
Abstract
Background
Repetitive hand movements during mobile device use, such as texting and typing, may lead to cumulative stress on hand structures and result in musculoskeletal conditions with potential surgical relevance. The increasing ubiquity of smartphone use raises concern for the development of overuse injuries, particularly among younger individuals and high-frequency users.
Objective
To systematically review and characterize surgically relevant hand and wrist pathologies associated with mobile phone use.
Methods
We conducted a systematic search of Embase, PubMed, and Scopus using terms related to mobile device use (e.g., “texting,” “smartphone”) and hand conditions requiring or potentially requiring surgical intervention (e.g., “de Quervain,” “trigger thumb”). Studies were included if they reported hand or wrist injuries in mobile device users with surgical implications. Studies unrelated to hand anatomy or lacking relevance to surgical pathology were excluded. Abstract and full-text screening were followed by data extraction.
Results
Of 588 articles initially identified, 42 met inclusion criteria, representing over 67,000 individuals. The mean age across studies was 24.6 years. The most commonly reported surgically relevant conditions included de Quervain's tenosynovitis (n=9), carpal tunnel syndrome (n=6), tendinitis (n=4), and trigger finger (n=1). Across studies, increased mobile phone use was associated with a higher risk of developing these pathologies.
Conclusions
As mobile device usage continues to rise, recognition of surgically relevant hand injuries is essential. Preventive strategies and ergonomic interventions may reduce the burden of these injuries, particularly in younger and high-use populations.
Keywords
Introduction
Mobile phone use has become increasingly prevalent, with more than 50% of children engaging with mobile phones before the age of one, and exposure reported as early as two months of age. 1 This early and prolonged exposure, spanning both pediatric and adult populations, raises important concerns about the potential musculoskeletal implications for the hand. 2 Among adolescents and young adults, sustained device use may contribute to the development of advanced musculoskeletal disorders, including those requiring surgical intervention. In occupational settings, where mobile devices are frequently integrated into daily workflows, identifying usage thresholds and associated diagnoses is critical for guiding ergonomic standards, occupational health evaluations, and employer-led prevention strategies.
Literature review
As mobile phone use has become ubiquitous across all age groups and occupations, concerns about its impact on musculoskeletal health have grown. Numerous studies have identified associations between frequent phone use and both upper extremity and postural conditions, including neck strain, cubital tunnel syndrome, and hand or wrist disorders such as carpal tunnel syndrome, De Quervain's tenosynovitis, osteoarthritis of the carpometacarpal joints, and “gamer's thumb”.3–5 These injuries can compromise occupational performance, reduce functional capacity, and result in substantial healthcare utilization.
Prior research has largely focused on symptom severity, ergonomic risk factors, or behavioral patterns of use, often relying on tools like the Smartphone Addiction Scale–Short Version (SAS-SV). 6 Higher scores on this scale have been linked to increased reports of wrist pain, reduced grip strength, and greater likelihood of musculoskeletal complaints such as hand and wrist pain, particularly among adolescents and young adults with extended daily use.7–9 These behavioral patterns may lead to chronic strain and structural injury, increasing the risk of developing conditions such as De Quervain's tenosynovitis and carpal tunnel syndrome.2,10–13 Preventive strategies including posture education, microbreaks, and stretching exercises have been proposed, reflecting the field's growing awareness of this emerging risk factor. 14 However, while the literature increasingly acknowledges musculoskeletal strain related to mobile technology use, fewer recent studies specifically examine hand pathologies requiring surgical management.
Additionally, prior systematic reviews have characterized the broad relationship between mobile phone use and musculoskeletal pathology. Yaghmour et al. reported that sending 55 or more text messages per day may be associated with increased risk of hand pain and tendinopathy. 15 Similarly, Zirek et al. found that frequent mobile phone use may be linked to higher prevalence of symptoms consistent with fibromyalgia, tendinitis, De Quervain's tenosynovitis, and myofascial pain syndrome. 16 These findings support a potential link between phone-related behaviors and more serious physical complaints.
Research gap
Despite growing recognition of musculoskeletal strain related to mobile phone use, a gap in the literature exists regarding hand-specific conditions that may progress to require surgical intervention. Most existing studies emphasize general symptoms or nonsurgical conditions, with limited attention to the types, severity, and clinical course of hand pathologies associated with device use. This gap restricts our ability to assess the true burden of surgically relevant hand disorders, particularly in occupational settings where prolonged mobile phone use is common.
Study purpose
To address the gap, this systematic review aims to exclusively focus on hand pathologies requiring surgical consideration, building upon prior work. Specifically, it seeks to categorize these conditions by pathology type, describe their clinical presentation and management, and evaluate the quality of the existing literature. This review addresses two core questions: (1) What surgical hand pathologies have been associated with mobile phone use? and (2) What is the management of these conditions? Findings are categorized by pathology type—grouped into inflammatory, nerve-related, pain-related, and other categories—followed by a discussion of the clinical presentation and management of each condition.
Given the pervasive use of mobile devices across all age groups and work environments, understanding the potential link between mobile phone use and surgically significant hand pathologies is increasingly important. This knowledge can help inform clinical decision-making, workplace ergonomic standards, and public health policies aimed at reducing injury risk. By systematically identifying and categorizing these surgical conditions, this review aims to provide valuable insights for healthcare providers, occupational health practitioners, and policymakers. Such information is essential to support targeted prevention efforts and timely interventions that may ultimately decrease disability, improve worker health, and reduce the overall healthcare burden associated with mobile phone overuse.
Methods
Study and methodology
A systematic literature review was conducted using Embase, PubMed, and Scopus databases. Inclusion criteria were all studies evaluating hand injuries in individuals who used handheld devices. Exclusion criteria were studies that evaluated non-hand anatomy or non-hand injuries. Two reviewers independently performed initial title and abstract screening for inclusion. If discordant, a discussion was held with the final decision made by the senior reviewer. Studies then underwent a full-text analysis.
A comprehensive Boolean search strategy was used across all databases, combining terms related to handheld device use and musculoskeletal conditions of the hand: (“texting” OR “text messaging” OR “mobile phone” OR “smartphone” OR “cell phone” OR “handheld device*” OR “phone use” OR “touchscreen device*” OR “mobile device*” OR “digital device*” OR “repetitive thumb use”) AND (“de Quervain” OR “trigger thumb” OR “thumb pain” OR “carpal tunnel” OR “arthritis” OR “tendinitis” OR “tenosynovitis” OR “hand pain” OR “wrist pain” OR “hand injury” OR “hand disorder*” OR “overuse injury” OR “repetitive strain injury” OR “musculoskeletal disorder*” OR “upper extremity pain” OR “hand pathology”)
Data extraction and synthesis
Data extraction was performed from the included studies. Relevant information including year of publication, population size, study design, measured outcomes, assessment of one or both hands of individuals, and type of handheld device were extracted. Of note, data involving elbows, shoulders, neck, upper back were not included in extraction. Methodological quality was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist. Two independent reviewers conducted the appraisal for each included study. Discrepancies in scoring were resolved by consensus or adjudicated by a third reviewer. The results of the appraisal were used to inform the interpretation of findings and to guide the synthesis of evidence across studies.
Patient and public involvement
The public was not involved in the design or conduct of this study due to the nature of systematic reviews.
Results
Study characteristics
A total of 588 studies were initially screened (
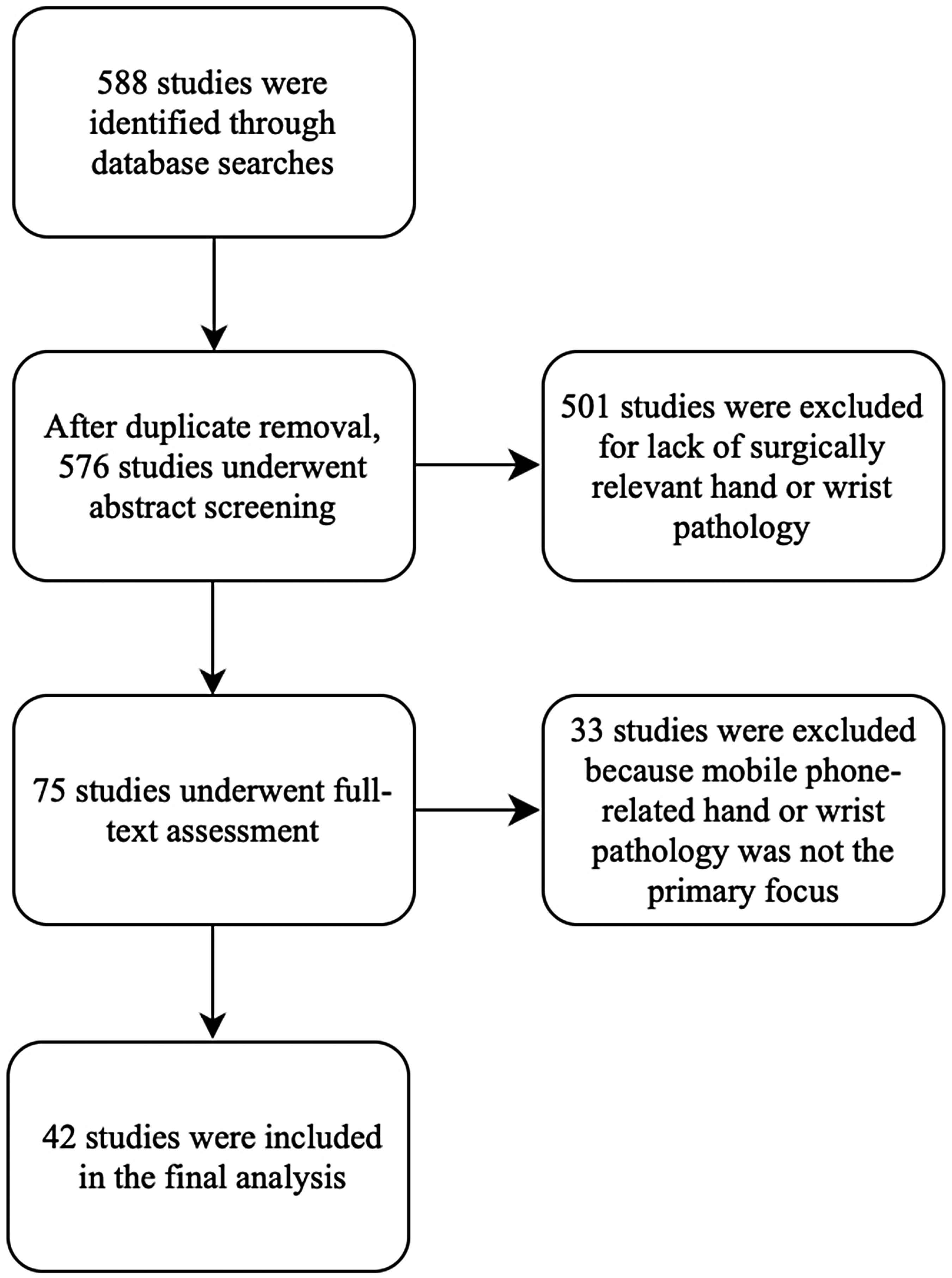
Flow diagram of study selection.
Study characteristics of the 42 included studies.
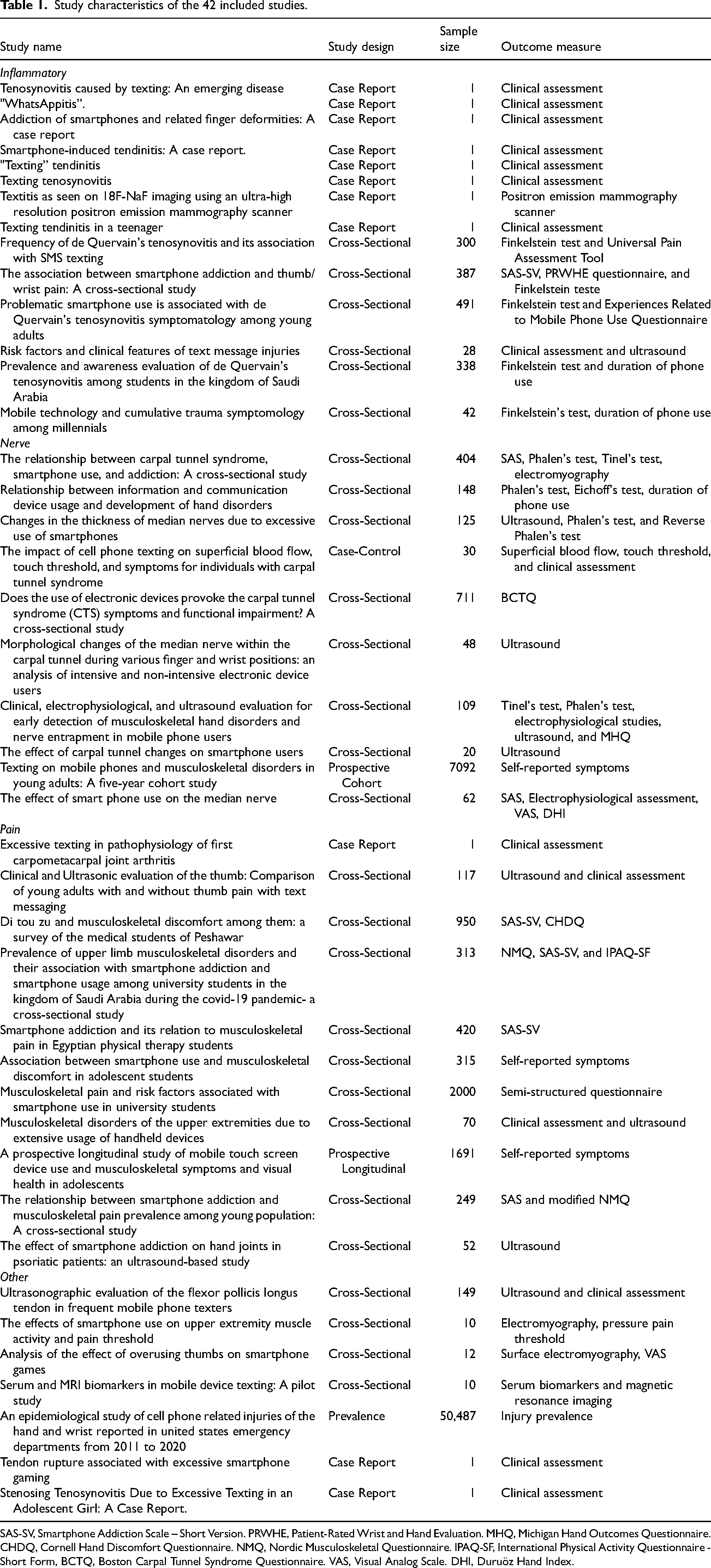
SAS-SV, Smartphone Addiction Scale – Short Version. PRWHE, Patient-Rated Wrist and Hand Evaluation. MHQ, Michigan Hand Outcomes Questionnaire. CHDQ, Cornell Hand Discomfort Questionnaire. NMQ, Nordic Musculoskeletal Questionnaire. IPAQ-SF, International Physical Activity Questionnaire - Short Form, BCTQ, Boston Carpal Tunnel Syndrome Questionnaire. VAS, Visual Analog Scale. DHI, Duruöz Hand Index.
The Joanna Briggs Institute (JBI) Critical Appraisal Checklist was utilized to assess methodological quality. 17 These structured tools evaluate parameters such as the identification and handling of confounding variables, validity of outcome measures, and clarity of inclusion criteria ( Supplemental Table 1 ). Appropriate checklists were applied based on study design, including cross-sectional, case report, case-control, prevalence, prospective cohort, and longitudinal cohort studies. The majority of studies (n=31) met all or most of the criteria for methodological quality. A common limitation observed in case reports was the lack of reporting on adverse events. As a whole, there was a wide spectrum of demographic, mobile phone usage, and intervention/outcomes data; however, studies were divided into four categories based on type of injury: inflammatory (n=14), nerve pathology (n=10), pain (n=11), and other (n=7).
Inflammatory (tendinitis/tenosynovitis)
The most common inflammatory hand condition in our study was De Quervain's tenosynovitis. Four studies on de Quervain's were case reports that involved patients sending 250 to 2500 text messages per month, using a 130 gram phone for six hours, or having a recent phone size change all with resultant wrist pain.18–21 These cases were treated conservatively with reduced phone usage, splinting, or activity modification. Another study found that patients with high mobile phone dependence, 42% of whom reported wrist/thumb pain, were more likely to have a positive Finkelstein test as their mobile use increased. 22 One study utilized the smartphone addiction scale (SAS) and reported 66.4% of the cohort to qualify as “phone addicts” and 20.4% of this cohort to have pain in the thumb/wrist; however, a positive Finkelstein test was not associated with smartphone addiction. 23 This is contrary to the remaining three studies that reported Finkelstein's test as a valuable test to diagnose de Quervain's in the setting of significant mobile phone usage.10,24,25
Furthermore, five studies focused on inflammatory-related pathology that was not classified as De Quervain's. Of these, one analyzed an individual who spent over 15 h daily with his hands in a fixed position, exhibiting a swan neck deformity of the third digit, and ultrasound findings suggesting extensor tenosynovitis of multiple digits. 26 Other studies have investigated patients with various presentations of hand tendinitis thought to be texting induced including tenderness when extending or abducting the thumb or wrist.27–29 Another study utilized a positron emission mammography scanner to reveal increased uptake in the first carpometacarpal, trapezium-scaphoid, and second metacarpophalangeal joints in the setting of excessive texting; as well, bone tracer F-NaF was able to identify repetitive strain injury to the thumb. 30
Nerve
Carpal tunnel syndrome (CTS) was the most common nerve pathology present in our studies. In one study involving 404 subjects, the risk of CTS symptoms increased by 29.2% when mobile phone usage increased by one hour. 9 A study also reported that an average of five hours of mobile phone usage per day was an approximate cutoff for median nerve impact. 31 Another study determined that Phalen's test and reverse Phalen's tests occurred in a statistically significant shorter amount of time in subjects with the highest duration of mobile phone use. 32 Others reported that there is no significant association between hand dominance and carpal tunnel syndrome development in frequent texters, though a significant association was observed with younger age, females, and high BMI. 33 In a study examining the effect of phone use on those with carpal tunnel syndrome diagnosis compared to those without, those with CTS had a 53% increase in touch threshold at baseline which increased even further following a texting task. Additionally, this threshold did not return to baseline even after 10 min. 34
Furthermore, a subset of studies examined median nerve pathology, but not in the context of carpal tunnel syndrome. Three studies investigated the median nerve's cross-sectional area or circumference, revealing an increase associated with texting.35–37 Additionally, one study tracked over 2000 texters for a five-year period and found that individuals without symptoms at baseline were more prone to developing hand paresthesia. 38 A study concentrated on median nerve function, noting that infrequent texters exhibited faster motor and sensory conduction than frequent texters. 39
Pain
Hand pain was the primary outcome analyzed in 11 studies. In patients with and without psoriatic arthritis, inflammatory changes were observed on ultrasound of hand joints when mobile phone addiction was present. 40 A case report highlighted a patient with arthritis of the first carpometacarpal joint requiring excision arthroplasty following more than three years of significant mobile phone use. 41 One study evaluating 117 students who sent up to 200 texts per day had statistically significant results for metacarpophalangeal and carpometacarpal joint pain, measured using the Numeric Pain Rating Scale. 42 A different study reported that in 950 students who utilized mobile phones frequently, discomfort in the thenar area was most common. 43 Three studies concluded that an SAS-SV score indicating phone addiction was significantly correlated with hand-related pain, particularly in the setting of more than six hours of phone use.44–46
Moreover, a study reported a significant relationship between the amount of mobile phone use and the number of body parts with musculoskeletal discomfort, with the 1–3 hours of texting group experiencing the highest level of discomfort. 47 Another study investigated characteristics of phone usage and concluded that the size of a smartphone was the strongest predictor of musculoskeletal pain, and 17.45% of 2000 students reported site-specific thumb pain. 48 Additionally, 70 patients with extensive handheld device usage were retrospectively analyzed and 100% reported thumb pain with correlation present between hand dominance and musculoskeletal disorder. 49 Conversely, a prospective study that evaluated 1691 students assessed at baseline and one-year follow-up reported no statistically significant dose-response relationship between smartphone use duration and musculoskeletal symptoms. 50
Other
The studies that did not fall into previous categories were grouped together. Muscle function was one area of exploration and in two studies, the flexor pollicis longus was found to be hypertrophied or with higher muscle activity in one-handed texters.51,52 Similarly, using median frequency as an indicator of muscle fatigue, abductor pollicis brevis and extensor pollicis brevis were found to be fatigued at a significantly higher rate following mobile phone use. 53 Additionally, inflammatory biomarkers such as TNF-RI were investigated and found to be elevated in frequent texters. 54 Another study focused on mobile phone-related injuries in over 50,000 patients, with falls being the most common mechanism of injury followed by phone repair injuries and texting. 55
Moreover, two case reports highlight less common, but significant injuries associated with texting. One study detailed a patient who engaged in all-day mobile phone video gaming for six to eight weeks, resulting in tendon rupture. 56 Another study described a case of trigger finger in the setting of sending 8507 texts per month. 57
Discussion
This systematic review of 42 studies, encompassing over 67,000 participants, aimed to characterize the spectrum of surgically relevant hand pathologies associated with mobile phone use. Our findings successfully address this objective by identifying a consistent pattern of conditions linked to repetitive strain from device usage. De Quervain's tenosynovitis and CTS were the most frequently reported conditions, linked to repetitive thumb and wrist strain and prolonged device use. Pain syndromes, particularly in the thumb and thenar areas, were commonly reported and correlated with phone addiction and usage duration. Less frequent but notable pathologies, including tendon ruptures and trigger finger, were also reported. These findings confirm that habitual mobile phone use can lead to musculoskeletal strain injuries, some of which may progress to require surgical evaluation or intervention.
Our findings align with and build upon previous systematic reviews examining musculoskeletal complaints associated with mobile phone use. Similar to Zirek et al., who identified pain as the most frequently reported symptom and tendinitis as the most common pathology, our review found that inflammatory conditions, particularly De Quervain's tenosynovitis, were the most prevalent diagnoses, especially among frequent texters. 16 However, in contrast to prior reviews that emphasized general discomfort or early-stage symptoms, our analysis focused on conditions with potential surgical implications, such as tendon ruptures and advanced carpal tunnel syndrome. This highlights the potential severity of cumulative strain injuries related to mobile phone use. Additionally, while Cao et al. broadly categorized the risk of chronic disorders associated with improper phone use, including wrist-related complaints, our review builds upon this framework by providing a more detailed breakdown of specific diagnoses, clinical signs (e.g., Finkelstein's test), and diagnostic modalities (e.g., EMG, ultrasound, nerve conduction testing), thereby enhancing the clinical and occupational applicability of these findings. 58
Several studies, including those by Mersal et al. and Yaghmour et al., have reported associations between texting frequency and tendinopathy or pain.15,59 Our review complements and expands on these observations by offering a more nuanced synthesis of device use patterns in relation to pathology type. For example, although Yaghmour et al. did not find a significant association between hours of device use and carpal tunnel syndrome, our analysis identified studies reporting an increased risk of CTS with longer daily usage, particularly beyond five hours per day. 15 Differences in population demographics, gender distribution, and diagnostic criteria may contribute to this variability. Our review further highlights female gender, younger age, and higher BMI as consistent risk factors, consistent with Mersal et al.'s findings of higher complaint rates among female users. 59 While studies like Bruyneel and Duclos emphasize injury risk during mobile use while walking, our findings demonstrate that sedentary, repetitive device use alone can produce clinically significant injuries. 60
Taken together, these findings contribute to the occupational health and rehabilitation literature by identifying mobile phone use as a modifiable risk factor for conditions such as De Quervain's tenosynovitis and carpal tunnel syndrome. These findings highlight the importance of early recognition and intervention, particularly in work environments where prolonged mobile device use is common. The synthesis of usage patterns—such as daily use exceeding specific thresholds—offers actionable benchmarks for developing ergonomic guidelines and workplace preventive strategies. By contextualizing these conditions within a framework of occupational exposure and cumulative strain, this review advances current understanding and supports targeted clinical assessments and interventions to mitigate long-term disability.
Several limitations warrant consideration. As a systematic review of studies with varied methodologies, populations, and outcome measures, the findings reflect a heterogeneous dataset. This variability limits the ability to draw statistically robust conclusions. Additionally, few of the included studies offered longitudinal follow-up, restricting insights into the long-term biomechanical consequences of mobile phone use. Despite these limitations, the convergence of key themes across studies suggests that the identified pathologies represent a credible and emerging area of concern for both medical and surgical practitioners.
Future research should prioritize longitudinal cohort and intervention studies using standardized outcome measures to clarify causality and evaluate preventive strategies. Mechanistic studies exploring the pathophysiology of mobile phone-related hand injuries could further elucidate underlying processes. Furthermore, given the increasing integration of mobile technologies into occupational settings, our findings highlight the need for employer education, ergonomic policy implementation, and occupational surveillance programs targeting mobile device–related musculoskeletal risk.
Conclusion
With mobile phone use continuing to increase across all age groups, its potential association with hand pathologies of surgical relevance is an emerging area of clinical and occupational interest. This systematic review identified common conditions, including De Quervain's tenosynovitis and carpal tunnel syndrome, that may be linked to prolonged or repetitive device use. Occupational health practitioners and employers should consider incorporating mobile device use assessments into routine screenings and promote ergonomic training to reduce cumulative strain injuries.
Supplemental Material
sj-docx-1-wor-10.1177_10519815261421502 - Supplemental material for Hand injuries associated with mobile phone use: A systematic review
Supplemental material, sj-docx-1-wor-10.1177_10519815261421502 for Hand injuries associated with mobile phone use: A systematic review by Savannah C Braud, Melinda J Choi, Kyle Y Xu and Kashyap Komarraju Tadisina in WORK
Supplemental Material
sj-xlsx-2-wor-10.1177_10519815261421502 - Supplemental material for Hand injuries associated with mobile phone use: A systematic review
Supplemental material, sj-xlsx-2-wor-10.1177_10519815261421502 for Hand injuries associated with mobile phone use: A systematic review by Savannah C Braud, Melinda J Choi, Kyle Y Xu and Kashyap Komarraju Tadisina in WORK
Footnotes
Acknowledgements
Not applicable.
Ethical approval
This systematic review involved only previously published literature and did not include new data from human participants, human tissue, or identifiable personal information. Therefore, ethical approval was not required.
Informed consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
This study is a systematic review of previously published literature. No new data were generated or analyzed during this study. Therefore, data sharing is not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.