-matched minimal interventions that preserve ethical integrity while enhancing assay sensitivity to isolate the treatment signal.49,50
Building on this, intervention fidelity in the telerehabilitation group was ensured through a structured, multi-phase delivery model combining asynchronous video-based instruction with periodic live teleconsultations by licensed physiotherapists. Adherence was further supported through automated reminder prompts encouraging participants to confirm session completion. However, the reliance on self-reported adherence data introduces potential recall and social desirability bias. Future research should incorporate objective monitoring technologies—such as wearable sensors, app-based activity trackers, or AI-driven motion-detection platforms—to improve the precision and reliability of adherence metrics and strengthen internal validity.51,52
Importantly, these clinical improvements were not only statistically significant but also clinically meaningful, as confirmed by large effect sizes and narrow confidence intervals across all primary outcomes. Specifically, the calculated Cohen's d values exceeded conventional thresholds for large effects, including d = −1.42 for pain (VAS), d = −2.63 for fatigue (FACIT-F), d = −1.16 for caregiver burden (CBS), and d = + 1.71 for physical functioning (SF-36), each supported by non-overlapping 95% confidence intervals. These magnitudes provide compelling evidence for the high therapeutic impact of telerehabilitation in this population.
As digital health systems evolve, integrating advanced engagement analytics—such as time-stamped session logs, real-time biofeedback, and user-interaction heatmaps—could further enhance adherence evaluation and inform adaptive delivery models. Such technological enhancements may not only optimize implementation fidelity but also facilitate the design of scalable, cost-effective, and patient-tailored telerehabilitation programs. This study contributes to this growing frontier by providing early evidence of feasibility, impact, and digital scalability in an underserved caregiver population.
Limitations
The target sample size was achieved; however, the relatively small cohort, lack of pre-specified subgroup analyses by age and gender, and single-center design may have limited both the statistical power and external validity of the findings. Future studies could benefit from employing stratified randomization or covariate-adjusted models to improve group comparability and analytical precision.
Although effect sizes and confidence intervals were reported to strengthen the interpretability of statistical findings, the relatively small sample size may have introduced wider variability and potentially affected the precision of the estimated confidence intervals. This limitation could restrict the generalizability of the results and underscores the need for future studies with larger, adequately powered samples to confirm the observed effect sizes and establish more stable confidence boundaries.
Another important limitation lies in the difference in supervision intensity across intervention arms. Although the total intervention duration was equivalent (12 weeks) for both telerehabilitation and conventional physiotherapy groups, the telerehabilitation group received continuous digital supervision and structured follow-up throughout the entire period. In contrast, the conventional group had only four weeks of supervised treatment followed by an unsupervised phase. This discrepancy in monitoring intensity may have introduced differential engagement or motivation, thereby potentially influencing outcomes independent of the intervention type, and represents a limitation in internal validity. Future trials should consider matching follow-up intensity across study arms or employing adaptive protocols that control for supervision dosage. Additionally, the use of electrotherapy and physical modalities exclusively in the conventional physiotherapy group—but not in the telerehabilitation group—may have introduced treatment heterogeneity, limiting the ability to isolate exercise-specific effects.
A further methodological limitation is the absence of a formal cost-effectiveness analysis. While the study qualitatively addressed potential economic benefits of telerehabilitation based on reduced resource use and logistical feasibility, no structured economic data were collected. This limits the ability to quantify its cost-benefit profile. Future research should incorporate formal economic evaluation frameworks—such as cost-utility, cost-minimization, or budget impact analyses—to enhance policy relevance and scalability in caregiver populations.
Additionally, adherence tracking in the telerehabilitation group relied on participant self-report, which may introduce recall or social desirability bias. To strengthen internal validity, future research should adopt objective digital adherence tools, such as wearable sensors, app-based logging systems, or motion-sensing platforms.
Because of the limited sample size and the non-stratified design of this study, subgroup analyses were not feasible. While a descriptive review of outcome trends did not suggest systematic differences based on gender, age, or caregiving context, future trials with larger, demographically stratified cohorts are warranted to explore potential moderating effects. Furthermore, while repeated measures ANOVA identified significant group-by-time interactions, no formal post hoc pairwise comparisons (e.g., Bonferroni-adjusted tests) were conducted due to the exploratory nature of the study and the small sample size. This omission limits the ability to precisely determine which specific groups differed at each time point, and should be addressed in future research with larger cohorts.
Furthermore, neck and back pain were analyzed as a combined outcome due to overlapping biomechanical etiologies in caregivers. While this approach was clinically justified, it limits the ability to draw condition-specific conclusions. Future trials should consider disaggregating outcomes by pain localization to identify potentially distinct therapeutic effects.
Finally, the use of a non-intervention control group, while valuable for baseline comparison, may have amplified between-group effect sizes due to the absence of therapeutic contact. This may have introduced expectancy effects that favored the active treatment arms. Future trials could mitigate such bias by employing attention-matched or minimally active comparator interventions, particularly in ethically sensitive caregiver population
Conclusion
This study demonstrated that telerehabilitation-based exercise training resulted in greater improvements in pain reduction, fatigue severity, and quality of life among caregivers of individuals with special needs compared to conventional physiotherapy, with clinically meaningful benefits that were largely sustained at the six-month follow-up. The remote format offers practical advantages for caregivers with limited access to in-person therapy due to caregiving responsibilities, mobility issues, or long waiting times, making it a viable and resource-efficient alternative to traditional care.
These findings contribute to the emerging literature on digital health interventions by offering one of the first randomized controlled evaluations of telerehabilitation in caregivers of individuals with special needs—a population largely underrepresented in rehabilitation research. By addressing this gap, the study provides novel evidence supporting the use of structured, remotely delivered physiotherapy in improving musculoskeletal outcomes and caregiver well-being.
Nonetheless, the generalizability of these findings is constrained by the single-center design, modest sample size, lack of demographic stratification, and differences in supervision intensity between groups. Therefore, the results are most applicable to caregiver populations with similar demographic and clinical characteristics to those studied here. These factors should be taken into account, and the findings interpreted with caution.
Future research should include larger, multi-center, demographically stratified trials to enhance external validity, explore the moderating role of gender, age, and caregiving context, and incorporate formal cost-effectiveness analyses to inform policy and support scalable implementation of telerehabilitation in diverse caregiver populations. Beyond its clinical efficacy, telerehabilitation also holds promise as a cost-conscious rehabilitation model. Its scalability and potential to reduce healthcare resource utilization underscore the importance of integrating structured economic analyses into future trials.
Footnotes
Acknowledgements
The authors thank the Inonu University Scinetific Research Projects Coordination Unit (BAP) for supporting project No. TCD-2021-2666.
Credit authorship contribution statement
Ethics committee approval
This study was approved by the Malatya Clinical Research Ethics Committee during its meeting on March 3, 2021, under decision number 2021/85. Written informed consent was obtained from all participants before their involvement in the study. The protocol was carried out in accordance with the principles outlined in the Declaration of Helsinki. The study was registered in the ClinicalTrials.gov registry (Study Identifier: NCT06095336).
Informed consent
All participants gave their informed consent, please see Ethical Aspects of the Study 2.6.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Inonu University Scientific Research Projects Coordination Unit (BAP) under the project number TCD-2021-2666.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Sharing Statement
Data information can be obtained from the author on request.