
Abstract
Background
Maintaining the correct posture is very important for students who spend most of the day at desks and tables.
Objective
This study aimed to determine the effect of ergonomics training given to university students on their musculoskeletal system, postural habits, and awareness, and ergonomic risk score evaluated by the REBA (rapid entire body assessment) method.
Method
A total of 130 university students participated in the study. The students were divided into two homogenized groups: intervention (65) and control (65). Only the intervention group received ergonomics training. All students were administered a semi-structured sociodemographic questionnaire, Cornell Musculoskeletal Discomfort Questionnaire (CMDQ), and Postural Habits and Awareness Scale (PHAS) at the beginning of the study. The Rapid Whole Body Assessment (REBA) was used to assess ergonomic risk. Ergonomics training was given to the intervention group. In the evaluation of static endurance of the core muscles, the trunk flexor endurance test, the trunk extensor endurance test, and the time spent in the right-left lateral bridge test positions were calculated. The evaluations were repeated immediately after the training and 1 month after.
Results
Following the training, no statistically significant differences were found between the CMDQ, PHAS, and core muscle endurance measurement groups. Additionally, ergonomics training was effective in reducing regional musculoskeletal complaints, decreasing ergonomic risk scores, and enhancing positional awareness.
Conclusion
Ergonomics training should be utilized to gain correct posture habits and reduce musculoskeletal disorders.
Introduction
The IEA [International Ergonomics Association] defines ergonomics as a discipline concerned with understanding the interaction of system factors with individuals and a science that applies theories, principles, and techniques to ensure their complete mental and physical well-being and full performance. 1 Ergonomic risk factors cover different areas, such as physical, environmental, individual, and psychological factors. Physical factors include carrying heavy loads, working from heights, standing or sitting for long periods, and squatting. 2 As a result of asymmetrical, inappropriate, long-term postures, tissues are overloaded and exceed the tolerable stress threshold. This can lead to musculoskeletal imbalances and overstrained injuries.3,4 Musculoskeletal disorders include degenerative and inflammatory conditions that affect tendons, muscles, bones, nerves, ligaments, and joints. These can frequently occur as a health problem. It is known that musculoskeletal disorders are high in working individuals, and in recent years, especially in university students, this situation has led to negative consequences. 5 Repetitive movements of the upper extremities in a fixed and generally poor posture within a limited space inevitably lead to problems in the musculoskeletal system. 6 With the activation of core muscles, our body maintains postural stability in the trunk with central key point control. Adequate trunk control is necessary to maintain body position and to ensure control when body position changes. It also plays an important role in mobility function and in performing activities of daily living. 7 If the strength and endurance of the muscles in the core area are low, it causes excessive physiological stress on the passive structures of the spine. 8 These passive structures consist of structures such as vertebrae, facet joints, intervertebral discs, spinal ligaments, and joint capsules. 9 The stability of the spine requires both passive rigidity through bone and ligament structures and active rigidity through muscles. A bare spine, not attached to muscles, cannot bear most compressive loads. 10 Spinal instability occurs if any of these components fail. In this case, pain may occur throughout other structures of the body and impair functional performance. 8 For example, excessive external loads on the disc may be caused by weak muscle control, which can lead to a vicious cycle where the disc no longer provides optimal passive resilience or stability. 10
Working position and posture have a vital role in musculoskeletal disorders. Therefore, the urgency of the risk levels arising from inappropriate body postures and the measures to be taken in this regard should be determined. 11 Many techniques are used when analyzing working postures. One of the appropriate methods when analyzing working postures is REBA (rapid entire body assessment), developed by Hignett and McAttamney (2000). This method allows the analysis of all body parts and is practical. It explains the risk associated with a work posture or movement that is planned to be analyzed using numerical data. REBA considers the loading that occurs in dynamic or static postures and the interaction between the load and the human being, and evaluates the postural risk of the body as a whole. Thus, reducing discomfort-related risks before and after the improvement can also be evaluated. 12 Student life includes long periods spent at school, most of which are spent sitting. 13 Therefore, it is essential to draw attention to the risks of working in a sitting position for long periods and to provide training on ergonomic sitting principles. 14 In the study conducted by Altuğ (2019) on students, it was observed that with the training on the back and lumbar posture, knowledge in this field increased. 13 Pain related to the musculoskeletal system is associated with learned posture and habits, and musculoskeletal pain occurring in older age is related to pain experienced in earlier life. Therefore, addressing this problem during the university years is particularly important for young adults in terms of awareness and prevention. 15
Although studies in the literature include such training programs in various professions16,17,18 and student groups, 13 no study examines the effect of face-to-face ergonomics training on postural habits and awareness among university students. Furthermore, no study has been found that examines the effect of ergonomics training on the level of ergonomic risk using the REBA method. The implementation of ergonomics training is essential in preventing musculoskeletal disorders that may occur, especially in situations requiring prolonged static postures, as the knowledge acquired in training applies to both daily life and working life. 19 For these reasons, the study aimed to determine the effects of planned ergonomics training on musculoskeletal complaints, postural habits and awareness, and ergonomic risk level of university students.
Methods
Participants
The study was conducted with students from a university's Vocational School of Health Services in a northeast province of Turkey. It was completed with 130 students: 65 in the intervention group and 65 in the control group. Institutional permission was obtained from the University where the research was conducted (October 16, 2023, E-16890724-044-1706), and ethical approval for the study was granted by the university's Clinical Research Ethics Committee (October 25, 2023, 2023-114). Written informed consent was obtained from the participants who agreed to participate in the study using the “Informed Consent Form.”
Exclusion/ İnclusion criteria
Only female students were included in the study due to the higher incidence of musculoskeletal disorders in the female gender 20 and differences in anthropometric characteristics and muscle strength. 21 Female students over 18 who had passed the anatomy course were included in the study. The study did not include students undergoing treatment for musculoskeletal problems or students with orthopedic deformities.
Study design
The study is a randomized controlled intervention doctoral thesis study conducted between October 2023 and January 2024. Students in the intervention group received ergonomics training, while students in the control group did not receive any training. Before the training, a semi-structured questionnaire (including age, Cornell Musculoskeletal Disorder Questionnaire (CMDQ), postural habits, and awareness scale) was applied to the students in both groups. Tests assessing the static endurance of the core muscles (trunk flexion test, trunk extension test, lateral plank test) were evaluated by the researcher. Ergonomic risk levels were determined by the researcher using the REBA method. The evaluations were repeated immediately after the 2-week ergonomics training and 1 month after (Figure 1).
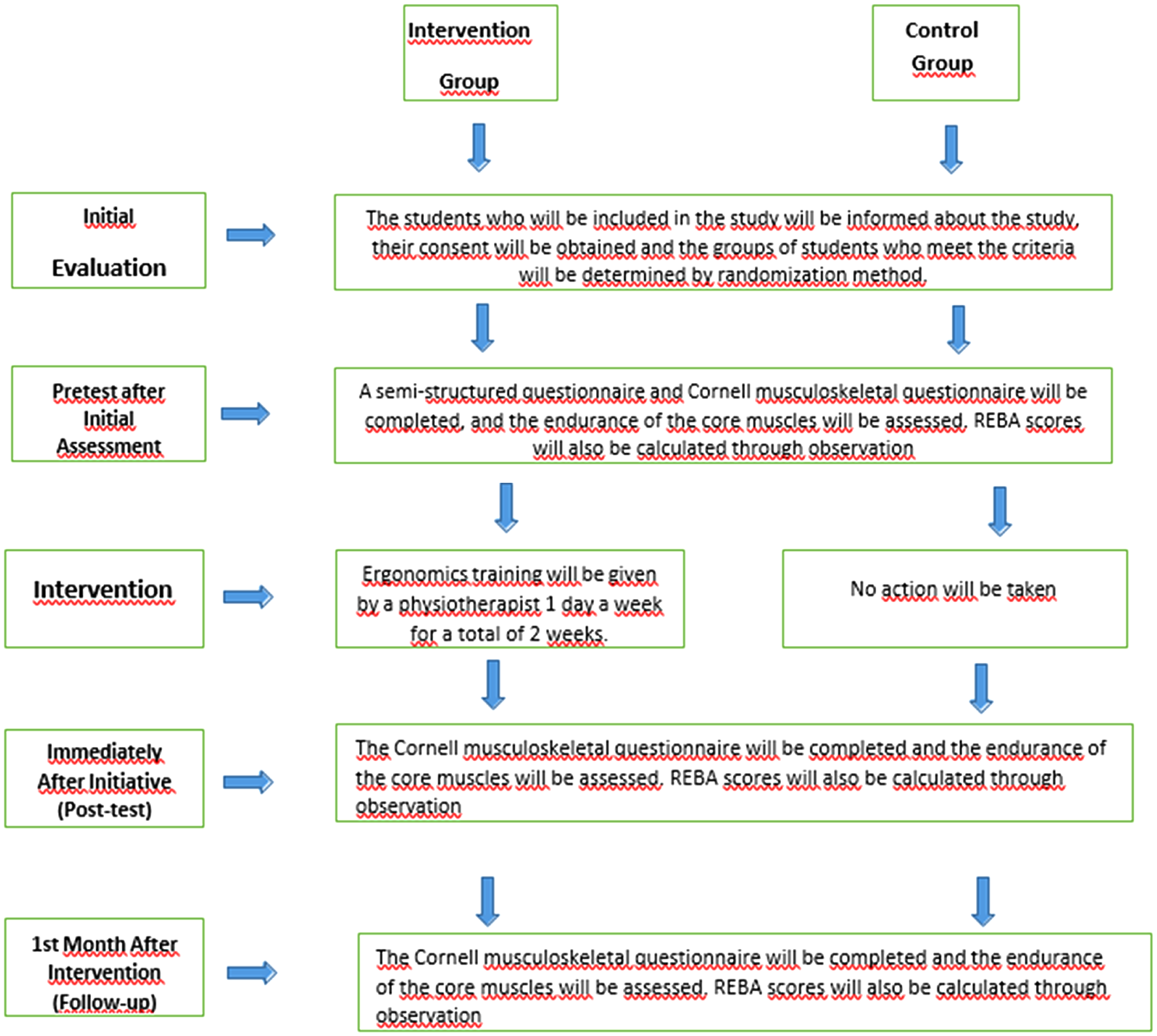
Research implementation scheme.
Application
Ergonomics education
The training content was transformed into a presentation using the Microsoft PowerPoint program. The training was given to the students face-to-face by the researcher's physiotherapist in the application classrooms of the university where the study was conducted. The training aimed to cover topics such as the basics of ergonomics, human anatomy, and preventive procedures to minimize the risk of musculoskeletal disorders, including safe working postures and the possible consequences of incorrect postures. The training days were planned to occur on different days outside of class hours according to the availability of all students in the intervention group (65 people). To increase the effectiveness of ergonomics training, the students who would receive training were divided into three groups, and Students were included in one of these three groups according to their availability in the course program. Students participated in the training for 2 weeks, one day a week for two hours. The exercises in the training content were practically shown to the students. Students were advised to comply with ergonomics principles and incorporate exercises into their daily lives.
Measurement parameters
Semi-structured question form
In the semi-structured questionnaire, individual characteristics were collected using a 10-question survey that included gender, age, the number of hours spent in class per week, the number of hours spent in sports per week, the duration of exposure to students’ static posture, such as ergonomic training, and factors that may cause musculoskeletal disorders.
Cornell musculoskeletal discomfort questionnaire
In the study conducted by Erdinç and colleagues, the scale was adapted to Turkish, and a reliability study was conducted. 21 The Cronbach Alpha reliability coefficients of the scale were found to be 0.87, 0.89, and 0.87. The CMDQ is a questionnaire form that questions the severity, periodicity, and impact on the workability of musculoskeletal problems in different parts of the body. High scores indicate increased musculoskeletal problems. 22 Permission to use the scale was obtained.
Postural habits and awareness scale (PHAS)
This scale was developed by Bayar et al.(2002). The Cronbach Alpha reliability coefficient of the scale was found to be > 0.85. This scale aims to determine the self-perceptions of healthy adults regarding their postural habits and awareness. 23 Permission to use the scale was obtained.
Rapid entire body assessment (REBA)
The REBA method assesses a person's body posture during work and evaluates the level of difficulty they encounter while performing the job. In this way, the areas where the individual has difficulty are identified, and what attention should be paid to prevent musculoskeletal disorders in the workplace is determined. The method evaluates postures in the torso, upper arms, legs, neck, wrists, and lower arms, considering the flexion, bending, and loads that occur during the working posture. As a result of this evaluation, a score ranging from 1 to 15 is determined for each region. 24
Physical measurement and evaluation method
Tests, including body flexion and extension and lateral bridge tests, measured static endurance of the core muscles.
Trunk flexion test
Students are positioned in a supine position with their hips and knees flexed at 90 degrees and their trunk flexed at 60 degrees. The physical therapist supports the student's feet and stabilizes them. The test is terminated when the student's trunk position deteriorates or when the student indicates that they cannot continue the test.
Trunk extension test
Students were placed in a prone position with the pelvis, hips, and knees on the bed. The evaluating physical therapist stabilized the student's lower extremities and asked the student to hold their arms in a cross position over the trunk. The test was terminated when the student's trunk fell below the bed level or when the student indicated they could not continue the test.
Lateral bridge test
This test was performed separately for the right and left sides. Students were positioned on their side, with the arm being assessed held straight, the elbow flexed at 90 degrees, and the upper extremity crossed over the torso. Students were asked to lift their bodies on their forearms and toes and maintain this position. The test was terminated when the student was unable to maintain a straight body position or when their hips fell toward the bed.
During the tests, the time participants spent in the designated positions was recorded using a stopwatch. Each test was terminated when the participant broke the position or indicated they could not continue. 25
Evaluation of data
The data obtained in the study were analyzed using SPSS (Statistical Package for Social Sciences) for Windows 22.0 program. Number, percentage, mean, and standard deviation were used as descriptive statistical methods to evaluate the data. Differences between the rates of categorical variables in independent groups were analyzed with the Chi-Square and Fisher's exact tests. An independent group t-test was used to compare continuous quantitative data between two independent groups. Repeated measures, the ANOVA test, and the complementary Bonferroni test were used to compare within-group measurements.
Results
Sociodemographic profile
While there was no statistical difference between the control and intervention groups in terms of age, weight, height, BMI, number of hours of sitting lessons per week, and total number of hours of sports per week (p > 0.05), the duration of using TV, computer and telephone while sitting at home was higher in the intervention group compared to the control group (p < 0.05) (Table 1).
Distribution of sociodemographic characteristics of the students.
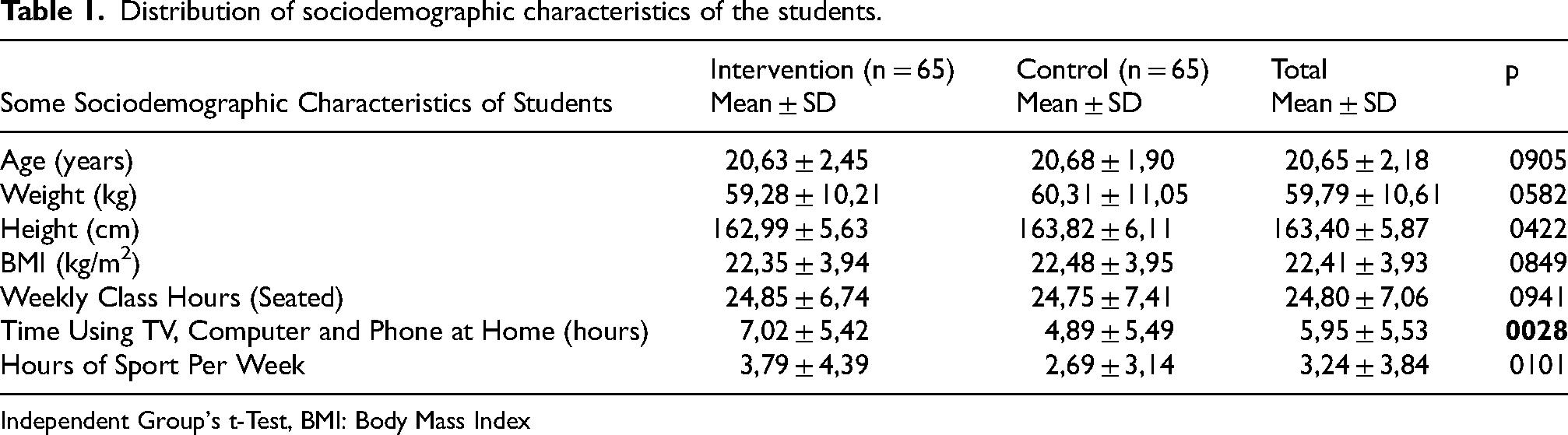
Independent Group's t-Test, BMI: Body Mass Index
Postural Habits and Awareness
In the intervention group, positional awareness measurements immediately after the training were higher than in the control group (p < 0.05). At the same time, ergonomic awareness measurements immediately after the training and 1 month after the training were higher in the control group than in the intervention group (p < 0.05) (Table 2).
Distribution of postural habits and awareness scale mean scores according to study groups and measurement time.
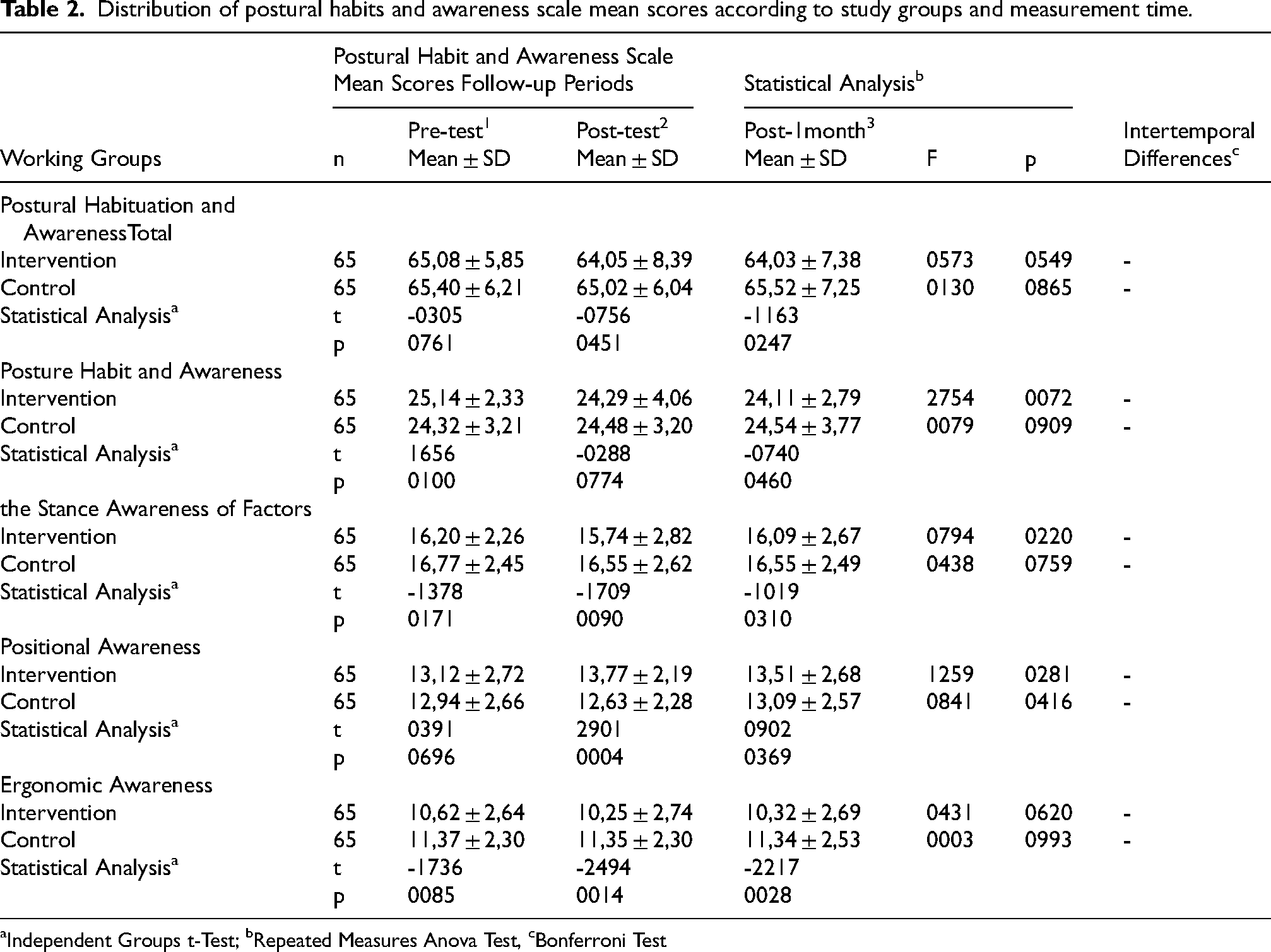
Independent Groups t-Test; bRepeated Measures Anova Test, cBonferroni Test
Core Muscle Endurance Test
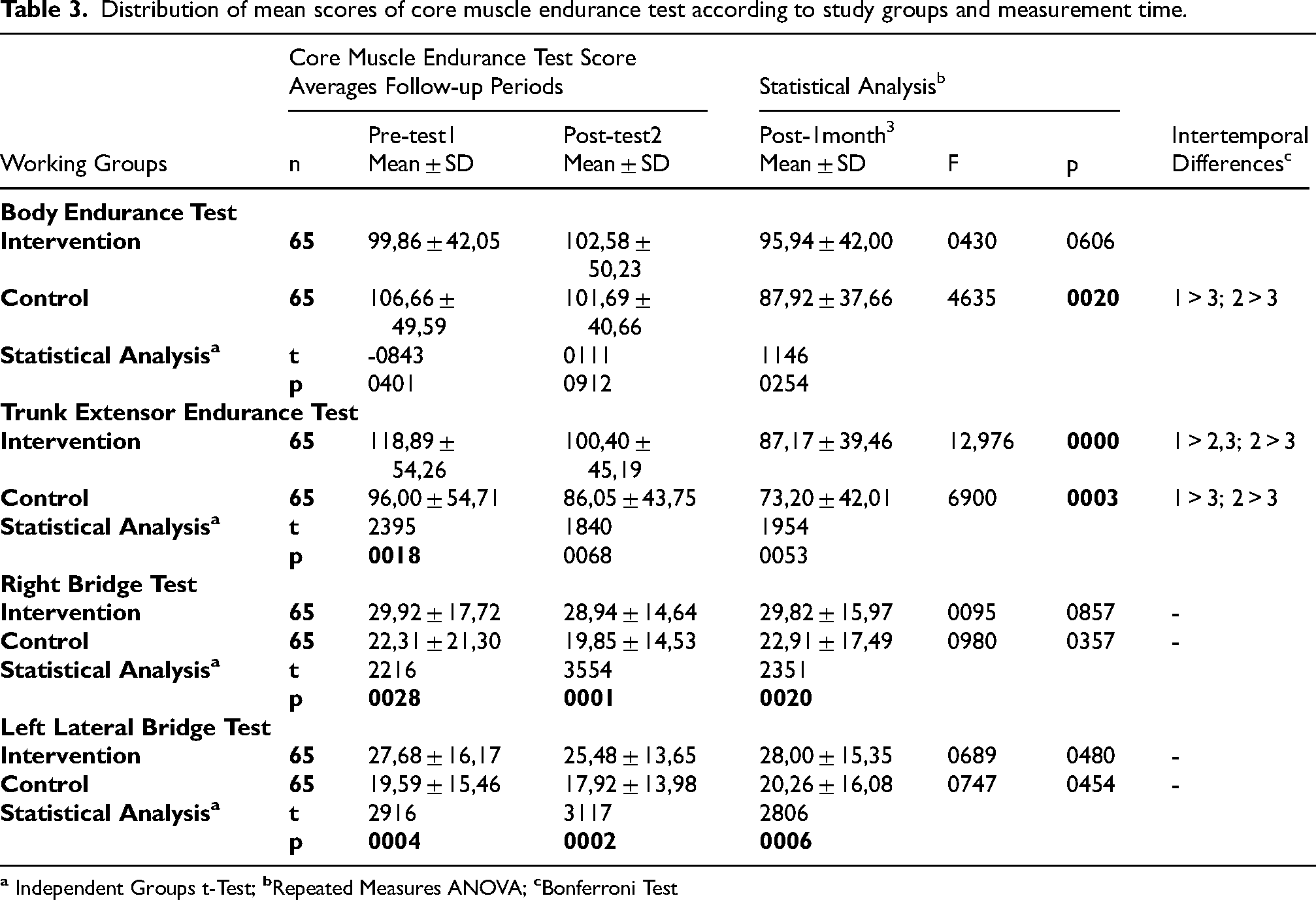
The trunk extensor endurance test, proper lateral bridge test, and left lateral bridge test pre-training measurements were higher in the intervention group compared to the control group (p < 0.05). The measurements of the students’ right and left lateral bridge tests immediately after the training and 1 month after the training were higher in the intervention group compared to the control group (p < 0.05). In the control group, the decrease in trunk flexor endurance test and trunk extensor endurance test measurements 1 month after training was significant compared to pre- and immediate post-training measurements (p < 0.05). In the intervention group, the decrease in the trunk extensor endurance test both immediately after the training and 1 month after the training was found to be significant compared to the pre-training measurements (p < 0.05) and the decrease in the measurement 1 month after the training was found to be significant compared to the measurement after the training (p < 0.05) (Table 3).
Distribution of mean scores of core muscle endurance test according to study groups and measurement time.
REBA Risk Assessment
There was no significant difference between the intervention and control groups in the REBA risk measurements of the students before the training (p > 0.05). In the intervention group, REBA risk measurements immediately after the training and 1 month after the training were lower than those of the control group (p < 0.05). In addition, a decrease was observed in the intervention group immediately after the training and 1 month after the training compared to before (p < 0.05). This decrease in the intervention group was more significant in the measurement 1 month after the training compared to the measurement immediately after the training (p < 0.05) (Table 4).
Distribution of mean REBA risk scores according to study groups and measurement times.
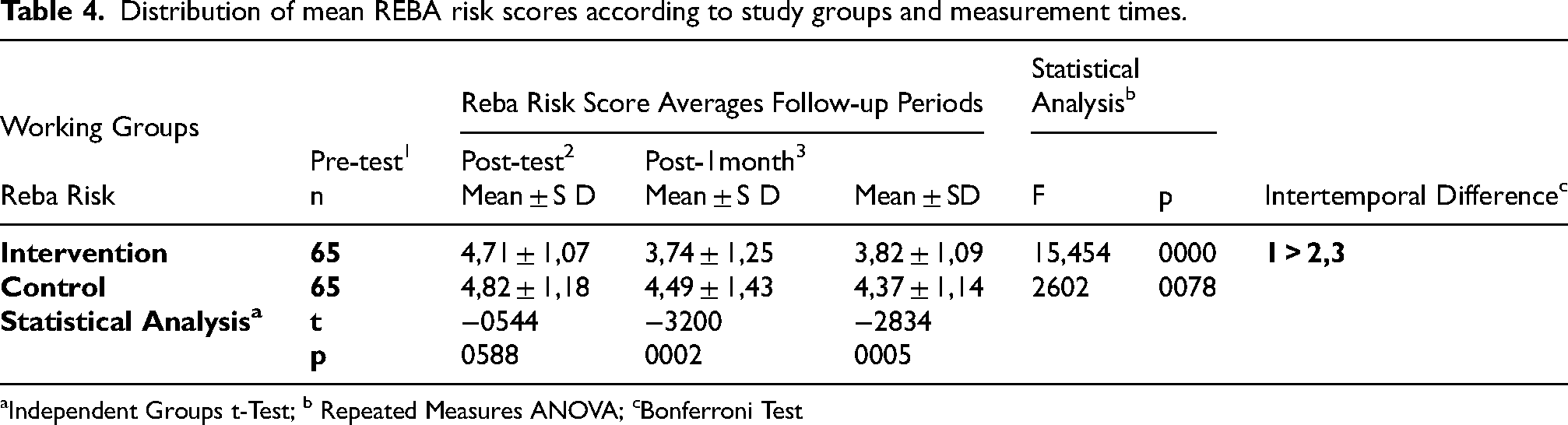
Independent Groups t-Test; b Repeated Measures ANOVA; cBonferroni Test
Spine, upper extremity, lower extremity, and total weighted cornell score averages
Cornell's total weighted score measurements before, immediately after, and 1 month after the training showed no difference between or within groups (p > 0.05) (Table 5).
Distribution of spine, upper extremity, lower extremity and cornell total weighted score averages according to study groups and measurement times.
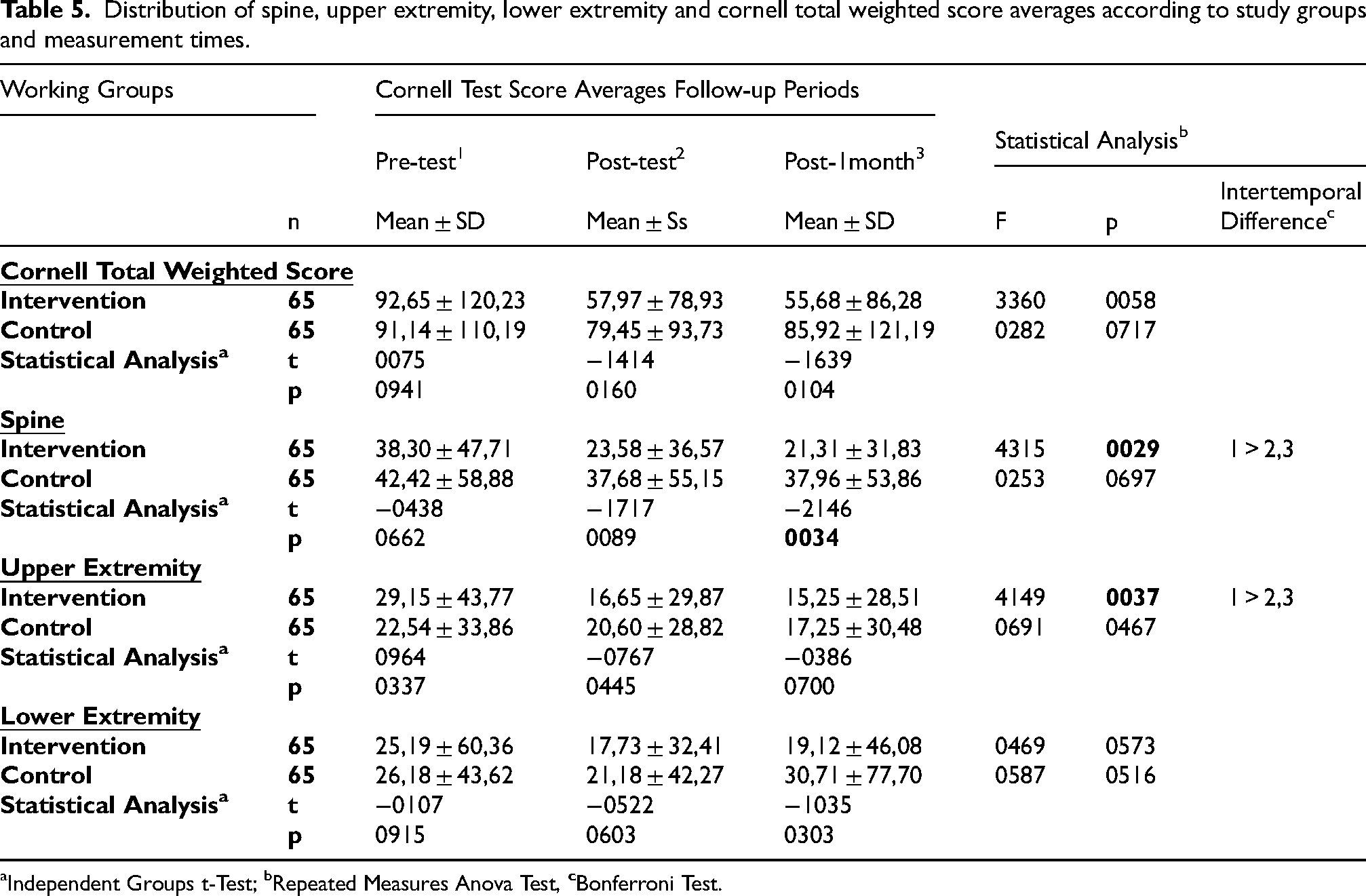
Independent Groups t-Test; bRepeated Measures Anova Test,
While there was no difference between the Cornell spine measurements of the students before and immediately after the training (p > 0.05), the Cornell spine measurements 1 month after the training were lower in the intervention group compared to the control group (t(128) = -2.146; p = 0.034 < 0.05). Cornell spine measurements 1 month after the training were higher in the control group (x̄ = 37.962) compared to the intervention group (x̄ = 21.308). In the intervention group, the measurements immediately after the training and 1 month after the training were found to be lower than the spine measurements before the training (p < 0.05), while there was no difference between the measurements in the control group (p > 0.05).
There was no difference in the Cornell upper extremity measurements of the students before, immediately after, and 1 month after the education (p > 0.05). In the intervention group, Cornell's upper extremity measurements immediately after training and 1 month after training were found to be lower compared to the measurements before training (p < 0.05). However, in the control group, no difference was found between the measurements (p > 0.05).
According to the group, there was no difference between the students’ lower extremity measurements before, after, and one month after the training (p > 0.05), and there was no difference between the measurements in the intervention and control groups (p > 0.05).
Discussion
This study was conducted to determine the effect of ergonomics training programs given to university students on musculoskeletal complaints, postural habits, and awareness, and to evaluate their effect on ergonomic risk scores.
The two groups’ similar daily living habits contributed to the objective interpretation of the educational effectiveness and other evaluation criteria applied in the study. On the other hand, in the intervention group, the duration of sitting in the home environment and using television, computers, and telephones was higher than in the control group. These results indicate that students in both the intervention and control groups maintained a static sitting posture for extended periods throughout the day. The study by Woo et al. (2016) shows that university students aged 18–25 years who use mobile phones are associated with musculoskeletal problems, especially in the neck and shoulder region. With the spread of such problems, it is emphasized that frequent use of electronic devices and poor postural habits lead to these disorders. In this context, it is reported that university students require ergonomics training and informative programs.26,27,28 Our findings showed that the spine (including the back, waist, and neck) was the musculoskeletal region with the most aches, pains, and discomfort in both groups, both before and after the training. Musculoskeletal disorders can occur when sitting ergonomically and when the ideal posture is not maintained, and they are often manifested by back pain. 29 This study observed a decrease in the total weighted Cornell score from all body parts of the intervention and control groups after the training. Still, this situation was found to be more effective in the group receiving ergonomics training than in the group immediately after the training and the group not receiving training.
Additionally, the decrease in intra-group spine and upper extremity Cornell scores was found to be significant in the group receiving training. These results show that ergonomics training can be practical for musculoskeletal system disorders. In the literature, many studies examine the relationship between the time spent at a desk and computer and musculoskeletal disorders. The studies emphasise a linear relationship between computer usage time and physical ailments 30 ; neck and right shoulder pain are associated with computer usage time. 31 It may pose a risk for upper extremity musculoskeletal Disorders. 32 However, a study examining lying down and standing found that the load on the spinal discs was higher during sitting, and prolonged sitting was associated with the risk of lower back pain. 33 For these reasons, it is stated that ergonomics training serves as a protective mechanism for the musculoskeletal system and effectively prevents disorders before they occur. 34 In this respect, some studies support our findings. Studies have shown that creating ergonomic awareness by applying ergonomics education in children can reduce musculoskeletal disorders, 35 ergonomic awareness programs can provide positive effects on health in young age groups, 13 ergonomic approaches are effective in reducing work-related low back pain, 36 ergonomics training given to computer users provides a reduction in musculoskeletal disorders in the neck and upper extremities, 37 and ergonomics training in musculoskeletal complaints related to computer use can reduce symptoms in the long term. 38 Many studies in the literature support these findings and emphasize that ergonomics training is an effective strategy for preventing and reducing musculoskeletal disorders.39,40,41
Ergonomics training contributed to the development of positional awareness. This emphasises the importance of acquiring healthy postural habits in the training content. 42 However, the unexpected increase in ergonomic awareness in the control group may have resulted from the fact that the students were able to distinguish unhealthy conditions because they were studying in the health department, were influenced by their friends who received training, or that the subject was investigated because the study aroused curiosity. The researchers stated that poor posture that persists for a long time can lead to musculoskeletal problems; therefore, it is crucial to intervene in the early stages. University students are also generally exposed to risk factors such as prolonged sitting, inadequate ergonomics in work environments, and excessive use of electronic devices. These behaviors can significantly contribute to the development of musculoskeletal pain, particularly in the neck, shoulders, and lower back, and can reduce an individual's quality of life, physical functioning, and academic performance. 43 Studies have emphasized that ergonomic training has positive effects on work-related musculoskeletal disorders and posture. 44 In this context, the ergonomics training given to the students in our study will successfully prevent posture problems that they can correct during activities such as writing and listening to lectures. This training can be an effective tool in protecting musculoskeletal system health and improving quality of life by helping individuals correct their posture. These findings support the importance of emphasizing ergonomics education and early intervention to prevent postural problems. Developing ergonomic awareness, especially from a young age, may reduce musculoskeletal problems and form healthy living habits.
It was observed that all trunk endurance test values of the students decreased after ergonomics training. This decrease was statistically significant in the control group for the trunk flexor endurance test and in the intervention and control groups for the trunk extensor endurance test. The decrease in the right and left lateral bridge test values was statistically significant in the control group compared to the intervention group. This situation may be attributed to the fact that right and left lateral bridge test values were lower in the control group compared to the intervention group, even before the training. Studies have shown that sitting in an upright position for a long time without support can be difficult because well-balanced trunk muscle strength and endurance are required to maintain proper posture, and sitting in an uncomfortable position for a long time can lead to an increase in joint load, causing pain and various musculoskeletal diseases, 45 that low muscle endurance will cause a decrease in work performance in jobs that require long-term continuity, 13 and that there is a significant relationship between trunk muscle endurance and static balance in male students. 46 It is crucial for students who remain in a static posture (sitting) for long periods to have sufficient endurance to maintain their posture and listen to lectures efficiently.
In our study, while the REBA risk score before the training was the same between the intervention and control groups, a significant decrease was observed in the risk score after the training and 1 month after the training in the trained group. The decrease in the ergonomic risk score is the effect of the ergonomics training provided. Upon examining the studies conducted, no study was found that evaluated the effectiveness of ergonomics training in students using the REBA method. However, there are studies evaluating the effectiveness of ergonomics training using the REBA method in different occupational groups. Studies have found that ergonomics training is effective in reducing the REBA risk score.47,48,49 These studies are similar to our study in that they show that ergonomics training is effective in reducing the REBA risk score.
Conclusion
This study was conducted on students enrolled in a department at a university and concluded that ergonomics training would reduce musculoskeletal complaints and ergonomic risk levels. However, conducting studies specific to students at different universities and departments would contribute to the literature. Extending this study, which is limited to university students, to students in younger age groups could help determine the effectiveness of ergonomics training and contribute to raising awareness at an early age by integrating it into educational programs. Furthermore, the fact that the exercises described in the ergonomics training content in this study were given as a home program and that it was not possible to monitor whether students performed them regularly could lead to different results in terms of musculoskeletal complaints, pain levels, and muscular endurance among students. The decrease observed in both MSDs and REBA risk scores after ergonomics training suggests that MSD complaints may be related to prolonged incorrect static postures. Therefore, further studies would be beneficial.
Footnotes
Ethical statement
The research was carried out according to the guidelines in the Declaration of Helsinki and the ethical rules specified in the ethics committee of Avrasya University between November 2023 and January 2024. Ethical permission was received from Avrasya University Clinical Research Ethics Committee (2023\15), and institutional permission was received from the relevant units (16.10.2023). Students approved the informed consent form before filling out the forms.
Informed consent
Before the data collection started, written informed consent was required and collected from all individuals who participated as informants in the study.
Authors contributions
Gamze ATALI, Füsun TERZİOĞLU contributed the conception and design of the study, acquisition of data, analysis and interpretation of data; drafting the article, revising it critically for important intellectual content, final approval of the version to be submitted. However the authors in the article were listed according to their contribution rates to the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Authors elects to not share data of this study
Generative artificial intelligence (ai)
Artificial intelligence was not used.